Back to Journals » International Journal of Women's Health » Volume 11
Depression symptoms in women with pelvic floor dysfunction: a case-control study
Authors Mazi B ![]() , Kaddour O, Al-Badr A
, Kaddour O, Al-Badr A ![]()
Received 13 September 2018
Accepted for publication 1 February 2019
Published 22 February 2019 Volume 2019:11 Pages 143—148
DOI https://doi.org/10.2147/IJWH.S187417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Baraa Mazi,1 Ouhoud Kaddour,2,3 Ahmed Al-Badr2,4
1National Neurosciences Institute, King Fahad Medical City, Riyadh, Saudi Arabia; 2Research Center, King Fahad Medical City, Riyadh, Saudi Arabia; 3Prince Naif Healthcare Research Center, King Saud University Medical City, Riyadh, Saudi Arabia; 4Urogynecology & Pelvic Reconstructive Surgery Department, Women’s Specialized Hospital, King Fahad Medical City, Riyadh, Saudi Arabia
Purpose: In this study, we aimed to estimate the prevalence of depression symptoms in women with pelvic floor dysfunction (PFD) and to assess their quality of life (QOL).
Patients and methods: A case-control study assessing depression and its severity in women with PFD (urinary incontinence, pelvic organ prolapse, and fecal incontinence) was conducted. Patients attending the Urogynecology Department of the Women’s Specialized Hospital, King Fahad Medical City, were requested to complete the self-reported Pelvic Floor Distress Inventory, Pelvic Floor Impact Questionnaire, and Beck Inventory Scale for Depression. Women presenting with no PFD symptoms were recruited from other clinics as controls.
Results: Data of 100 women diagnosed with PFD (mean age, 45.18±10.50 years) and 100 control participants (mean age, 45.14±13.03 years; P=0.644) were collected. Patients with PFD showed significantly higher (7.3%) body mass index (BMI) (32.59±6.22 kg/m2) than controls (30.37±8.08 kg/m2) (OR, 1.044, 95% CI: 1.001–1.091; P=0.043). Patients with PFD exhibited a threefold higher prevalence of depression symptoms than controls (43% vs 14%, respectively; P<0.001). QOL scores in patients with PFD were significantly higher in patients with depression (P-values, 0.024 to <0.001).
Conclusion: There is a significant association between depression and PFD, and QOL scores in patients with PFD were significantly higher in patients with depression.
Keywords: urinary incontinence, pelvic organ prolapse, fecal incontinence, Saudi Arabia
Introduction
Female pelvic floor dysfunction (PFD) constitutes urinary incontinence (UI), pelvic organ prolapse (POP), and fecal incontinence (FI).1 UI is characterized by the presence of involuntary leakage of urine.2 Some population-based epidemiological studies conducted in Western countries have established a correlation between PFD and multiple factors, including age, parity, obesity, and chronic cough. In a review of 35 studies,3 the median prevalence of UI in women was 27.6% (range, 4.8%–58.4%), with stress urinary incontinence (SUI) accounting for majority of the cases (50%), followed by mixed urinary incontinence (MUI, 32%) and urge urinary incontinence (UUI, 14%).3,4 Reportedly, the mean prevalence of UI in 16 developing countries was 28.7% (range, 5.2%–70.8%), which is similar to that reported in the Western countries.5 In addition, prevalence of UI in developing regions is associated with poor nutrition and hard physical labor.5
FI is characterized by the accidental loss of liquid or solid stool. A meta-analysis of 30 studies has suggested that the FI prevalence – based on the methodology – ranged from 1.4% to 19.5%, with an average of 5.9%.6 A study investigating FI in low- and middle-low-income countries has reported 17% higher prevalence of this condition (range, 5.3%–41%).5 Moreover, several studies have reported the impact of this embarrassing and potentially socially isolating condition on the quality of life (QOL).7 Nevertheless, efforts to determine the community-based prevalence of FI have been challenging since many patients with FI are reluctant to report their symptoms;6 this limitation has led many investigators to assess specific populations, such as postpartum women, or to focus on groups exhibiting potential risk factors, such as delivery type or UI.8,9
