Back to Journals » Patient Preference and Adherence » Volume 12
Dental professionalism and influencing factors: patients’ perception
Authors Taibah SM ![]()
Received 1 May 2018
Accepted for publication 17 July 2018
Published 3 September 2018 Volume 2018:12 Pages 1649—1658
DOI https://doi.org/10.2147/PPA.S172788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Salwa Mahmoud Taibah
Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia
Background: Professionalism was recognized as a fundamental competency of medical/dental practice at the beginning of the twenty-first century. Organizations and experts published several definitions of professionalism, but research on patients’ perception of professionalism has been limited. To address this gap in literature, this study explored dental patients’ perception of dental professionalism, and then compared their perception with that of dental professionals.
Methods: Of the 800 questionnaires that were distributed to dental patients in public and private clinics and hospitals, 504 were returned and were used in the analysis. A factor analysis was used to generate themes and sub-themes. Independent sample t-tests were performed to compare two independent groups and the ANOVA tests to compare means in more than two independent groups.
Results: A factor analysis revealed four factors: excellence and communication skills; humanism, commitment, and service mindedness; competence in practice; and dentists’ duties and management skills. Adherence to sterilization and infection control rules and procedures; personal hygiene and clean professional attire; good communication skills; diagnostic and clinical judgment and provision of the most efficient dental treatment; and ethical decisions and ethical care were ranked as the first five most important elements of dental professionalism from patients’ perspective. Several demographic factors showed significant differences in perception.
Conclusion: Patients’ and dentists’ perception of dental professionalism and professional behavior vary in certain aspects. These differences must be addressed to ensure excellence of dental service. Dental professionals must also be aware of the personal factors that affect a patient’s perception of professionalism.
Keywords: dental professionalism, dentist behavior, patients’ perception
Introduction
In 2000, the American Board of Internal Medicine, in collaboration with the American College of Physicians Foundation and the European Federation of Internal Medicine, published the Physician Charter that recognized professionalism as among the fundamental competencies of medical practice. Following the Physician Charter, several organizations published various definitions of professionalism, such as the Accreditation Council of Graduate Medical Education,1 the United Kingdom (UK) General Medical Council, the UK Royal College of Physician, and the Royal College of Physician and Surgeons of Canada.2 In addition to the organizational models of professionalism, the medical literature is filled with hundreds of author publications in an attempt to define professionalism.3–9 These definitions’ common feature is that they reflect mainly the perception of health care providers. Few studies have highlighted patients’ perception of the professional behavior of health care givers.
Several authors have discussed what they called the medicine’s social contract and how professionalism serves as the base of this contract.10–13 Such implicit contract determines the rights and obligations of both sides (ie, health care provider and the public), and sets the context of several responsibilities on both the giver and the taker of the service. Consequently, dentists are granted privileges, prestige, and financial status on the expectation that they will be professional and ethical. The expectations of society and the profession are apparently diverging, leading to a gap between the dental profession and society. The dental profession believed for a long time that it should define itself. However, professional status cannot be simply claimed by the profession; it must be gained and decided by society. In addition, dental professionalism and profession values are threatened in the modern, more materialistic world of the twenty-first century, and these threats are expressed as a loss of trust in the profession in the Kingdom. Within such context, society’s contract with the dental profession should be renegotiated. With the evolution of professionalism as a fundamental competency, such implicit contract must be more explicit, with professionalism to remain as the basis of the contract. This process must be achieved through a continuous discussion between all parties involved (eg, society, the dental profession, dental organizations and associations, the government, the court, patient representatives, sociologists, and ethicists).11 These entities should act together to reach a mutual agreement on the terms and conditions of the medical/dental contract and be a part of the profession’s definition of professionalism and profession values; otherwise, society’s loss of trust in the dental profession is expected and any failure in these expectations and agreements will increase the gap and divergence. Therefore, the nature of public expectations from the medical/dental profession must be determined by both the profession and the public. This philosophy highlights the importance of involving the public, which is represented by patients, in defining professionalism, and expresses their perception of what they think to be professional.
