Back to Journals » Patient Preference and Adherence » Volume 19
Deriving Drug Treatment Preference for Osteoporosis Patients Using Discrete Choice Experiments: A Scoping Review
Authors Wang Y ![]() , Lu H, Liu G, Niu C, Zhang Z, Zhan Q, Liu M, Qin H
, Lu H, Liu G, Niu C, Zhang Z, Zhan Q, Liu M, Qin H
Received 7 July 2025
Accepted for publication 16 October 2025
Published 6 November 2025 Volume 2025:19 Pages 3483—3492
DOI https://doi.org/10.2147/PPA.S552204
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yue Wang,1 Hui Lu,1 Guoqing Liu,2 Congying Niu,3 Zhenwei Zhang,1 Qiongling Zhan,4 Mengmeng Liu,4 Hanzhi Qin1
1Department of Nursing, The First Affiliated Hospital of USTC, Hefei, Anhui, People’s Republic of China; 2Department of Nursing,Tianjin First Central Hospital, Tianjin, People’s Republic of China; 3Department of Cardiology, The First Affiliated Hospital of USTC, Hefei, Anhui, People’s Republic of China; 4Department of Joint Surgery Ward 2, The First Affiliated Hospital of USTC, Hefei, Anhui, People’s Republic of China
Correspondence: Hanzhi Qin, Department of Nursing, The First Affiliated Hospital of USTC, Hefei, Anhui, People’s Republic of China, Email [email protected]
Objective: To conduct a scoping review of discrete choice experiment (DCE) studies assessing medication preference patterns in patients with osteoporosis, focusing on quantifying preference intensities, willingness-to-pay for treatment attributes, and heterogeneity in preferences across patient subgroups. This analysis aims to support evidence-based clinical decision-making.
Methods: A scoping review was undertaken, where five electronic databases were searched for key terms to identify eligible DCE studies related to drug treatment preference for osteoporosis patients. We included studies that met criteria, including being published from database establishment until April 20, 2024. Data were systematically extracted, tabulated, and summarised in a narrative review.
Results: Nine studies met the inclusion criteria, six of which were conducted in Europe. The included DCE studies contained between 3 and 6 attributes and 2 to 6 levels per attribute. The number of choice sets per study ranged from 8 to 36. Treatment efficacy emerged as the most critical attribute. Subgroup analyses revealed significant preference heterogeneity associated with age, educational attainment, and fracture history.
Conclusion: Incorporating quantified patient preferences and WTP metrics into treatment planning may optimize adherence rates and osteoporosis management outcomes. This preference-sensitive approach demonstrates potential to reduce both clinical burden and patient financial burden through value-based treatment allocation.
Keywords: osteoporosis, discrete choice experiment, preference, scoping review
Background
The aging population in China has led to a rising prevalence of osteoporosis (OP), a systemic metabolic bone disorder pathophysiologically characterized by diminished bone mineral density and disrupted trabecular microarchitecture, resulting in increased bone fragility and fracture risk.1,2 Contemporary epidemiological modeling estimates a global incidence of 8.9 million osteoporosis-related fractures annually, equating to one fracture event every 3 seconds.3,4 In China, the prevalence among adults aged ≥65 years is 32.0%, with a significant gender disparity (51.6% in women vs 10.7% in men).5,6 Economic projections using Markov modeling forecast osteoporosis-attributable annual direct healthcare expenditure will reach ¥1429.8 billion (USD 199.3 billion) by 2035.7
OP pathophysiology centers on an imbalance between bone resorption by osteoclasts and bone formation by osteoblasts. Pharmacological interventions are accordingly stratified into two mechanistically distinct categories: antiresorptive agents (bone turnover inhibitors, eg bisphosphosates, anti-RANKL, etc.) targeting osteoclast-mediated bone resorption, and osteoanabolic therapies (bone-forming agents, eg teriparatide, human monoclonal anti-sclerostatin, etc.) stimulating osteoblast-mediated bone formation.8
Medication adherence is a critical determinant of treatment success, and patient preferences for drug attributes significantly influence adherence behavior.9 With the advancement of OP drugs and the increasing adoption of patient-centered care paradigms, clinical decision-making has progressively emphasized patient preferences and values, and many scholars have invested in researching patients’ preferences for OP drugs and exploring the attributes or factors that affect their preferences.10 The discrete choice experiment (DCE) is a well-established method for quantifying patient preferences by analyzing trade-offs among hypothetical drug profiles defined by a set of attributes.11 While DCEs have been applied to study OP drug preferences, a systematic synthesis of these studies is lacking. Identifying the key attributes influencing patient choices and highlighting evidence gaps are essential for translating preference evidence into clinical practice.
Therefore, this study conducts a scoping review of DCE-based research on drug treatment preferences of OP patients. The following research question was formulated: 1) What are the key drug attributes influencing OP patients’ preferences as identified in DCE studies? 2) How do preferences vary across different patient subgroups (eg, by gender, age, or fracture history)? 3) How can the findings from preference studies be leveraged to improve clinical dosing regimens and enhance patient compliance?
