Back to Journals » Risk Management and Healthcare Policy » Volume 14
Dental Professional’s Knowledge, Preventive Awareness and Attitude Towards COVID-19 in Saudi Arabia: A Cross-Sectional Survey
Authors Alwazzan RA, Baseer MA ![]() , ALMugeiren OM, Ingle NA
, ALMugeiren OM, Ingle NA
Received 29 January 2021
Accepted for publication 9 May 2021
Published 1 June 2021 Volume 2021:14 Pages 2277—2288
DOI https://doi.org/10.2147/RMHP.S303858
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Rayyan Abdallah Alwazzan, Mohammad A Baseer, Osamah Mohammed ALMugeiren, Navin Anand Ingle
Department of Preventive Dentistry, College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia
Correspondence: Mohammad A Baseer
Department of Preventive Dentistry, College of Dentistry, Riyadh Elm University, Namuthajiya Campus, PO Box No. 84891, Riyadh, 11681, Saudi Arabia
Email [email protected]
Background: Given the COVID-19 pandemic, it is necessary to assess the dentist’s knowledge, preventive awareness, and attitude towards COVID-19 in Saudi Arabia. This study aimed to assess dental professionals’ knowledge, preventive awareness, and attitude towards dental care during the COVID-19 pandemic in Saudi Arabia.
Study Subjects and Methods: The study participants consisted of dental professionals working in government, private and academic sectors in Saudi Arabia. An online questionnaire (Whatsapp and Twitter) was sent to dental professionals in July 2020. The questionnaire consisted of questions on dental professional’s demographic variables, their knowledge of the incubation period, the symptoms, mode of transmission, preventive awareness of COVID-19, and their attitude toward treating patients with COVID-19. Mann–Whitney U and Kruskal–Wallis tests were applied to compare mean ranks and a p< 0.05 is considered statistically significant.
Results: This study included a total of 356 dental professionals (dentists and dental students) aged 22– 60 years (mean±SD, 32.14± 7.48 years). Majority of the participants were graduates/general practitioners (GP) 145 (40.7%), followed by post graduate (PG) student 108 (30.3%), undergraduate students 23 (6.5%) and specialist 80 (22.5%). Dental professionals showed a high level (> 90% correct responses) of knowledge of COVID-19 except for the infection among comorbid patients 283 (79.5%) and incubation period of COVID-19, 164 (46.1%). An overall high knowledge of COVID-19 (87.26%), preventive awareness (88.64%) and a positive attitude (65.26%) towards dental care were observed among the study participants. The mean knowledge ranks differed significantly in different genders (p=0.029) and marital status (p=0.023), whereas preventive awareness differed significantly across various qualifications (p=0.004). The mean attitude rank was significantly higher among Saudi (182.29) compared to non-Saudi (141.36) study participants (p=0.025).
Conclusion: The dental professionals participated in this study demonstrated adequate knowledge of symptoms, preventive awareness, and a positive attitude towards dental care of the COVID-19 infected patients.
Keywords: attitude, awareness, COVID-19, dental professional, knowledge
Introduction
Corona Virus Disease 19 (COVID-19) is a recently identified viral infection that originated in Wuhan, China, and triggered a pneumonia epidemic in the rest of the world.1 It seems that the quickly circulating virus is more infectious than Severe Acute Respiratory Syndrome (SARS-CoV) and Middle East Respiratory Syndrome (MERS-CoV).2 The disorder is triggered by severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2)3 and is believed to be transmitted from human to human in various ways, including droplets, aerosols, and fomites.4 Globally, as of April 20, 2021, there have been 141,754,944 confirmed cases of COVID-19, including 3,025,835 deaths, reported to World Health Organization (WHO). A survey conducted among 2195 licensed dentists in United States of America in June-2020 found that 20 dentists had contracted COVID-19.4
COVID-19 infection induces severe respiratory disease, with fever, cough, myalgia, and exhaustion as typical signs at the start of the disease.5,6 Organisms causing infection, can spread from their particular habitat to a susceptible host in various pathways. Viral spread may occur by human-human transmission, airborne transmission, and other forms of dissemination, such as endogenic virus, and vector spread.7 However, certain respiratory viruses are known to be spread through several channels, in which the transmission mechanisms in droplets and aerosols are of primary importance, but their role in the transmission of the disease remains uncertain.7,8
Respiratory particles may be classified as droplets or aerosols depending on particle size and aerodynamic diameter.9 There is no evidence of the least infectious viral load for the COVID-19 pandemic, although several researchers suspect that a few hundred SARS-CoV-2 viruses would enough to induce disease among susceptible hosts.10 People infected with COVID-19 can transmit viral particles anytime they speak, smoke, cough, or sneeze. Such viral particles are likely to be encapsulated in globs of mucus, saliva, and water, and globs behavior in the atmosphere depends on its size. Big-sized globs sink quicker than they evaporate, splashing in droplets nearby.11
Many medical workers contracted the disease while working with COVID-19 infected patients.12 The dental clinic is no exception to a relative probability of sharing and contracting the infection between dental staff or patients, although the dental clinic may be a more dangerous place for the spread of the virus due to close interaction with patients and the type of dental care.13 Often, extended disease incubation up to 14 days before any symptoms are identified, and the post-infection phase challenges medical staff to identify the COVID-19 patients.12
Hence, COVID-19 infected patients without showing symptoms are a significant threat to dentists and other dental team members. Therefore, dentists should exercise a high level of awareness and integrity to deal with the disease and control and manage its spread.14 Because of this, the ministry of health issued a dental emergency protocol during the COVID-19 pandemic that recommended only urgent/emergency dental care of the patients with a high infection control level in dental treatment. The recommendation included postponing all the elective dental treatment until further notification.13
Like any other contagious infection prevention guidelines, COVID-19 prevention recommendations included personal protective equipment, hand wash, detailed patient evaluation, rubber dam isolation, anti-retraction handpiece, mouth rinsing before dental procedures, and disinfection of the clinic. Besides, some guidelines and reports had provided useful information about the signs and symptoms of the disease, ways of transmission, and referral mechanisms, to increase dentists’ knowledge and prevention practices so they could contribute at a population level to disease control and prevention.15,16
Recent studies have indicated adequate knowledge, attitude, and practices towards COVID-19 prevention and control among dentists. In contrast, gaps in taking extra precautions of specific dental procedures in the context of the current outbreak and disinfection protocols have been identified.14–16 The Ministry of Health (MOH) in Saudi Arabia reacted promptly to this pandemic by following World Health Organisation (WHO) guidance and issuing dental practice guidelines, which were widely circulated and published on the ministry website.13 Given these guidelines, it is necessary to assess the dentist’s knowledge, preventive awareness, and attitude towards COVID-19 to strengthen prevention and control measures within the dental practice.
Therefore, this cross-sectional study aimed to assess dental professionals’ knowledge, preventive awareness, and attitude towards dental care during the COVID-19 pandemic in Saudi Arabia.
Materials and Methods
Study Design and Participants
This cross-sectional survey was conducted in July 2020. Study participants consisted of dental students and dentists working in Saudi Arabia regardless of their nationality or workplace. Dentists and dental students registered under the Saudi Dental Society were accessed through social media platforms (Twitter and WhatsApp).
Ethical Approval
The research proposal submitted to the Riyadh Elm University Research Centre, with registration number FPGRP/2020/473/223 and approved by the Institutional Review Board FPGRP/2020/473/223/219. All the participants were informed about the purpose and scope of the study. Online written consent was obtained before completing the survey and respondents were informed that their participation in the study was completely voluntary. Those who agreed to participate were included in the study. The questionnaire was anonymous to protect the integrity and confidentiality of the information. This study was conducted in accordance with the Declaration of Helsinki.