A more patient-centered dental service is now recognized as a fundamental dimension of dental service quality, as this type of service will augment patient satisfaction and thus improve service outcomes. As all health professions depend on patients’ loyalty, attending the multiple dental appointments, and keeping long periods of treatment, quality dental service is the target of both patients and dental profession. Gaining the required loyalty comes only through satisfied patient and good dentist–patient relationship. Changing this implicit contract to a more explicit one, by discussion of all involved parties, will augment a more trustful relationship between the profession and the public. In return, patients’ loyalty and thus service excellence are enhanced and improved. Few studies have explored the perception of patients on the professional behavior of a dentist. A number of these studies have highlighted the importance of dentists’ professional behavior toward their patients. In Green et al’s qualitative study on the behavioral signs of professionalism, medical patients prioritized ethical manner, honesty, confidentiality, and good hygiene.14 In another study conducted in the eastern region of Saudi Arabia, El-Amin et al studied factors used by patients to evaluate the standards of professional practice; more than 95% of the participants thought an empathetic dentist with high dental skills and updated hygienic practice is important.15 Karydis et al also found that sincere interest and empathy, followed by assurance and responsiveness, were patients’ top priorities.16 Several other studies explored mainly the patients’ opinion on dentist or health provider attire.17–20
Most definitions of professionalism in the literature were generated from organizations, professionals’ viewpoints, or medical/dental students’ opinion. However, for the health service to be at the highest quality possible, patients’ perception of a dentist’s professional behavior must be considered.21 The present study aims to:
- Derive dental patients’ perception of the required professional behavior for a quality dental service
- Describe a model of dental team professionalism in Saudi Arabia based on patients’ perception
- Verify whether factors, such as patients’ gender and level of education, type of delivery of treatment, culture, and age, affect patients’ perception in constructing a conceptual model of dental team professionalism
- Compare patients’ perception with that of the dental professionals, which was derived from a PhD dissertation.21
Methods
Sample
This study was a cross-sectional survey with a convenient sample conducted in Jeddah city, Saudi Arabia. The General Authority for Statistics census estimated the population of Jeddah city to be 3,457,794 in 2010. To obtain a representative sample size, with a 5% margin of error and 95% CI, the minimum number of participants recommended was 385. With an assumption of a response rate of 50%, 800 questionnaires were distributed to patients over 18 years old in public and private clinics and hospitals; 504 returned the questionnaires (63% response rate).
Ethical considerations
Internal Review Boards at the King Abdulaziz University approved the present study, which was performed following the Declaration of Helsinki ethical guidelines. The participants’ submission of the completed questionnaire implied their consent to the study, as it was assumed that they read the information sheet at the first page of the questionnaire.
Questionnaire
The questionnaire on the patients’ perception of professional and ethical dental behavior consisted of two parts. The first part comprised questions on demographic data, including age, sex, type of educational institution attended (public or private), educational level, type of dental treatment, and type of dental clinic (public or private hospital or clinic). The second part comprised 24 statements that were used to evaluate their perception of the elements of dental professionalism, such as communication skill, professional and ethical qualities, and personal attributes. The elements were derived from several publications, such as the General Dental Council in United Kingdom’s (GDC’s) “Standards for Dental Profession,”22 American Board of Internal Medicine’s “Medical Professionalism in the New Millennium: A Physician Charter,”23 and the Royal College of Physicians and Surgeons of Canada’s (CanMEDS’s)2 and Swick’s Normative definition of professionalism.3 A five-point Likert scale (1= strongly disagree, 2= disagree, 3= neither agree nor disagree, 4= agree, and 5= strongly agree) was used. An open-ended question was also added at the end of the questionnaire to capture other elements or themes that might have been overlooked. As the participants’ native language is not English, a forward – backward translation of the questionnaire was conducted through a licensed translation service.
To test the reliability of the questionnaire, 40 questionnaires were distributed among dental patients. Based on the Cronbach’s alpha for each statement, final adjustments related to the sentence structure were made. Cronbach’s alpha was 0.926, indicating the scale had good reliability.
