Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Dermatoscopic Features of Hyperpigmented Dermatoses
Authors Hua Y, Xie B ![]() , Shen Y, Song X
, Shen Y, Song X
Received 20 March 2026
Accepted for publication 21 May 2026
Published 2 June 2026 Volume 2026:19 609514
DOI https://doi.org/10.2147/CCID.S609514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
You Hua, Bo Xie, Yuqing Shen, Xiuzu Song
Department of Dermatology, Hangzhou Third People’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Xiuzu Song, Email [email protected]
Abstract: In recent years, dermatoscopy has emerged as a valuable adjunctive tool for the diagnosis of various cutaneous disorders. Initially developed for the evaluation of melanocytic lesions, this non-invasive technique has since demonstrated significant utility in the assessment of non-melanocytic hyperpigmented dermatoses. This review provides an up-to-date and practical overview of the dermatoscopic manifestations of common non-melanocytic hyperpigmented conditions, including melasma, nevus of Ota, freckles, lentigines, solar lentigines, seborrheic keratosis, porokeratosis, acquired dermal macular hyperpigmentation, lichen planus-like keratosis, pigmented actinic keratosis, pigmented Bowen’s disease, basal cell carcinoma, and acanthosis nigricans. Many of these hyperpigmented disorders exhibit distinct and characteristic dermatoscopic features. Given the clinical diagnostic challenges posed by these conditions and their significant psychological impact on patients, dermatoscopy offers a complementary approach to enhance the accuracy of evaluation and differential diagnosis.
Keywords: dermatoscopy, hyperpigmented dermatoses, melasma
Dermatoscopy is an established non-invasive diagnostic technique that was first introduced for the assessment of melanocytic neoplasms. Accumulating evidence from recent studies has validated its role in the differential diagnosis of hyperpigmented dermatoses.1 This review synthesizes the current knowledge on the dermatoscopic features of major non-melanocytic hyperpigmented dermatoses, aiming to provide clinicians with a practical reference to optimize the application of dermatoscopy in the clinical evaluation of such conditions.
Melasma
Melasma is a prevalent acquired hyperpigmented dermatosis, characterized by symmetric macules and patches predominantly distributed on the facial convexities, most commonly the malar eminences. It has a striking predilection for women, with a lower incidence in men. The classic dermatoscopic features of melasma include a pigmented pseudoreticular pattern, scattered brown or grey punctate pigmentation, and telangiectasia. Melasma is histopathologically classified into epidermal and dermal subtypes based on the predominant layer of melanin deposition. Epidermal melasma typically displays a well-defined light-to-dark brown pseudoreticular pigment network on dermatoscopy (Figure 1a).2,3 In contrast, dermal melasma is characterized by an irregular pigmented network, accompanied by amorphous pigmentation and perifollicular pigment aggregation in most cases (Figure 1b).4,5 However, in clinical practice, determining the depth of melanin deposition in melasma solely by dermatoscopy remains a considerable challenge. Telangiectasia is a common finding in telangiectatic melasma, and its presence is independent of the depth of melanin deposition in the epidermis or dermis.6
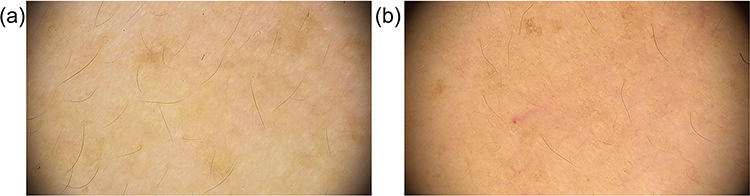 |
Figure 1 (a) Melasma (polarized ×30) (b) Melasma (polarized ×30). |
Nevus of Ota
Nevus of Ota is a rare congenital dermal melanocytosis, characterized by clonal proliferation of dermal melanocytes in the distribution area of the trigeminal nerve on the face.7 Dermatoscopically, nevus of Ota presents with a heterogeneous mixture of yellowish-brown, blue-grey, and taupe pigmentation, with a pathognomonic blue-grey perifollicular halo (Figure 2). Several studies have identified grey amorphous pigmented areas and scattered brown-grey punctate lesions as the specific dermatoscopic pattern of nevus of Ota,8 which corresponds histopathologically to the deposition of dendritic melanocytes and melanophages within the collagen bundles of the reticular dermis.
 |
Figure 2 Nevus of Ota (polarized ×20). |
Freckles, Lentigines and Solar Lentigines
Freckles and solar lentigines are common benign macular hyperpigmentations, predominantly affecting Caucasians and Asians, while lentigines represent a distinct entity with no direct association with sun exposure. Freckles are small, 1–2 mm light brown macules that first appear in early childhood (2–3 years of age), increase in number during puberty, and may partially fade with advancing age, with a strong correlation to cumulative sun exposure.9 In contrast, lentigines are larger lesions (ranging from millimeters to centimeters in diameter) with dark brown pigmentation and no association with ultraviolet exposure. Solar lentigines occur exclusively on sun-exposed sites and present as asymptomatic, flat, light-to-dark brown macules with well-demarcated borders on clinical examination.1
Dermatoscopically, freckles are characterized by light brown clumped pigmentation, a faint pseudoreticular pattern, and scattered brown punctate foci (Figure 3a). Lentigines typically display a uniform brown pseudoreticular network (Figure 3b). Solar lentigines feature an irregular but distinct “serpiginous” or “eroded” border, with a prominent pigmented grid and a characteristic “fingerprint” pattern being the hallmark dermatoscopic findings (Figure 3c).10
 |
Figure 3 (a) Freckles (polarized ×30) (b) Lentigines (polarized ×30) (c) Solar Lentigines (polarized ×20). |
Seborrheic Keratosis
Seborrheic keratosis is one of the most common benign epithelial neoplasms, with a high prevalence in the elderly population.10 While most typical lesions can be diagnosed on clinical grounds alone, atypical variants often mimic melanocytic tumors, making dermatoscopy a valuable adjunctive tool for clinical evaluation. The classic dermatoscopic features of seborrheic keratosis include a “gyriform” or “cerebriform” surface pattern, comedo-like openings, and milia-like cysts (Figure 4a)—among which milia-like cysts are more readily identified under non-polarized light dermatoscopy (Figure 4b).11 Regularly distributed hairpin-shaped blood vessels may also be observed in some lesions. Histopathologically, the gyriform surface pattern corresponds to epidermal papillomatous hyperplasia; comedo-like openings represent pseudohorn cysts communicating with the lesion surface; milia-like cysts are intraepidermal horn cysts; and hairpin vessels reflect dilated capillaries within the dermal papillae.12 Notably, hairpin-shaped blood vessels are not a specific dermatoscopic feature of seborrheic keratosis and may be seen in other cutaneous lesions.