Objective
(1) To identify the drug attributes and non-drug attributes that affect the medication treatment preferences of OP patients.
(2) To determine the strength and willingness to pay of these attributes.
Methods
This study is guided by Joanna Briggs Institute (JBI) guidelines for scoping reviews.12
Search Strategies
Five electronic databases (Web of Science, PubMed, CNKI, Wanfang Database, and VIP, with the search timeframe spanning from database inception to April 30, 2024) were searched with the assistance of a librarian to identify the studies that applied a DCE method to elicit osteoporosis patients’ preferences towards medication. The search strategies are detailed in Table 1.
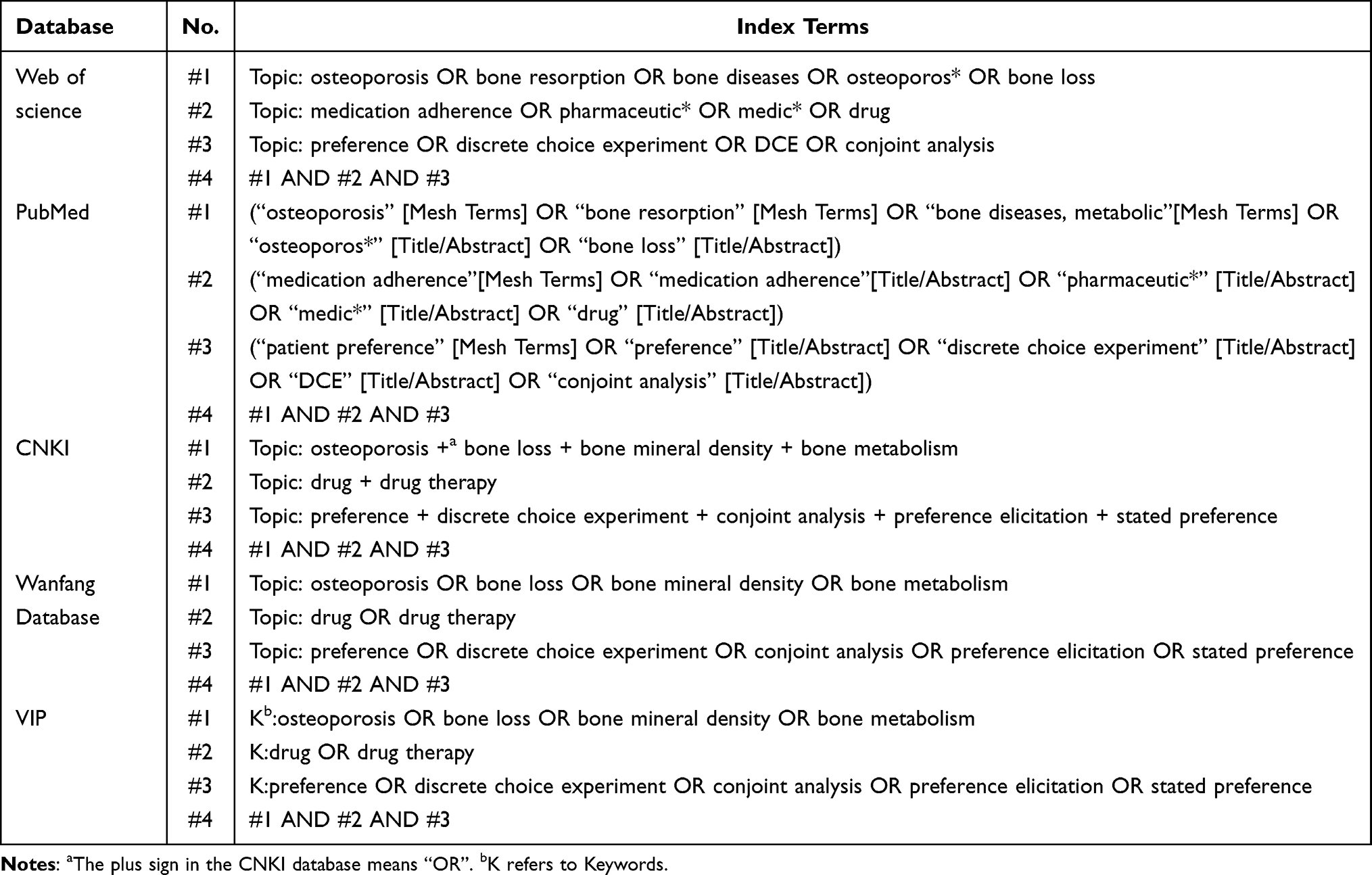 |
Table 1 Search Strategies |
Study Selection
After combining the search results from five databases, duplicates were removed. The inclusion criteria were: 1) study participants were OP patients; 2) methodology employed DCE; and 3) research focused on pharmacotherapy preferences of OP patients. The exclusion criteria were: 1) duplicate publications; 2) non-Chinese/English publications; 3) articles with unavailable full text; 4) grey literature (eg, conference abstracts, dissertations); and 5) non-primary research (eg, reviews, commentaries, news reports).
