Back to Journals » Clinical Interventions in Aging » Volume 17
Depressive Symptoms and ADL/IADL Disabilities Among Older Adults from Low-Income Families in Dalian, Liaoning
Authors Zhao L, Wang J, Deng H, Chen J, Ding D
Received 23 December 2021
Accepted for publication 20 April 2022
Published 6 May 2022 Volume 2022:17 Pages 733—743
DOI https://doi.org/10.2147/CIA.S354654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Lu Zhao,1 Junting Wang,2 Haoyuan Deng,3 Junfeng Chen,2 Ding Ding2
1Department of Medical Sociology, School of Humanities and Social Sciences, Dalian Medical University, Dalian, 116044, People’s Republic of China; 2Department of Social Medicine, School of Public Health, Dalian Medical University, Dalian, 116044, People’s Republic of China; 3Department of Nutrition and Food Health, School of Public Health, Dalian Medical University, Dalian, 116044, People’s Republic of China
Correspondence: Junfeng Chen; Ding Ding, Department of Social Medicine, School of Public Health, Dalian Medical University, No. 9 West Section Lvshun South Road, Dalian, 116044, People’s Republic of China, Tel +86 13009493030 ; +86 18249517190, Email [email protected]; [email protected]
Purpose: This study aimed to assess the prevalence of depressive symptoms and ADL/IADL disabilities and explore their correlation and associated factors for depressive symptoms among community-dwelling older adults from low-income families in Dalian, Liaoning Province, China.
Methods: This cross-sectional study included 522 participants aged 60 years and older from low-income families in Dalian. The 30-Item Geriatric Depression Scale was employed to measure depressive symptoms. The Katz ADL Scale and IADL Scale were used to evaluate the performance of activities necessary for independent life. SPSS 22.0 was employed to analyze the data. Logistic regression was used to estimate the relationship between depressive symptoms and ADL/IADL disabilities in five models.
Results: The prevalence of depressive symptoms among older people from low-income families in Dalian was 57.3%. A total of 19.0% had difficulties performing ADLs, and 40.2% had difficulties performing IADLs. Logistic regression analysis revealed that ADL/IADL disabilities were associated with depressive symptoms even after controlling for people’s sociodemographic characteristics, welfare, health conditions and informal care. The following factors were associated with depressive symptoms: education, self-reported health, number of chronic diseases, and emotional support from families.
Conclusion: Given that older people from low-income families in Dalian have a notable prevalence rate of depressive symptoms, and ADL/IADL disabilities were independently associated with these symptoms, it is crucial to give priority to this particular group in geriatric health services due to economic and health disparities.
Keywords: depressive symptoms, ADL disabilities, IADL disabilities, older adults from low-income families, China
Introduction
Aging has become a serious social problem in China, which has the largest elderly population in the world.1 According to the Communiqué of the Seventh National Population Census, the proportion of elderly people aged 60 or above reached 18.70% in 2020, and Liaoning Province ranked first among all provinces in China in terms of the proportion of people aged 60 (25.72%) and over 65 (17.42%). As a common mental disorder in elderly individuals, geriatric depression may even become the second leading cause of disability in the world.2
Studies have revealed that depressive symptoms in later life can be associated with low economic status, and the possibility of depressive symptoms is higher among poorer people across societies and countries. Financial difficulty was one of the risk factors for depressive symptoms in people aged 65+ in Europe.3 In Japan, there was a correlation between relative deprivation and income rank with depressive symptoms among older adults.4 In addition, socioeconomic inequalities have also been proven to be determinants of depressive symptoms among elderly people in China.5,6 Due to the frequent coexistence of poverty and depressive symptoms, it is necessary to examine the current status of depressive symptoms among elderly individuals from low-income families in China.
Depressive symptoms are also reportedly associated with disability, which is widely understood as the limitation of activities necessary for independent life.7 Existing data suggest that financial conditions are correlated with the development of functional limitations, and the number of people with ADL/IADL disabilities has increased in countries and regions with low levels of social and economic development.8 Moreover, a higher prevalence of difficulties in ADLs/IADLs has been reported in studies involving urban elderly people with financial constraints.9 However, little is known about the association between depressive symptoms and ADL/IADL disabilities among community-dwelling older Chinese individuals from urban low-income families.
Dalian is a subprovincial city in Liaoning Province located in the south end of the Liaodong Peninsula, with a geographical area of 12,574 km2. The per capita gross domestic product was 109,644 CNY (approximately 7210 dollars) in 2019, and the level of economic development was at a medium level according to measurements in China. At the end of 2020, the resident population of Dalian was 5.987 million, of which the proportion aged 60 and over was 26.82%. It is an important central and scenic tourism city in the coastal area of northern China. The phenomenon of large-scale elderly population and uneven economic development of regions is prominent, which have drawn our attention to the older adults in low-income families in Dalian.
Geriatric depression is an important public health issue that may have a major impact on primary health care systems, but there are few studies examining depressive symptoms among poor elderly people in urban areas of China, and relevant research data for the correlation between depressive symptoms and ADL/IADL disabilities in this population have not been previously reported. Against this backdrop, we aimed to assess the prevalence of depressive symptoms and ADL/IADL disabilities, explore their correlation and associated factors for depressive symptoms among community-dwelling older adults from urban low-income families in China, and provide a scientific theoretical reference for further improving the health outcomes of such special groups.
