Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Describing and Quantifying Wrong-Patient Medication Errors Through a Study of Incident Reports
Authors Takahashi M ![]() , Okudera H, Wakasugi M, Sakamoto M, Shimizu H, Wakabayashi T, Yamanouchi T, Nagashima H
, Okudera H, Wakasugi M, Sakamoto M, Shimizu H, Wakabayashi T, Yamanouchi T, Nagashima H
Received 26 April 2022
Accepted for publication 13 August 2022
Published 23 August 2022 Volume 2022:14 Pages 135—146
DOI https://doi.org/10.2147/DHPS.S371574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Megumi Takahashi,1 Hiroshi Okudera,2 Masahiro Wakasugi,2 Mie Sakamoto,2 Hiromi Shimizu,3 Tokie Wakabayashi,3 Tsuneaki Yamanouchi,3 Hisashi Nagashima2
1Department of Quality and Patient Safety, Tokyo Medical University, Tokyo, Japan; 2Department of Crisis Medicine and Clinical Safety, University of Toyama, Toyama, Japan; 3Department of Medical Management Office, Toyama University Hospital, Toyama, Japan
Correspondence: Megumi Takahashi, Department of Quality and Patient Safety, Tokyo Medical University, 6-7-1, Nishishinjuku, Shinjuku, Tokyo, Japan, Tel +81 3 3342 6111 Ext 3939, Fax +81 3 5339 3791, Email [email protected]
Purpose: Our aim was to inform a new definition of wrong-patient errors, obtained through an analysis of incident reports related to medication errors.
Methods: We investigated wrong-patient medication errors in incident reports voluntarily reported by medical staff using a web-based incident reporting system from 2015 to 2016 at a university hospital in Japan. Incident report content was separately evaluated by four evaluators using investigational methods for clinical incidents from the Clinical Risk Unit and the Association of Litigation and Risk Management. They investigated whether it was the patient or drug that was incorrectly chosen during wrong-patient errors in drug administration in incident reports and assessed contributory factors which affected the error occurrence. The evaluators integrated the results and interpreted them together.
Results: Out of a total 4337 IRs, only 30 cases (2%) contained wrong-patient errors in medication administration. The cases where the intended drugs were administered to incorrect patients occurred less frequently than cases where the wrong drugs were administered to the intended patients through the investigation of wrong targets. After a discussion, the evaluators concluded that the patient - drug/CPOE screen mismatch, caused by choosing the wrong patient, drug, or CPOE screen (mix-ups), occurred in the wrong-patient medication errors. These errors were caused by three conditions: (1) where two patients/drugs were listed next to one another, (2) where two patients’ last names/drugs’ names were the same, and (3) where the patient/drug/CPOE screen in front of the staff involved was believed to be the correct one. Additionally, these errors also involved insufficient confirmation, which led to failure to detect and correct the mismatch occurrences.
Conclusion: Based on our study, we propose a new definition of wrong-patient medication errors: they consisted of choosing a wrong target and insufficient confirmation. We will investigate other types of wrong-patient errors to apply this definition.
Keywords: wrong-patient error, medication error, web-based incident reporting system, computerized physician order entry, human error
Introduction
Medication errors are defined as errors in the process of ordering or delivering a medication and can occur at any stage in the drug ordering, dispensing, and administration process.1 These errors often lead to serious patient injuries, which are categorized as adverse drug events (ADEs).1,2 The representative study on medication errors reported that 6.5% of adult inpatients suffered ADEs2 and another study reported ADEs occurred in 27.4% of adult outpatients.3 Most of the medication errors and ADEs occurred at the ordering and administration stages.1–4 Before-after studies, which evaluated the effect of a computerized physician order entry (CPOE) system or barcode verification within an electronic medication-administration system (eMAR), showed the reduction of ADEs at the ordering and administration stages.5,6
Among medication errors, there are several error types, such as “wrong dose”, “wrong frequency”, and “wrong drug” errors.2,5–8 In addition, wrong-patient errors in medication administration are often reported. Wrong-patient errors can occur in various areas of healthcare, such as drug administration, phlebotomy, blood transfusions, and surgical interventions.9 Regarding medication administration, wrong-patient error may also cause ADEs.9,10 For instance, administration of sedative drugs to the wrong patient can lead to a disturbance in consciousness, or an insulin injection given to the wrong patient can lead to hypoglycemia or a life-threatening condition.9–11 Although in the usual wrong-patient errors, patients themselves are incorrectly chosen, several other patterns or errors in medication administration also exist, such as the intended patient receiving the wrong drug or the intended drug going to the incorrect patient. To date, few studies have investigated whether it was the patient or drug that was incorrectly chosen during wrong-patient errors in drug administration,11–14 but no clear definition of wrong-patient errors in drug administration has been proposed. Therefore, our aim was to further investigate and define wrong-patient errors in medication administration by examining incident reports (IRs), which were voluntarily reported by medical staff, through a web-based incident reporting system.