Data Extraction and Quality Assessment
Two investigators independently conducted the initial title/abstract screening. Subsequently, they performed full-text reviews of potentially eligible publications meeting the inclusion criteria, maintaining independent evaluation throughout the process. If there is no consensus, it will be decided through joint discussion by a third researcher. For each of the included publications data were charted: author(s), objective(s), study design, study population and sample size, attributes (levels), and conclusion. Data extraction encompassed: 1) Basic information (author(s), country, sample size); 2) DCE-specific components (sample size calculation method, included attributes/levels, number of choice sets, presence of opt-out options, key findings).
This study applied the 13-item quality assessment criteria previously published and validated by Mandeville et al,13 which comprehensively address all four critical phases of DCEs. These criteria have been consistently employed in prior research to evaluate the methodological rigor of included studies.14
Results
Selection of the Studies Included in the Review
The literature screening process is shown in Figure 1. A systematic search across five databases yielded 1,157 records. Following duplicate removal and exclusion of records not meeting inclusion/exclusion criteria, nine studies were ultimately retained for analysis.
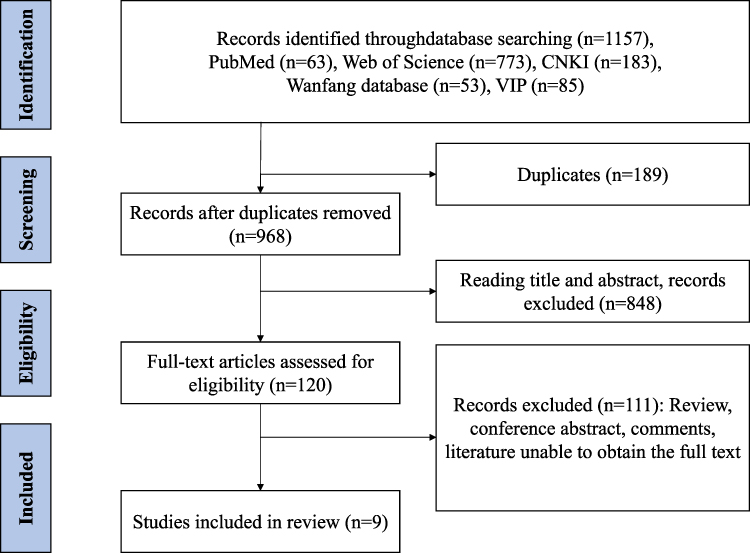 |
Figure 1 PRISMA flow diagram showing process of study selection for inclusion in review. |
Quality Assessment
All studies were scored against a list of 13 criteria,13 with median count of 8/13, and a range between 515 and 11,16 shown in Table 2.
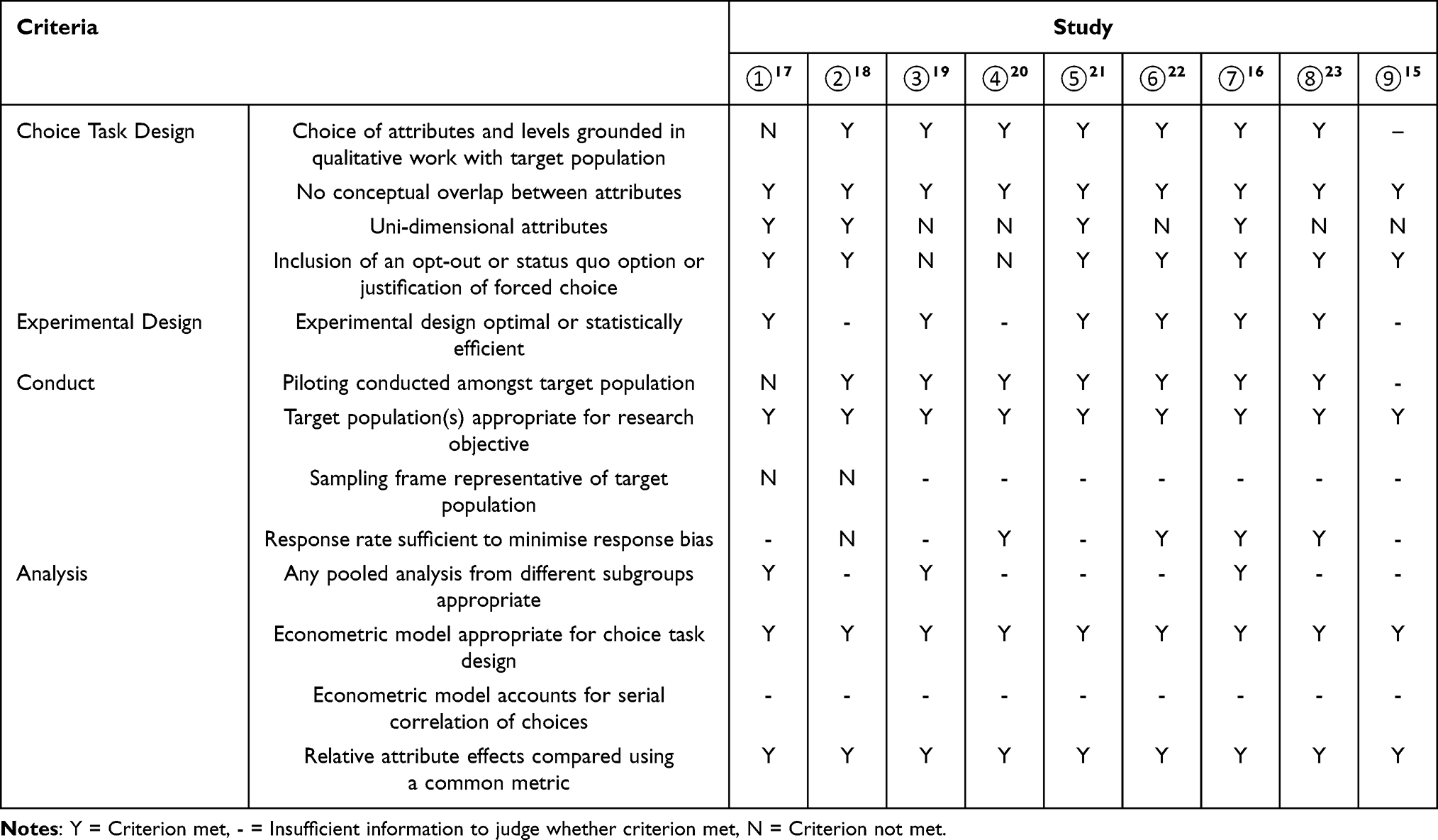 |
Table 2 Validity Assessment of Included Studies |
Overview of the Studies Included in the Review
Six of the nine studies were conducted in Europe, and all the details regarding the sample and DCE characteristics of the included studies are shown in Table 3.
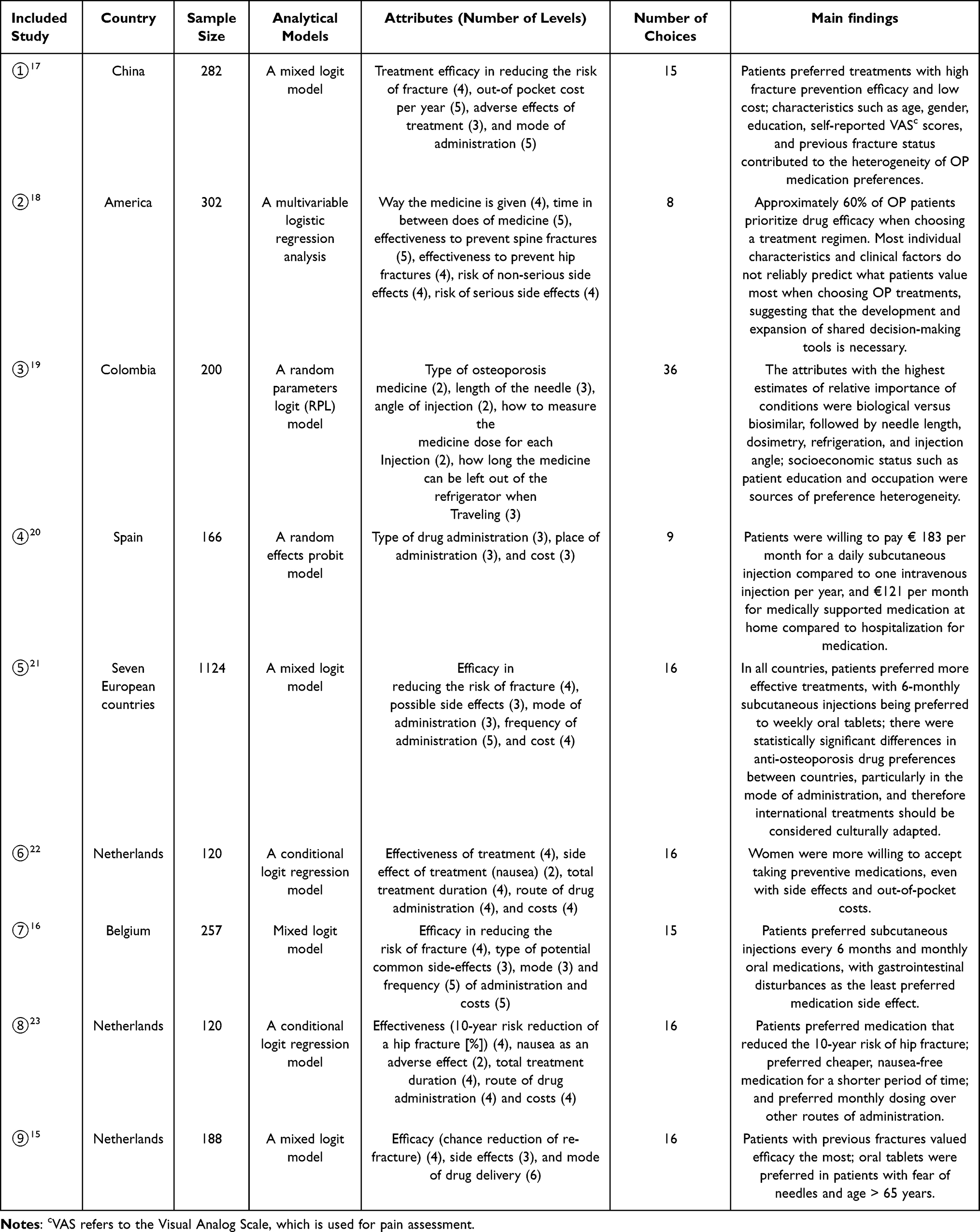 |
Table 3 Basic Characteristics of Included Studies |