Methods
Study Participants
We conducted a cross-sectional study among community-dwelling older adults (aged ≥60) from low-income families in Dalian, Liaoning Province, China, with an effective response rate of 96.49% (522/541). Low-income families were identified according to the enrolment list of Civil Affairs Department. A multistage sampling survey method was used to randomly select 20 streets in 4 districts of Dalian. 2 communities were randomly selected from each street, and 11 families were randomly selected from each community. Elderly individuals aged 60 years and older were the participants among the households surveyed. A total of 440 families with 541 individuals were interviewed from August to December 2019. Questionnaires were completed through a face to face interview conducted by trained investigators visiting the participants’ homes.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Dalian Medical University. Written informed consent was obtained from all the study participants.
Study Variables
Outcome Variable: depressive symptoms
Depressive symptoms were measured with the 30-Item Geriatric Depression Scale (GDS-30). With high reliability and validity, this scale has been widely used in many countries around the world, especially for studies measuring depressive symptoms in Chinese elderly individuals.10–12 Each item in the scale is a question that respondents need to answer using “Yes” or “No”. Scale items 1, 5, 7, 9, 15, 19, 21, 27, 29, and 30 are scored with 1 point for “No” and 0 points for “Yes”; the remaining 20 items are scored with 1 point for “Yes” and 0 points for “No”; thus, the total score ranges from 0 to 30 points. Scores higher than or equal to 11 for older adults were strongly suggestive of depressive symptoms.13 In this study, the GDS-30 demonstrated excellent reliability with a Cronbach’s alpha of 0.916.
Main Independent Variable: ADL/IADL disabilities
Disability can be determined by assessing the performance of activities of daily living (ADLs) and instrumental activities of daily living (IADLs). The Katz ADL Scale is mainly used to assess the needs of caregivers for long-term care based on self-reported performance levels of six basic activities, such as bathing, dressing, and feeding. The scale was proven to have good reliability and validity.14,15 A score of 0 indicates that participants do not need help with activities of daily living, and a score of 1 indicates that they need help. The total score is between 0 and 6, and a participant with a score of 0 is considered to be completely independent. Those participants with scores greater than or equal to 1 are considered to have at least one limitation in ADLs. Our analyses of the ADLs measure demonstrated good reliability with a Cronbach’s alpha of 0.879.
Lawton’s Instrumental Activities of Daily Living (IADLs) Scale is used to assess the independent living functions in one’s daily life in eight different activities, such as food preparation and shopping, which require more complex systemic movement.16 Measuring IADLs required participants to self-report their needs for help with these 8 activities, and a score of 1 indicates that they have difficulty in performing IADLs. A continuous variable with a score range of 0–8 was created. The participants were divided into those without limitations and those who reported at least one hard limitation to IADLs.17 The Cronbach’s alpha of this measure was 0.802.
Covariates
The four groups of control variables in the analysis based on previous studies and subject to information availability were sociodemographic variables, welfare, health conditions and informal care. For sociodemographic variables, gender, age, marital status and education were used. Welfare was measured as receiving aid from the government, having a pension, and receiving medical insurance.
For health conditions, self-reported health status was first assessed by participants in five grades (very good, good, fair, poor, very poor), and then “very good”, “good”, and “fair” were integrated into “good” and “very poor” into “poor”. Each participant was asked to select the number of diseases they had from a list of 7 chronic diseases (hypertension, diabetes, cancer, chronic lung disease, heart disease, stroke, arthritis or rheumatism and others). Hospitalization within the previous year was dichotomized as “yes” or “no”.
For informal care, studies have long documented the beneficial effects of informal care for elderly individuals living with families or having family caregivers in line with the traditional structure of Chinese society.18,19 Thus, living arrangements and caregivers were used to assess informal care. Regarding emotional and instrumental support, emotional support of family was measured by asking participants the question “How satisfied are you with relationships with family?” There were 5 options for the question (very satisfied, satisfied, fair, dissatisfied, very dissatisfied), and then “very satisfied”, “satisfied” and “fair” were integrated into “satisfied”, and “very dissatisfied” was integrated into “dissatisfied”. The participants were also asked whether they received financial support from their families, and independent variables were divided into 2 groups: 1 = yes, 2 = no.
Statistical Analysis
Descriptive statistics were used to calculate the number and proportion of the distribution of participants by whether they had depressive symptoms. Pearson’s chi-square test was used to compare the difference in the distribution between the two groups. Logistic regression was used to estimate the odds ratio of the prevalence of depressive symptoms in participants with ADL/IADL disabilities adjusting for other covariates, first separately or in sets, and finally for all variables simultaneously. Logistic regression analysis was used to test the associated factors for depressive symptoms. For all comparisons, differences were tested using two-tailed tests, and p values less than 0.05 were considered statistically significant. The area under the receiver operating characteristic curve (AUC) were calculated to evaluate the discrimination ability of the model. The Akaike information criterion (AIC) and Bayesian information criterion (BIC) statistics were used to assess goodness of fit.
Results
Sample Characteristics
A total of 57.3% of participants had depressive symptoms (61.4% for men and 55.5% for women). With respect to physical function, 19.0% needed support while performing ADLs, and 40.2% needed support while performing IADLs. A large majority were females (69.7%) and 60–69 years old (60.2%). A total of 12.1% received aid from the government every month. Almost all of them (94.3%) had medical insurance, and 78.5% had a pension. Most older adults (67.0%) reported poor health and chronic diseases (76.4%). Nearly half of them (44.6%) were hospitalized in the past 12 months. A total of 21.8% had no caregiver or others apart from their families in their daily lives, 82.0% did not have financial support, and 46.0% did not receive satisfactory emotional support from their families. Without any adjustment, ADL/IADL disabilities were associated with depressive symptoms (p<0.05). The covariates (sociodemographic characteristics, welfare, health condition, and informal care) included in the baseline were associated with depressive symptoms (p<0.05), except for gender, age, marital status and living arrangements (Table 1).
