Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Dermoscopic Response Predictors in Papulopustular Rosacea Treated with Topical Ivermectin and Metronidazole: A Prospective Observational Comparative Study
Authors Plozner N ![]() , Lai M, Figini M, Mehta N
, Lai M, Figini M, Mehta N ![]() , Szykut-Badaczewska A
, Szykut-Badaczewska A ![]() , Kyrgidis A, Stinco G, Errichetti E
, Kyrgidis A, Stinco G, Errichetti E
Received 1 January 2026
Accepted for publication 6 February 2026
Published 13 February 2026 Volume 2026:19 589715
DOI https://doi.org/10.2147/CCID.S589715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Noemi Plozner,1,* Michela Lai,1,* Matteo Figini,1 Nikhil Mehta,1 Agata Szykut-Badaczewska,2 Athanassios Kyrgidis,3 Giuseppe Stinco,1 Enzo Errichetti1
1Institute of Dermatology, Department of Medicine, University of Udine, Udine, Italy; 2Department of Dermatology and Venereology, State Hospital Klagenfurt, Klagenfurt am Wörthersee, Austria; 3Department of Oral and Maxillofacial Surgery, Aristotle University of Thessaloniki, Thessaloniki, Greece
*These authors contributed equally to this work
Correspondence: Enzo Errichetti, Institute of Dermatology, Department of Medicine, University of Udine, Udine, Italy, Email [email protected]
Background: Over recent years, dermoscopy has proven useful not only for diagnosing skin conditions but also as a tool for predicting treatment response in inflammatory dermatoses. However, no data are available on dermoscopic predictors in papulopustular rosacea (PPR).
Objective: To evaluate whether certain clinical and dermoscopic findings serve as positive or negative predictors of response to topical ivermectin or metronidazole in PPR.
Methods: Twenty-three patients with moderate-to-severe PPR were enrolled. Ten patients received ivermectin 10 mg/g cream and 13 received metronidazole 1% gel (non-randomized, based on physician preference), applied once daily for 8 weeks. Inflammatory lesion counts and key clinical/dermoscopic features were assessed at baseline and after 8 weeks by two independent, blinded physicians. Post-treatment clinical outcomes (optimal response: > 75% lesion reduction; partial response: 50– 75% reduction) were correlated with baseline features.
Results: Both treatments significantly reduced inflammatory lesion counts (p< 0.001 for both). Any response (optimal or partial) occurred in 7/10 (70%) ivermectin-treated and 8/13 (62%) metronidazole-treated patients. Optimal response occurred in 5/10 (50%) ivermectin-treated and 4/13 (31%) metronidazole-treated patients. In the ivermectin group, all patients who achieved optimal response had baseline protruding follicular plugs (PFPs) (5/5, 100%) in dermoscopy, which are indicators of demodex tails. Those with partial or minimal/no response in the ivermectin group did not have baseline PFPs (0/5). Baseline PFPs were significantly associated with optimal response to ivermectin (p=0.004). In the metronidazole group, all 4 optimal responders did not have baseline PFPs. All the 4 patients in the metronidazole group with baseline PFPs showed minimal/no response, though this was not statistically significant (p=0.176). No other baseline features significantly predicted response in either treatment group.
Conclusion: PFPs in dermoscopy of moderate-to-severe PPR serve as positive predictors for optimal response to topical ivermectin, but not metronidazole. This observation warrants validation in larger controlled trials.
Keywords: rosacea, papulopustular rosacea, dermoscopy, protruding follicular plugs, demodex, ivermectin, metronidazole
Introduction
Papulopustular rosacea (PPR) is a common variant of rosacea characterized by papules and pustules on an erythematotelangiectatic background, typically affecting the convex and central areas of the face (forehead, cheeks, nose, and periocular/perioral skin). Multiple treatments can help manage PPR, including both topical and systemic agents. Given their favorable safety profile and efficacy, topical therapies are often preferred first-line for moderate-to-severe PPR; among these, metronidazole and ivermectin are the most frequently prescribed.1,2 In clinical practice, however, choosing between such topical agents relies largely on physician experience, as no specific clinical factor has been identified to guide this decision.