Determination of Attributes and Levels of Medication Preferences in OP Patients
Determining the attributes and levels that influence medication preferences of OP patients is a fundamental and important step in the implementation of DCE, and every decision in its process affects the study design of the DCE.11 Attributes and levels can be determined through literature review, qualitative research (eg, semi-structured interviews), focus group discussions, priority setting, etc., and need to be integrated with respondent perspectives, specific policies, and decision-making settings.24 In this study, attributes were either quantitative (eg, frequency of administration, out-of-pocket costs, etc.) or qualitative (eg, drug type, mode of administration). The number of attributes of DCE studies in healthcare generally ranges from 3 to 9, with a median of 5, and the number of levels also generally ranges from 2 to 5.25 The number of DCE study attributes included in this study ranged from 3 to 6 and the number of levels ranged from 2 to 6. The included attributes were drug and non-drug attributes: efficacy/effectiveness, mode of administration, frequency of administration, side effects/adverse reactions, out-of-pocket costs, total treatment time, angle of injection, length of the needle, how to measure the drug dosage, and the length of time the drug does not need to be refrigerated.
OP Medication Preference Choice Set Construction and Experimental Design
After determining the attributes and levels, it is necessary to construct drug regimens with different characteristics for different combinations of attribute levels, ie, hypothetical choice sets. The complete combination of all attribute levels is called a “full factorial design”, which allows for the independent estimation of all main effects (the effect of each attribute) and interaction effects (the effect of interactions between two or more attributes).26 However, given the patient burden and practicalities, researchers usually choose a departmental analysis dependent design, which likewise allows for the estimation of all effects of interest to the researcher. A common approach to DCE