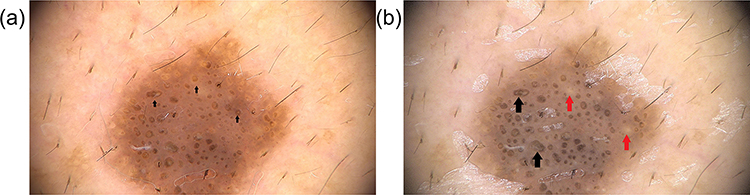 |
Figure 4 (a) Seborrheic Keratosis (polarized ×30) Black arrow: Comedone-like opening. (b) Seborrheic Keratosis (non-polarized ×30) Black arrow: Comedone-like openings. Red arrow: Milia-like cysts. |
Porokeratosis
Porokeratosis is a group of rare, genetically heterogeneous keratinization disorders of unknown etiology, characterized by diverse clinical manifestations and a pathognomonic histopathological finding of a cornoid lamella. It is broadly classified into focal and generalized variants based on the extent of cutaneous involvement. Common focal variants include classic Mibelli’s porokeratosis, linear porokeratosis, punctate porokeratosis, facial porokeratosis, and genital porokeratosis. Generalized variants comprise disseminated superficial porokeratosis, disseminated superficial actinic porokeratosis, and disseminated palmoplantar porokeratosis. Less common variants include hyperkeratotic porokeratosis, eruptive pruritic papular porokeratosis, verrucous porokeratosis (limited to the buttocks), and reticulated porokeratosis.13 Although not all variants present with hyperpigmentation, the dermatoscopic features are relatively consistent across different subtypes of porokeratosis. A well-defined keratinous border is the most specific dermatoscopic feature, present in the majority of lesions. Additional supportive dermatoscopic findings include pigmentation or erosion along the keratinous border, vascular structures, as well as scaling, punctate pigmentation, or shiny white structures within the border.14 Hyperpigmented porokeratosis typically exhibits a keratinous border with associated intra-border brown punctate pigmentation and confluent pigmentation (Figure 5a), while non-hyperpigmented variants are more likely to show erosion along the keratinous border and prominent vascular structures within and along the border (Figure 5b).
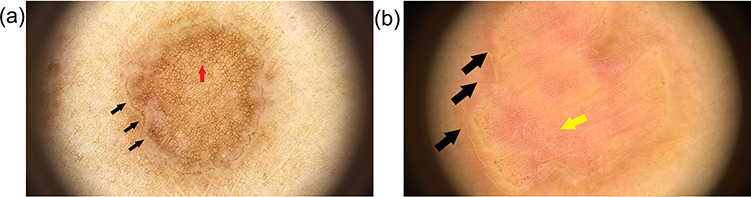 |
Figure 5 (a) Porokeratosis (polarized ×20) Black arrow: Keratin rim. Red arrow: Reticular pigmentation. (b) Porokeratosis (polarized ×20) Black arrow: Keratin rim. Yellow arrow: Vascular structure. |
Lichen Planus-Like Keratosis
Lichen planus-like keratosis (LPLK) is a benign inflammatory cutaneous lesion, clinically presenting as a solitary pink, erythematous, or grey macule, plaque, or papule, most commonly located on the face, upper extremities, or upper chest, with lesion diameters ranging from 5 to 20 mm. Most LPLK lesions coexist with other benign sun-induced skin changes, such as seborrheic keratosis or solar lentigines. The pathogenesis of LPLK remains elusive, with several hypotheses proposing that it represents an intermediate inflammatory stage in the spontaneous regression of seborrheic keratosis or solar lentigines.15
Characteristic dermatoscopic features of LPLK include a light brown pseudoreticular pattern, ill-defined pink erythematous areas, a grey pseudoreticular pattern, annular granular structures, and fine scattered blue-grey dots (Figure 6). The initial dermatoscopic findings of LPLK are thought to consist of a residual light brown pseudoreticular pattern from underlying solar lentigines, overlaid with pink erythematous areas secondary to lichenoid inflammatory infiltrate.16 Annular granular structures and a grey pseudoreticular pattern are considered hallmark features of the regressive stage, which further evolve into fine blue-grey dots in the late regressive phase.16 There is a strong correlation between the clinical, histopathological, and dermatoscopic features of LPLK, which is now recognized as a spectrum of sun-induced cutaneous lesions undergoing inflammatory regression, with distinct dermatoscopic patterns corresponding to different stages of resolution.17
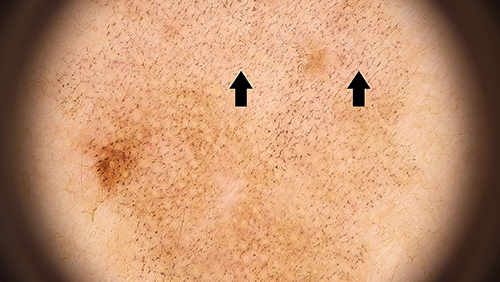 |
Figure 6 Lichen planus-like keratosis (polarized ×20) Black arrow: Blue-gray dots. |
Acquired Dermal Macular Hyperpigmentation
Acquired dermal macular hyperpigmentation is a newly unified diagnostic term in the field of hyperpigmented dermatoses, encompassing a group of previously distinct entities including Riehl’s melanosis, pigmented contact dermatitis, pigmented lichen planus, and ashy dermatosis—with Riehl’s melanosis now recognized as a subtype of pigmented contact dermatitis. These disorders are characterized by progressive dermal hyperpigmentation, predominantly affecting the face, neck, and trunk, and often cause significant cosmetic disfigurement and psychological distress in patients.1
Riehl’s melanosis, pigmented lichen planus, and ashy dermatosis exhibit overlapping dermatoscopic features, with the consistent findings including a pseudoreticular pigment pattern, scattered blue or grey punctate pigmentation, and telangiectasia across all three conditions (Figure 7a–c).1 The severity of the disease is correlated with the density of blue/grey punctate pigmentation and the degree of irregularity of the pseudoreticular pattern.18 In addition, prominent or faint Wickham’s striae may be observed in cases of pigmented lichen planus (Figure 7b), serving as a key dermatoscopic clue for differential diagnosis.