POP is a substantial descent of the uterus and vagina, which may protrude partly or entirely beyond the vulva.10 It leads to distressing symptoms, such as pelvic fullness, back pain, incontinence, vaginal discharge, and bleeding.11 Majority of women with bulging of uterus 1 cm beyond the hymen report discomfort.12 The global prevalence of POP has been reported to be between 2% and 20% among women ≤45 years of age.13 However, estimates in developing countries vary extensively, ranging from 3.4% in South India to as high as 56% in Egypt.14,15 Multiparity, chronic health problems increasing abdominal pressure, hard physical labor, difficult first delivery, first delivery at a young age, gynecological complications, and miscarriage are predisposing factors for POP.13,15,16
Despite the high prevalence of PFD, very little is known regarding the effects of this condition on the development of depression in affected women. Studies investigating depression in women with UI have reported high prevalence of depression and panic disorder in this population. Furthermore, these mental health complications markedly affect the reporting of symptoms by patients as well as their QOL and functional status.17,18 One of the first case-control studies investigating depression symptoms in women with POP has demonstrated that patients with prolapse displayed a markedly higher incidence of depression, with symptoms ranging from moderate to severe.19 Importantly, another study has reported evident alleviation in depression symptoms after 6 months of corrective surgery.19 Considering the paucity of data regarding the association between PFD and depression, the primary objective of this study was to ascertain a link between these two clinical entities. In addition, we aimed to identify correlations between depression and severity of PFD symptoms and their impact on QOL. To the best of our knowledge, this is the first study assessing depression in patients with PFD in Saudi Arabia.
Patients and methods
Study design and sample size
This case-control study was conducted at the Urogynecology Department of Women’s Specialized Hospital, King Fahad Medical City– a tertiary care hospital in Riyadh, Saudi Arabia. Sample size was calculated assuming 30%–45% prevalence of PFD and at least twofold increase in incidence of depression in women with PFD, yielding the predicted statistical power of at least 87% and statistical significance of 0.05. Meeting these requirements necessitated the recruitment of 200 candidates – 100 patients with PFD and 100 control participants.
Eligibility criteria
Women ≥18 years of age who were diagnosed with PFD and were symptomatic were included. Women receiving treatment or had undergone surgery for PFD, those with a previous diagnosis of psychiatric illness, and those unable to read or complete the questionnaire owing to cognitive impairments were excluded.
Participants
Patients
From October 2015 to March 2016, all new patients attending the urogynecology clinic for PFD were approached to participate in this study. After being explained regarding the study objectives and methods, all patients provided written informed consent. Furthermore, patients were provided the option of being informed about study results and their psychological score.
Patients underwent standard evaluation as well as general physical and urogynecological examinations including pelvic examination using the POP quantification system as well as the cough stress test. Patients’ medical, surgical, and obstetric histories were noted, and data on age; body mass index (BMI); and symptoms of POP, SUI, overactive bladder (OAB)-wet (OAB with UUI), MUI, or OAB-dry (OAB without UUI) were collected. Inquiries were made by a specialized urogynecologist assisted by residents and interns. Of note, all assessments were based on patient symptoms. QOL was measured using the International Consultation on Incontinence Modular Questionnaire (ICIQ),20 Pelvic Floor Distress Inventory (PFDI), and Pelvic Floor Impact Questionnaire (PFIQ), with higher scores representing worse QOL.
Controls
Women from the waiting areas of gynecology clinics in the same hospital were approached randomly. Women were screened by the researcher for PFD symptoms, and those who answered “No” to the following questions were selected: 1) Do you usually have a sensation of bulging or protrusion from the vaginal area; 2) Do you usually have a bulge or something falling out that you can see or feel in the vaginal area; 3) Have you ever felt something protruding from your vagina; 4) Have you undergone medical or surgical repair for a PFD; 5) Have you been diagnosed with any mental health illness; and 6) Do you have symptoms of inability to control your urine, feces, or bowel contents? Women included in the control group were considered as women with no PFD symptoms, but were not examined to confirm the absence of POP.