choice set construction in health care is the small-part analytic factorization design known as orthogonal main effects plans (OMEPs), which implies strictly additive indirect utility functions (IUFs).26 The number of choice sets in the DCE studies included in this study ranged from 8 to 36, and most of the studies set an opt-out option (opt-put), which can effectively reduce the bias of parameter estimation. In order to reduce the cognitive burden of OP patients, some DCE studies randomly assigned the medication regimen choice sets to different questionnaires to improve the survey quality.19 Also, in order to test the validity of the questionnaire, some studies set up a repeated choice set as a way to assess the consistency of OP patients’ pre and post choices,16,21 and some studies set up a dominant choice set as a way to test whether OP patients understood the DCE choice set.22,23
Data Collection and Statistical Analysis
Patient recruitment in the DCE studies included in this study was done through a variety of online and offline methods such as outpatient clinics, e-mail, and mailed questionnaires, and the sample size calculations included the thumb rule proposed by Johnson and Orme17,19 and the rule of thumb proposed by Pearmain and Kroes,16,18,21,22 while the other three studies did not mention the sample size calculation method, and the sample sizes included ranged from 120 to 1124, which meets the sample size requirements of the DCE study’s requirements for sample size.
Conditional logit models and their variants (including random parametric/mixed logit models, hierarchical Bayes, latent class mixture models, etc.) are often used for DCE data analysis, and five studies in this study applied random parametric/mixed logit models to analyze the data, which can reduce the impact of patients’ individual differences and heterogeneity of preferences on the results of the study, and is currently the most widely used in the field of health care;27 two studies used conditional logit regression models, one study used a random effects probit model, and one study used multivariate logistic regression analysis.