Beyond its diagnostic applications, dermoscopy has recently shown promise in predicting and monitoring treatment responses in various inflammatory dermatoses by revealing microscopic features not visible to the naked eye. This approach can optimize patient management by reducing exposure to ineffective therapies. For example, dermoscopic clues have been linked to therapeutic outcomes in conditions like psoriasis and vitiligo.3–5 Nevertheless, no prior study has specifically addressed dermoscopic predictors of treatment response in rosacea, particularly PPR.
Recent evidence suggests that papulopustular rosacea may represent a heterogeneous condition with distinct pathophysiological subsets. One subset appears to be primarily driven by Demodex mite proliferation, characterized by follicular obstruction, mechanical irritation, and immune responses to mite antigens and associated bacteria such as Bacillus oleronius. This Demodex-associated variant typically demonstrates elevated mite densities (>5/cm2) and responds preferentially to acaricidal therapies. In contrast, a non-Demodex-associated subset may be predominantly inflammatory, driven by dysregulated innate immunity, abnormal cathelicidin processing, neurovascular hyperreactivity, and barrier dysfunction, with normal or minimally elevated Demodex counts. This subset may respond equally well to anti-inflammatory agents without specific acaricidal activity. Understanding which pathophysiological mechanism predominates in individual patients could enable more targeted, personalized treatment selection.6–9
Dermoscopic examination has proven valuable in identifying Demodex-related follicular disturbances in various facial dermatoses. Follicular hyperkeratosis, protruding follicular plugs (PFPs, also termed “Demodex tails”), and dilated follicular openings are characteristic dermoscopic features associated with Demodex mite overgrowth. PFPs likely represent keratotic debris and collections of mites within follicles protruding above the skin surface.10 These dermoscopic findings correlate with increased Demodex density on standardized skin surface biopsy and can serve as non-invasive markers of mite proliferation.
The aim of this prospective study was to identify clinical and dermoscopic features that could serve as positive or negative predictors of response in PPR patients treated with topical ivermectin or metronidazole. Ultimately, such predictors could assist clinicians in selecting the most appropriate therapy for individual patients.
Materials and Methods
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and the institutional ethical guidelines, with the required ethical approval. All participants provided informed consent for inclusion and for the use of clinical data and photographs, and the local ethics committee approved the study protocol.
Study Population
Consecutive consenting adult patients (age ≥18 years) presenting at the study center and clinically diagnosed by the investigator dermatologists with facial moderate-to-severe PPR (defined by ≥11 inflammatory papules/pustules) were prospectively enrolled during an 8-month period. Patients with other rosacea variants or phenotypes (erythematotelangiectatic without papulopustular lesions, phymatous, ocular, granulomatous, or steroid-induced), other facial dermatoses (eg, seborrheic dermatitis, demodicosis, atopic or contact dermatitis), or who were pregnant/breastfeeding were excluded. Patients who had used any rosacea treatments in the 12 weeks prior, or who were on medications that could affect rosacea like vasodilators and systemic antibiotics at the time of recruitment, were also excluded.
Interventions
Each patient received either topical metronidazole 1% gel or ivermectin 10 mg/g (1%) cream, applied once daily to affected areas for 8 weeks (in accordance with the Italian national drug agency guidelines for rosacea therapy).11 Investigator dermatologists were free to prescribe their own first-line treatment as per their choice. Treatment allocation was not randomized or blinded. No additional systemic or topical treatments were permitted during the study. Patients who did not follow up, required rescue treatment, or failed to complete the 8-week course were recorded separately, and excluded from the per protocol analysis.
Assessments
At baseline (week 0), each patient underwent independent clinical and dermoscopic evaluations by two experienced dermatologists (one assessing clinical lesions and another performing dermoscopy), each blinded to the other’s findings. Clinically, the number of inflammatory lesions (papules and pustules) was counted and baseline photographs were taken. Dermoscopic examination (performed with a DermLite DL3, 10× polarized) documented the presence or absence of predefined features based on literature and consensus criteria for inflammatory dermatoses.12,13 Examination was conducted on the central facial areas, specifically both cheeks, nose, and chin, where rosacea lesions were predominantly present. At least 2–3 representative areas on each cheek were examined, and images were captured for documentation. The dermoscopic variables assessed included: polygonal vessels, linear branched vessels, white/yellow scales, follicular dilation, protruding follicular plugs (PFPs), orange-yellow areas, pigmented structures, rosettes, and follicular red dots.