Sample Size Calculation
A minimum sample size of 356 dental professionals were calculated by considering the margin of error 5%, confidence interval of 95%, and a total of 16,887 licensed dental professionals in Saudi Arabia as was reported by Al Baker et al (2017)17 with expected 64% response distribution from active members on social media.18 A convenience sampling methodology was utilized to recruit dental professionals in Saudi Arabia based on ease of availability during the survey period. RaoSoft online sample size calculator was used to estimate the required sample.
Questionnaire Development, Design, and Administration
A structured, closed-ended, and self-administered questionnaire consisting of 25 items and demographic information was prepared and administered to the study participants. Questions of the survey were developed after reviewing published literature and the guidelines issued by the Centre for Disease Control and health ministry, Saudi Arabia, towards COVID-19. The validity of the questionnaire was established by obtaining an expert opinion from the dental public health faculty. The expert gave their concerns about the ease, relativity, and importance of the instrument. The questionnaire was pretested by recruiting ten dentists, who gave their feedback on the questionnaire. The study instrument demonstrated adequate reliability, as indicated by Cronbach’s alpha (0.798).
An online questionnaire was prepared by utilizing google forms. This questionnaire’s online link was made available on social media platforms (Twitter and WhatsApp) associated with the dental professional groups in Saudi Arabia. The questionnaire was divided into four parts. The first part included the respondents’ demographic information (gender, experience, health sector, nationality, qualification, and marital status).
The second part consisted of 11 items that explored the study participants’ knowledge about the symptoms and spread of the COVID-19. The questionnaire included items on the development of severe acute respiratory illness, hallmark symptoms of disease, comorbid people likely getting an infection, incubation period, the spread of infection through close contacts, spread in dental clinics, availability of the vaccine, use of antibiotics as first-line treatment, fatality, dangerous infection and public concern of COVID 19. Each item’s responses in the knowledge section were recorded and classified as either correct or incorrect. Every correct answer was scored one and incorrect answer 0. Therefore, knowledge was scored on a scale ranging from 0–11, with a higher score indicating better knowledge of COVID 19 among dental professionals. A Cronbach’s alpha value of 0.763 was observed with knowledge items.
The third part included five items on preventive awareness of the COVID-19. The questionnaire items on dental emergency protocol during the COVID-19 pandemic, awareness of universal precautions and infection control measures, transmission prevention in dental clinics, frequent cleaning of hands, and wearing the mask were assessed. Every correct answer was scored 1, and an incorrect answer 0. Therefore, preventive awareness scores ranged between 0–5, with a higher score indicating a better preventive awareness of COVID 19 among dental professionals. A Cronbach’s alpha value of 0.833 was observed with preventive awareness items.
The fourth part included seven items that assessed dental professional’s attitudes towards the patient’s dental care during the pandemic. The questionnaire items included dental professional’s attitudes towards the treatment of patients diagnosed or suspected of COVID-19, emergency dental treatment of diagnosed patients, postponement of routine/elective dental treatment for all patients, referral of sneezing or coughing patients and allowing the staff to work with patients having flu-like symptoms, and the role in spreading COVID 19 awareness information. Every correct answer was scored 1, and an incorrect answer 0. Therefore, attitude scores ranged between 0–7, with a higher score indicating a positive attitude of dental professionals towards patient’s dental care during the pandemic. A Cronbach’s alpha value of 0.798 was observed with attitude items.