Key Findings on Medication Preferences in OP Patients
Strength of Preference and WTP for Medication in Patients with Osteoporosis
Drug efficacy in OP patients generally refers to the ability of a drug to reduce the incidence/risk of fractures in patients and is an attribute that is valued by patients receiving drug therapy. Hip fracture prevention efficacy was the most valued attribute of patient medication in the study by Liu et al18 which is consistent with the findings of Cornelissen et al.15 Si et al17 reported that OP patients were willing to pay more monetarily to improve the efficacy of medication for fracture prevention, an additional $3689 annually for each 1% improvement in efficacy. Patients preferred medication that reduced the 10-year risk of hip fracture, and for every 10% reduction in fracture risk, patients were willing to adhere to medication for 7.5 years and were willing to pay €175 in the De Bekker-Grob et al study.22
The mode of administration, which includes the route of administration as well as the frequency of administration, is likewise an important factor influencing the medication preferences of many OP patients. A study by Si et al17 showed that annual intravenous infusion was the most strongly preferred method of administration, with patients willing to pay an additional $30,884 compared to weekly oral tablets, followed by 6-monthly subcutaneous injections. Similarly in the study by Hiligsmann et al,16 patients preferred a dosing regimen of subcutaneous injections every 6 months over weekly oral tablets, were willing to pay an additional monthly cost of €19.53, or were willing to give up 13.52% of the drug’s efficacy in exchange for a 6-month subcutaneous treatment pattern, which is in line with the results of a DCE study conducted by Hiligsmann et al21 in 7 European countries, where patients favored a regimen with less frequent and longer intervals of administration, regardless of the mode of administration. In contrast, Darba et al20 who investigated the preferences of 166 OP patients in Spain for medication, showed the opposite result, patients were willing to pay €142 per month for a daily subcutaneous injection compared to a daily or weekly tablet, and €183 per month for a daily subcutaneous injection compared to an annual intravenous injection. These differences may be related to the fact that customs vary from region to region.
Medication side effects are likewise a major consideration for OP patients. In two studies by Hiligsmann et al,16,21 patients valued the impact of side effects the most, with gastrointestinal disturbances being more unacceptable than the two side effects of skin reactions and flu-like symptoms. In two studies by De Bekker-Grob et al, patients favored cheaper, nausea-free medication for a shorter period of time,23 and patients were willing to pay $752 to avoid nausea as a side effect.22
Factors such as the type of medication, the angle of administration, and the location of administration similarly influence patient medication preferences. A study by Graham-Clarke et al19 showed that despite the availability of biosimilar teriparatide in Colombia, patients preferred to receive the original biologic, preferring drugs with shorter needles, 45-degree injections, automated administration, and drugs that could be stored in the refrigerator for longer periods of time. A study by Darba et al20 showed that patients preferred to administer medication at home once a day with medical support, and were willing to pay €59 per month to administer medication at home with medical support compared to administering medication at home alone, and were willing to pay €121 per month for medical support while receiving medication at home compared to receiving medication for a couple of hours in a hospital.
Heterogeneity of Drug Treatment Subgroup Preferences in OP Patients
There are differences in medication preferences for OP patients with different traits. Si et al17 suggested that patients age was the main factor for preference heterogeneity, there was a statistically significant difference in preference for adverse effects in patients ≤ 60 years of age, whereas there was no statistically significant difference in patients > 60 years of age, and the difference in preference for mode of administration was statistically significant in both cases, but the preference was stronger in patients ≤ 60 years of age. In the study by Cornelissen et al,15 oral intake had the greatest impact on medication preference in elderly patients, who preferred monthly oral tablets to intravenous therapy, with medication side effects being the attribute they cared least about. There is an effect of patient education on their preference. Patients who graduated from college highly valued the efficacy of medication in fracture prevention when choosing medication in the study of Liu et al,18 and highly educated patients preferred the attribute of automated drug administration in the study of Graham-Clarke et al.19 The presence or absence of a history of fracture is also an important influence on medication preference in OP patients, with patients with a history of previous fracture valuing efficacy more than those with no history of fracture,15 which were similar to the findings of Darba et al, who reported that patients that have suffered one or more fractures would be willing to pay more for their treatment preferences to avoid more risks.20 Patients’ beliefs about the necessity of medication also influence their preferences, with patients with strong beliefs focusing more on the efficacy of medications in preventing fractures.18
Discussion
Osteoporosis poses a significant burden in aging populations, where poor medication adherence remains a major clinical challenge.28 Understanding patient preferences is crucial for improving adherence.29 A scoping review is an evidence-based approach to knowledge integration and evidence identification, with strengths such as breadth of search, rigor of study design, and a higher level of evidence in scoping reviews compared to traditional reviews.30 Therefore, this study was based on a scoping review to retrieve and summarize the studies on medication preferences of OP patients to understand the factors influencing their preferences as well as the strength of each factor and WTP, so as to provide scientific references for healthcare professionals when making medication decisions.