Data analysis
All statistical analyses were performed using the SPSS, version 20 (SPSS Inc., Chicago, IL, USA), as follows: 1) a descriptive statistical analysis of the mean of demographic data and the questionnaire elements was performed; 2) a factor analysis was also conducted to explore the generated themes and sub-themes; 3) independent sample t-test was used to compare means in two independent groups; and 4) ANOVA test was performed to compare means in more than two independent groups.
Negative statements were also recorded by reversing the scale to avoid any false-negative or -positive responses.
Results
Table 1 presents the participants’ descriptive characteristics. The 504 participants comprised 201 males (39.9%) and 303 females (60.1%), with a mean age of 33.59 years (SD =10.4). Most participants were Saudi nationals (67.1%). Data on the educational level of the respondents were as follows: diploma and bachelor’s degree (59.3%), high school (18.8%), postgraduate (15.3%), and intermediate school (6.5%).
 | Table 1 Participants’ descriptive characteristics (N=504) |
Ranking of elements of dental professionalism
The participants rated nearly all the elements of dental professionalism as agree or strongly agree (Table 2). The three most important elements, in order, were adherence to sterilization and infection control rules and procedure, personal hygiene and clean professional attire, and good communication skills. Other important elements deemed by the participants, in order, included diagnostic and clinical judgment and provision of the most efficient dental treatment, ethical decision and ethical patient care, accurate documentation of a patients’ data and treatment progress, and respect to the patient and his/her family.
 | Table 2 Participants’ ranking of the elements of dental professionalism (N=504) |
In contrast, the three least important elements, in order, were explaining to the patient his/her condition and all treatment options and cost-effective treatment in an easily understood way, confidentiality to other patients (or exposing dental information to others and patients’ family), and educating the patient about his/her legal rights and obligations that govern doctor/patient relations (or awareness of legal rights).
Factor analysis
Four factors were derived. To check the internal consistency of the statements comprising each factor, Cronbach’s alpha (α) was tested: Factor 1 (F1) α=0.797, Factor 2 (F2) α=0.710, Factor 3 (F3) α=0.774, and Factor 4 (F4) α=0.625, indicating that all factors had good reliability. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.8, and the Bartlett’s test of sphericity was significant (χ2=2,258.914, df=276, P<0.001), indicating high appropriateness for factor analysis.