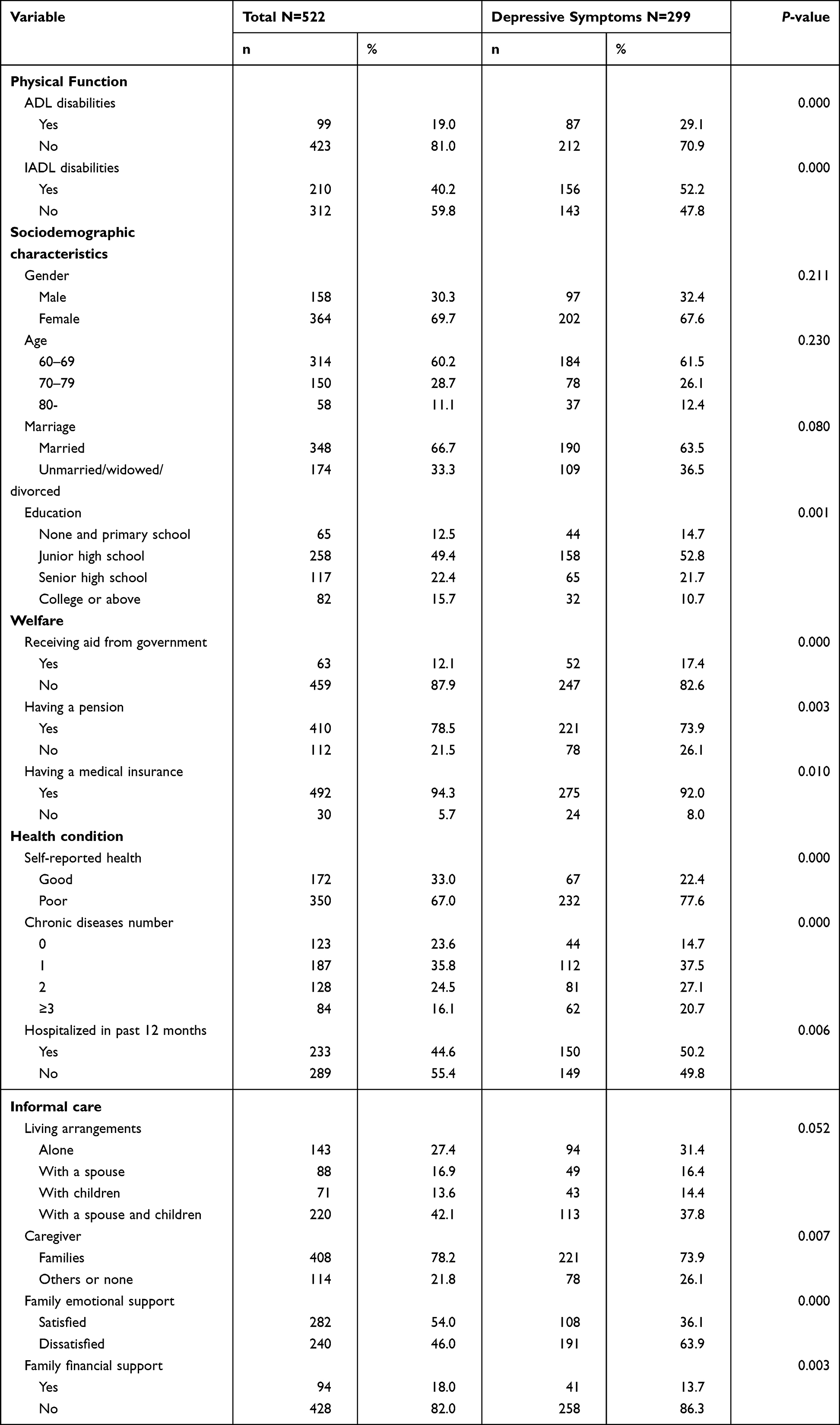 |
Table 1 Distribution of Study Variables Overall |
Depressive Symptoms and ADL/IADL Disabilities
Table 2 shows the association between depressive symptoms and ADL/IADL disabilities. In summary, elderly individuals with ADL/IADL disabilities have a higher prevalence of depressive symptoms (p<0.05). Having difficulties in bathing (17.2%) ranks first among the ADL disabilities, and having difficulties in shopping (30.3%) ranks first among the IADL disabilities.
 |
Table 2 Association Between ADL/IADL Disabilities and Depressive Symptoms |
Correlation of Depressive Symptoms and ADL/IADL Disabilities
Logistic regression was conducted to identify whether depressive symptoms were associated with ADL/IADL disabilities (Table 3). In the unadjusted analysis (R2=0.21), depressive symptoms were significantly associated with ADL disabilities (OR=6.71) and IADL disabilities (OR=3.21). After controlling for the sociodemographic characteristics in Model 2, welfare in Model 3, health condition in Model 4, and controlling for all confounding variables in Model 5 (R2=0.38), the models all show that ADL/IADL disabilities are associated with depressive symptoms (p<0.01).