 |
Figure 7 Acquired Dermal Macular Hyperpigmentation. (a) Riehl’s melanosis (polarized ×30) Black arrow: Blue-gray dots. (b) lichen planus pigmentosus (polarized ×30) Black arrow: Blue-gray dots. Red arrow: wickham pattern. (c) Ashy dermatosis (polarized ×20) Black arrow: Blue-gray dots. |
Pigmented Actinic Keratosis
Actinic keratosis (AK) is the most common precancerous cutaneous lesion, predominantly affecting elderly and fair-skinned individuals, with lesions strictly limited to chronic sun-exposed areas. Dermatoscopy has become an irreplaceable tool in the diagnosis and evaluation of AK, with high sensitivity and specificity for distinguishing AK from other benign and malignant cutaneous lesions.19 Clinically, AK is divided into pigmented and non-pigmented subtypes, each with distinct dermatoscopic features. Non-pigmented AK is characterized by the pathognomonic “strawberry sign”—a red pseudoreticular pattern formed by background erythema and targetoid follicular orifices on dermatoscopy.20 In contrast, pigmented AK displays a pigmented pseudoreticular pattern composed of targetoid follicular orifices surrounded by confluent brown pigmentation (Figure 8), which may be associated with a superimposed red pseudoreticular pattern in some cases.21,22
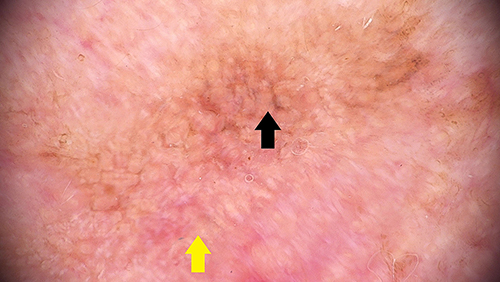 |
Figure 8 Pigmented actinic keratosis (polarized ×30) Black arrow: Pigmented pseudonetwork. Yellow arrow: Red pseudo-network. |
Another characteristic dermatoscopic feature of AK is the “rose sign”, a four-leaf clover-like structure formed by four clustered white punctate foci corresponding to follicular infundibula. Histopathologically, the rose sign is attributed to alternating hyperkeratosis and parakeratosis in the follicular infundibulum, accompanied by perifollicular fibrosis and inflammatory infiltrate.21,23
Pigmented Bowen’s Disease
Bowen’s disease, or squamous cell carcinoma in situ, is a malignant cutaneous neoplasm involving the full thickness of the epidermis without dermal invasion. The non-pigmented subtype is the most common form, predominantly occurring on sun-exposed sites including the head, neck, and extremities, and presenting as a solitary, well-demarcated erythematous scaly plaque on clinical examination.24 The pigmented subtype is rare, accounting for only 1.7% of all Bowen’s disease cases,25 and typically affects non-sun-exposed areas in patients with darker skin types, clinically manifesting as a hyperpigmented scaly plaque with ill-defined borders.