If a patient exhibited PFPs on dermoscopy, a direct microscopic examination was performed to evaluate Demodex mite density. Follicular material from a representative 1 cm2 facial area (with the highest concentration of PFPs) was scraped and treated with 20% KOH for microscopy and observed under 40–100x magnification. The Recommendations from the global ROSacea COnsensus panel (ROSCO) mention that demodicidosis/demodicosis should be excluded while considering inflammatory lesions of rosacea.14 While the way to exclude it has not been mentioned, it can be presumed that the Demodex density can be used for it.7 According to literature, a density greater than 5 Demodex folliculorum mites/cm2 are correlated with clinically overt manifestations.6 Any patients meeting this criterion (indicating primary Demodex overgrowth rather than rosacea) were excluded from the study to avoid confounding.
After 8 weeks of therapy (week 8), clinical and dermoscopic assessments were performed by the same dermatologists as the baseline assessment, and they were again blinded to either each other’s findings or patients’ treatment group. Clinical improvement was evaluated by recounting inflammatory lesions, and response categories were defined as: optimal response- greater than 75% reduction in lesion count from baseline; partial response- 50–75% reduction; minimal or no response- less than 50% reduction.
Statistical Analysis
All data were analyzed using Microsoft Excel 2013 and R software. Continuous data were summarized with means ± standard deviations (SD), and categorical data with percentages. Between-group comparisons (ivermectin vs metronidazole) for baseline characteristics used the z-test for continuous variables and chi-square or Fisher’s exact test for proportions, as appropriate. Clinical and dermoscopic findings were correlated with treatment outcomes. Associations between baseline predictors and treatment outcome were assessed using chi-square or Fisher’s exact tests. A two-tailed p < 0.05 was considered statistically significant. Additionally, odds ratios (OR) with 95% confidence intervals (CI) were calculated via univariate logistic regression for key associations. Spearman’s rank correlation (ρ) was used to assess the strength of correlation between the presence of specific dermoscopic features and the degree of clinical response.
Results
Patient Characteristics
A total of 35 patients were screened, out of which 12 were considered to have primary demodicidosis on the basis of having more than 5/cm2 density of Demodex mites, and were excluded. Data for the remaining 23 patients (16 females, 7 males) were analyzed. The mean age was 51.9 years (SD 16.2), with females averaging 43.8 (SD 10.8) and males 70.4 (SD 9.5) years. Ten patients (~43%) received topical ivermectin and 13 (~57%) received topical metronidazole. Baseline age and sex distribution did not differ significantly between the two treatment groups.
All patients had moderate-to-severe PPR by inclusion criteria (mean inflammatory lesion count 27.6, range 11–63). No severe adverse effects were reported during the 8-week treatment, and no patient discontinued therapy due to side effects.
Baseline Dermoscopic Features
These are compiled in Table 1. Certain dermoscopic findings were common across the cohort. Polygonal (geometric) vessel networks were present in all patients. Follicular keratotic features were frequently observed: white/yellow scales in 8 patients (35%), follicular hyperkeratosis in 20 patients (87%), and follicular ostia dilatation in 14 patients (61%). Branched linear vessels were noted in 6 patients (26%). Pigmented structures (eg, brown dots or globules) were seen in 14 patients (61%). Rosettes (four-dots shining white crosses under polarized light) were uncommon, seen in only 3 patients (13%). No patient showed orange-yellowish areas (a finding sometimes associated with sebaceous gland hyperplasia or granulomatous rosacea) or follicular red dots (usually a feature of active discoid lupus erythematosus). Notably, protruding follicular plugs (PFPs), the target feature of interest, were present in 9 patients (39%) at baseline. Among these, 5 were in the ivermectin group and 4 in the metronidazole group.