Materials and Methods
Hospital Setting
The participating hospital was a tertiary care hospital, which has 612 beds and provides highly advanced medical care, technology, and training, with the help of 372 physicians, 569 nurses, 34 pharmacists, 120 medical technology staff and 68 administrative staff.15
Study Design
This study was planned as a retrospective observational study and approved by the Toyama University Hospital’s Clinical Research and Ethical Committee (2015–89) on November 25, 2015. It was conducted in accordance with the guidelines outlined in the Declaration of Helsinki. The subjects of this study were IRs, not patients; therefore, patient information was not obtained, and the need for informed consent from patients was waived by the committee. Data were fully anonymized and were considered not to include identifying information for involved patients and medical staff.
Incident Reporting System
A web-based incident reporting system (HOPE incident reporting system, Fujitsu Limited, Japan) was introduced at the participating hospital, which is linked to the electronic health record (EHR) system. Health care professionals involved in or witnessing patient safety incidents submit IRs through this system. This system can be accessed from all computer terminals in the hospital EHR system, allowing for anonymous incident reporting. Reporters enter the incident information in the recommended format.15,16 The required information consists of the medical category in which the incident occurred, severity of incident, type of staff involved, type of error, and incident details, which were established by the national adverse event reporting system of the Japan Council for Quality Health Care17 and widely accepted throughout Japan. The medical category in which the incident occurred consists of “medication”, “blood transfusion”, “therapeutics and procedures”, “medical devices and equipment”, “lines and tubes”, “clinical laboratory tests”, “medical care (eg, falls, slips, meals, etc.)”, and “other” (Table 1).17 The “medication” category further requires that the stage of drug administration (eg, prescribing, dispensing, formulation management, medication preparation, and administration) be listed when reporting the error.17 The incident severity also needs to be entered, based on the national incident severity classification, which is defined by the National University Hospital Council of Japan (Table 2).18 For example, incident level 0 means that an error occurred, but was corrected before implementation, while the most severe, incident level 5, means there was a patient death caused by provided medical care. Cases that are incident level 3b or higher are regarded as ADEs. IRs which were submitted by reporters are stored in a database and are available by using keyword retrieval.
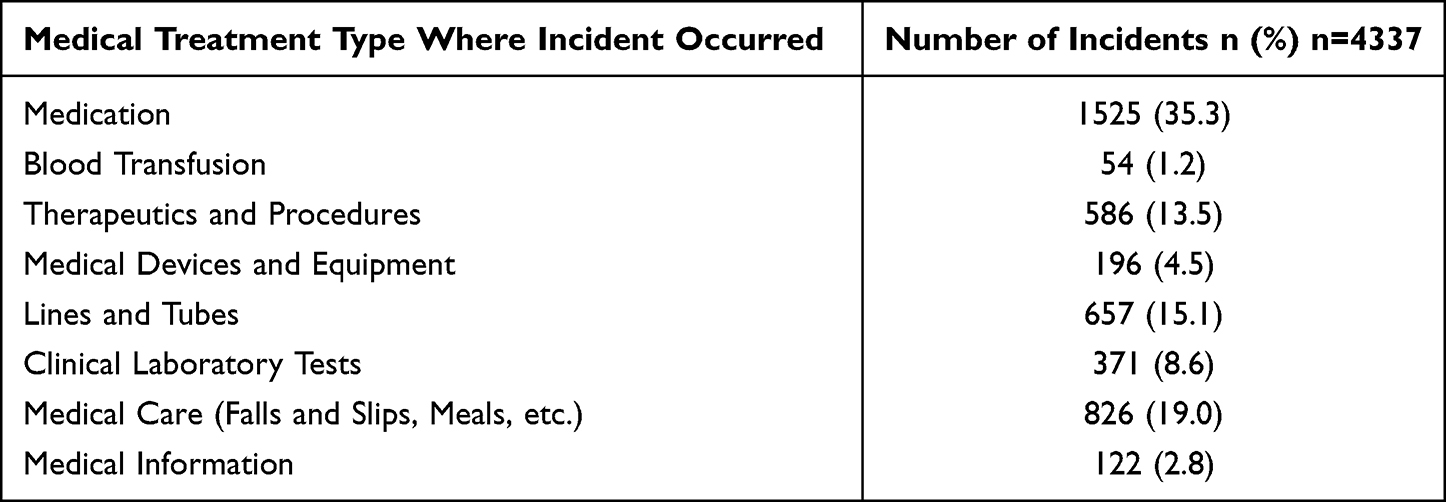 |
Table 1 Medical Treatment Type for Incident Reports |
 |
Table 2 Incident Levels Representing the Degree of Impact on Patients |
Flow of Drug Administration