Questionnaires
All participants completed the following four questionnaires: PFDI, PFIQ, ICIQ, and Beck Depression Inventory-II (BDI-II). Although all questionnaires were self-reported, an interviewer was available for any questions or clarifications. After solving the queries, participants were left alone or with the next of kin in a room to ensure privacy.
BDI-II is a 21-question, multiple-choice, self-report inventory, which is one of the most widely used tools for assessing the likelihood of having depression.21,22 In the current version, the questionnaire is designed for individuals ≥13 years of age and comprises items related to symptoms of depression (hopelessness and irritability), cognitions (guilt or feelings of being punished), and physical condition (fatigue, weight loss, and lack of interest in sex). A validated Arabic translation of BDI was used in this study.23 The results were segregated into two categories according to BDI-II scores: scores of 1–10 (normal), 11–16 (mild mood disturbance), and 17–20 (borderline clinical depression) were considered as “non-depressed” patients, whereas scores of 21–30 (moderate depression), 31–40 (severe depression), and >40 (extreme depression) were considered as “clinical depression.”
Statistical analyses
A specialized psychiatrist and a psychologist calculated and analyzed the results. Categorical variables, including social status, education, employment, and parity, are presented as numbers and percentages; continuous variables, including age, weight, height, BMI, and pelvic function scores, are expressed as a mean and SD. Chi-squared and Fisher’s exact