Dermatoscopically, pigmented Bowen’s disease is characterized by regularly arranged brown punctate pigmentation with patchy distribution and homogeneous brown to grey amorphous pigmentation (Figure 9).1 In contrast, non-pigmented Bowen’s disease features pathognomonic glomerular vessels, which are the key diagnostic clue.26 A recent dermatoscopic classification system for Bowen’s disease categorizes lesions into three subtypes: classic non-pigmented, partially pigmented, and fully pigmented. Partially pigmented Bowen’s disease is defined as lesions with less than 50% pigmented structures, and is the second most common subtype (accounting for 35% of cases) following the classic non-pigmented form. The most frequently detected dermatoscopic features in partially pigmented Bowen’s disease include surface scaling, glomerular vessels, amorphous pigmentation, and grey dots or globules, with additional findings including pinkish-white amorphous areas and punctate vessels. The dermatoscopic pattern of partially pigmented Bowen’s disease represents a combination of the features seen in both non-pigmented and fully pigmented subtypes.27
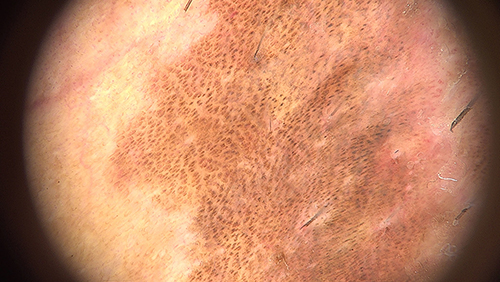 |
Figure 9 Pigmented Bowen’s disease (polarized ×20). |
Basal Cell Carcinoma
Dermatoscopy has been well validated to significantly improve the diagnostic accuracy of basal cell carcinoma (BCC),28 with a pooled sensitivity and specificity exceeding 90% for distinguishing BCC from other cutaneous neoplasms. One of the most recent and clinically relevant applications of dermatoscopy in BCC is the prediction of histopathological subtypes, particularly for distinguishing superficial BCC from non-superficial (nodular, infiltrative) subtypes. Additionally, dermatoscopy can help identify aggressive BCC variants with a high risk of recurrence, facilitating early intervention and optimized treatment planning. Thorough dermatoscopic examination during follow-up of high-risk patients (eg, those with chronic actinic damage or a history of multiple BCCs) is crucial for detecting early and subtle lesions, which significantly impacts treatment outcomes and long-term prognosis.28
Pigmented BCC exhibits distinct dermatoscopic pigmented structures, with blue-grey ovoid nests being the largest and most characteristic (Figure 10a)—these are aggregated ovoid or elongated pigmented foci that histopathologically correspond to large tumor nests in the dermis.29 Blue-grey globules are smaller, scattered round or elliptical pigmented structures, representing small dermal tumor nests on histopathology.29,30 Blue-grey dots are well-circumscribed, sharply focused, randomly scattered punctate pigmentation, corresponding to small tumor aggregates at the dermoepidermal junction or in the superficial dermis, or less commonly, free melanin or melanophages at the dermoepidermal junction.30 The maple leaf sign, spoke-wheel sign, and concentric sign are additional characteristic pigmented patterns of BCC (Figure 10b), all of which histopathologically correspond to tumor nests at the dermoepidermal junction and in the superficial dermis.30 Arborizing telangiectasia is the most prominent and common vascular structure in BCC (detected in 94% of cases), which histopathologically reflects dilated neovascularization within the dermal tumor stroma.29,30
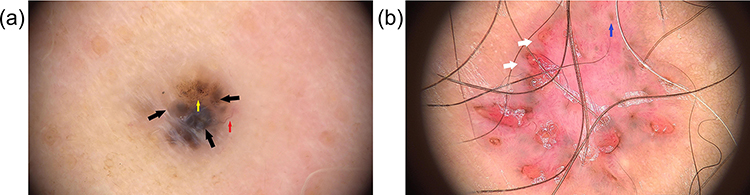 |
Figure 10 (a) Basal cell carcinoma (polarized ×30) Black arrow: Blue-gray oval nest. Yellow arrow: Blue-gray dots. Red arrow: Dendritic vessels. (b) Basal cell carcinoma (polarized ×20) White arrow: Spoke structures. Blue arrow: concentric structures. |
Acanthosis Nigricans
Acanthosis nigricans is a chronic hyperpigmented and hyperkeratotic dermatosis, characterized by velvety thickening and darkening of the skin, predominantly affecting intertriginous areas including the neck, axillae, inguinal folds, popliteal fossae, cubital fossae, and other flexural sites.31 It is often associated with underlying systemic conditions, including insulin resistance, obesity, and malignant neoplasms, making its early recognition clinically important.
The classic dermatoscopic findings of acanthosis nigricans include prominent skin ridges and furrows, papillary projections, scattered pigmented dots, crypts, and mottled pigmentation (Figure 11);32 some studies have also described a characteristic “cerebral sulcus appearance” due to the deepened and irregular skin furrows.33 Skin ridges and furrows are universal findings in all acanthosis nigricans lesions, with the corresponding histopathological features of marked hyperkeratosis and papillomatous hyperplasia—these changes lead to the invagination of skin ridges and formation of crypts, which are the basis of the characteristic dermatoscopic pattern.32 Importantly, the clinical severity of acanthosis nigricans shows a direct correlation with the degree of prominence of skin ridges and furrows on dermatoscopy, as well as the severity of papillomatous hyperplasia and hyperkeratosis on histopathological examination.32
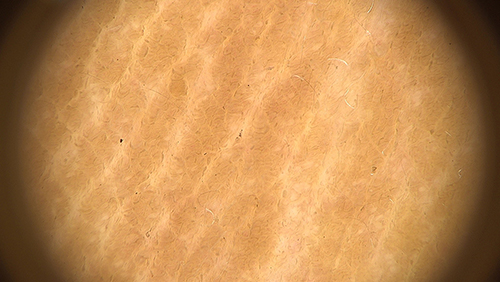 |
Figure 11 Acanthosis nigricans (polarized ×20). |
Discussion
Dermatoscopy, as a non-invasive diagnostic technique, has undergone remarkable development in the field of dermatology over the past few decades. Initially established as a gold-standard auxiliary tool for the diagnosis and differential diagnosis of melanocytic neoplasms, its application scope has been continuously expanded with in-depth research, and it now plays an increasingly important role in the evaluation of non-melanocytic hyperpigmented dermatoses. This review systematically summarizes the characteristic dermatoscopic manifestations of common non-melanocytic hyperpigmented dermatoses, and the core value of dermatoscopy in this field lies in its ability to identify subtle morphological features invisible to the naked eye, thereby bridging the gap between clinical macroscopic observation and histopathological microscopic findings.