Statistical Analysis
A Shapirowilk’s test (p<0.05) and visual examination of the histograms indicated the non-normal distribution of the data. Descriptive statistics on frequency distribution and percentages have been determined for categorical variables. Mean, median and inter quartile ranges and mean ranks were calculated for continuous variables (knowledge, awareness, and attitude). Non-parametric tests of Mann–Whitney U were used to compare the mean ranks between gender, nationality, and marital status. Whereas the Kruskal–Wallis test was used to compare mean ranks between different experiences, health sector, and qualification categories of study participants. Bivariate and multivariable analysis were performed for the factors associated with knowledge, attitude and practice. All data were analyzed using IBM-SPSS (version 25 Armonk, NY: USA). A value of p<0.05 was considered to be significant for all statistical tests.
Results
A total of 356 subjects aged 22–60 years (mean±SD, 32.14±7.48 years) participated in this study. The majority of the 212 (59.6%) participants were males 150 (42.1%), having < 5 years of experience. A large proportion of 223 (62.6%) of the study subjects worked in the government health sector. Most of the 323 (90.7%) participants were Saudi nationals with graduate/GP 145 (40.7%) dentistry qualification. More than half of the 209 (58.7%) of the subjects were married and 147 (41.3%) were unmarried/single (Table 1). Participants in this study demonstrated a mean, median and inter quartile ranges for knowledge (9.69, 10 and 9–10), preventive awareness (4.43, 5 and 4–5) and attitude (4.88, 5 and 4–6) scores towards COVID 19.
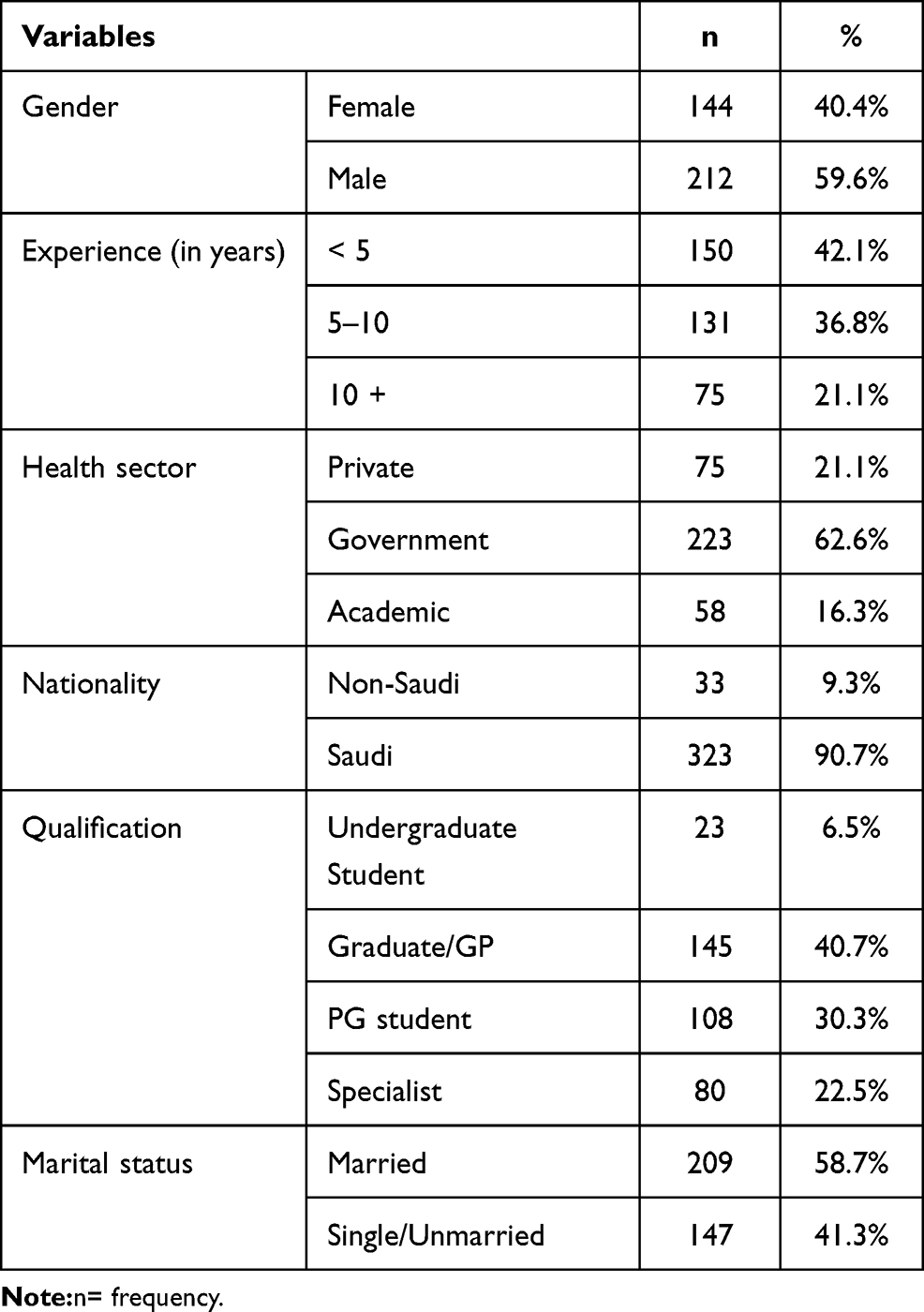 |
Table 1 Demographic Characteristics of the Study Participants (N=356) |
Distribution of the responses to the Knowledge items of COVID-19 is displayed in (Table 2). A very high percentage (more than 90%) of correct responses were observed for the items: COVID-19 patients can develop severe acute respiratory illness, fever, dry cough, and shortness of breath are hallmark symptoms of COVID-19, COVID-19 spread through close contact with infected persons, vaccination of COVID-19 is available in the market, COVID-19 can be fatal, dental patients suffering from COVID-19 can spread infection in dental clinics, do you think that COVID-19 is a dangerous infection, COVID-19 is a serious public health issue. However, less than half of the participants 164 (46.1%) correctly answered the exact incubation period of COVID-19. Multiple response analyses on knowledge of COVID-19 symptoms showed that the subjects were aware of fever (17.3%), cough (17%), shortness of breath (16.5%) followed by other symptoms, as shown in (Figure 1). An overall high knowledge (87.26%) of COVID-19 was observed among the study participants.
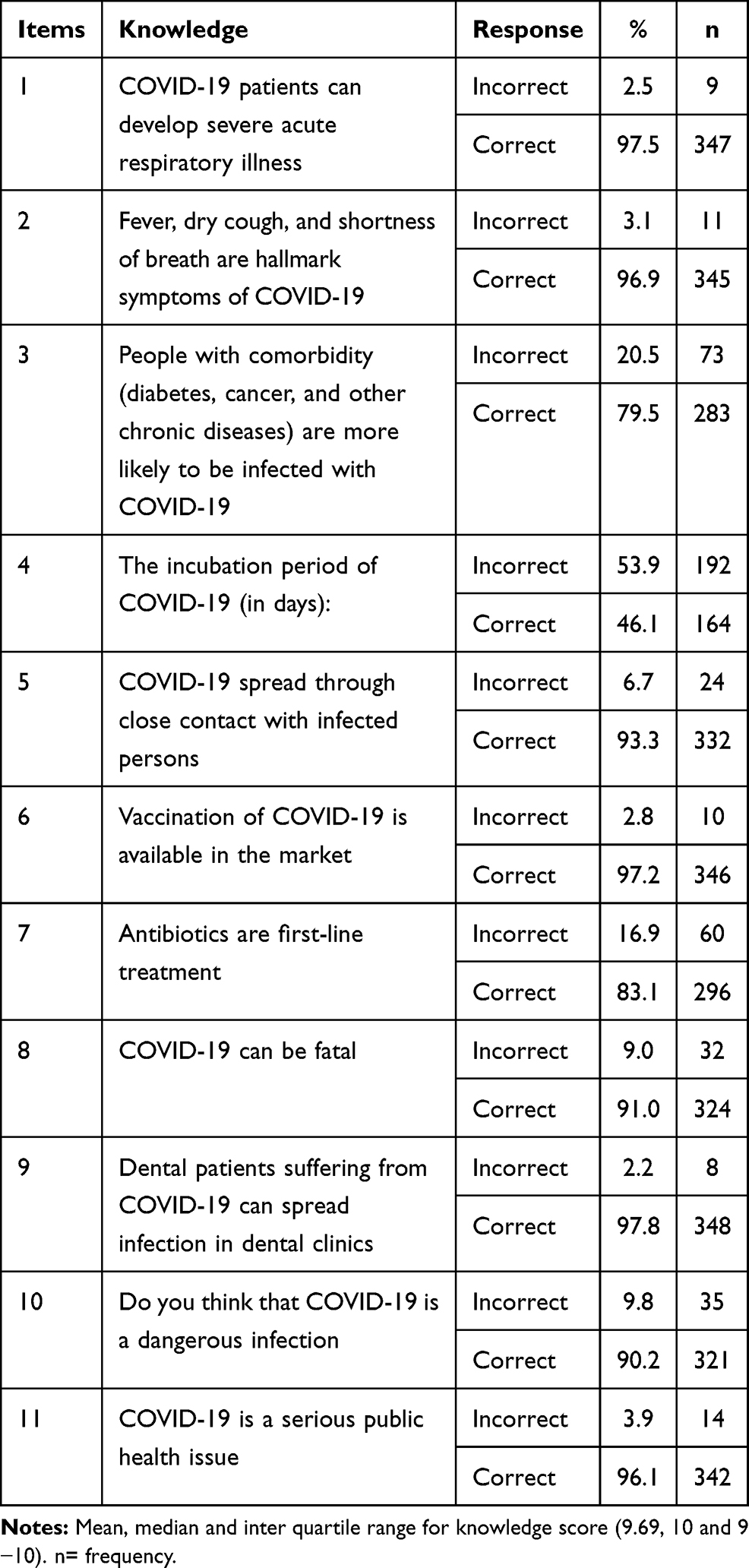 |
Table 2 Distribution of the Responses to the Knowledge of COVID-19 |
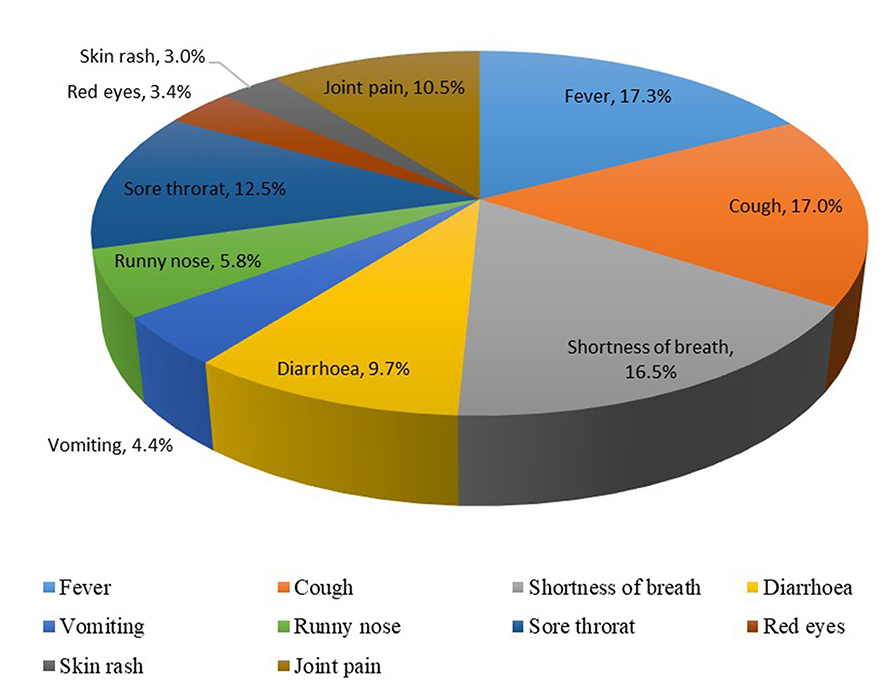 |
Figure 1 Knowledge of symptoms of COVID-19 among study subjects (Responses=2022). |
The preventive awareness of COVID-19 among the study participants was evaluated via a set of questions. Results showed that the majority (96.9%) of participants were conscious of regular hand-cleaning by utilizing alcohol-based hand rub or soap and water (item 4) and usage of a mask by the patient while in the workplace (96.1%) (item 5). Dental emergency protocol during the COVID-19 pandemic published by the Saudi ministry of health (84%) (Item 1), prevention of transmission of COVID-19 infection by using universal precautions given by the Centre for Disease Control, World Health Organization, American Dental Association, (83.1%) (Item 3) and universal precautions and infection control measures carried out by dentists for preventing COVID-19 in the dental office given by the Centre for Disease Control, World Health Organization, American Dental Association (83.1%) (Item 2) are well aware among study participants as shown in (Table 3). An overall high preventive awareness (88.64%) was observed among the study participants.