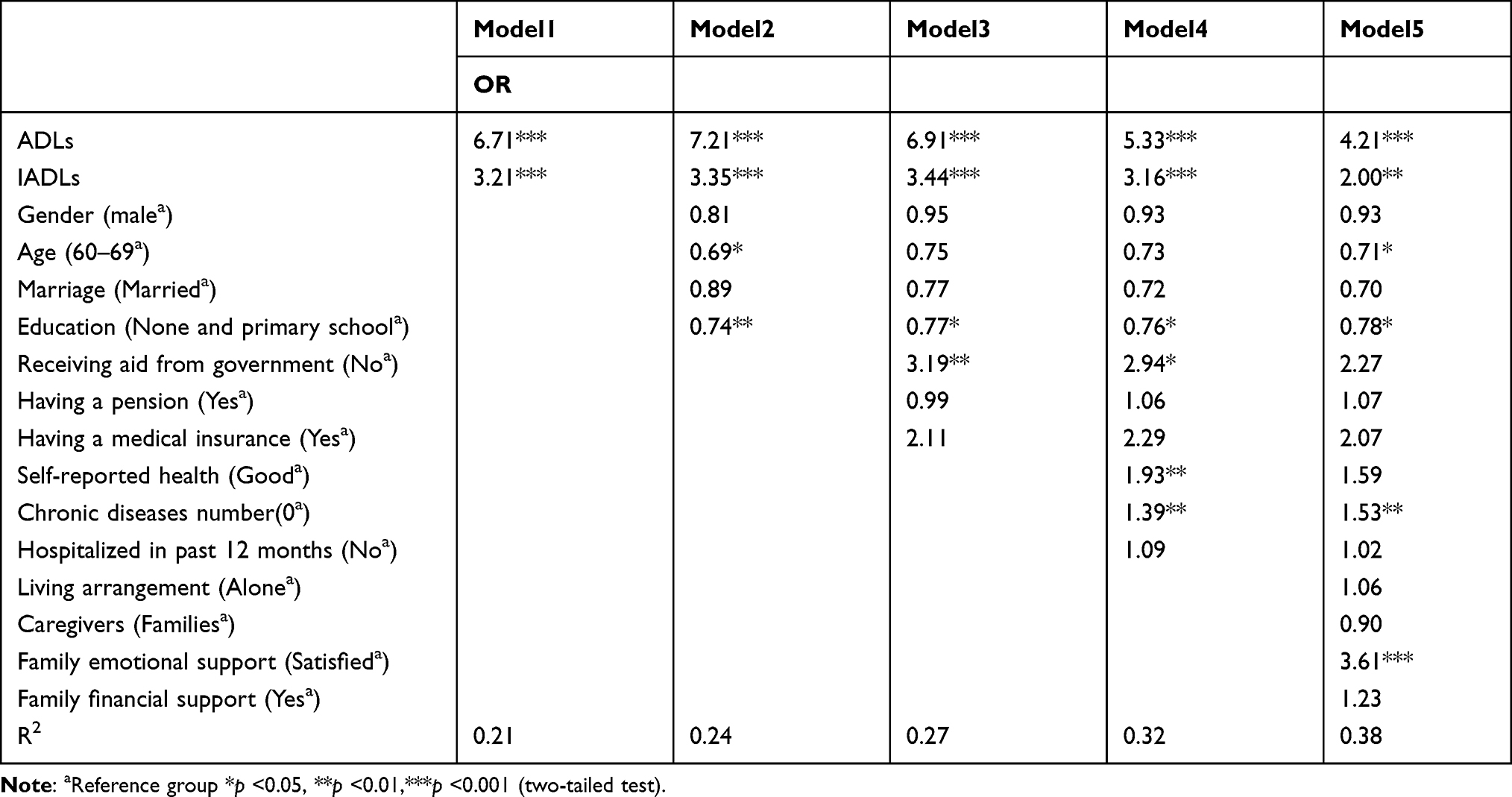 |
Table 3 Logistic Regression Analysis of the Relationship Between ADL/IADL Disabilities and Depressive Symptoms |
Associated Factors for Depressive Symptoms
Variables showing a univariate relationship with the outcome were included in the logistic regression analysis (Table 4). Older adults with lower levels of education (OR=0.75, 95% CI: 0.59–0.95) were more likely to have depressive symptoms than those with higher levels of education. Participants who self-reported poor physical health (OR=1.79, 95% CI: 1.15–2.81) or chronic diseases (OR=1.58, 95% CI: 1.25–2.00) were more likely to have depressive symptoms. Depressive symptoms were also found in elderly individuals without satisfactory emotional support from families (OR=5.05, 95% CI: 3.22–7.92). Compare to the univariate analysis results, receiving aid from the government, having a pension, having medical insurance, hospitalization in the past 12 months, caregivers, and financial support from families were not statistically significant variables in the logistic regression analysis.