The results of the analysis showed four domains: excellence and communication skills, comprising six items with factor loading between 0.83 and 0.57; humanism, commitment, and service mindedness, comprising eight items with factor loading between 0.73 and 0.50; competence in practice, comprising seven items with factor loading between 0.74 and 0.45; and a dentist’s duties and management skills, comprising three items with factor loading between 0.65 and 0.50. Figure 1 presents domains and subdomains of professionalism from patients’ perspective and elements influencing each domain.
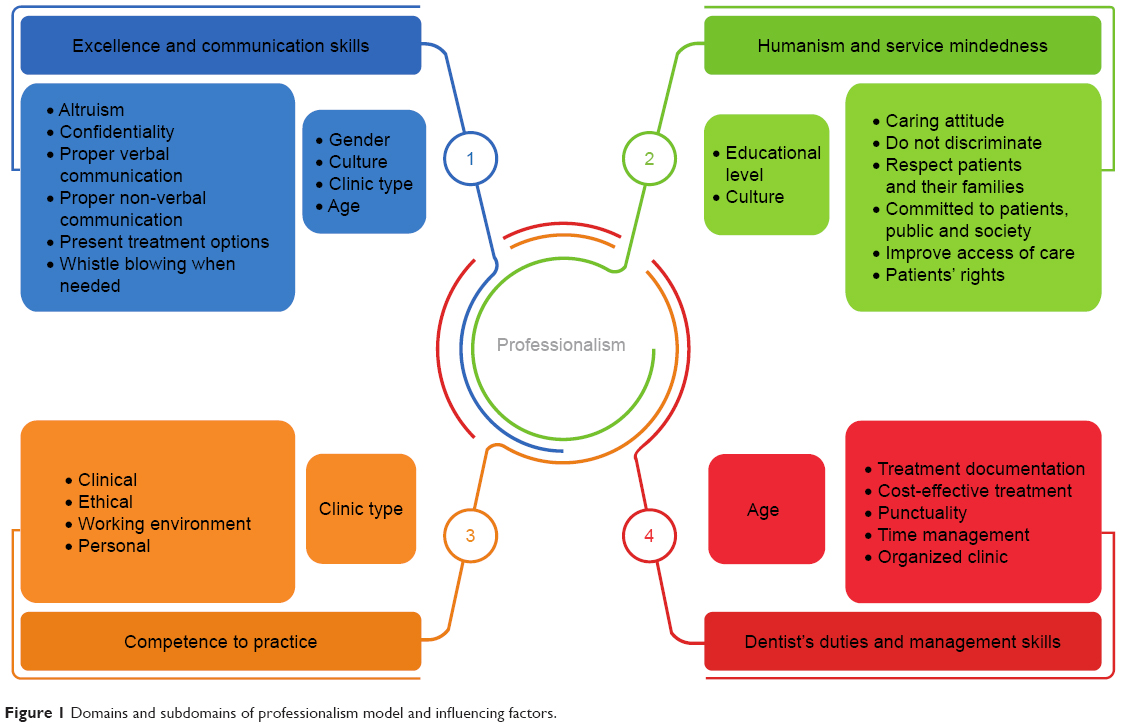 | Figure 1 Domains and subdomains of professionalism model and influencing factors. |
Factors affecting patients’ perception
As shown in Table 3, a statistically high significant difference in the perception of males and females was observed in the first domain, that is, excellence and communication skills. The former deemed confidentiality to other patients (P<0.001), good communication skills (both verbal and nonverbal) (P<0.006), altruism (P<0.001), and blowing the whistle to any illegal or unethical practice of colleagues (P<0.001) as more important than females did.
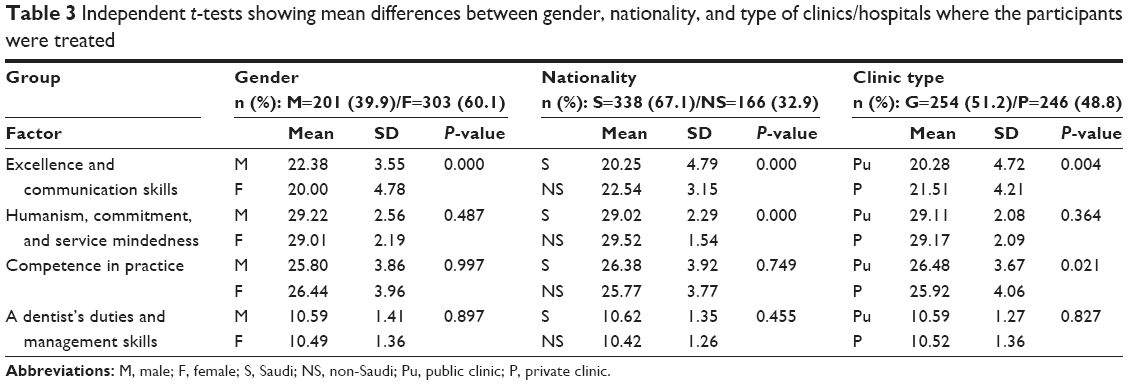 | Table 3 Independent t-tests showing mean differences between gender, nationality, and type of clinics/hospitals where the participants were treated |
Similarly, a statistically high significant difference in the perception of Saudis and non-Saudis was observed in the first and second domains, that is, excellence and communication skills, and humanism, commitment, and service mindedness. The Saudis believed that the following elements were more important than did the others: confidentiality to other patients (P<0.001), explaining to the patient his/her condition and all treatment options and cost-effective treatment in an easily understood way (P=0.001), having responsibility to improve dental health and knowledge of society (P=0.008), and positive caring attitude (P=0.047). In contrast, the latter considered the following as slightly more important than the former did: ethical decisions and ethical patient care (P=0.022) and respect of patients’ autonomy (P=0.025). A statistically high and slight significant difference in excellence and communication skills and competence in practice, respectively, were observed depending on the type of clinic/hospitals where the participants were treated. Patients treated in public hospitals believed that an accurate documentation of patients’ data and treatment progress (P=0.033) is more important than did the patients treated in private hospitals. The latter believed that explaining to the patient his/her condition and all treatment options and cost-effective treatment in an easily understood way (P=0.003) is more important than did the former (Table 3).