The core findings of this review highlight that most non-melanocytic hyperpigmented dermatoses exhibit distinct and recognizable dermatoscopic features (Table 1), which can be used to facilitate differential diagnosis and disease evaluation. Specifically, melasma is characterized by a pigmented pseudoreticular pattern and telangiectasia, with epidermal and dermal subtypes showing subtle differences in pigment network regularity;3,5 nevus of Ota presents with heterogeneous yellowish-brown to blue-grey pigmentation and a pathognomonic blue-grey perifollicular halo;8 solar lentigines are distinguished by an “eroded” border and “fingerprint” pattern;10 seborrheic keratosis is marked by gyriform surface patterns, comedo-like openings, and milia-like cysts;11 porokeratosis is defined by a specific keratinous border;14 lichen planus-like keratosis (LPLK) shows dynamic dermatoscopic changes corresponding to its inflammatory regression stages;17 acquired dermal macular hyperpigmentation is dominated by blue/grey punctate pigmentation and a pseudoreticular pattern;18 pigmented actinic keratosis features a pigmented pseudoreticulum and the characteristic “rose sign”;21,22 pigmented Bowen’s disease presents with regularly arranged brown punctate pigmentation and glomerular vessels;1 pigmented basal cell carcinoma (BCC) is identified by blue-grey ovoid nests, blue-grey globules, and arborizing telangiectasia;28 and acanthosis nigricans is characterized by prominent skin ridges, furrows, and a “cerebral sulcus appearance”32 Additionally, a consistent histopathological correlation was observed for most dermatoscopic features, where each characteristic structure corresponds to specific pathological changes (eg, gyriform pattern of seborrheic keratosis corresponding to epidermal papillomatous hyperplasia, keratinous border of porokeratosis corresponding to cornoid lamella), providing a theoretical basis for the clinical application of dermatoscopy.
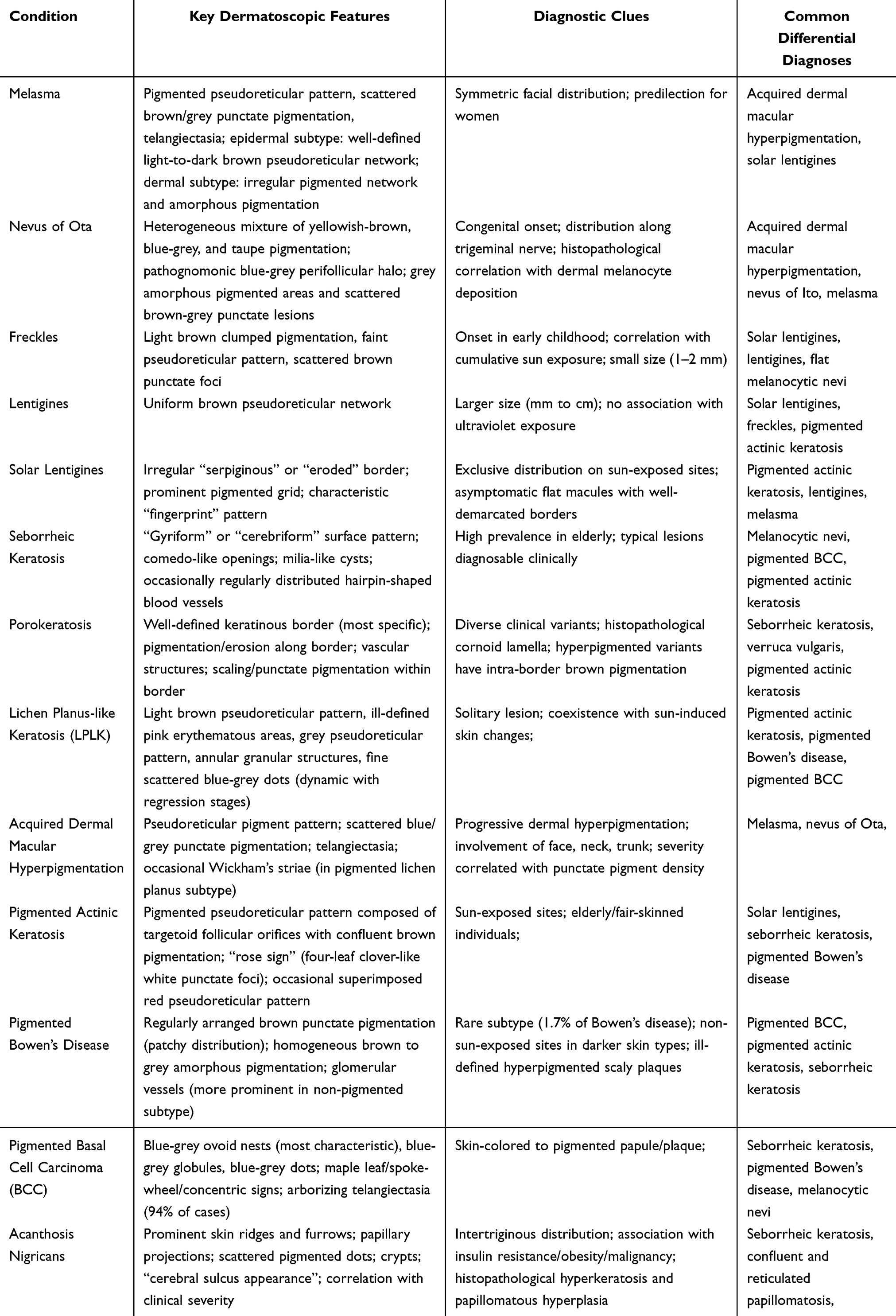 |
Table 1 Non-Melanocytic Hyperpigmented Dermatoses and Their Dermatoscopic Features |
Dermatoscopy has revolutionized the clinical management of hyperpigmented dermatoses by addressing key challenges in diagnosis, treatment selection, efficacy monitoring, and prognosis assessment, thereby optimizing patient outcomes. In terms of diagnosis, dermatoscopy reduces the rate of misdiagnosis and missed diagnosis by distinguishing between clinically overlapping conditions. For example, solar lentigines (benign) can be reliably differentiated from pigmented actinic keratosis (precancerous) using dermatoscopic features (fingerprint pattern vs targetoid follicular orifices and rose sign), preventing unnecessary invasive biopsies for benign lesions and avoiding delayed treatment for precancerous ones.10,21 Dermatoscopy guides treatment selection by providing insights into disease pathophysiology—for instance, the distinction between epidermal and dermal melasma (though limited) helps clinicians choose appropriate depigmentation therapies (eg, topical agents targeting epidermal melanin vs more invasive approaches for dermal melanin).3,5 It serves as an objective tool for monitoring treatment response: for melasma and acquired dermal macular hyperpigmentation, reductions in the density of blue/grey punctate pigmentation and the irregularity of the pseudoreticular pattern indicate therapeutic efficacy, allowing for timely adjustment of treatment regimens. In the follow-up of precancerous and malignant hyperpigmented lesions (eg, pigmented actinic keratosis, pigmented Bowen’s disease, BCC), dermatoscopy detects subtle changes (eg, new vascular structures, increased pigmentation) at an early stage, enabling prompt intervention and reducing recurrence rates. Dermatoscopy enhances patient counseling by providing visual evidence of lesion nature, reducing anxiety associated with uncertain diagnoses and improving treatment adherence.