A CPOE system and clinical decision support system (CDSS) were available at the participating hospital. At ordering, the CDSS not only provides computerized advice regarding drug dose, but also checks for drug allergy.19,20 Prescriptions are completed by physicians on computer terminals (prescription stage), and the transcriptions are generated in the CPOE system. Medication, which is dispensed (dispensing stage) and prepared by a pharmacist (formulation management and medication preparation stage), is dispatched from the pharmacy department and distributed by the ward nurses to the designated patient location. Intravenous (IV) drugs are placed in boxes and oral drugs are placed in small plastic cases with a note attached including the patient’s name (medication preparation stage). The nurses manually carry the IV drugs or oral drugs to the rooms where the patients are located and administer the medication. At the drug administration stage, the nurses have to identify the patients by asking them to provide their names and checking the ID number on the patients’ wristbands before oral medication administration. For IV drug administration only, the nurses can use the barcodes on the wristband to scan and check the patient’s identity. This is because our CPOE and eMAR systems can issue the labels which the barcodes for patient identification are printed on only for ordering IV drugs, not oral medication.
Data Collection
We collected IRs related to medication errors from the hospital incident reporting system, between April 1, 2015 and March 31, 2016. We used simple statistics for each type of medication error, incident level, type of staff involved, and the stage of drug administration where the error occurred. Among them, the IRs for wrong-patient errors in medication errors were extracted. Then the types of drugs (oral drugs, IV drugs), which were handled in the wrong-patient errors in medication errors and “the wrong targets” (patients, drugs), that is incorrectly chosen targets during these errors, were investigated. In addition, the incident level items, the type of staff involved, and the stage of drug administration were examined. Then, four evaluators consisting of a physician, two nurses, and a pharmacist, belonging to the hospital’s department of patient safety management, analyzed the content of the IRs separately, and identified the contributing factors for wrong-patient errors in medication administration. The methods of analysis for wrong-patient errors in medication errors in the IRs were adapted from the investigation methods for clinical incidents provided by the Clinical Risk Unit and the Association of Litigation and Risk Management.21 Finally, the four evaluators integrated their evaluations and discussed their interpretations.
Results
Medication Errors in Incident Reports
A total of 4337 incidents were reported between April 2015 and March 2016. Among them, medication-related incidents were the most prevalent (1525 cases, 35.3%) (Table 1). Of the medication-related incidents, the largest number of incidents occurred at the medication administration stage (977 cases, 64.1%), followed by the preparation stage (200 cases, 13.1%), prescription stage (188 cases, 12.3%), dispensing stage (95 cases, 6.2%), and formulation management stage (65 cases, 4.3%; Table 3). The most frequent errors were due to “omission” (361 cases, 23.7%) and “wrong dose”, including “overdose” and “underdose” (242 cases, 15.9%), throughout all stages of drug administration (Table 3). At the prescription stage, responses of “others” was most prevalent (73 cases, 38.8%), followed by “wrong dose” (52 cases, 27.7%) and “omission” errors (36 cases, 23.7%). On the other hand, at the medication administration stage, the most frequent errors were “omission” (281 cases, 28.7%), “wrong dose” (155 cases, 15.9%), “wrong administration timing” (106 cases, 10.8%), and “others” (233 cases, 23.8%).