Meanwhile, the ANOVA test revealed that the importance of excellence and communication skills domain increases along with age. The middle age group (26–40 years old) was also observed to place a slightly higher significance on dentists’ duties and management skills domain compared with the other two age groups. Moreover, it was observed that the importance of humanism, commitment, and service mindedness domain increases with the level of education (Table 4).
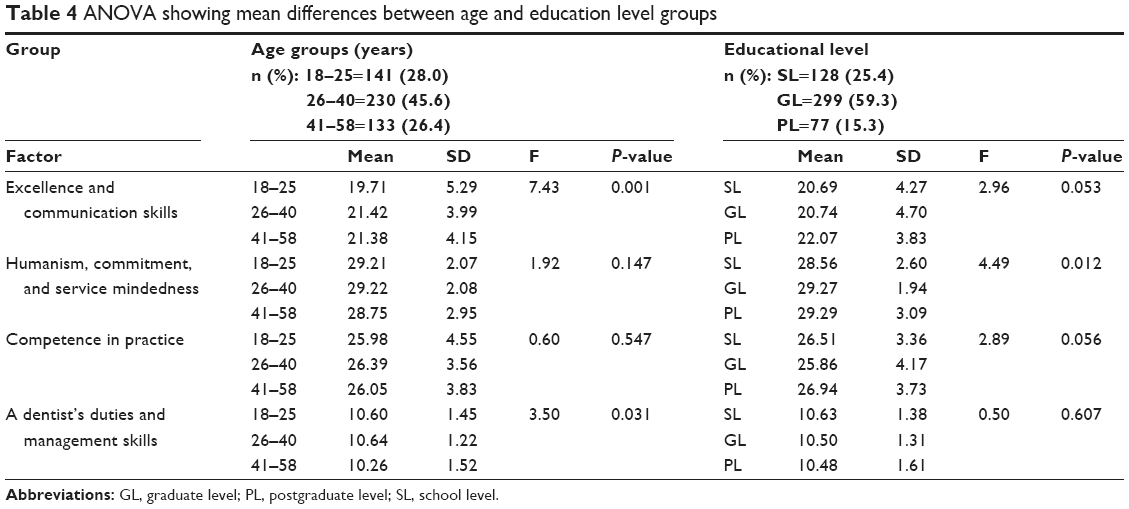 | Table 4 ANOVA showing mean differences between age and education level groups |
Perceptions of patients vs dental professionals
Table 5 shows the independent t-tests comparing the perception of dental patients with that of dental professionals. Patients placed more importance on adherence to sterilization and infection control rules and procedures; personal hygiene and clean professional attire; management skills, punctuality, time management, and having an organized clinic; altruism; and good communication skills (P<0.001). In contrast, dental professionals place more importance on respect to the patient and his/her family; explaining to the patient his/her condition and all treatment options and cost-effective treatment in an easily understood way; proper nonverbal responses; positive caring attitude (P<0.001), and working collaboratively with other medical professionals (P=0.002).