Despite its significant clinical value, the application of dermatoscopy in hyperpigmented dermatoses is associated with several limitations that must be acknowledged. There is a notable overlap of dermatoscopic features among certain hyperpigmented disorders, which can complicate differential diagnosis. For example, both melasma and acquired dermal macular hyperpigmentation exhibit a pseudoreticular pattern and telangiectasia, making it difficult to distinguish them solely by dermatoscopy without combining clinical information (eg, disease onset, distribution, and associated symptoms). Distinguishing between epidermal and dermal melanin deposition remains a major challenge, even with dermatoscopy. While epidermal melasma typically shows a more defined pigmented pseudoreticular network and dermal melasma shows more amorphous pigmentation, these differences are not always definitive, leading to uncertainty in treatment selection. Histopathological confirmation is still necessary in ambiguous cases, particularly for lesions with atypical dermatoscopic features or those suspected of being malignant. Dermatoscopy is an auxiliary tool, not a substitute for histopathology—the gold standard for diagnosing cutaneous lesions— and overreliance on dermatoscopy alone may lead to misdiagnosis of malignant lesions such as pigmented BCC or Bowen’s disease. Additionally, the interpretation of dermatoscopic features is highly dependent on the clinician’s experience and skill level, leading to interobserver variability, especially for subtle or atypical structures. Most current research on dermatoscopic features is based on small sample sizes and retrospective studies, lacking large-scale, multicenter prospective data to validate the sensitivity and specificity of these features, particularly for rare hyperpigmented dermatoses.
Dermatoscopy is not the only non-invasive tool used in the evaluation of hyperpigmented dermatoses, and its advantages and limitations can be better understood by comparing it with other commonly used techniques, such as Wood’s lamp and reflectance confocal microscopy (RCM). Wood’s lamp, a UV light-based tool, is simple, low-cost, and widely available, and it is primarily used to distinguish between epidermal and dermal melanin (epidermal melanin fluoresces bright brown, while dermal melanin does not fluoresce).34,35 However, Wood’s lamp has limited resolution and cannot identify subtle structural features (eg, vascular patterns, pigment distribution), making it less useful for differential diagnosis of overlapping conditions. In contrast, dermatoscopy provides higher magnification and better visualization of surface and subsurface structures (eg, pigment networks, vessels, cysts), making it superior for distinguishing between benign and malignant lesions and for detailed disease evaluation. Reflectance confocal microscopy (RCM) is a more advanced non-invasive technique that provides real-time, high-resolution images of the epidermis and superficial dermis, allowing for visualization of individual cells (eg, melanocytes, keratinocytes) and subcellular structures.36 RCM is particularly useful for evaluating the depth of melanin deposition and distinguishing between benign and malignant lesions with high accuracy, but it is more expensive, time-consuming, and requires specialized training, limiting its availability in primary care settings. In summary, Wood’s lamp is suitable for initial screening and basic differentiation of melanin depth, dermatoscopy is ideal for routine differential diagnosis and disease monitoring due to its balance of accessibility and diagnostic value, and RCM is reserved for complex or ambiguous cases where higher resolution is needed.
The future of dermatoscopy in the evaluation of hyperpigmented dermatoses lies in the integration of advanced technologies to overcome current limitations and enhance its diagnostic and prognostic value. Two key directions are particularly promising: AI-assisted diagnosis and integration with total body photography. AI-assisted dermatoscopic diagnosis systems, trained on large-scale datasets of dermatoscopic images, have the potential to automatically identify and analyze characteristic features of hyperpigmented dermatoses, reducing interobserver variability and improving diagnostic efficiency. These systems can assist clinicians—especially those in primary care or areas with limited dermatological resources—in making accurate initial diagnoses, particularly for subtle or atypical lesions. Future research should focus on expanding training datasets to include diverse skin types and rare hyperpigmented dermatoses, improving the accuracy of AI algorithms for complex cases. Additionally, the integration of dermatoscopy with total body photography (TBP) is expected to enhance long-term monitoring and early detection of hyperpigmented lesions, particularly in high-risk populations (eg, individuals with chronic actinic damage, a history of skin cancer). TBP allows for systematic documentation of the entire skin surface, and when combined with dermatoscopy, it enables precise tracking of lesion changes (eg, size, pigmentation, vascular patterns) over time, facilitating early detection of malignant transformation or recurrence. Other future directions include the development of portable, handheld dermatoscopic devices for point-of-care diagnosis, the integration of dermatoscopy with other imaging modalities (eg, RCM, optical coherence tomography), and the establishment of standardized diagnostic criteria and training programs to reduce interobserver variability. Collectively, these advancements will further expand the role of dermatoscopy in the management of hyperpigmented dermatoses, moving toward more personalized, accurate, and accessible care.