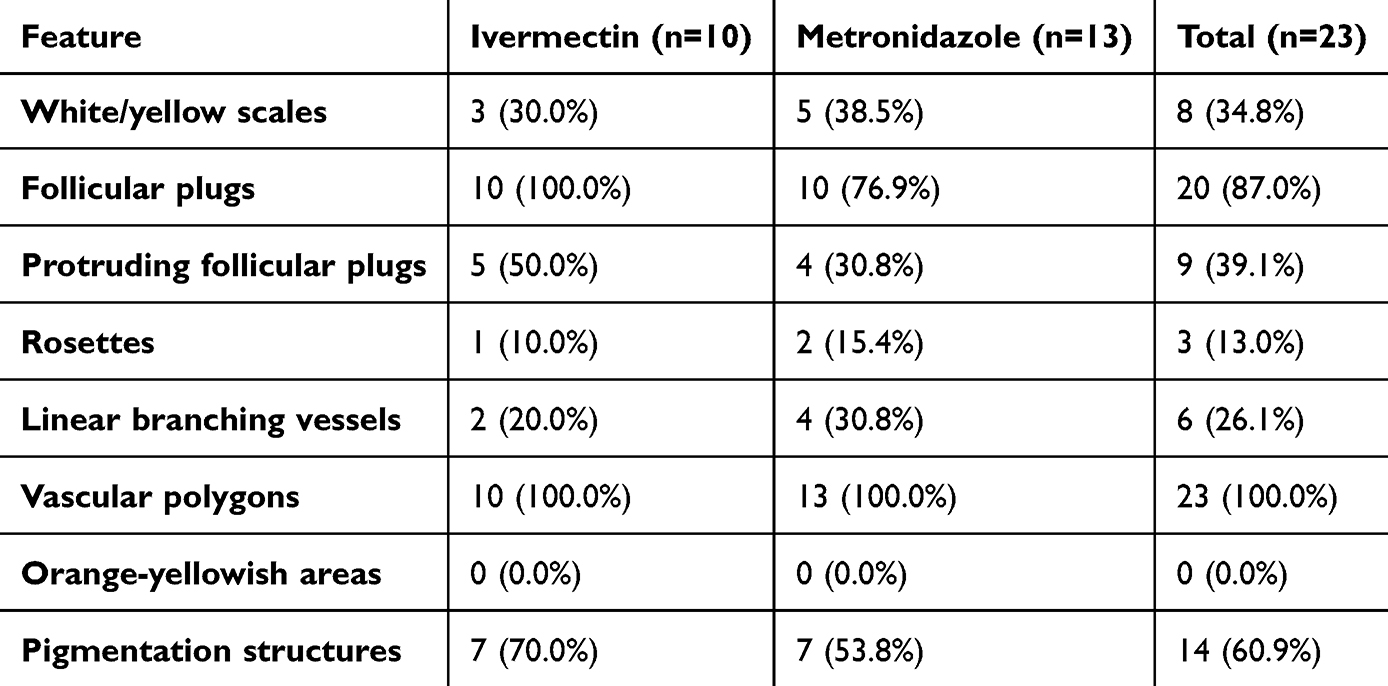 |
Table 1 Baseline Dermoscopic Features in Ivermectin and Metronidazole Groups |
Clinical Outcomes
Overall, lesion counts improved in both groups by week 8, though the magnitude varied. The overall combined reduction for all patients was from 27.6 to 16.0 (42% decrease). In the ivermectin arm, the mean papule/pustule count decreased from 31.0 (± 14.7) at baseline to 15.7 (± 12.9) at week 8 (average reduction of 49%). In the metronidazole arm, the mean count decreased from 24.9 (± 13.7) to 16.3 (± 14.0) (average reduction of 35%). While both treatments showed improvement, the ivermectin-treated patients had a greater average lesion reduction than those on metronidazole, though this difference was not statistically significant (p>0.05).
When categorized by response grade, 7/10 patients (70%) in the ivermectin group achieved at least a partial response, out of which 5/10 (50%) had an optimal response (>75% clearance) and 2/10 (20%) had a partial response. The remaining 3/10 (30%) ivermectin patients showed minimal or no improvement. In the metronidazole group, 8/13 (62%) patients had at least a partial improvement, out of which 4/13 (31%) patients attained an optimal response and 4/13 (31%) a partial response, while the rest 5/13 patients (39%) had minimal or no response. The distribution of responders vs non-responders was not significantly different between the two treatments, likely due to the sample size.