tests (for expected cell frequency <5) were used to evaluate the significance of correlation among categorical variables. ANOVA or independent sample t-test was used to ascertain mean significant difference between pelvic scores and depression symptoms. Binary and multiple logistic regressions were used to determine the most important predictors of pelvic disorders among patients with depression. A P<0.05 was considered statistically significant. All statistical analyses were performed using the statistical package SPSS version 22.
Results
Table 1 summarizes clinical and demographic characteristics of the two groups. Data of patients with (n=100) and without PFD (controls; n=100) were collected. Mean age, parity, and past medical history of patients with PFD and that of controls were similar. BMI was significantly higher in the PFD group compared to the control group (7.3%; 32.59±6.22 vs 30.27±8.08; P=0.043). The prevalence of depression symptoms was nearly threefold higher in the PFD group than in the control group (43% vs 14%; P<0.001).
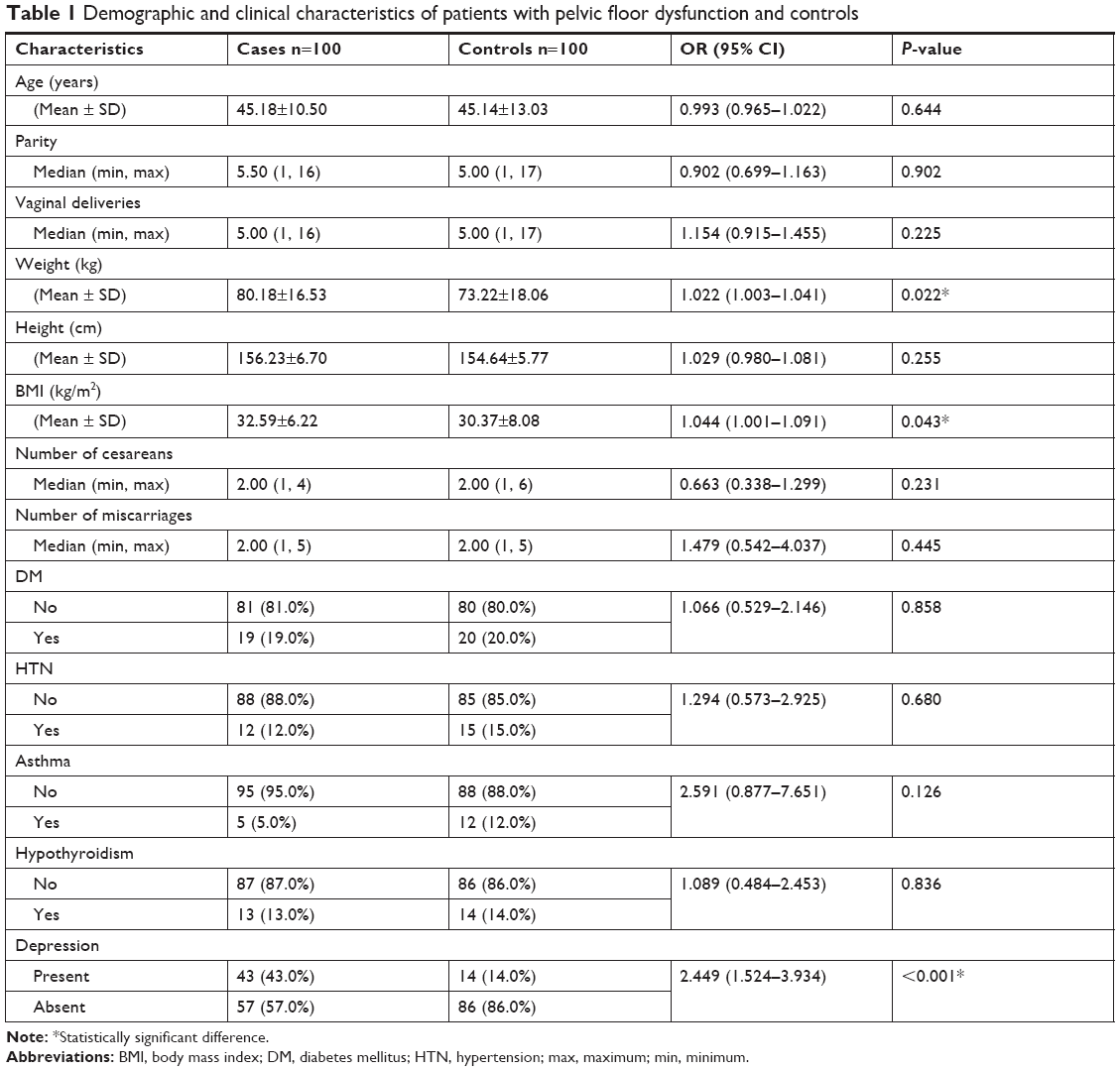 | Table 1 Demographic and clinical characteristics of patients with pelvic floor dysfunction and controls |
QOL scores in patients with PFD (ICIQ, Pelvic Organ Prolapse Distress Inventory, Colorectal-Anal Distress Inventory, Urogenital Distress Inventory, PFDI, Urinary Impact Questionnaire, Colorectal-Anal Impact Questionnaire, Pelvic Organ Prolapse Impact Questionnaire, and PFIQ) were significantly higher (worse symptoms) in patients with depression (P-values, 0.024 to <0.001; OR, 1.02 (PFIQ score) to 1.078 (ICIQ score); Table 2).