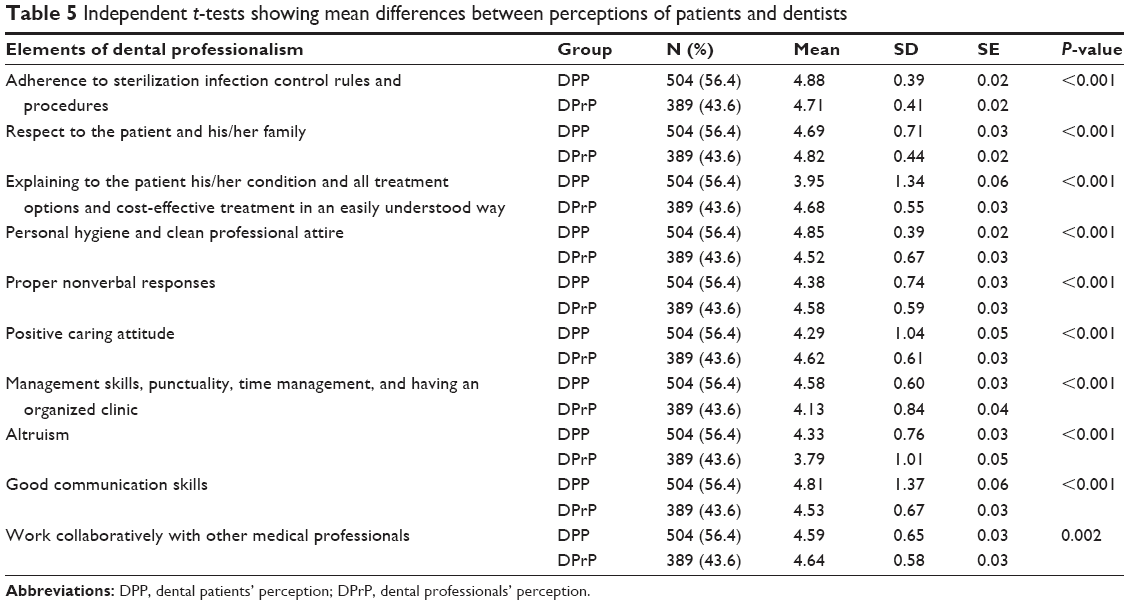 | Table 5 Independent t-tests showing mean differences between perceptions of patients and dentists |
Discussion
A patient’s first impression influences his/her perception of a dentist’s competency, and thus determines his/her expectation, satisfaction, and compliance with dental treatment and procedures. In addition to dentists’ perception of professionalism, knowing patients’ expectation of a dentist provides the foundation to teach professionalism in dental schools at both undergraduate and postgraduate levels. Moreover, patients’ and dentists’ perception of professionalism and dental professional behavior must converge to ensure patient satisfaction. Consequently, patient involvement in the decision of the level of dental care they will receive is an important and essential step to achieve excellent dental service and a step forward toward patient-centered care and professionalism.
In a study that evaluates a social phenomenon, such as professionalism, heterogeneity of the sample gives more strength to the study findings. The sample of 504 participants in the present study resembled the population heterogeneity of Jeddah city, and thus covered more perceptions and opinions.
The results showed that the patients perceive dentists’ behavior in four domains: excellence and communication skills; humanism, commitment, and service mindedness; competency in practice; and dentists’ duties and management skills. Other studies have highlighted these domains, but they were titled differently.13,24,25
Communication skills (both verbal and nonverbal) with either a patient, a colleague, or another health professional are among the important domains in most studies on patients’ perception of professionalism.13,14,26,27 Stern also represented communication skills as among the foundations of professionalism, in addition to clinical competence and ethical and legal understanding.28 The present study found a statistically significant difference in the perception of the importance of communication skills of the dentists between patients and dentists. The same difference was observed in Alnasser et al’s study, where a clear discrepancy was found between the perception of physicians and parents concerning communication skills in a pediatric clinic setting.29 Such communication gap was also found by Kee et al in their retrospective evaluation of 125 patients, in which important differences in verbal and nonverbal communication were found between patients and doctors.30
Altruism was also considered important but differently perceived between patients and dental professionals. Taibah’s study showed that dentists ranked altruism as second least important in defining dental professionalism.21 In the present study, patients considered it as more important than dentists do. This finding indicates that altruism must be emphasized to improve dental service and increase patient satisfaction. Specifically, this finding must be discussed at the undergraduate and postgraduate schools.
Humanism, commitment, and service mindedness are highlighted in the second domain. The patients place premium on a respectful behavior and a caring attitude, which means that a dentist does not discriminate against patients’ views and values. These humanistic values are essential principles that direct the interaction between patients in demand of assistance and professionals offering it. The participants believed that a dental service based on respect, equality, and empathy is a highly professional service. This finding is consistent with that found in Lebanon, suggesting that humanness is the most valued quality in health care.24 Likewise, Sbaraini et al stated that a respectful relationship between a patient and a dentist is considered highly satisfying to the patients.31
Several studies have evaluated the level of student empathy during medical school, and found a decline in the empathy level, particularly when the students are moving toward patient care.32,33 As these studies have been performed in countries that are culturally different than the present study, similar studies are required to evaluate the level of empathy change among dental students in the dental schools of Saudi Arabia.