Sub-Group Analysis of Predictors of a Good Response
Clinical variables (age, gender, baseline lesion count, and choice of therapy overall as mentioned above) did not differ significantly in responders and non-responders. The baseline dermoscopy features were not significantly different in responders compared to non-responders, except for the presence of protruding follicular plugs (PFPs), which has been summarized in Table 2. In the ivermectin arm, 5 out of 10 patients (50%) had PFPs on initial dermoscopy. All 5 of these patients went on to achieve an optimal clinical response after 8 weeks, with complete resolution of their PFPs on follow-up dermoscopy. In contrast, none of the 5 ivermectin-treated patients who lacked PFPs at baseline achieved an optimal outcome: - 2 of those had only a partial response, and the remaining 3 had little to no improvement (p=0.004, Fisher’s exact test, Odds ratio cannot be computed, Spearman rank correlation coefficient of ρ = 1.0). In the metronidazole arm, 4/13 (31%) patients showed PFPs at baseline. Notably, none of these 4 patients responded optimally to metronidazole; in fact, they tended to have poor outcomes, and all 4 still displayed PFPs on dermoscopy after treatment. Of the 9 metronidazole patients without baseline PFPs, 8 (89%) achieved at least a partial improvement (including all 4 optimal responders in this arm), whereas only 1 patient without PFPs showed no significant response, but this did not reach statistical significance (p = 0.176), likely due to small sample size (Figure 1).
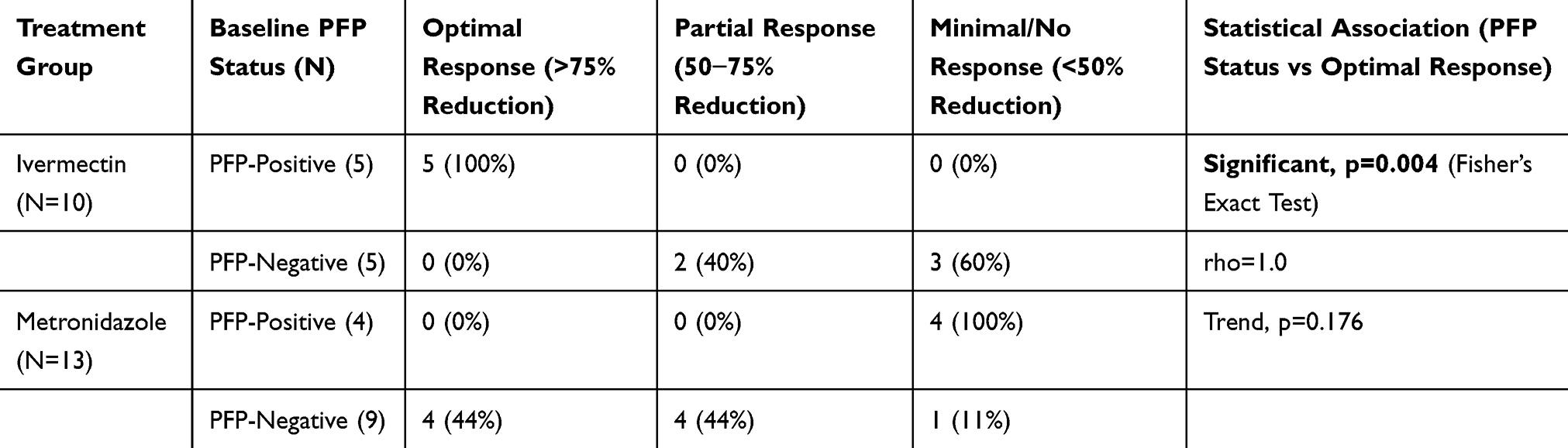 |
Table 2 Results of Response with Ivermectin 1% or Metronidazole Cream for 8 Weeks for Papulopustular Rosacea. PFP- Protruding Follicular Plugs |
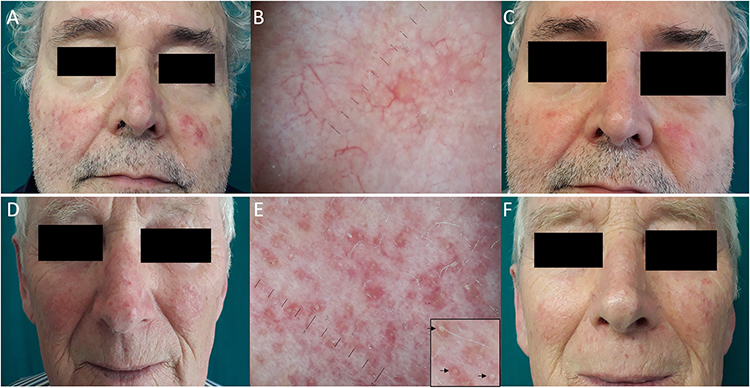 |
Figure 1 Dermoscopy and treatment outcomes in PPR. Upper row- response to metronidazole (A) Patient with papulopustular rosacea (B) Baseline polarized dermoscopy showing red linear branched vessels and polygons, some follicular plugs but without any protruding follicular plugs (PFPs). (C) Good response in inflammatory lesions with topical metronidazole for 8 weeks. Lower row- response to ivermectin (D) Patient with papulopustular rosacea (E) Baseline dermoscopy, showing several PFPs/demodex tails, as yellowish keratotic concretions emerging from follicular openings (highlighted in inset with black arrows). (F) Good response in inflammatory lesions with topical ivermectin for 8 weeks, along with disappearance of PFPs dermoscopically. (Dermoscopy images using DermLite DL3 at 10× magnification.). |
Discussion
This prospective study identifies PFPs as a novel dermoscopic predictor of therapeutic response in PPR. Our results demonstrate that PFPs at baseline herald a markedly better outcome with topical ivermectin, whereas their presence appears to portend a suboptimal response to topical metronidazole. To our knowledge, this is the first report of a dermoscopic feature predicting treatment response in rosacea.