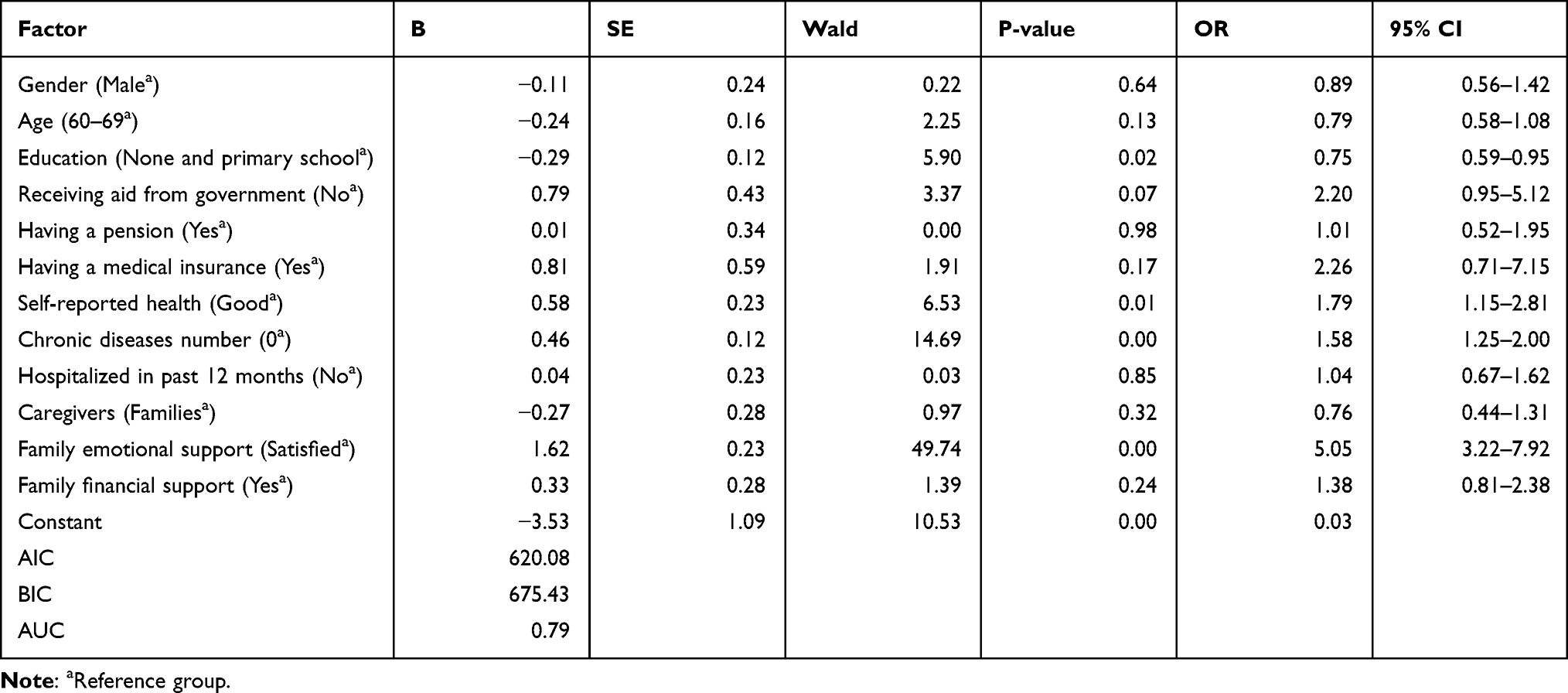 |
Table 4 Logistic Regression Analysis of Associated Factors for Depressive Symptoms |
Discussion
Depression and ADL/IADL disabilities in older adults from low-income families in urban areas are important public health issues that cannot be ignored. In light of this, we evaluated depressive symptoms among community-dwelling older adults from low-income families in Dalian and confirmed that ADL/IADL disabilities can positively predict depressive symptoms. We also found that education, self-reported physical health status and family emotional support were all independently associated with depressive symptoms.
Prevalence of Depressive Symptoms
According to our investigation, the prevalence of depressive symptoms among older adults from low-income families in Dalian was 57.3%, which was much higher than the prevalence in community-dwelling older adults in Xi’an of 27.0% and in Hangzhou, China of 19.2%, according to the GDS-30 Scale.20,21 And higher than the prevalence in some developing countries in Asia; for example, the prevalence of depression among community-dwelling older adults in Malaysia was 11.5% and 39.3% in the Philippines.22,23 Lower than the prevalence in urban elderly individuals from low-income families in developing countries in Asia; for instance, the prevalence of depression was 75.3% in elderly people receiving aid from the Penang state government, Malaysia.24 The prevalence of depression among elderly individuals in urban slums was close to 80% in Cuttack, India according to the GDS-30 Scale.25 These differences could be due to socioeconomic status (SES), and low SES was a strong predictor of depressive symptoms in older adults. Those with a lower household income in later life were more likely to have depressive symptoms.26 In addition, complaints of physical symptoms caused by aging may obscure underlying psychological issues, and depression in older adults is often neglected. Even if depression has been detected, Asian elderly individuals are less likely to seek formal services because of stigmas associated with mental health care.27,28 Therefore, community-dwelling older adults from low-income families are at increased risk for undertreatment of these conditions.29 The community has been proven to be the most accessible way to expand coverage for elderly individuals. Social workers may act as gatekeepers to identify and manage depressive symptoms for this particular group.30
Prevalence of ADL and IADL Disabilities
ADLs have been recognized by the World Health Organization (WHO), and research is recommended on the epidemiology of elderly individuals. Evidence suggests that late-life depression may predict an increase in physical function impairment, and these two factors reinforce each other in later life.31,32 Because of the frequent coexistence of ADL/IADL disabilities and depression, it is necessary to explore the current status of ADL/IADL disabilities among community-dwelling older adults from low-income families. The results of this study showed that elderly individuals are vulnerable to physical function limitations such as ADL/IADL disabilities. Nearly one in five had ADL difficulties, and two in five had IADL difficulties. Regarding ADL disabilities, older people had the highest need for help with bathing (17.2%) and shopping (30.3%), in terms of IADL disabilities; these results seem consistent with previous studies in China.33–35 However, these elderly people are less likely to receive socialized care and rely more on home-based care to limit expenses and unstable long-term care (LTC) in China. Thus, services provided by formal care facilities, such as social service agencies and voluntary service organizations, should be accessible to this population.