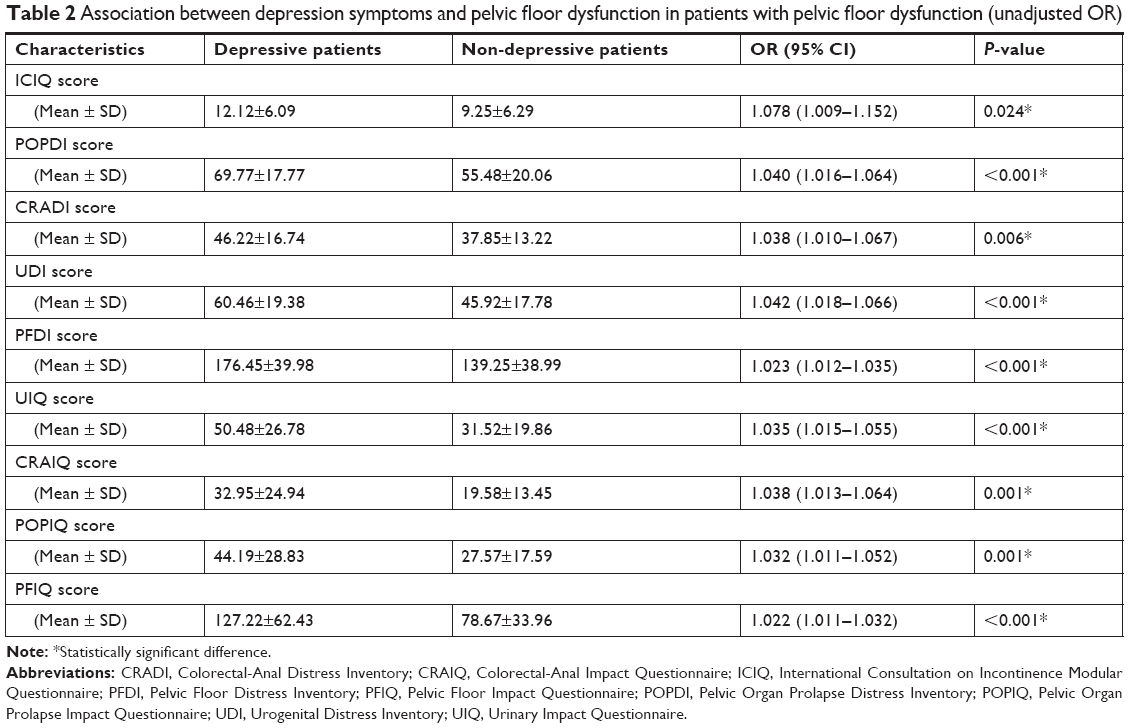 | Table 2 Association between depression symptoms and pelvic floor dysfunction in patients with pelvic floor dysfunction (unadjusted OR) |
Multiple logistic regression revealed that BMI (OR, 1.032; 95% CI: 1.000–1.077; P=0.047) was the most significant risk factor for depression.
Discussion
The seminal finding of the present study is that women seeking treatment for PFD exhibit a threefold higher prevalence of depression symptoms compared with women without PFD. According to BDI-II scores, depression in our study population ranged from mild to severe. In a study on UI, Zorn et al, for the first time, have proposed a correlation between PFD and depression.24 Although they only investigated UI, the probability of depression was approximately twofold higher in patients with UI – a value similar to that reported in the present study. In addition, low serotonin levels may be the common cause underlying depression and UI, providing a mechanistic explanation for the frequent co-occurrence of these two disorders. Similarly, a large-scale study in Norwegian population has reported a 2.09-fold increased probability of depression among women with UI.25,26 Our findings suggest that PFD is the major risk factor for depression since affected women exhibited fewer other medical conditions such as hypothyroidism, which leads to depression.27 Mechanistically, a correlation between depression and PFD may be bidirectional as changes in neurotransmitter functions, which cause depression, can affect the innervation of the bladder as well.28
Contrary to the conclusions of abovementioned studies, Yip et al have established that, after adjusting for confounders9 such as presence of depression, women experiencing UI on a daily basis were only 22% more likely to experience depressive episodes. Nevertheless, they noted that these patients were three times more likely to experience loneliness, which alone was reported to promote depressive states in the Western population.29 In addition, patients with PFD who underwent surgical intervention or physiotherapy exhibited poor response in the presence of depression symptoms.30 Of note, some studies have suggested that the presence of UI does not predict the development of depression at a later time point.31 Therefore, there may be multiple causes underlying the correlation between PFD and depression, warranting further investigation in this regard.
Based on the accumulated data, we can hypothesize that QOL and severity of PFD contribute to the likelihood of having depression symptoms and that patients cannot cope with consequences of PFD because of their depression. Disruption of this vicious cycle should be a priority of therapeutic efforts. In addition, depression may contribute to the worsening of PFD because depressed women may not be able to take care of their physical health, such as by not performing the Kegel muscle exercises. Moreover, increased parity affects the severity of depression symptoms, which can be explained by the increased burden of responsibilities on these women. Therefore, further studies are warranted to address age-associated differences in depression symptoms among women with PFD.