 |
Table 3 Error Types and Stages of Medication Errors in the Incident Reports |
Wrong-Patient Errors in Medication Administration
Wrong-patient errors were included in only 30 cases (2.0%) in the IRs related to medication administration (Table 3). These mostly occurred at the medication administration stage (23 cases, 76.7%). In contrast, six cases (20%) occurred at the medication preparation stage and 1 case (3.3%) occurred at the prescription stage (Table 3). For the type of staff involved, nurses were involved in 27 cases (90%), a physician was involved in one case (3.3%), and a pharmacist was involved in two cases (6.7%; Table 4). For incident level, there were no cases of incident level 3a or higher, which were considered ADEs. There were 12 incident level 2 cases (40%) where errors were implemented and slightly affected patients’ health without treatment and 14 incident level 1 cases (46.7%) where errors were implemented without harm. There were four incident level 0 cases (13.3%) where errors were corrected before implementation (Table 4). As for drug type, there were 21 cases of oral drug errors (70%) and 9 cases of IV drug errors (30%; Table 4).
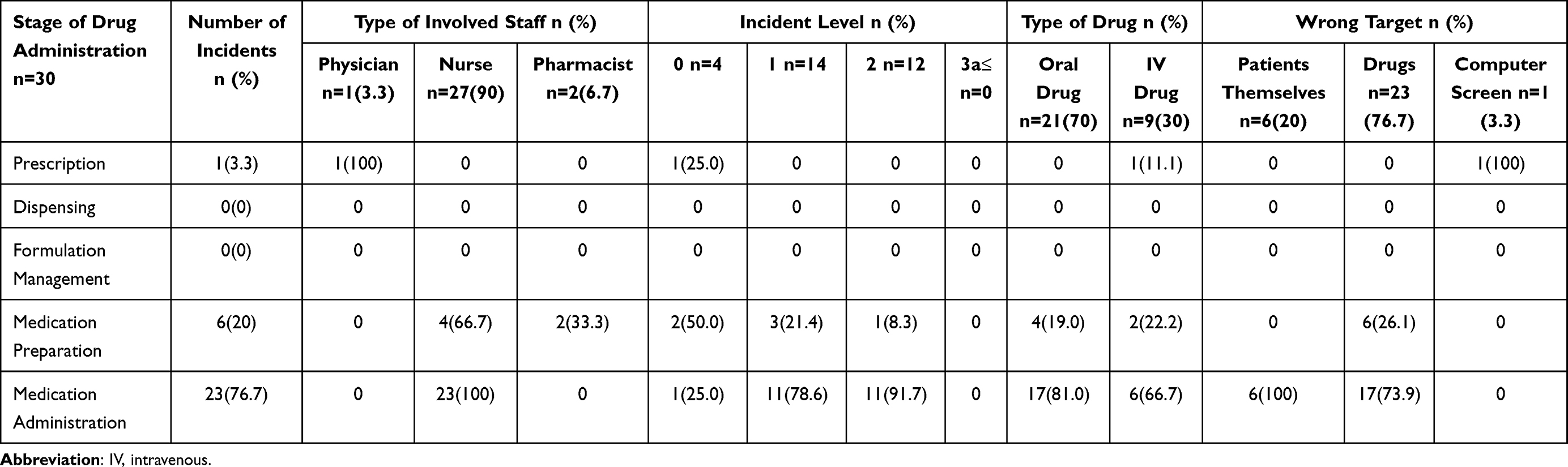 |
Table 4 Wrong Targets and Event Information in Incident Reports with Wrong-Patient Errors |
Wrong Targets in Wrong-Patient Errors of Medication Administration
For incorrectly chosen targets during wrong-patient errors in medication administration, there were only six cases (20%) where the wrong patient was chosen, and all of these cases occurred at the administration stage. Most of them (23 cases, 76.7%) were caused by picking up the wrong patient’s drugs. Furthermore, in one case (3.3%), the ward physician ordered the antibiotic drug through the CPOE screen of the wrong patient, which was due to using the same screen from another patient’s examination order before prescribing (Table 4). The evaluators found that cases where the intended drugs were administered to incorrect patients occurred less frequently than cases where the wrong drugs were administered to the intended patients. After a discussion, the evaluators concluded that the drug-patient mismatch or the CPOE screen-patient mismatch, caused by choosing the wrong patient, drug, or CPOE screen (mix-ups), occurred in the wrong-patient errors in medication administration through the investigation of wrong targets. (Table 4)
Contributory Factors for Wrong-Patient Medicaiton Errors