Correlation of ADL/IADL Disabilities and Depressive Symptoms
This study found that ADL/IADL disabilities significantly increased the risks for depressive symptoms, as evidenced by the adjusted odds ratios of 4.21 and 2.00 after controlling for sociodemographic characteristics, welfare policies, health conditions, and informal care, which confirmed that ADL/IADL disabilities were independent predictors for depression. A plausible explanation is that disabilities impose constraints on elderly people’s ability to perform fundamental but essential activities to fulfill their social roles, and over time, such age-related disorders may induce and aggravate depressive symptoms.36–40 The implication is that elderly people from families with low household incomes who suffer from ADL/IADL disabilities should be given priority for community-based LTC programs to prevent a high prevalence of depression.19
Associated Factors for Depressive Symptoms
This study found no significant difference in the prevalence of depressive symptoms among older adults of different genders. Some studies have reported that gender are risk factors for depressive symptoms, while gender differences are not always shown because of variations in research populations and sampling regions 26,41 Age was inversely associated with depressive symptoms in the logistic regression analysis in this study, similar to previous studies.5,41 This could be explained by the complex interaction of age, age associated risk factors, and depressive symptoms. If the confounding variables were simultaneously controlled, depressive symptoms can potentially be prevented with increased age.42
This study clearly demonstrated that significantly more depressive symptoms were found among those with lower education levels. Educated participants had a lower risk of depression than illiterate participants, which was similar to previous studies.43 Education as an SES variable means more human capital and resources to deal with life events, which might alleviate the negative effects of psychosocial deterioration in later life. A lower education level generally leads to lower self-care awareness, unmet financial need and unhealthier lifestyles, which increase the risks for developing depressive disorders.44
Obstacles to welfare access, which include receiving aid from the government and having a pension or medical insurance, may make older persons vulnerable to depression.45,46 In contrast to previous studies, our findings indicate that there was not a strong aggravating or alleviating effect between welfare and depressive symptoms among the participants. Welfare does not give an advantage to those with financial constraints or weaken the link between socioeconomic resources and health disparities. This indicates that nonmonetary resources may be insufficient for life stresses in this context.
Studies have confirmed that depression in elderly individuals is associated with health status.47 This study found that elderly individuals with poor self-reported health were 1.15 and 2.81 times more likely to have depressive symptoms according to ORs for physical health status. Relevant studies have shown that poor self-rated health imposes activity restriction on older people and contributes to depressive symptoms. In addition, an increasing frequency of disease impairs self-perceived health and causes physical pain and ADL/IADL disabilities, all of which predispose individuals to depression.48,49 In our study, as expected, elderly individuals with chronic diseases were 1.25 and 2.00 times more likely to be depressed than those without chronic diseases.
In this study, the prevalence of depressive symptoms in elderly individuals without satisfactory family emotional support was statistically high. Scarce family emotional support can be an important reason for the poor mental health of elderly people, especially for Chinese older adults who place great emphasis on traditional family values and family ties formed by mutual attachment.50 This finding also corresponds to prior studies indicating that good family relations moderate the impact of stressful events on health and motivate elderly individuals to engage in more health promotion behaviors, subsequently reducing the risk of depressive symptoms.51,52
Strength and Limitations
The strength of this study lies in its being the first of its kind to be conducted in low-income families in Dalian. Previous studies estimating depression in poor Chinese elderly individuals were only conducted among rural residents or defined poor individuals by self-reported income, while our survey sample was chosen from the list of low-income families identified by the Civil Affairs Department. Second, a community-based study design can be considered the most appropriate setting for generalizing the findings to the elderly people of the community, and many potential correlates of depression in elderly individuals were measured in this study. The findings can also contribute to the international literature on late-life depression.
This study has several limitations. First, we conducted a cluster cross-sectional study in Dalian. However, the factors associated with depressive symptoms might be different in other urban areas in China. Future studies need to investigate participants from different parts of China to examine geographic variation and risk factors for depression. Second, the GDS-30 Scale was adopted for screening depressive symptoms; however, the prevalence of depression obtained by the questionnaire was generally higher than that of the study using clinical diagnostic criteria for depression, which may partly explain the high prevalence of depressive symptoms in this study.53 Finally, a cross-sectional study such as ours cannot establish causal relationships among time-varying variables. Future research may determine how these variables interact based on the sequence of time.
Conclusions
We found that depressive symptoms were prevalent among elderly individuals from low-income families in Dalian. For them, depression was significantly associated with education, health condition and emotional support from family, and there may be a specific relationship between ADL/IADL disabilities and depression. These results seem to suggest that older people with a low household income in Dalian face a double “deficit” relating to both economy and health. This highlights the urgent need for more support to be provided to this particular group due to economic and health disparities. Accordingly, welfare systems should be further improved by policy-makers, and programs for populations living in poverty should place greater emphasis on medical and other health-promoting advances to eliminate health inequalities.