This study has some limitations. This was a single-center study conducted at a tertiary care referral hospital. In Saudi Arabia, only 19.5% of the women are unemployed;32 however, 77.9% of the women included in this study were unemployed; this fourfold difference may have acted as a confounder. Moreover, BMI of the participants was high, which limits the generalization of our results to other populations, although they reflect the higher-than-average BMI of the Saudi Arabian population. Indeed, our findings cannot be further generalized even to the entire Saudi Arabian population as the hospital receives referrals from across the country. Finally, we encountered recruitment difficulty owing to the sensitivity of the questionnaire used.
Conclusion
Our findings strongly support the hypothesis that depression and PFD are correlated, highlighting the fact that women with PFD require additional attention from their health care providers owing to their high probability of suffering from depressive disorders. Moreover, QOL scores in patients with PFD were significantly higher in patients with depression. To the best of our knowledge, this is the first study investigating depression in Saudi Arabian women with PFD, and our findings may impact the type of services provided to the community in near future. Hopefully, this study will prompt further research in this field in Saudi Arabia and other countries in the region. We believe that our findings will improve patient care by ensuring better appreciation of the extent of this problem, which can further change the manner of handling of such cases, ultimately improving referral systems and introducing novel interventions for this population.
Ethical approval and informed consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The King Fahad Medical City Institutional Review Board approved the study protocol. Informed consent was obtained from all participants included in the study.
Acknowledgment
This study was supported by a grant from King Fahad Medical City (IRF 015-002).
Disclosure
The authors report no conflicts of interest in this work.
References
Sung VW, Hampton BS. Epidemiology of pelvic floor dysfunction. Obstet Gynecol Clin North Am. 2009;36(3):421–443. | ||
Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the international continence society. Urology. 2003;61(1):37–49. | ||
Minassian VA, Drutz HP, Al-Badr A. Urinary incontinence as a worldwide problem. Int J Gynaecol Obstet. 2003;82(3):327–338. | ||
Al-Badr AH, Kamil AG, Wahbah EF, Zimmerman VA, Al-Tannir MA. Characteristics of women attending a urogynecology clinic in Riyadh. Saudi Med J. 2010;31(1):86–87. | ||
Walker GJA, Gunasekera P. Pelvic organ prolapse and incontinence in developing countries: review of prevalence and risk factors. Int Urogynecol J. 2011;22(2):127–135. | ||
Sharma A, Yuan L, Marshall RJ, Merrie AE, Bissett IP. Systematic review of the prevalence of faecal incontinence. Br J Surg. 2016;103(12):1589–1597. | ||
Saldana Ruiz N, Kaiser AM. Fecal incontinence – Challenges and solutions. World J Gastroenterol. 2017;23(1):11–24. | ||
Melville JL, Fan MY, Newton K, Fenner D. Fecal incontinence in US women: a population-based study. Am J Obstet Gynecol. 2005;193(6):2071–2076. | ||
Yip SO, Dick MA, McPencow AM, Martin DK, Ciarleglio MM, Erekson EA. The association between urinary and fecal incontinence and social isolation in older women. Am J Obstet Gynecol. 2013;208(2):146.e1–146.e7. | ||
Haylen BT, Maher CF, Barber MD, et al. An International Urogynecological Association (IUGA)/International Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Neurourol Urodyn. 2016;35(2):137–168. | ||
Aoyama A [webpage on the Internet]. Reproductive health in the Middle East and North Africa: well-being for all. The world bank; 2000. Available from: https://openknowledge.worldbank.org/handle/10986/13952. Accessed November 2, 2017. | ||