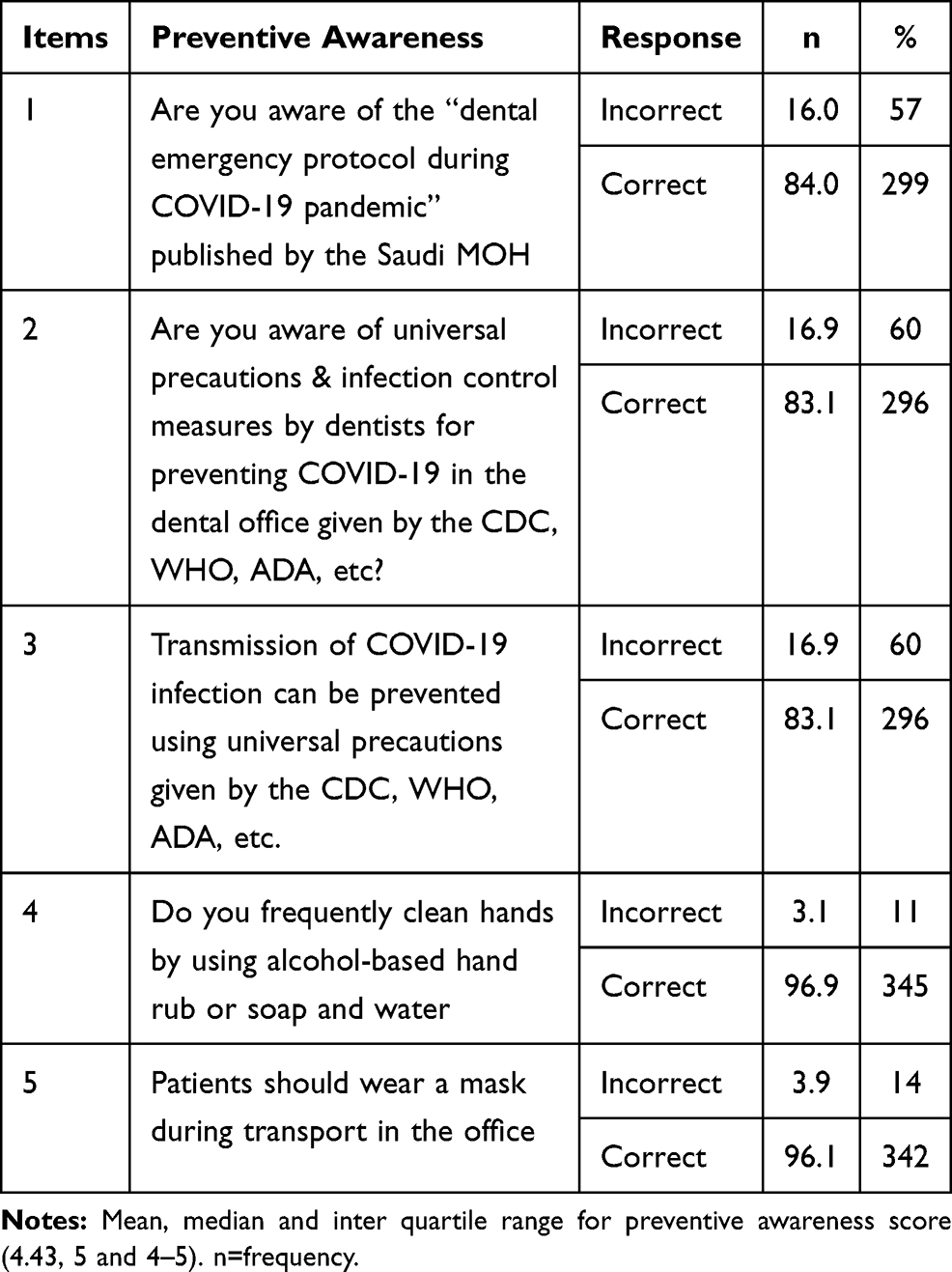 |
Table 3 Preventive Awareness of COVID-19 Among Study Participants |
Multiple response analysis showed that a large percentage of the study subjects agreed to wear gowns (20.30%), gloves (20.10%), masks (20.10%), face shield (20%), and goggles (17.80%) as a preventive measure of COVID1-19 in dental practice as shown in (Figure 2).
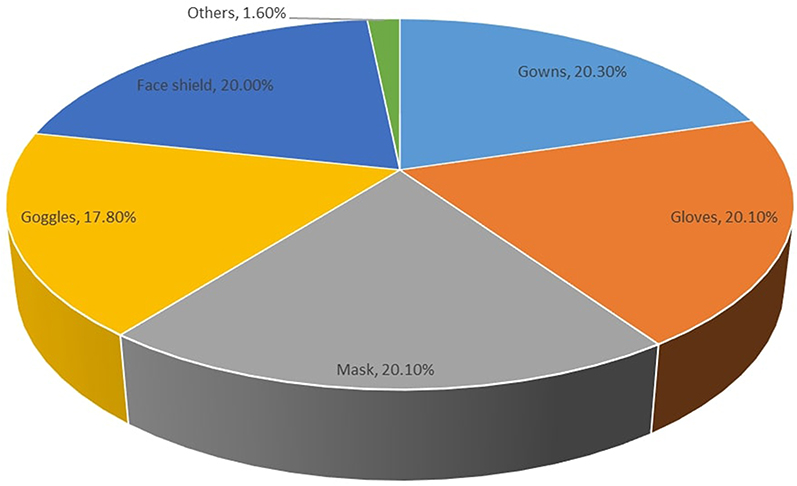 |
Figure 2 Preventive measures of COVID-19 in dental practice (Responses=1718). |
Study participants’ attitude towards the dental care of COVID-19 patients is displayed in (Table 4). A high percentage of study participants correctly answered the attitude item 3 (85.1%) (Will you provide only emergency dental treatment to COVID-19 diagnosed patients) and item 7 (83.4%) (Your role in spreading COVID 19 information and increasing awareness significant). The lowest correct responses were observed for item 4 (31.7%) (Will you postpone routine/elective dental treatment and procedures for all patients), followed by others. An overall a positive attitude (65.26%) towards dental care were observed among the study participants.