Medication effectiveness remains the most important attribute for the majority of OP patients, which is consistent with the results obtained by other research methods (eg, Likert scale, OP treatment questionnaire).31 Medication effectiveness refers to a reduced risk of fracture/re-fracture, and patients are willing to pay a higher price and experience longer treatment cycles in exchange for efficacy. In terms of the mode of administration, patients preferred less frequent and longer intervals of administration as well as safer medication regimens, which are more convenient for patients and easy to follow in the long term. Gastrointestinal reactions are the least acceptable side effect of drug therapy for all patients, which is informative for pharmaceutical groups when determining the composition of drugs. In addition pharmacological attributes such as the type of drug administered and non-pharmacological attributes such as the angle of administration and the place of administration significantly influence patients’ medication preferences. OP patients weigh different attributes when making medication choices to make the choice that best meets their needs. Compared with the systematic review on women’s values and preferences regarding OP treatments conducted by Barrionuevo et al,32 our study confirms the key priorities they identified, particularly patients’ emphasis on effectiveness and less frequent administration.However, by focusing on DCEs, our review provides critical quantitative advancements. It addresses the limitations in Barrionuevo et al’s study32 that were unable to guide trade-offs, offering previously unavailable actionable data for policy and clinical decision-making.
There are differences in medication preferences among OP patients with different demographic characteristics due to cognitive, environmental, and other differences. Older patients are more likely to accept relatively safe and non-invasive medication regimens, which may be related to the physical condition of the elderly. Differences in drug treatment preferences among patients from different countries may be related to differences in cultural background, economic level and health care system. Patients whom have suffered from a previous fracture are more aware of the inconvenience of a fracture than patients without a previous fracture, so they value the efficacy of the medication and have a higher WTP. The greater focus on efficacy as well as convenience in more educated patients may be related to the fact that such patients are more capable of learning about medication and have higher expectations of medication efficacy.
Improving medication adherence may have a more significant impact on patient health status than other treatment measures. Healthcare professionals are becoming aware of the differences in treatment preferences with their patients and are therefore fully incorporating patient preferences and values in their decision-making. At the same time, the results of this study provide a scientific basis for health insurance policy making, especially in terms of drug reimbursement, which should take into account medical and economic factors as well as patient group preferences.
Limitation of this scoping review included: 1) The retrieval work was completed in May 2024, therefore relevant studies may have been published subsequently; and 2) The relative importance of OP patient preference attributes across different studies must be used with caution, as the selection of assumed attributes and levels, as well as differences in patient populations across regions and economic levels, may influence the relative importance.
This scoping review delineates the current landscape of utilizing DCE to investigate medication preferences among OP patients. To further deepen understanding and translate research findings, future studies could: 1) conduct meta-analyses on specific attributes to quantify preference strength; 2) transform DCE results into clinical decision aids to facilitate shared decision-making; and 3) implement longitudinal studies to directly validate the impact of preference matching on medication adherence.
Conclusion
This scoping review demonstrates that medication effectiveness has always been the most valued attribute for the majority of OP patients. Preference heterogeneity was observed across subgroups based on fracture history, education, and cultural context. By providing robust, quantitative evidence on patient priorities, this study offers a critical foundation for shared clinical decision-making, patient-centered drug development, and informed health policy formulation, ultimately aiming to enhance adherence and treatment outcomes in osteoporosis care.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Anhui Provincial Key Research and Development Program–Clinical Medical Research Translation Specialization (Grant No. 202304295107020020) and the USTC Research Funds of the Double First-Class Initiative (Grant No. YD9110002053).
Disclosure
The authors declare that they have no competing interests.
References
1. Li Q, Peipei C, Tiemin Z, et al. Analysis of the disease burden and trend of osteoporosis in China from 1990 to 2021. Chinese Health Economics. 2024;43(12):33–37.
2. Zhang L, Zheng Y, Wang R, et al. Exercise for osteoporosis: a literature review of pathology and mechanism. Front Immunol. 2022;13:1005665. doi:10.3389/fimmu.2022.1005665
3. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. doi:10.1007/s00198-006-0172-4
4. Black DM, Rosen CJ. Clinical practice. postmenopausal osteoporosis. N Engl J Med. 2016;374(3):254–262. doi:10.1056/NEJMcp1513724
5. Jinxiang Y, Jiaming L, Zihao L, et al. The survey of the prevalence of osteoporotic fractures at different locations. Chinese Journal of Bone and Joint Surgery. 2024;17(01):79–83.
6. Center for Prevention and Control of Chronic Non-communicable Diseases, Chinese Center for Disease Control and Prevention (CDC). China osteoporosis epidemiology survey report-2018. People’s Health Publishing House, 2021.
7. Xiao P, Cui A, Hsu C, et al. Global, regional prevalence, and risk factors of osteoporosis according to the World Health Organization diagnostic criteria: a systematic review and meta-analysis. Osteoporos Int. 2022;33(10):2137–2153. doi:10.1007/s00198-022-06454-3
8. Oliveira LG, Carneiro LRG, Souza MPGD, et al. Osteoporosis drug treatment update. Rev Bras Ortop. 2021;56(5):550–557.
9. Barrett-Connor E, Wade SW, Do TP, et al. Treatment satisfaction and persistence among postmenopausal women on osteoporosis medications: 12-month results from POSSIBLE US. Osteoporos Int. 2012;23(2):733–741. doi:10.1007/s00198-011-1620-3
10. Hiligsmann M, Bours SP, Boonen A. A review of patient preferences for osteoporosis drug treatment. Curr Rheumatol Rep. 2015;17(9):61. doi:10.1007/s11926-015-0533-0
11. Qiuchen W, Xiuying Z, Hui X, et al. Research progress in developing attributes and levels of discrete choice experiments. Modern Preventive Med. 2020;47(12):2199–2201.