The strong association between PFPs and ivermectin efficacy is biologically plausible. Ivermectin is an antiparasitic agent with known acaricidal action against Demodex folliculorum mites. By effectively reducing Demodex mites, ivermectin addresses one of the drivers of inflammation, apart from its anti-inflammatory effects. Indeed, in our ivermectin-treated patients, the complete remission of PFPs after therapy, denoting the clearance of mites, corresponded with excellent clinical improvement. This observation is in line with previous evidence that reduction of Demodex density correlates with rosacea improvement.15
In contrast, we found that PFP-positive patients responded poorly to metronidazole. Metronidazole’s mode of action in rosacea is thought to be primarily anti-inflammatory and possibly antibacterial, but it is not known to have significant acaricidal effects on Demodex. All baseline PFPs persisted in our metronidazole group, and notably, every patient with PFPs at baseline ended up as a non-responder to metronidazole. This trend, although not statistically significant in our small sample, suggests that PFPs might serve as a negative predictor for metronidazole therapy, likely because the underlying Demodex overpopulation remains unaddressed by that treatment.
Our data supports the possibility that there are at least two subsets of papulopustular rosacea with differing pathogenesis and treatment responses: one subset associated with Demodex overgrowth (PFP-positive), which responds optimally to acaricidal therapy (ivermectin), and another subset not primarily driven by Demodex (PFP-negative), which may respond adequately to non-acaricidal anti-inflammatories like metronidazole. In this sense, PFP-positive rosacea might be considered an endogenous Demodex-associated variant of rosacea. Some authors have argued that papulopustular rosacea with high Demodex density is essentially the same entity as Demodex dermatosis (demodicosis), and that what we call PPR could actually be viewed as rosacea-like demodicosis, and that pityriasis folliculorum (the subclinical Demodex infestation characterized by diffuse follicular scaling) may represent a precursor to rosacea in these cases.7,8 Demodicosis is diagnosed by demonstrating >5 mites/cm2 via skin surface biopsy. But this overgrowth can be seen in PPR too, and in similar high proportion of cases. In fact, this cut-off was first described for PPR cases by Forton, who has also repeatedly highlighted the view point that both demodicosis and PPR are manifestation of a same disease on a spectrum.6–8 But in order to adhere to ROSCO guidelines, we had excluded patients above this threshold. However, our findings support that even below that diagnostic cutoff, relative Demodex overabundance (detected dermoscopically as PFPs) is clinically relevant. Thus, for patients with dermoscopic evidence of Demodex proliferation (PFPs), it seems prudent to opt for ivermectin over metronidazole in order to directly target the mites. Conversely, in PFP-negative patients (where Demodex is less implicated), metronidazole or other anti-inflammatory agents could be equally effective. This hypothesis of PFP negative papulopustular rosacea, while biologically plausible, remains speculative based on our data and requires prospective validation in larger, controlled studies with comprehensive Demodex quantification in all patients regardless of PFP status.
Also, we demonstrate that dermoscopy can serve as a rapid painless and practical qualitative/semi-quantitative (albeit just for superficial demodex) substitute for the standard methods of demodex demonstration and quantification by collection through standardized skin surface biopsy using cyanoacrylate glue/tape stripping using cellophane tape/skin scraping and visualization under a microscope.