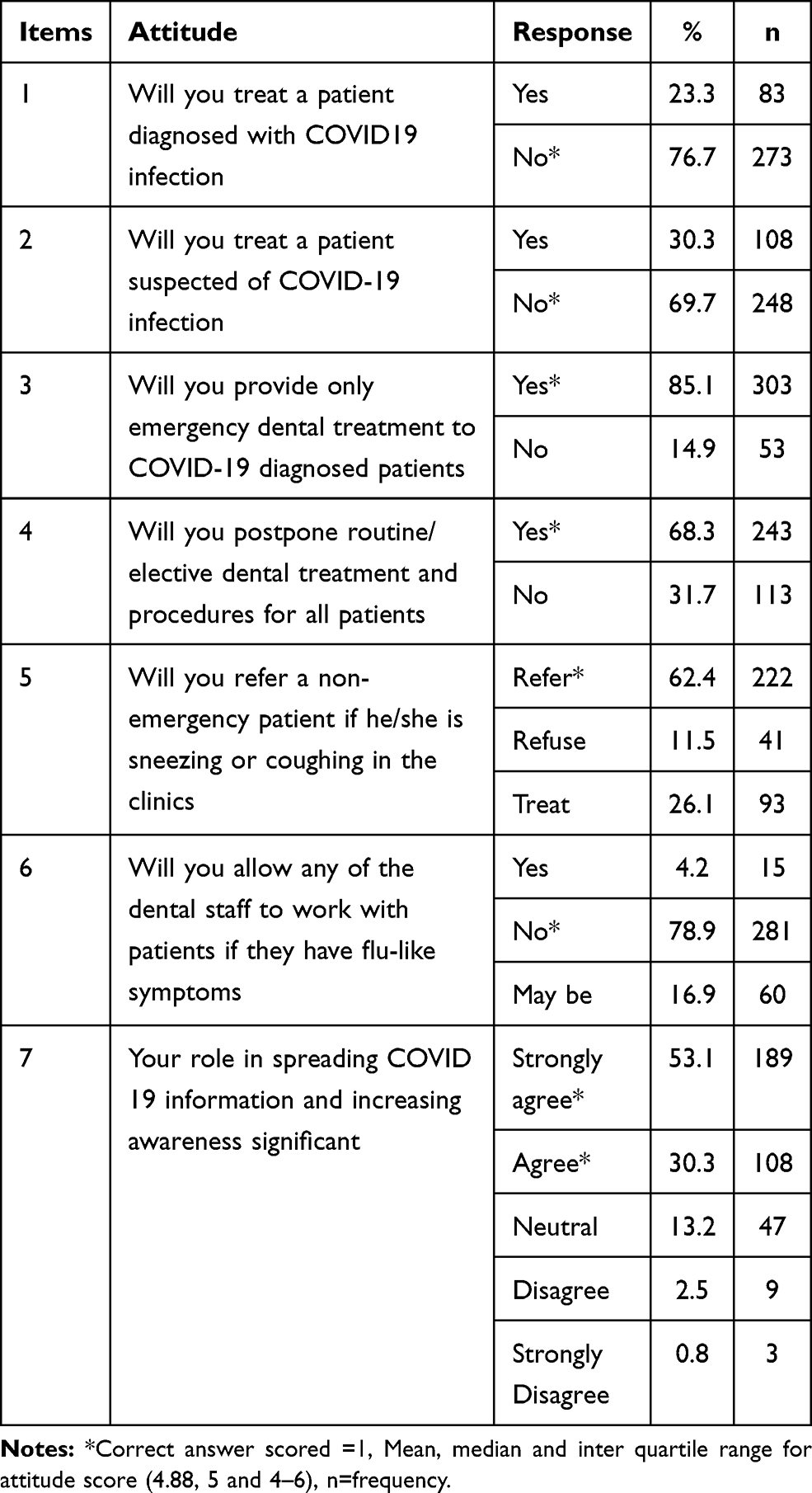 |
Table 4 Attitude of Study Participants Towards COVID-19 Patients Dental Care |
The gender and marital status were significantly associated with the mean knowledge ranks p<0.05. Female (192.06 vs.169.29, p=0.029) dental professionals demonstrated significantly higher knowledge ranks than the male dental professionals. Similarly, married (188.29 vs 164.59, p=0.023) dental professionals showed significantly higher knowledge ranks than single/unmarried professionals. However, nationality [Non-Saudi vs Saudi (179.42 vs 178.41, p=0.954)] did not significantly differ in the mean ranks of knowledge. In contrast, the mean preventive awareness was insignificantly higher among males (185.25 vs.168.56, p=0.082), Saudi nationals (179.68 vs 166.97, p=0.434), and married (181.73 vs 173.90, p=0.413) dental professionals compared to their counterparts. An insignificant higher mean attitude ranks were found among females (178.77 vs 178.32, p=0.967) and married (183.36 vs 171.59, p=0.273) compared to males and single/unmarried dental professionals. On the contrary, Saudi (182.29 vs 141.36, p=0.025) dental professionals showed significantly higher attitude ranks than non-Saudi professionals. Study participants with more than ten years of experience showed higher knowledge (189.59), awareness (189.53), and attitude (195.17) scores compared to the other experience categories. Similarly, study participants working in government health sectors showed higher mean knowledge (183.38), awareness (185.59), and attitude (183.65) ranks compared to other categories. The mean ranks did not differ significantly across different experiences and categories of health sectors. Graduates/general practitioners showed higher knowledge (182.77) and awareness (195.01) ranks, while a higher attitude (197.95) score was reported among specialists. A comparison of mean preventive awareness scores by the Kruskal–Wallis test showed a statistically significant difference among different qualifications (p=0.004). Further comparison by the Mann–Whitney U-test indicated that the undergraduate dental students had significantly lower preventive awareness scores than the graduates/general practitioners (p=0.001) and postgraduate dental students (p=0.034). Similarly, dental specialists demonstrated significantly lower awareness scores compared to the graduates/general practitioners (p=0.009) (Table 5).