The first evaluator, who was a physician, focused on the environment where mix-ups occurred. The evaluator found that contributory factors for the mix-up occurrence included conditions where two patients/drugs were listed next to one another, where two patients’ last names/drugs’ names were the same, and where staff involved firmly believed that the patient/drug/CPOE screen in front of him/her was the correct one (Table 5). The second and third evaluators, who were nurses, focused on the confirmation action. They found that most of the incidents were caused by insufficient confirmation, which is a violation of the hospital patient identification rule. It was mostly caused by the impatience of medical staff. Furthermore, they found that 20–30% of the cases were categorized by recognition failures where the patient/drug/CPOE screen in front of the staff involved was believed to be correct. They concluded that in these cases, medical staff did not confirm it in the fixed procedure because it was believed to be correct (Table 5). The fourth evaluator, who was a pharmacist, found the same contributory factors for the drug-patient mismatch as the first evaluator. This evaluator further noted that two cases (6.7%) where pharmacists were involved in the medication preparation were caused by insufficient patient identification, making it a case of confirmation rule violation (Table 5).
 | 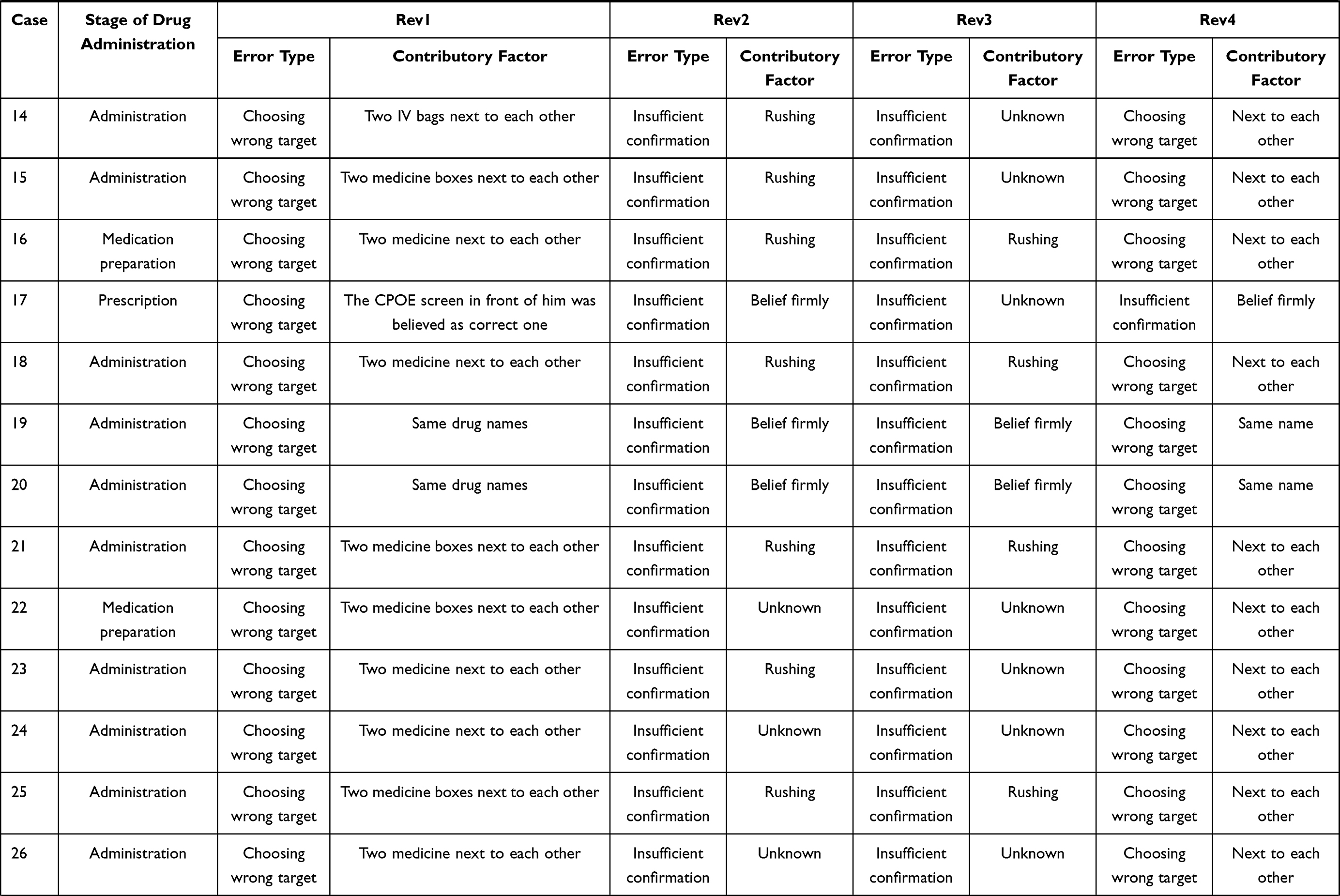 |  |
Table 5 Contributory Factors for the Error Occurrences |
After discussing the findings, the evaluators concluded that wrong-patient errors in medication administration consisted of two types of errors: choosing wrong targets and insufficient confirmation. Choosing wrong targets led to mismatches between the patient and the drug or the CPOE screen, and insufficient confirmation was the violation of confirmation rules set by the hospital, which failed to detect and correct the mismatch occurrences. Furthermore, in medication administration, choosing wrong targets, which led to the occurrence of mismatches between the patient and the drug or the CPOE screen, was caused by three types of conditions: (1) where two patients/drugs existed next to one another, (2) where two patients’ last names/drug names were the same, and (3) where the patient/drug/CPOE screen in front of the staff involved was believed to be correct without confirmation (Table 5). The contributory factor for insufficient confirmation, which was the violation of the hospital confirmation rule in wrong-patient errors in medication administration, was the provider’s psychological state, resulting in the involved staff being impatient, or having recognition failure, where the patient/drug/CPOE screen in front of the staff involved was believed to be correct.
Discussion