12. Peters M G C M P. Chapter 11: scoping Reviews. In: JBI Manual for Evidence Synthesis. 2020.
13. Mandeville KL, Lagarde M, Hanson K. The use of discrete choice experiments to inform health workforce policy: a systematic review. BMC Health Serv Res. 2014;14(1):367. doi:10.1186/1472-6963-14-367
14. Brain D, Jadambaa A, Kularatna S. Methodology to derive preference for health screening programmes using discrete choice experiments: a scoping review. BMC Health Serv Res. 2022;22(1):1079. doi:10.1186/s12913-022-08464-7
15. Cornelissen D, Boonen A, Bours S, et al. Understanding patients’ preferences for osteoporosis treatment: the impact of patients’ characteristics on subgroups and latent classes. Osteoporos Int. 2020;31(1):85–96. doi:10.1007/s00198-019-05154-9
16. Hiligsmann M, Dellaert BG, Dirksen CD, et al. Patients’ preferences for osteoporosis drug treatment: a discrete-choice experiment. Arthritis Res Ther. 2014;16(1):R36. doi:10.1186/ar4465
17. Si L, Tu L, Xie Y, et al. Chinese patients’ preference for pharmaceutical treatments of osteoporosis: a discrete choice experiment. Arch Osteoporos. 2019;14(1):85. doi:10.1007/s11657-019-0624-z
18. Liu X, Makaroff KE, Almario CV, et al. Determining patient preferences for the medical management of osteoporosis using conjoint analysis. Osteoporos Int. 2024;35(1):153–164. doi:10.1007/s00198-023-06882-9
19. Graham-Clarke PL, Hauber B, Boeri M, et al. Patient preferences for biologic and biosimilar osteoporosis treatments in Colombia. Patient Prefer Adherence. 2020;14:1049–1064. doi:10.2147/PPA.S250745
20. Darba J, Restovic G, Kaskens L, et al. Patient preferences for osteoporosis in Spain: a discrete choice experiment. Osteoporos Int. 2011;22(6):1947–1954. doi:10.1007/s00198-010-1382-3
21. Hiligsmann M, Dellaert BG, Dirksen CD, et al. Patients’ preferences for anti-osteoporosis drug treatment: a cross-European discrete choice experiment. Rheumatology. 2017;56(7):1167–1176. doi:10.1093/rheumatology/kex071
22. De Bekker-Grob EW, Essink-Bot ML, Meerding WJ, et al. Patients’ preferences for osteoporosis drug treatment: a discrete choice experiment. Osteoporos Int. 2008;19(7):1029–1037. doi:10.1007/s00198-007-0535-5
23. De Bekker-Grob EW, Essink-Bot ML, Meerding WJ, et al. Preferences of GPs and patients for preventive osteoporosis drug treatment: a discrete-choice experiment. Pharmacoeconomics. 2009;27(3):211–219. doi:10.2165/00019053-200927030-00004
24. Bridges JF, Hauber AB, Marshall D, et al. Conjoint analysis applications in health--a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
25. Yue W. Toward Preference for Choosing an Elderly Care institution-Adiscrete Choice Experiment for Community Elderly in Tianjin. Tianjin University of Traditional Chinese Medicine; 2023.
26. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. Pharmacoeconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
27. Yuzhen Y, Qian H, Yachao J, et al. Scoping review of factors influencing vaccination preferences based on discrete choice experiments. Chinese Journal of Vaccines and Immunization. 2023;29(06):698–707.
28. Ruxu Y, Cong Z, Yu Z. Expert consensus on rational use of anti-osteoporosisagents(2023). Chinese Journal of Hospital Pharmacy. 2024;44(09):985–1006.
29. Losi S, Berra CCF, Fornengo R, et al. The role of patient preferences in adherence to treatment in chronic disease: a narrative review. Drug Target Insights. 2021;15:13–20. doi:10.33393/dti.2021.2342
30. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
31. Makras P, Galanos A, Rizou S, et al. Development and validation of an osteoporosis treatment questionnaire (OSTREQ) evaluating physicians’ criteria in the choice of treatment. Hormones. 2016;15(3):413–422. doi:10.14310/horm.2002.1684
32. Barrionuevo P, Gionfriddo MR, Castaneda-Guarderas A, et al. Women’s values and preferences regarding osteoporosis treatments: a systematic review. J Clin Endocrinol Metab. 2019;104(5):1631–1636. doi:10.1210/jc.2019-00193
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.