Our study also contributes to the broader understanding that dermoscopy can serve as a bedside tool for prognostication in inflammatory skin disease, complementing clinical examination. Analogous findings have been reported in other dermatoses, including psoriasis and vitiligo.3–5 Data on dermoscopic predictors in other conditions like seborrheic dermatitis or acne are still limited. However, it stands to reason that dermoscopy might help monitor features such as scaling patterns or vascular changes in seborrheic dermatitis, or the resolution of perifollicular inflammation in acne, thereby assisting in assessing treatment efficacy. Our findings in rosacea add to this emerging field of “theragnostic dermoscopy”, suggesting that incorporating dermoscopic evaluation into routine practice could enhance personalized treatment strategies for inflammatory skin disorders.
While our study relied on conventional dermoscopy and direct microscopy, reflectance confocal microscopy (RCM) represents a more advanced non-invasive technique for Demodex visualization and quantification in vivo. RCM enables real-time detection and counting of Demodex mites within follicles at the cellular level, without requiring skin sampling. Studies using RCM have demonstrated significantly higher Demodex densities in papulopustular rosacea patients compared to healthy controls, with mean counts of 1.77 mites/follicle in PPR versus 0.13 in controls. Furthermore, RCM has been successfully used to monitor Demodex reduction during ivermectin treatment, showing correlation between mite clearance and clinical improvement. Future studies incorporating RCM could provide more precise quantification of Demodex burden in both PFP-positive and PFP-negative patients, potentially strengthening the predictive value of baseline mite density for treatment selection.16–18 However, it is expensive, less commonly available, takes skill and time, while dermoscopy is an easy alternative non-invasive investigation.
Strengths and Limitations
Key strengths of our study include its prospective design and the blinded, paired evaluations of dermoscopic and clinical parameters, which reduce observer bias. By correlating dermoscopic findings with outcomes, we controlled for baseline disease severity and other confounders as much as possible in an observational setting. To the best of our knowledge, this is the first study to identify a dermoscopic predictor of therapy response in rosacea, filling a gap in the literature. On the other hand, our sample size was small (n=23), drawn from a single center, which limits statistical power and generalizability. Some potentially meaningful differences (eg, the trend in the metronidazole subgroup) may not have reached significance due to the low number of patients. The follow-up duration of 8 weeks, while sufficient to gauge initial treatment response, does not inform us about long-term outcomes or whether PFP status might predict relapse or sustained remission over time. Additionally, treatment allocation was not randomized, so prone to selection bias. Though baseline characteristics were similar between groups, an RCT design would provide stronger evidence for differential treatment efficacy. Another limitation is that we did not perform quantitative Demodex count/density for all patients (only those with evident PFPs were tested for demodicosis). It is possible that some PFP-negative patients had moderate Demodex involvement below the threshold of detection. The method for testing used was skin scraping, which is less sensitive and accurate than standardized skin surface biopsy using cyanoacrylate glue or tape stripping, and perhaps we could get these number of PPR cases with <5/cm2 mite density due to this. Future studies might incorporate standardized mite counts without any exclusion for >5/cm2 mite density for better characterization. Despite these limitations, our findings generate a testable hypothesis and have practical implications: dermoscopic examination is simple and non-invasive, and identifying PFPs could immediately influence therapeutic choice in PPR.
Conclusion
In summary, this study suggests that the dermoscopic finding of protruding follicular plugs (PFPs) in patients with papulopustular rosacea may serve as a positive predictor for a favorable response to topical ivermectin therapy. PFPs appear to indicate a Demodex-associated form of rosacea that particularly benefits from acaricidal treatment. In contrast, PPR patients lacking PFPs may respond equally well to non-acaricidal treatments such as metronidazole. These insights can be readily applied in clinical practice to improve patient stratification and optimize treatment selection, potentially decreasing the need for sequential trials of different topical agents and improving patient outcomes through earlier disease control, reducing time to effective treatment. Dermatologists managing rosacea should consider a quick dermoscopic evaluation for PFPs as part of the initial assessment. Given the limited sample size and scope of our study, further research is warranted to confirm these findings. Larger controlled studies, ideally randomized, and with longer follow-up, should be conducted to validate PFPs as a marker of Demodex-driven rosacea and to explore whether early intervention with ivermectin in PFP-positive patients leads to improved long-term outcomes in terms of less frequent relapses.