In this study, medication-related incidents were the most prevalent in IRs reported during 2015–2016. Among medication-related incidents, the largest number of incidents occurred at the medication administration stage (64.1%) with IRs occurring at the prescribing stage accounting for only 12.3% of the total incidents. The most frequent errors were “omission” (23.7%) and “wrong dose” (15.9%). In previous reports of medication errors, medication errors and ADEs mostly occurred at the prescribing and administration stages, and the most frequent error type was “wrong dose.”1,2,4 However, it was also reported that CPOE systems, where physicians wrote orders directly on the computer, reduced legibility problems and transcriptional errors, and that the CDSS, which provided computerized advice regarding drug dose and checked for drug allergy, reduced dose errors and ADEs.1,5,19,20 In the participating hospital, the CPOE system and CDSS were available, so the few errors at the prescribing stage and those due to “wrong dose” should have been prevented by these systems. On the other hand, in our study, errors at the medication administration stage were most frequent. In previous studies, the use of barcode scanning, which connected to the eMAR, improved the accuracy of patient identify verification and medication administration and reduced the occurrence rate of medication errors at the administration stage.6,22 In the participating hospital, verification using barcode scanning was used only in the implementation of IV drugs because of our CPOE and eMAR systems. This might have affected the large number of IRs related to medication administration occurring at the administration stage.
Wrong-patient errors were included in only 30 cases (2.0%) of IRs involving medication errors in this study. However, this small sample was still able to provide us with useful information for enhancing the definition of wrong-patient errors. From our results, wrong-patient errors in drug administration were involved in two primary types of actions: (1) choosing an incorrect target (patient, drug, or CPOE screen) which led to a mismatch between a patient and a drug or CPOE screen and (2) a failure to correct these mismatches caused by insufficient patient confirmation, in violation of the hospital confirmation rule. Furthermore, we discussed and expected that common wrong-patient errors also consisted of incorrectly choosing a target (patient or medical care) which led to the mismatch between patients and their medical care, and insufficient confirmation by medical staff. We concluded it was necessary to investigate other type of wrong-patient errors and consider whether this definition fitted those errors.