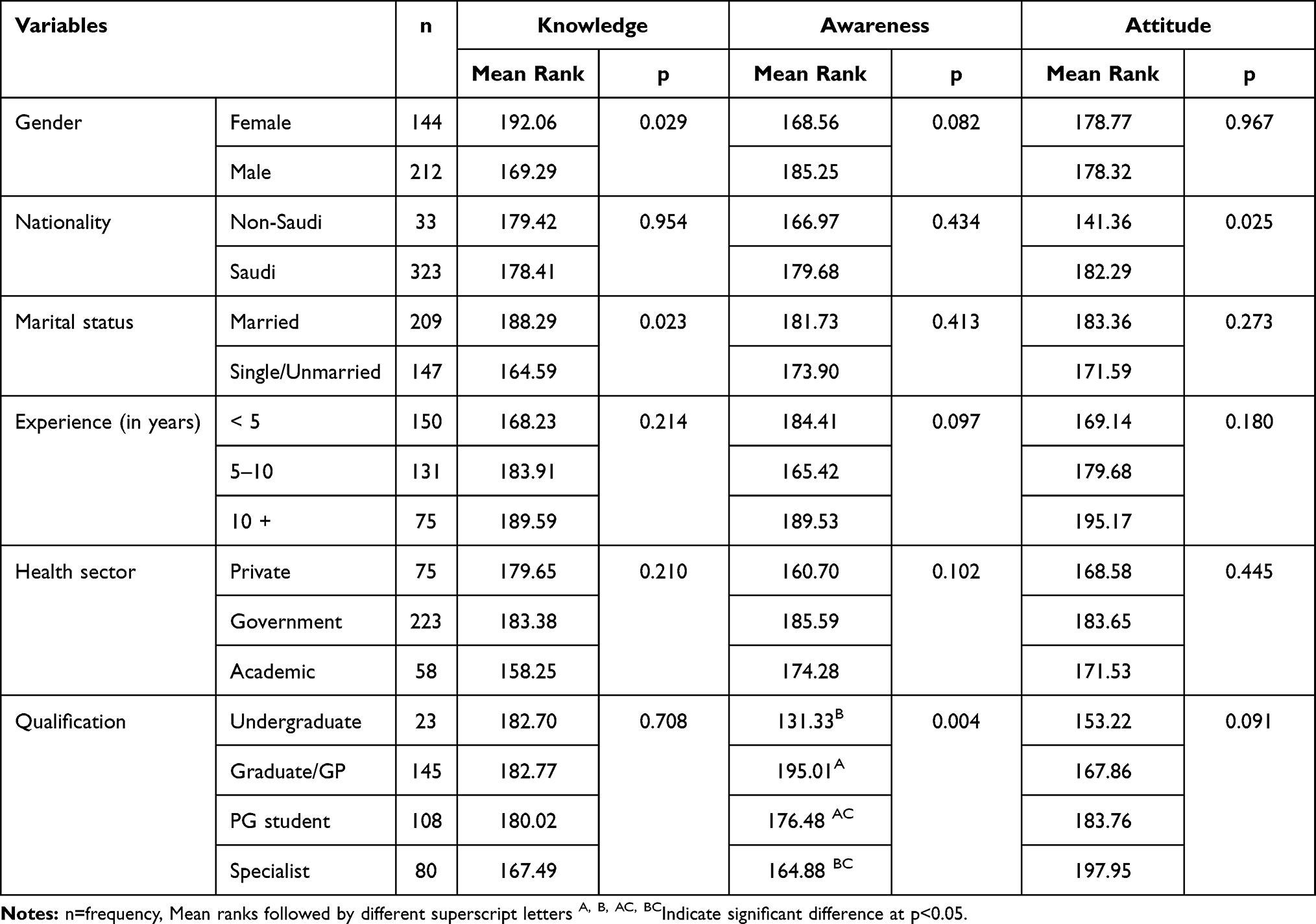 |
Table 5 Comparison of Mean Ranks of Knowledge, Preventive Awareness, and Attitude |
Regarding gender, the results indicate that, compared to females, males have lower knowledge (β = −0.212; p< 0.05). However no significant association was observed with awareness and attitude toward COVID-19. Compared to the Non-Saudi dental professionals, Saudi dental professionals demonstrated a significantly positive attitude (β=0.357; p< 0.01) towards COVID-19. Similarly, compared to undergraduate students, the graduate/GP demonstrated a significantly positive awareness (β=0.638, p< 0.01) of COVID 19. On the contrary, experience and marital status of the dental professionals did not show any significant association knowledge, preventive awareness and attitude towards COVID-19 (Table 6).
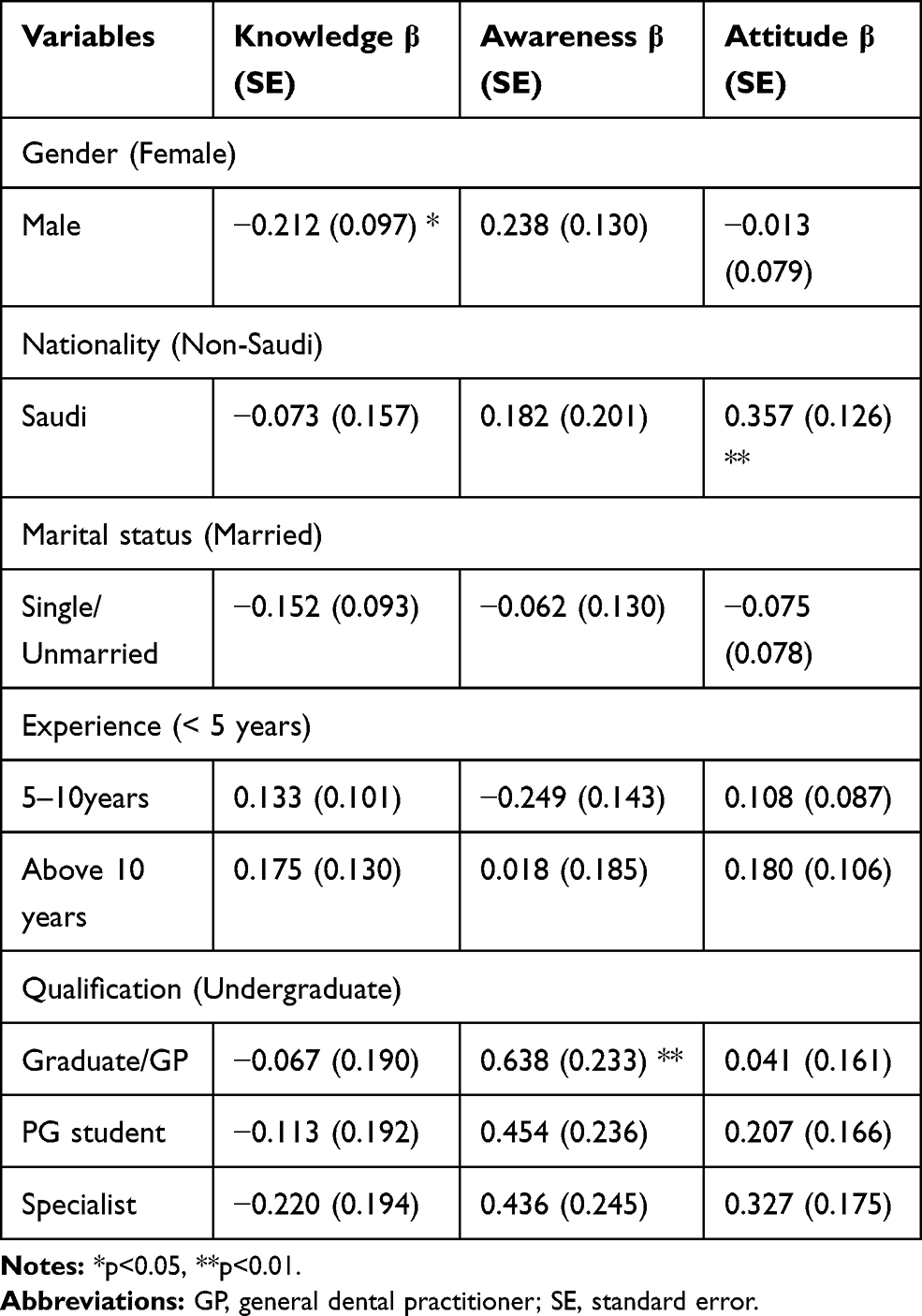 |
Table 6 Bivariate and Multivariable Analysis for the Factors Associated with Knowledge, Attitude and Practice |
Discussion
The Pandemic of COVID-19 contributed to a worldwide crisis. Not only the dissemination of COVID-19 posed global public health issues, has imposed significant pressure on economic, social, and global health systems, especially health staff, including dental health professionals.16 Many dental practices have modified their services according to the recommended guidelines to emergency treatment only or closed down practices for an uncertain period.20 COVID-19 is a highly infectious disease requiring stringent infection control. A high level of knowledge is essential and must be maintained to minimize disease spread in dental health care facilities and the community. Hence a judicious knowledge and preventive awareness of COVID-19 should be conveyed to the dental health professionals during this global disaster. In this regard, the present research explored dental professionals’ knowledge, preventive awareness, and attitude towards dental care patients during the COVID-19 pandemic.