Dentists’ commitment to the patient, the public, and society are also considered important to dental professionalism from the participants’ perception. This commitment must be in the form of dedication to the profession, as dental service quality and obligation to patient benefit the country. Service mindedness represents the third subdomain, and is defined by American Dental Education Association as “acting for the benefit of the patients and the public we serve, and approaching those served with compassion.”34 This subdomain indicates a dentist’s role in improving access of the dental service in Saudi Arabia. The present study supports the findings of studies conducted in other countries, indicating the importance of humanism and service mindedness. These humanistic values are tied to religion, and thus it is highly respected and expected to be the base of a person’s communication intentions.
The third domain highlighted the clinical, ethical, environmental, and personal competencies from the patients’ perspective. Patients’ autonomy and rights were also highlighted in this domain. Although patients felt that it is their right to understand their condition and all treatment options available, this element showed a statistically significant difference with the professionals’ feeling that this element is more important. This trait is gaining more importance from the patients’ perspective. A few years ago, patients played a more passive role, thinking that the health care provider knows best with respect to treatments. The present study showed that patient perception is changing toward a collaborative role in treatment planning, emphasizing the importance of patient-centered dental practice. Nomura et al reported similar results.35 Dental service in the Kingdom is showing important steps toward patient-centered care; this movement should continue by accentuating the importance of this type of practice in dental schools.
The accurate documentation element came fifth in the descending ranking. The results showed a statistically significant difference between the sexes, with females feeling the importance of this type of communication (P=0.012). This element also showed a statistically significant difference according to culture, where Saudis deemed it more important (P=0.036). With the revolution of digital technology, documentation has been improving, owing to ease of digitization, especially in leading educational institutes in the Kingdom. Newly established private clinics, public hospitals, and small clinics are recognizing the importance of this element, and are gradually improving their documentation system. This point is shown in the statistically significant difference of this element between patients attending private clinic and those attending public clinics (P=0.033).
In certain areas, dentistry is becoming more a business than a profession. This issue could be the reason that patients are asking for their autonomy and rights to understand their condition and all treatment options available.
Among the first five elements ranked, competency in practice elements was highlighted, summarized as adherence to infection control, professionals’ attire, good diagnostic and clinical judgment, and ethical decisions. Adherence to infection control showed a statistically significant difference between patients, who placed more importance on this element (Table 5), and dentists, although both tended to “strongly agree” on this element. This difference points to the importance of emphasizing the application and assessment of infection control measures in the undergraduate and postgraduate clinical dental courses.
The “dentists’ duties and management skills” factor showed a statistically significant difference with respect to age. The age group of 26–40-year old participants thought that dentists’ duties and management skills are more important to dentist professionalism compared with younger and older participants and dental professionals.
A dynamic phenomenon such as professionalism is influenced by environment and culture. Dentists should be aware of these factors to foster their professionalism. Lesser et al emphasized the influence of context on physician/dentist behavior, showing behavior is affected by interactions with patients and families, the health care team, the practice environment, and the broad external environment.36 The present study evaluated the patient-side factors that may affect patients’ perception of dentists’ professionalism, and thus satisfaction. The communication and excellence factor is affected by the age, gender, and cultural background of the patient, in addition to clinic type. Notably, level of education did not have an effect on the way the patient expected the dentist to communicate. However, the level of education has an effect on the perception of the participant on the humanistic expectation of the patient; that is, expectations for respect, equality, and caring increased with the level of education. Expectations from the dentist to improve society’s dental health also increased (Figure 1).
One limitation of the present study is related to the wide age range in the sample; a smaller range will yield a clearer idea on how patients’ expectations change with age. A qualitative type of data collection will enrich the outcomes regarding patients’ perception of professionalism, and ultimately improve patient–dentist relationship and dental health service in the Kingdom. Additional limitation is that the generalizability of the results may be limited due to cultural difference factor.
Conclusion
- The study identified four factors of professionalism to form its definition according to patients’ perception: 1) excellence and communication skills; 2) humanism, commitment, and service mindedness; 3) competence in practice; and 4) duties and management skills.