Acknowledgments
This work was supported by Social Science Planning Office of Liaoning Province, China (No L21CRK001) and the Educational Department of Liaoning Province, China (No LJKQR2021052). We would like to acknowledge all the subjects who participated in the survey. We are grateful to all reviewers for their valuable suggestions on improving the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bai L, Gu S, Gu H, et al. The impact of disability on intergenerational care needs of the elderly in China. Inquiry. 2021;58:469580211018283. doi:10.1177/00469580211018283
2. Sivertsen H, Bjørkløf GH, Engedal K, et al. Depression and quality of life in older persons: a review. Dement Geriatr Cogn. 2015;40(5–6):311–339. doi:10.1159/000437299
3. Conde-Sala JL, Garre-Olmo J, Calvó-Perxas L, et al. Course of depressive symptoms and associated factors in people aged 65+ in Europe: a two-year follow-up. J Affect Disord. 2019;245:440–450. doi:10.1016/j.jad.2018.10.358
4. Gero K, Kondo K, Kondo N, et al. Associations of relative deprivation and income rank with depressive symptoms among older adults in Japan. Soc Sci Med. 2017;189:138–144. doi:10.1016/j.socscimed.2017.07.028
5. Xu Y, Yang J, Gao J, et al. Decomposing socioeconomic inequalities in depressive symptoms among the elderly in China. BMC Public Health. 2016;16(1):1214. doi:10.1186/s12889-016-3876-1
6. Chen R, Hu Z, Qin X, et al. A community-based study of depression in older people in Hefei, China–the GMS-AGECAT prevalence, case validation and socio-economic correlates. Int J Geriatr Psychiatry. 2004;19(5):407–413. doi:10.1002/gps.1103
7. Ćwirlej-sozańska AB, Sozański B, Wiśniowska-Szurlej A, Wilmowska-Pietruszyńska A. An assessment of factors related to disability in ADL and IADL in elderly inhabitants of rural areas of south-eastern Poland. Ann Agric Environ Med. 2018;25(3):504–511. doi:10.26444/aaem/81311
8. Verropoulou G, Tsimbos C. Disability trends among older adults in ten European countries over 2004–2013, using various indicators and Survey of Health, Ageing and Retirement in Europe (SHARE) data. Ageing Soc. 2016;1:1–31. doi:10.1017/S0144686X16000842
9. Nóbrega JCL, Medeiros JB, Santos TTM, et al. Socioeconomic factors and health status disparities associated with difficulty in ADLs and IADLs among long-lived populations in Brazil: a cross-sectional study. Inquiry. 2021;58:469580211007264. doi:10.1177/00469580211007264
10. He G, Xie JF, Zhou JD, et al. Depression in left-behind elderly in rural China: prevalence and associated factors. Geriatr Gerontol Int. 2016;16(5):638–643. doi:10.1111/ggi.12518
11. Dong Q, Liu JJ, Zheng RZ, et al. Obesity and depressive symptoms in the elderly: a survey in the rural area of Chizhou, Anhui province. Int J Geriatr Psychiatry. 2013;28(3):227–232. doi:10.1002/gps.3815
12. Chan AC. Clinical validation of the Geriatric Depression Scale (GDS): Chinese version. J Aging Health. 1996;8(2):238–253. doi:10.1177/089826439600800205
13. Rong J, Chen G, Wang X, et al. Correlation between depressive symptoms and quality of life, and associated factors For depressive symptoms among rural elderly In Anhui, China. Clin Interv Aging. 2019;14:1901–1910. doi:10.2147/CIA.S225141
14. Brorsson B, Asberg KH. Katz index of Independence in ADL. Reliability and validity in short-term care. Scand J Rehabil Med. 1984;16(3):125–132. doi:10.1249/00005768-198410000-00001
15. Katz SC, Ford AB, Moskowitz RW, et al. Studies of illness in the aged. The index of adl: a standardized measure of biological and psychosocial function. JAMA JAMA-J am Med Assoc. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
16. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. doi:10.1093/geront/9.3_Part_1.179
17. Dong X, Chang ES, Simon MA. Physical function assessment in a community-dwelling population of U.S. Chinese older adults. J Gerontol a Biol Sci Med Sci. 2014;69(2):S31–8. doi:10.1093/gerona/glu205
18. Gong Y, Wen X, Guan C, et al. The associations between family characteristics and depressive symptoms in older adults: a community-based survey in rural China. Int Psychogeriatr. 2012;24(8):1226–1234. doi:10.1017/S1041610211002663
19. Lu J, Zhang L, Zhang K. Care preferences among Chinese older adults with daily care needs: individual and community factors. Res Aging. 2021;43(3–4):166–176. doi:10.1177/0164027520939321
20. Yunming L, Changsheng C, Haibo T, et al. Prevalence and risk factors for depression in older people in Xi’an China: a community-based study. Int J Geriatr Psychiatry. 2012;27(1):31–39. doi:10.1002/gps.2685
21. Cao W, Li L, Zhou X, Zhou C. Social capital and depression: evidence from urban elderly in China. Aging Ment Health. 2015;19(5):418–429. doi:10.1080/13607863.2014.948805
22. Ahmad NA, Abd Razak MA, Kassim MS, et al. Association between functional limitations and depression among community-dwelling older adults in Malaysia. Geriatr Gerontol Int. 2020;20(2):21–25. doi:10.1111/ggi.14012
23. Dominguez J, Fe de Guzman M, Reandelar M, Thi Phung TK. Prevalence of dementia and associated risk factors: a population-based study in the Philippines. J Alzheimers Dis. 2018;63(3):1065–1073. doi:10.3233/JAD-180095
24. Rashid A, Tahir I. The prevalence and predictors of severe depression among the elderly in Malaysia. J Cross Cult Gerontol. 2015;30(1):69–85. doi:10.1007/s10823-014-9248-3
25. Ashe S, Routray D. Prevalence, associated risk factors of depression and mental health needs among geriatric population of an urban slum, Cuttack, Odisha. Int J Geriatr Psychiatry. 2019;34(12):1799–1807. doi:10.1002/gps.5195
26. Li N, Pang L, Chen G, et al. Risk factors for depression in older adults in Beijing. Can J Psychiatry. 2011;56(8):466–473. doi:10.1177/070674371105600804
27. Bartels SJ. Improving system of care for older adults with mental illness in the United States. Findings and recommendations for the President’s new freedom commission on mental health. Am J Geriatr Psychiatry. 2003;11(5):486–497. doi:10.1097/00019442-200309000-00003
28. Ju-K’Ang T. Traditional Chinese beliefs and attitudes toward mental illness. Chinese Culture and Mental Health. 1985;67–81. doi:10.1016/B978-0-12-701630-6.50012-5
29. Dabelko-Schoeny H, Anderson KA, Guada J. Adult day services: a service platform for delivering mental health care. Aging Ment Health. 2013;17(2):207–214. doi:10.1080/13607863.2012.724653
30. Smith PD, Becker K, Roberts L, et al. Associations among pain, depression, and functional limitation in low-income, home-dwelling older adults: an analysis of baseline data from CAPABLE. Geriatr Nurs. 2016;37(5):348–352. doi:10.1016/j.gerinurse.2016.04.016
31. Zeiss AM, Lewinsohn PM, Rohde P, Seeley JR. Relationship of physical disease and functional impairment to depression in older people. Psychol Aging. 1996;11(4):572–581. doi:10.1037//0882-7974.11.4.572
32. Ormel J, Rijsdijk FV, Sullivan M, et al. Temporal and reciprocal relationship between IADL/ADL disability and depressive symptoms in late life. J Gerontol B Psychol Sci Soc Sci. 2002;57(4):P338–47. doi:10.1093/geronb/57.4.p338
33. Qian JH, Wu K, Luo HQ, et al. Prevalence of loss of activities of daily living and influencing factors in elderly population in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2016;37(9):1272–1276. doi:10.3760/cma.j.issn.0254-6450.2016.09.018 Chinese.