To date, only a few studies investigated the knowledge and attitude of the dentist towards COVID-19 infection in Saudi Arabia. Most of the previous investigations on this topic were mainly included, dental students and faculties.16,19,20 Only limited studies reported dental practitioners and dental students’ perspectives on COVID-19. Hence present study assessed dental professionals’ knowledge, preventive awareness, and attitude towards providing dental care during the COVID-19 pandemic in Saudi Arabia. Males were predominant in this sample, which might be explained because the number of male dentists in Saudi is higher than that of female dentists based on the Saudi Commission for Health Specialties (SCFHS) database.17
The present study revealed a high level of knowledge of dental professionals towards COVID-19 symptoms. More than 90% of the dental professionals in this study correctly identified fever, dry cough, and shortness of breath as hallmark symptoms of COVID-19. A similar, high percentage of participants correctly answered about the development of severe acute respiratory illness, spread through close contact with an infected person, vaccination of COVID-19, use of antibiotics, and fatality COVID-19.
Almost 97.8% of dental professionals agreed that dental patients suffering from COVID-19 could spread infection in dental clinics. Nearly 90.2% of participants viewed COVID-19 as a dangerous infection in our study. On the contrary, a total of 17.7% of the 368 dentists perceived COVID-19 as very dangerous in a Jordanian study, 71.7% perceived it as moderately dangerous, and 9.5% perceived it as not a dangerous infection.14 This study found that 96.1% of dental professionals believed that COVID-19 is a severe public health issue. In contrast, one-third (36.7%) of dentists in a Jordanian study believed that COVID-19 is not a serious public health issue.14
The expected incubation period of COVID-19 is up to 14 days.21,22 Less than half of the dental professionals in this study correctly answered the exact incubation period of the COVID-19 infection. Dental professionals need to know about the right incubation period because of its role in determining the safe period to treat suspected COVID-19 patients.23 People with comorbidity (diabetes, cancer, and other chronic diseases) are more likely to contract COVID-19 and experience a more severe course and progression of the disease.26 The knowledge of such comorbidities varied among dental professionals in this study. Nearly 79.5% of the participants correctly answered about the impact of comorbidities and susceptibility to the COVID-19. A possible explanation could be that respiratory infections’ knowledge was somewhat lower among dental professionals than the other healthcare workers,24 even though dental care involves the patient proximity by the dental professionals.28
Nevertheless, a sample of dental professionals in this study could correctly identify the main symptoms of COVID-19, as evidenced by multiple responses analysis in which fever, cough, shortness of breath, followed by other COVID-19 symptoms. It helps dental professionals recognize the potential risk of COVID-19 and take the possible actions in management25 and control the spread of contagion.25
Owing to an individual’s proximity during dental procedures and aerosols production, dentists, auxiliaries, and patients are at high risk of COVID-19 transmission. Ministry of Health, Saudi Arabia, limited all dental services to emergency or urgent care. Hence, all other dental care specialties were postponed during this pandemic period until further notice to reduce the risk of spread. When enquired about this, a high percentage (84%) of dental professionals were aware of the dental emergency protocol during the COVID-19 pandemic published by the Saudi ministry of health.
Healthcare Infection Control Practices Advisory Committee (HICPAC) combined the Universal Precaution, and Body Substance Isolation features into Standard Precautions. These guidelines also introduced three transmission-based precautions: airborne, droplet, and contact. All transmission-based precautions are to be used in conjunction with standard precautions. These included hand hygiene and personal protective equipment (PPE). Personal protective equipment is a barrier to protect the skin, mucous membranes, airway, and clothing, and includes gowns, gloves, masks, and face shields or goggles.26 In our study, high responses were observed towards the use of personal protective equipment such as gowns (20.30%), gloves (20.10%), masks (20.10%), face shield (20%), goggle (17.80%), and others (1.2%).
When enquired about the use of precautions and other infection control recommendations provided by the Centre for Disease Control, World Health Organization, and America Dental Association, a high percentage of the study participants responded positively. Almost 83.1% were aware that transmission of COVID-19 infection could be prevented by implementing infection prevention and control measures recommendations provided by various agencies.
Hand hygiene is considered the most critical way to prevent disease.30 In our study, 96.9% of the dental professionals were aware of frequent cleaning of hands using alcohol-based hand rub or soap and water. Besides, 96.1% of the participants were aware of patients wearing masks during the dental office movement. On the contrary, most of the dentist believed that it was necessary to wear masks while in the waiting room, and wash hands before getting in the dental chair to decrease disease transmission.14
Seven questions assessed the attitude of study participants towards COVID-19 patient’s dental care. In this study, 76.7% of dental professionals indicated their unwillingness to treat a patient diagnosed with COVID-19 infection, while 69.7% did not agree to treat patients suspected of COVID-19 infection. In line with this finding, 82% of the Jordanian dentists preferred to avoid working with a patient suspected of COVID-19. It was believed that COVID-19 symptoms often resolve with time and do not require any special treatment.14
Ministry of Health, Saudi Arabia has issued strict guidelines for providing emergency dental care for the patients during the COVID-19 pandemic and the postponement of any elective dental treatment. In line with this recommendation, a high percentage of study participants showed a positive attitude to provide emergency dental care to the COVID-19 diagnosed patients and agreed to postpone routine/elective dental treatment and procedures for all patients. Similarly, a very high percentage of the participants showed a positive attitude by referring non-emergency patient if he/she is sneezing or coughing in the clinics while more than one-fourth agreed to treat the patients. These findings are higher than those reported by Khader et al (2020).14
During the COVID-19 pandemic, it is highly encouraged to assess transmission risk by checking every staff and patients’ temperature daily. Further, patients should be inquired about recent contact with COVID-19 patients and travel history (WHO 2020). Patients should be given medical masks while entering the clinic. If a patient or staff is found to have a fever, he/she should be directly referred to the particular hospitals dealing with COVID-19 cases. When a patient reports about visiting any of the high-risk areas within the last 14 days, quarantining for at least 14 days is recommended.27 In our study, more than three-fourth of the study participants did not agree to work with dental patients if they have flu-like symptoms. This finding further highlights the positive attitude towards controlling the spread of infection. In a study by Khader et al, 32.3% dentists allowed their dental staff to work with patients if they had flu-like symptoms.14 However, in this study, only 4.2% of the dentists agreed to do so.
As health care professionals, dental practitioners can actively contribute to increasing the preventive awareness of COVID-19 in the community. More than eighty percent of participants agreed to play an essential role in spreading COVID 19 information and increasing awareness in this study. However, Khader et al (2020) reported 97.8% of dentists were aware of the importance of educating others about COVID-19 to prevent in line with the guidelines issued by CDC, ADA, and the ministry of health Saudi Arabia.14
The mean knowledge, awareness, and attitude ranks were compared across different gender, nationality, and marital statuses of the study participants. Females and married dental professionals demonstrated significantly higher knowledge of COVID-19 compared to their counterparts. Similarly, Saudi dental professionals compared to non-Saudi professionals showed higher attitude scores indicating a more positive attitude towards the prevention of COVID-19. This may be attributed to health authorities’ information and guidelines during the outbreak of Middle East respiratory syndrome in Saudi Arabia.