Ghetti C, Gregory WT, Edwards SR, Clark AL. Pelvic organ descent and the perception of prolapse. Am J Obstet Gynecol. 2005;193:53–57. | ||
Bonetti TR, Erpelding A, Pathak LR. Reproductive morbidity – a neglected issue? A report of a clinic-based study held in far-western Nepal. Kathmandu: Nepal Ministry of Health; 2002. | ||
Bhatia JC, Cleland J, Bhagavan L, Rao NSN. Levels and determinants of gynecological morbidity in a district of South India. Stud Fam Plann. 1997;28(2):95–103. | ||
Younis N, Khattab H, Zurayk H, et al. A community study of gynecological and related morbidities in rural Egypt. Stud Fam Plann. 1993;24(3):175–186. | ||
Rogers RG, Fashokun TB [database on the Internet]. Pelvic organ prolapse in women: epidemiology, risk factors, clinical manifestations, and management. Wolters Kluwer health/UpToDate; 2017. Available from: www.uptodate.com/contents/pelvic-organ-prolapse-in-women-epidemiology-risk-factors-clinical-manifestations-and-management. Accessed November 2, 2017. | ||
Melville JL, Walker E, Katon W, et al. Prevalence of comorbid psychiatric illness and its impact on symptom perception, quality of life, and functional status in women with urinary incontinence. Am J Obstet Gynecol. 2002;187(1):80–87. | ||
Bovbjerg VE, Trowbridge ER, Barber MD, et al. Patient-centered treatment goals for pelvic floor disorders: association with quality-of-life and patient satisfaction. Am J Obstet Gynecol. 2009;200(5):568.e1–568.e6. | ||
Ghetti C, Lowder JL, Ellison R, Krohn MA, Moalli P. Depressive symptoms in women seeking surgery for pelvic organ prolapse. Int Urogynecol J. 2010;21(7):855–860. | ||
Al-Shaikh G, Al-Badr A, Al Maarik A, Cotterill N, Al-Mandeel HM. Reliability of Arabic ICIQ-UI short form in Saudi Arabia. Urol Ann. 2013;5(1):34–38. | ||
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4(6):561–571. | ||
Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of Beck depression inventories-IA and-II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. | ||
West J. An Arabic validation of a depression inventory. Int J Soc Psychiatry. 1985;31(4):282–289. | ||
Zorn BH, Montgomery H, Pieper K, Gray M, Steers WD. Urinary incontinence and depression. J Urol. 1999;162(1):82–84. | ||
Felde G, Bjelland I, Hunskaar S. Anxiety and depression associated with incontinence in middle-aged women: a large Norwegian cross-sectional study. Int Urogynecol J. 2012;23(3):299–306. | ||
Felde G, Ebbesen MH, Hunskaar S. Anxiety and depression associated with urinary incontinence. A 10-year follow-up study from the Norwegian HUNT study (EPINCONT). Neurourol Urodyn. 2017;36(2):322–328. | ||
Dayan CM, Panicker V. Hypothyroidism and depression. Eur Thyroid J. 2013;2(3):168–179. | ||
Melville JL, Delaney K, Newton K, Katon W. Incontinence severity and major depression in incontinent women. Obstet Gynecol. 2005;106(3):585–592. | ||
Blazer DG. Depression and social support in late life: a clear but not obvious relationship. Aging Ment Health. 2005;9(6):497–499. | ||
Khan ZA, Whittal C, Mansol S, et al. Effect of depression and anxiety on the success of pelvic floor muscle training for pelvic floor dysfunction. J Obstet Gynaecol. 2013;33(7):710–714. | ||
Melville JL, Fan MY, Rau H, Nygaard IE, Katon WJ. Major depression and urinary incontinence in women: temporal associations in an epidemiologic sample. Am J Obstet Gynecol. 2009;201(5):490.e1–490.e7. | ||
The World Bank [webpage on the Internet]. Unemployment, female (% of female labor force) (modeled ILO estimate); 2017. Available from: https://data.worldbank.org/indicator/SL.UEM.TOTL.FE.ZS?view=map. Accessed January 15, 2018. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.