In clinical practice, the application of dermatoscopy in hyperpigmented dermatoses should adhere to the principle of combining clinical features and dermatoscopic findings. Dermatoscopy is an auxiliary diagnostic tool rather than a substitute for clinical judgment. For hyperpigmented lesions with typical clinical and dermatoscopic features, a definite diagnosis can be made through non-invasive examination; for lesions with atypical manifestations or overlapping dermatoscopic features, histopathological examination is still the gold standard for diagnosis to avoid misdiagnosis of malignant lesions such as pigmented BCC and Bowen’s disease. In addition, clinicians should master the histopathological correlations of dermatoscopic features and combine the patient’s clinical information (eg, age, gender, lesion location, medical history) to make a comprehensive diagnosis, which is the key to improving the clinical application value of dermatoscopy.
In conclusion, dermatoscopy has become an indispensable auxiliary tool in the diagnosis and management of non-melanocytic hyperpigmented dermatoses, with unique advantages in differential diagnosis, disease severity evaluation and treatment follow-up. Its characteristic findings provide a visual and non-invasive approach for clinicians to understand the nature and progression of hyperpigmented lesions. Although there are still limitations such as the lack of standardized diagnostic criteria, overlapping features, and the influence of operator experience, the continuous improvement of research methods and the development of digital, AI, and imaging technologies will effectively solve these problems and further expand the application scope of dermatoscopy in this field. For clinical practice, standardized training of dermatoscopic diagnosis, the establishment of multicenter research databases and the rational combination of clinical and dermatoscopic findings are the key to maximizing the diagnostic value of dermatoscopy, which will help improve the diagnostic accuracy of hyperpigmented dermatoses, optimize treatment strategies and ultimately improve the clinical outcomes of patients.
Acknowledgment
All images were provided by You Hua and sourced from Department of Dermatology, Hangzhou Third People’s Hospital.
Funding
This manuscript was funded by Hangzhou Biomedicine and Health Industry Development Supporting Science and Technology Special Project (2023WJC306).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Krueger L, Saizan A, Stein JA, et al. Dermoscopy of acquired pigmentary disorders: a comprehensive review. Int J Dermatol. 2022;61(1):7–12. doi:10.1111/ijd.15741
2. Chatterjee M, Neema S. Dermoscopy of pigmentary disorders in brown skin. Dermatol Clin. 2018;36(4):473–485. doi:10.1016/j.det.2018.05.014
3. Yalamanchili R, Shastry V, Betkerur J. Clinico-epidemiological study and quality of life assessment in melasma. Indian J Dermatol. 2015;60(5):519. doi:10.4103/0019-5154.164415
4. Agamia N, Apalla Z, Salem W, et al. A comparative study between oral tranexamic acid versus oral tranexamic acid and Q-switched Nd-YAG laser in melasma treatment: a clinical and dermoscopic evaluation. J Dermatolog Treat. 2021;32(7):819–826. doi:10.1080/09546634.2019.1708847
5. Navya A, Pai V. Comparison of dermoscope and woods lamp as a tool to study melanin depth in melasma. Indian Dermatol Online J. 2022;13(3):366–369. doi:10.4103/idoj.idoj_245_21
6. Punchihewa N, Rodrigues M. A comprehensive review of dermoscopy in melasma. Clin Exp Dermatol. 2024;49(9):956–960. doi:10.1093/ced/llad266
7. Zhao W, Yang Y, Shi H, et al. Picosecond alexandrite laser treatment of nevus of Ota in children. Lasers Surg Med. 2024;56(5):437–445. doi:10.1002/lsm.23795
8. Elmas ÖF, Kilitçi A. Dermoscopic Findings of Nevus of Ota. Balkan Med J. 2020;37(2):116–118. doi:10.4274/balkanmedj.galenos.2019.2019.11.46
9. Praetorius C, Sturm RA, Steingrimsson E. Sun-induced freckling: ephelides and solar lentigines. Pigm Cell Melanoma Res. 2014;27(3):339–350. doi:10.1111/pcmr.12232
10. Elgart GW. Seborrheic keratoses, solar lentigines, and lichenoid keratoses. Dermatoscopic features and correlation to histology and clinical signs. Dermatol Clin. 2001;19(2):347–357. doi:10.1016/S0733-8635(05)70272-2
11. García-Rayo MC, Avilés-Izquierdo JA, García-Piqueras P, et al. Clues on dermoscopy. Seborrheic keratoses: when the good ones look bad. Eur J Dermatol. 2022;32(6):814–815. doi:10.1684/ejd.2022.4385
12. Minagawa A. Dermoscopy-pathology relationship in seborrheic keratosis. J Dermatol. 2017;44(5):518–524. doi:10.1111/1346-8138.13657