Data Sharing Statement
Data is available from corresponding author upon reasonable request.
Statement of Ethics
This study was approved by the ethics committee for the university of Udine, Udine, Italy, namely Comitato Etico Unico Regionale Friuli Venezia Giulia. The approval number is CEUR-2022-Os-199.
Patient Consent
Written informed consent was obtained from all patients for publication of their case details and photographs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nguyen C, Kuceki G, Birdsall M, et al. Rosacea: practical guidance and challenges for clinical management. Clin Cosmet Investig Dermatol. 2024;17:175–8. doi:10.2147/CCID.S391705
2. Lara Rivero A, Whitfeld M. An update on the treatment of rosacea. Aust Prescr. 2018;41:20–24. doi:10.18773/austprescr.2018.004
3. Lallas A, Argenziano G, Zalaudek I, et al. Dermoscopic hemorrhagic dots: an early predictor of response of psoriasis to biologic agents. Dermatol Pract Concept. 2016;6:7–12. doi:10.5826/dpc.0604a02
4. Omar SI, Hassan EM. Dermoscopy as a prognostic tool for the therapeutic response of phototherapy and methotrexate in psoriasis. J Egypt Women Dermatol Soc. 2020;17:164–174.
5. Errichetti E, Zelin E, Pinzani C, et al. Dermoscopic and clinical response predictor factors in nonsegmental vitiligo treated with narrowband ultraviolet b phototherapy: a prospective observational study. Dermatol Ther. 2020;10:1089–1098. doi:10.1007/s13555-020-00431-6
6. Forton F, Seys B. Density of demodex folliculorum in rosacea: a case-control study using standardized skin-surface biopsy. Br J Dermatol. 1993;128:650–659. doi:10.1111/j.1365-2133.1993.tb00261.x
7. Forton FMN. The pathogenic role of demodex mites in rosacea: a potential therapeutic target already in erythematotelangiectatic rosacea? Dermatol Ther. 2020;10:1229–1253. doi:10.1007/s13555-020-00458-9
8. Forton FMN. Rosacea, an infectious disease: why rosacea with papulopustules should be considered a demodicosis. A narrative review. J Eur Acad Dermatol Venereol. 2022;36:987–1002. doi:10.1111/jdv.18049
9. Jarmuda S, O’Reilly N, Żaba R, et al. Potential role of demodex mites and bacteria in the induction of rosacea. J Med Microbiol. 2012;61:1504–1510. doi:10.1099/jmm.0.048090-0
10. Segal R, Mimouni D, Feuerman H, et al. Dermoscopy as a diagnostic tool in demodicidosis. Int J Dermatol. 2010;49:1018–1023. doi:10.1111/j.1365-4632.2010.04495.x
11. Pini P. Rosacea: gli strumenti per conoscerla e gestirla.
12. Errichetti E, Zalaudek I, Kittler H, et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): an expert consensus on behalf of the international dermoscopy society. Br J Dermatol. 2020;182:454–467. doi:10.1111/bjd.18125
13. Stefanou E, Gkentsidi T, Spyridis I, et al. Dermoscopic spectrum of rosacea. JEADV Clin Pract. 2022;1:38–44. doi:10.1002/jvc2.6
14. Tan J, Almeida LMC, Bewley A, et al. Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176:431–438. doi:10.1111/bjd.15122
15. Trave I, Micalizzi C, Cozzani E, et al. Papulopustular rosacea treated with ivermectin 1% cream: remission of the demodex mite infestation over time and evaluation of clinical relapses. Dermatol Pract Concept. 2022;12:e2022201. doi:10.5826/dpc.1204a201
16. Sattler EC, Hoffmann VS, Ruzicka T, et al. Reflectance confocal microscopy for monitoring the density of demodex mites in patients with rosacea before and after treatment. Br J Dermatol. 2015;173:69–75. doi:10.1111/bjd.13783
17. Turgut Erdemir A, Gurel MS, Koku Aksu AE, et al. Demodex mites in acne rosacea: reflectance confocal microscopic study. Australas J Dermatol. 2017;58(30):e26. doi:10.1111/ajd.12452
18. Logger JGM, Peppelman M, van Erp PEJ, et al. Value of reflectance confocal microscopy for the monitoring of rosacea during treatment with topical ivermectin. J Dermatolog Treat. 2022;33:195–203. doi:10.1080/09546634.2020.1741501
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.