Similarly, knowledge, awareness, and attitude scores did not differ significantly across the study participants’ experience and practice sectors. However, graduates/general practitioners demonstrated significantly higher preventive awareness than undergraduates. This finding contradicts the study reported by Al-Jasser et al (2020)28 in which postgraduate students had the highest mean knowledge ranks, followed by interns and undergraduate students. Several studies with similar outcomes are reported from Saudi Arabia.29–31 All these studies had lower response rate than our study.
Unlike many other studies, this particular research has some limitations. During the COVID-19 pandemic, most of the dental professionals were busy with their affairs. Only those who were active on Twitter and WhatsApp during July could able to participate in the study. This might have led to selection bias and sampling error, limiting our study findings’ generalizability. Hence further study with large sample sizes is needed to confirm our findings.
Conclusion
Within the study’s limitations, it can be concluded that the dental professionals who participated in this study demonstrated adequate knowledge of symptoms, preventive awareness, and a positive attitude towards dental care of the COVID-19 infected patients. Dental professional organizations should undertake regular online continuing education programs to update members about emerging dental care concerns of the COVID-19 pandemic in Saudi Arabia.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Phelan AL, Katz R, Gostin LO. The novel coronavirus originating in Wuhan, China: challenges for global health governance. JAMA. 2020;323(8):709–710. doi:10.1001/jama.2020.1097
2. Raoult D, Zumla A, Locatelli F, Ippolito G, Kroemer G. Coronavirus infections: epidemiological, clinical and immunological features and hypotheses. Cell Stress. 2020;4(4):66–75. doi:10.15698/cst2020.04.216
3. Lai -C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
4. Estrich CG, Mikkelsen M, Morrissey R, et al. Estimating COVID-19 prevalence and infection control practices among US dentists. J Am Dent Assoc. 2020;151(11):815–824. doi:10.1016/j.adaj.2020.09.005
5. Judson SD, Munster VJ. Nosocomial transmission of emerging viruses via aerosol-generating medical procedures. Viruses. 2019;11(10):940. doi:10.3390/v11100940
6. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
7. Morawska L. Droplet fate in indoor environments, or can we prevent the spread of infection? Indoor Air. 2006;16(5):335–347. doi:10.1111/j.1600-0668.2006.00432.x
8. Shiu EYC, Leung NHL, Cowling BJ. Controversy around airborne versus droplet transmission of respiratory viruses: implication for infection prevention. Curr Opin Infect Dis. 2019;32(4):372–379. doi:10.1097/QCO.0000000000000563
9. William C, Hinds Z. Aerosol Technology: Properties, Behavior, and Measurement of Airborne Particles. Wiley-Blackwell; 1999.
10. Beggs CB. Is there an airborne component to the transmission of COVID-19?: a Quantitative Analysis Study. medRxiv. 2020.
11. Grayson SA, Griffiths PS, Perez MK, Piedimonte G. Detection of airborne respiratory syncytial virus in a pediatric acute care clinic. Pediatr Pulmonol. 2017;52(5):684–688. doi:10.1002/ppul.23630
12. Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172(9):577–582. doi:10.7326/M20-0504
13. MOH. Dental emergency protocol during COVID-19 pandemic; 2020. Available from: https://www.moh.gov.sa/Ministry/MediaCenter/Publications/Documents/MOH-Dental-emergency-guidline.pdf.
14. Khader Y, Al Nsour M, Al-Batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: Cross-Sectional Study among Jordanian dentists. JMIR Public Health Surveill. 2020;6(2):e18798. doi:10.2196/18798
15. Sarfaraz S, Shabbir J, Mudasser MA. et al., Knowledge and attitude of dental practitioners related to disinfection during the COVID-19 pandemic. In: Healthcare. Vol. 8. Multidisciplinary Digital Publishing Institute; 2020:232.
16. Javed MQ, Khan AM, Nawabi S. Dental Faculty’s Knowledge and Attitude Regarding COVID-19 Disease in Qassim, Saudi Arabia. 2020.
17. AlBaker AM, Al-Ruthia YSH, AlShehri M, Alshuwairikh S. The characteristics and distribution of dentist workforce in Saudi Arabia: a Descriptive Cross-Sectional Study. Saudi Pharm J. 2017;25(8):1208–1216. doi:10.1016/j.jsps.2017.09.005
18. Bahabri RH, Zaidan AB. The impact of social media on dental practice promotion and professionalism amongst general dental practitioners and specialists in KSA. J Taibah Univ Med Sci. 2021. doi:10.1016/j.jtumed.2020.12.017
19. Ahmed MA, Jouhar R, Ahmed N, et al. Fear and practice modifications among dentists to combat novel coronavirus disease (COVID-19) outbreak. Int J Environ Res Public Health. 2020;17(8):2821. doi:10.3390/ijerph17082821
20. ALNohair SF, Mahmud I, ALShehri F, ALShuqayran R, ALBatanouni M. Knowledge, Attitudes, and Practices of Medical Interns Toward COVID-19 in Saudi Arabia: A Cross-Sectional Survey, April-May 2020. 2020.
21. Backer JA, Klinkenberg D, Wallinga J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. 2020;25(5). doi:10.2807/1560-7917.ES.2020.25.5.2000062
22. Li Q, Guan X, Wu P, et al. Early transmission dynamics in wuhan, china, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
23. Gaffar BO, El Tantawi M, Al-Ansari AA, AlAgl AS, Farooqi FA, Almas KM. Knowledge and practices of dentists regarding MERS-CoV. A cross-sectional survey in Saudi Arabia. Saudi Med J. 2019;40(7):714–720. doi:10.15537/smj.2019.7.24304
24. Abolfotouh MA, AlQarni AA, Al-Ghamdi SM, Salam M, Al-Assiri MH, Balkhy HH. An assessment of the level of concern among hospital-based health-care workers regarding MERS outbreaks in Saudi Arabia. BMC Infect Dis. 2017;17(1):4. doi:10.1186/s12879-016-2096-8
25. Meng L, Hua F, Bian Z. Coronavirus disease 2019 (COVID-19): emerging and future challenges for dental and oral medicine. J Dent Res. 2020;99(5):481–487. doi:10.1177/0022034520914246
26. Broussard IM, Kahwaji CI. Universal precautions. StatPearls. StatPearls Publishing; 2020. Available from: http://www.ncbi.nlm.nih.gov/books/NBK470223/.
27. ADA. ADA recommending dentists postpone elective procedures. American Dental Association; 2020. Available from: https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-recommending-dentists-postpone-elective-procedures#.
28. Al Jasser R, Al Sarhan M, Al Otaibi D, Al Oraini S. Awareness toward COVID-19 precautions among different levels of dental students in King Saud University, Riyadh, Saudi Arabia. J Multidiscip Healthc. 2020;13:1317–1324. doi:10.2147/JMDH.S267956
29. Mustafa RM, Alshali RZ, Bukhary DM. Dentists’ knowledge, attitudes, and awareness of infection control measures during covid-19 outbreak: a Cross-Sectional Study in Saudi Arabia. Int J Environ Res Public Health. 2020;17(23):9016. doi:10.3390/ijerph17239016
30. Srivastava KC, Shrivastava D, Sghaireen MG, et al. Knowledge, attitudes and practices regarding COVID-19 among dental health care professionals: a Cross-Sectional Study in Saudi Arabia. J Int Med Res. 2020;48(12):300060520977593. doi:10.1177/0300060520977593
31. Tarakji B, Nassani MZ, Alali FM, et al. COVID-19-awareness and practice of dentists in Saudi Arabia. Int J Environ Res Public Health. 2021;18(1):330. doi:10.3390/ijerph18010330
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.