13. Sankar PA, Khare S, Ganguly S. Ultraviolet-induced fluorescence dermoscopy of porokeratosis. Indian Dermatol Online J. 2025;16(4):700–701. doi:10.4103/idoj.idoj_20_25
14. Zaar O, Polesie S, Navarrete-Dechent C, et al. Dermoscopy of porokeratosis: results from a multicentre study of the International Dermoscopy Society. J Eur Acad Dermatol Venereol. 2021;35(10):2091–2096. doi:10.1111/jdv.17439
15. Pogorzelska-Antkowiak A. Lichen planus-like keratosis: what do we know about it? Clin Exp Dermatol. 2022;47(11):1923–1927. doi:10.1111/ced.15318
16. Watanabe S, Sawada M, Dekio I, et al. Chronology of lichen planus-like keratosis features by dermoscopy: a summary of 17 cases. Dermatol Pract Concept. 2016;6(2):29–35. doi:10.5826/dpc.0602a06
17. Bugatti L, Filosa G. Dermoscopy of lichen planus-like keratosis: a model of inflammatory regression. J Eur Acad Dermatol Venereol. 2007;21(10):1392–1397. doi:10.1111/j.1468-3083.2007.02296.x
18. Vinay K, Bishnoi A, Parsad D, et al. Dermatoscopic evaluation and histopathological correlation of acquired dermal macular hyperpigmentation. Int J Dermatol. 2017;56(12):1395–1399. doi:10.1111/ijd.13782
19. Sgouros D, Theofili M, Zafeiropoulou T, et al. Dermoscopy of actinic keratosis: is there a true differentiation between non-pigmented and pigmented lesions? J Clin Med. 2023;12(3):1063. doi:10.3390/jcm12031063
20. Casari A, Chester J, Pellacani G. Actinic keratosis and non-invasive diagnostic techniques: an update. Biomedicines. 2018;6(1):8. doi:10.3390/biomedicines6010008
21. Akay BN, Kocyigit P, Heper AO, et al. Dermatoscopy of flat pigmented facial lesions: diagnostic challenge between pigmented actinic keratosis and lentigo maligna. Br J Dermatol. 2010;163(6):1212–1217. doi:10.1111/j.1365-2133.2010.10025.x
22. Zalaudek I, Ferrara G, Leinweber B, et al. Pitfalls in the clinical and dermoscopic diagnosis of pigmented actinic keratosis. J Am Acad Dermatol. 2005;53(6):1071–1074. doi:10.1016/j.jaad.2005.08.052
23. Balagula Y, Braun RP, Rabinovitz HS, et al. The significance of crystalline/chrysalis structures in the diagnosis of melanocytic and nonmelanocytic lesions. J Am Acad Dermatol. 2012;67(2):194.e1–194.e8. doi:10.1016/j.jaad.2011.04.039
24. Weyers W. The Centennial of Bowen’s disease-a critical review on the occasion of the 100th anniversary of its original description. Dermatol Pract Concept. 2012;2(4):204a02. doi:10.5826/dpc.0204a02
25. Ragi G, Turner MS, Klein LE, et al. Pigmented Bowen’s disease and review of 420 Bowen’s disease lesions. J Dermatol Surg Oncol. 1988;14(7):765–769. doi:10.1111/j.1524-4725.1988.tb01161.x
26. Zalaudek I, Argenziano G, Leinweber B, et al. Dermoscopy of Bowen’s disease. Br J Dermatol. 2004;150(6):1112–1116. doi:10.1111/j.1365-2133.2004.05924.x
27. Wozniak-Rito AM, Rudnicka L. Bowen’s disease in dermoscopy. Acta Dermatovenerol Croat. 2018;26(2):157–161.
28. Álvarez-Salafranca M, Ara M, Zaballos P. Dermoscopy in Basal cell carcinoma: an updated review. Actas Dermosifiliogr. 2021;112(4):330–338. doi:10.1016/j.ad.2020.11.011
29. Lallas A, Apalla Z, Argenziano G, et al. The dermatoscopic universe of basal cell carcinoma. Dermatol Pract Concept. 2014;4(3):11–24. doi:10.5826/dpc.0403a02
30. Yélamos O, Braun RP, Liopyris K, et al. Dermoscopy and dermatopathology correlates of cutaneous neoplasms. J Am Acad Dermatol. 2019;80(2):341–363. doi:10.1016/j.jaad.2018.07.073
31. Stuart CA, Driscoll MS, Lundquist KF, et al. Acanthosis nigricans. J Basic Clin Physiol Pharmacol. 1998;9(2–4):407–418. doi:10.1515/JBCPP.1998.9.2-4.407
32. Pardeshi SS, Khemani UN, Kamath RR, et al. Therapeutic implications of dermoscopic findings in acanthosis nigricans: a clinical and histopathological study. Dermatol Ther. 2020;33(6):e14521. doi:10.1111/dth.14521
33. Elmas ÖF, Demirbaş A, Kutlu Ö, et al. Utility of dermatoscopy in the diagnosis of acanthosis nigricans. J Cosmet Dermatol. 2020;19(12):3426–3427. doi:10.1111/jocd.13670
34. Gilchrest BA, Fitzpatrick TB, Anderson RR, et al. Localization of melanin pigmentation in the skin with Wood’s lamp. Br J Dermatol. 1977;96(3):245–248. doi:10.1111/j.1365-2133.1977.tb06132.x
35. Bae JM, Lee RW. 365-nm narrowband Wood’s lamp for vitiligo and hypopigmentation disorders. J Am Acad Dermatol. 2020;83(4):e283–e284. doi:10.1016/j.jaad.2019.08.064
36. Lan J, Wen J, Cao S, et al. The diagnostic accuracy of dermoscopy and reflectance confocal microscopy for amelanotic/hypomelanotic melanoma: a systematic review and meta-analysis. Br J Dermatol. 2020;183(2):210–219. doi:10.1111/bjd.18722
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.