The Emergency Care Research Institute (ECRI) published a special report on “patient identification error”, which presented a literature review on studies related to wrong-patient incidents.23 In this report, “wrong-patient errors” were defined as “patient identification errors” and the cause of these errors was identified as poor adherence to the patient identification protocol. We considered that wrong-patient errors consisted not only of patient misidentification, but of mismatches between patients and their medical care, and poor identification by medical staff was not the cause of them, but the error itself which consisted of them.
Reason divided human errors into mainly two types of actions: unintended and intended.23
The errors caused by unintended actions were called “slips” or “lapses”, which resulted from some failures in the execution and/or storage stage of an action sequence. Those caused by intended actions were called “mistakes”, defined as deficiencies or failures in the judgment and/or inferential processes involved in the selection of an objective, or in the specification of the means to achieve it.23 We considered that choosing wrong targets which led to the occurrences of mismatch belonged to “slips”, while insufficient confirmation which failed to correct the errors belonged to “mistakes.”
Slips were reported to occur in simple tasks caused by the impairment of automatic procedural routines, which was affected by extrinsic factors.23 We identified three types of conditions as the contributory factors for the occurrence of the drug-patient/CPOE screen-patient mismatch: (1) where two patients/drugs existed next to one another, (2) where two patients’ last names/drugs’ names were the same, and (3) where the patient/drug/CPOE screen in front of the staff involved was believed to be correct. Although the condition where the patient names were similar has been reported as a contributory factor of the wrong-patient errors,8 the other conditions have not been mentioned in previous studies on wrong-patient errors. In these cases, the staff involved firmly believed that the patient/drug/CPOE screen that was picked up by him/her or in front of him/her was the correct one. It was supposed that the targets (patients/drugs/CPOE screen) next to the correct ones or in front of the staff involved, caught his/her attention and were believed to be correct ones. We thought that it is necessary to investigate the contributory factors for other types of wrong-patient errors in the future.
On the other hand, mistakes were reported to occur in rather complicated tasks caused by failures of higher-order cognitive processes, which were affected by intrinsic/extrinsic factors.23 We identified that the contributory factors for insufficient confirmation in wrong-patient errors in drug administration were conditions where the staff involved was rushing, or strongly believed that the patient/drug/CPOE screen was the correct one. In previous studies, a contributory factor for insufficient patient confirmation was the cumbersome and unclear identification protocol process.11–14 In our study, we revealed that staff involved in the error believed that the patient/drug/CPOE screen was correct, which introduces another contributory factor for insufficient patient confirmation. One explanation for this action may be the concept of “cognitive bias”.24–26 Based on this concept, humans tend to find ways to justify their own actions as correct. We concluded that, in wrong-patient errors in medication administration, because the targets which were chosen by involved medical staff were believed to be correct, the procedures for confirmation were supposed to be unnecessary and omitted by him/her. We thought that it is also necessary to investigate the contributory factors for insufficient confirmation in other wrong-patient errors.
Limitations and Future Direction
Although we examined IRs to inform the definition of wrong-patient errors in medication administration in the current study, the number of IRs involving wrong-patient errors in medication administration was small. It would be beneficial to evaluate a larger number of cases in the future. Furthermore, we plan to consider whether the revised definition and newly defined contributory factors from the current study will apply to other wrong-patient errors in future studies.
Conclusion
Through our study, we proposed a new definition of wrong-patient medication errors: that they consisted of choosing a wrong target which led to mismatch between patients and drugs/CPOE screen, and insufficient confirmation which failed to detect and correct them. We identified three contributory factors for the occurrence of a mismatch between the drug/CPOE screen and the patient, which included situations where two patients/drugs were listed next to one another, where two patients’ last names/drugs’ names were the same, or where the patient/drug/CPOE screen in front of the staff involved was assumed to be correct. We will investigate IRs related to other types of wrong-patient errors and consider if this definition fits those errors, and investigate the contributory factors for them.