34. Zhang L, Zeng Y, Wang L, Fang Y. Urban-rural differences in long-term care service status and needs among home-based elderly people in China. Int J Environ Res Public Health. 2020;17(5):1701. doi:10.3390/ijerph17051701
35. Chen S, Qin J, Li Y, et al. Disability and its influencing factors among the elderly in a County, Guangxi Province, China. Int J Environ Res Public Health. 2018;15(9):1967. doi:10.3390/ijerph15091967
36. Li X, Wang W, Gao Q, et al. The trajectories and correlation between physical limitation and depression in elderly residents of Beijing, 1992–2009. PLoS One. 2012;7(8):e42999. doi:10.1371/journal.pone.0042999
37. Bruce ML. Depression and disability in late life: directions for future research. Am J Geriatr Psychiatry. 2001;9(2):102–112. doi:10.1176/appi.ajgp.9.2.102
38. Geerlings SW, Beekman AT, Deeg DJ, Van Tilburg W. Physical health and the onset and persistence of depression in older adults: an eight-wave prospective community-based study. Psychol Med. 2000;30(2):369–380. doi:10.1017/s0033291799001890
39. Schillerstrom JE, Royall DR, Palmer RF. Depression, disability and intermediate pathways: a review of longitudinal studies in elders. J Geriatr Psychiatry Neurol. 2008;21(3):183–197. doi:10.1177/0891988708320971
40. Penninx BW, Guralnik JM, Ferrucci L, et al. Depressive symptoms and physical decline in community-dwelling older persons. JAMA. 1998;279(21):1720–1726. doi:10.1001/jama.279.21.1720
41. Zhang L, Xu Y, Nie H, et al. The prevalence of depressive symptoms among the older in China: a meta-analysis. Int J Geriatr Psychiatry. 2012;27(9):900–906. doi:10.1002/gps.2821
42. Blazer D, Burchett B, Service C, George LK. The association of age and depression among the elderly: an epidemiologic exploration. J Gerontol. 1991;46(6):M210–5. doi:10.1093/geronj/46.6.m210
43. Xu T, Jiao J, Zhu C, et al. Prevalence and potential associated factors of depression among Chinese older inpatients. J Nutr Health Aging. 2019;23(10):997–1003. doi:10.1007/s12603-019-1270-2
44. Torres JL, da Silva SLA, Lustosa LP. The role of education on the association between disability and depressive symptoms among community-dwelling older adults: Evidence from Frailty in Brazilian Older People (Fibra) study. Arch Gerontol Geriatr. 2019;80:120–124. doi:10.1016/j.archger.2018.11.004
45. Chauhan P, Kokiwar P, Shridevi K, et al. A study on prevalence and correlates of depression among elderly population of rural South India. Int J Community Med Public Health. 2016:236–239. doi:10.18203/2394-6040.ijcmph20151569
46. Li Z, Zhang L. Poverty and health-related quality of life: a cross-sectional study in rural China. Health Qual Life Outcomes. 2020;18(1):153. doi:10.1186/s12955-020-01409-w
47. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5:363–389. doi:10.1146/annurev.clinpsy.032408.153621
48. Arslantas D, Ünsal A, Ozbabalık D. Prevalence of depression and associated risk factors among the elderly in Middle Anatolia, Turkey. Geriatr Gerontol Int. 2014;14(1):100–108. doi:10.1111/ggi.12065
49. Huang CQ, Dong BR, Lu ZC, et al. Chronic diseases and risk for depression in old age: a meta-analysis of published literature. Ageing Res Rev. 2010;9(2):131–141. doi:10.1016/j.arr.2009.05.005
50. Silverstein M, Gong CH, Kendig H. Perceived availability of future care and depressive symptoms among older adults in China: evidence from CHARLS. BMC Geriatr. 2020;20(1):31. doi:10.1186/s12877-020-1435-1
51. Djernes JK. Prevalence and predictors of depression in populations of elderly: a review. Acta Psychiatr Scand. 2006;113(5):372–387. doi:10.1111/j.1600-0447.2006.00770.x
52. Umberson D, Crosnoe R, Reczek C. Social relationships and health behavior across life course. Annu Rev Sociol. 2010;36:139–157. doi:10.1146/annurev-soc-070308-120011
53. Cole MG, Dendukuri N. Risk factors for depression among elderly community subjects: a systematic review and meta-analysis. Am J Psychiatry. 2003;160(6):1147–1156. doi:10.1176/appi.ajp.160.6.1147
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.