Funding
This research was only supported by research fund of our department which was distributed by Tokyo Medical University, without any external fund.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Bates DW, Boyle DL, Vander Vliet MBV, Schneider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10:199–205. doi:10.1007/BF02600255
2. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE prevention study group. JAMA. 1995;274:29–34. doi:10.1001/jama.274.1.29
3. Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med. 2003;348:1556–1564. doi:10.1056/NEJMsa020703
4. Leape LL, Bates DW, Cullen DJ, et al. System analysis of adverse drug events: ADE prevention study group. JAMA. 1995;274:35–43. doi:10.1001/jama.274.1.35
5. Bates DW, Leape LL, Cullen DJ, et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280:1311–1316. doi:10.1001/jama.280.15.1311
6. Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010;362:1698–1707. doi:10.1056/NEJMsa0907115
7. Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med. 1991;324:377–384. doi:10.1056/NEJM199102073240605
8. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285:2114–2120. doi:10.1001/jama.285.16.2114
9. World Health Organization collaborating Centre for Patient Safety Solutions. Patient identification; 2007. Available from: http://www.who.int/patientsafety/solution/patientsafety/PS-Solution2.pdf.
10. The Joint Commission for Accreditation of Health Care Organizations. Improving America’s hospitals, The Joint Commission’s annual report on quality and safety; 2007. Available from: http://www.jointcommission.org/assets/1/6/2007_Annual_Report.pdf.
11. Härkänen M, Tiainen M, Haatainen K. Wrong-patient incidents during medication administrations. J Clin Nurs. 2018;27:715–724. doi:10.1111/jocn.14021
12. Yang A, Grissinger M. Wrong-patient medication errors: an analysis of event reports in Pennsylvania and strategies for prevention. Pa Saf Advis. 2013;10(2):41–49.
13. Dougherty L, Sque M, Crouch R. Decision-making processes used by nurses during intravenous drug preparation and administration. J Adv Nurs. 2012;68(6):1302–1311. doi:10.1111/j.1365-2648.2011.05838.x
14. Härkänen M, Kervinen M, Ahonen J, et al. An observational study of how patients are identified before medication administrations in medical and surgical wards. Nurs Health Sci. 2015;17(2):188–194. doi:10.1111/nhs.12158
15. Shimada Y, Fujimoto M, Nogami T, et al. Patient safety incident reports related to traditional Japanese Kampo medicines: medication errors and adverse drug events in a university hospital for a ten-year period. BMC Compl Altern Med. 2017;17:547–554. doi:10.1186/s12906-017-2051-2
16. Nakajima K, Kurata Y, Takeda H. A web-based incident reporting system and multidisciplinary collaborative projects for patient safety in a Japanese hospital. Qual Saf Health Care. 2005;14:123–129. doi:10.1136/qshc.2003.008607
17. Japan Council for Quality Health Care. National database of medical adverse events. Available from: http://www.med-safe.jp.
18. National University Hospital Council of Japan. Guidelines for the public announcement of medical accidents at national university hospital; 2012. Available from: http://www.univ-hop.net/guide_cat_04_15.pdf.
19. Bates DW, Cohen M, Leape LL, et al. Reducing the frequency of errors in medicine using information technology. J Am Med Inform Assoc. 2001;8:299–308. doi:10.1136/jamia.2001.0080299
20. Kaushal R, Shojania KG, Bates DW. Effects of computerized physician order entry and clinical decision support systems on medication safety: a systematic review. Arch Intern Med. 2003;163:1409–1416. doi:10.1001/archinte.163.12.1409
21. Vincent C, Taylor-Adams S, Chapman EJ, et al. How to investigate and analyse clinical incidents: clinical risk unit and association of litigation and risk management protocol. BMJ. 2000;320:777–781. doi:10.1136/bmj.320.7237.777
22. Wright AA, Katz IT. Bar coding for patient safety. N Engl J Med. 2005;353:329–331. doi:10.1056/NEJMp058101
23. ECRI Institute. Patient identification errors; 2016. Available from: https://www.ecri.org/Resources/Patient_Identification_Evidence_Based_Literature_final.pdf.
24. Reason J. Human Error.
25. Reason J. Clinical Risk Management: Enhancing Patient Safety.
26. Leape LL. Error in medicine. JAMA. 1994;272(23):1851–1857. doi:10.1001/jama.1994.03520230061039
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.