- Gender, age, culture, clinic type and level of education are factors that influence patients’ perceptions of professionalism.
- For promoting excellence in dental service in the Kingdom, patient and dentist perspectives regarding professionalism and professional behavior of the dentist should match. Indeed, the triangulation of professionalism definitions and perspectives between dental professionals and dental patients is essential for dental service satisfaction.
- Dental professionals should be aware of the personal factors that affect patients’ perception of dentists’ professionalism.
- Altruistic behavior and communication skills of the dentist are believed to be more important by the patient; these two elements are considered the base for a good patient–dentist professional relationship. Both dentist and patient should see eye-to-eye on these concepts for quality patient-centered service.
- There is a need for substantial efforts of medical/dental educators to reflect the dynamic nature of professionalism on dental curricula.
Acknowledgments
The author would like to thank Dr Fatehia El-Halawani, Assistant Professor of Biostatistics at King Abdulaziz University, for her valuable help in conducting the statistics of the present study. Also, the author would like to thank the Editage Author Service for English language editing of the manuscript. This work was self-funded.
Disclosure
The authors report no conflicts of interest in this work.
References
ACGME. Accreditation Council for Graduate Medical Education [cited 2011 June]. Available from: https://www.google.com.sa/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&cad=rja&uact=8&ved=2ahUKEwi_2o6W14fdAhVMQRoKHfTyBBYQFjABegQICBAC&url=http%3A%2F%2Fwww.ucdenver.edu%2Facademics%2Fcolleges%2Fmedicalschool%2Fdepartments%2Fpediatrics%2Fmeded%2Ffellowships%2FDocuments%2FACGME%2520Outcome%2520Project.pdf&usg=AOvVaw2tBmoGw5u-_d0uEnaf_tmR. Accessed August 29, 2018. | ||
CanMEDS. The CanMEDS 2005, Physician Competency, Framework 2005 [cited 2010 November]. Available from: http://meds.queensu.ca/medicine/obgyn/pdf/CanMEDS2005.booklet.pdf. Accessed August 29, 2018. | ||
Swick HM. Toward a normative definition of medical professionalism. Acadic Medicine. 2000;75(6):612–616. | ||
Stevens RA. Themes in the history of medical professionalism. Mount Sianai Med. 2002;69(6):357–362. | ||
van de Camp K, Vernooij-Dassen M, Grol R, Bottema B. Professionalism in general practice: development of an instrument to assess professional behaviour in general practitioner trainees. Med Educ. 2006;40(1):43–50. | ||
van de Camp K, Vernooij-Dassen MJ, Grol RP, Bottema BJ. How to conceptualize professionalism: a qualitative study. Med Teach. 2004;26(8):696–702. | ||
van Mook WN, van Luijk SJ, O’Sullivan H, et al. The concepts of professionalism and professional behaviour: conflicts in both definition and learning outcomes. Eur J Intern Med. 2009;20(4):e85–e89. | ||
Wagner P, Hendrich J, Moseley G, Hudson V. Defining medical professionalism: a qualitative study. Med Educ. 2007;41(3):288–294. | ||
Jha V, Bekker HL, Duffy SR, Roberts TE. Perceptions of professionalism in medicine: a qualitative study. Med Educ. 2006;40(10):1027–1036. | ||
Bhugra D. Medicine’s contract with society. J R Soc Med. 2014;107(4):144–147. | ||
Cruess RL, Cruess SR, Johnston SE. Professionalism and medicine’s social contract. J Bone Joint Surg Am. 2000;82-A(8):1189–1194. | ||
Cruess SR, Cruess RL. Professionalism: a contract between medicine and society. CMAJ. 2000;162(5):668–669. | ||
Sari MI, Prabandari YS, Claramita M. Physicians’ professionalism at primary care facilities from patients’ perspective: the importance of doctors’ communication skills. J Family Med Prim Care. 2016;5(1):56–60. | ||
Green M, Zick A, Makoul G. Defining professionalism from the perspective of patients, physicians, and nurses. Acad Med. 2009;84(5):566–573. | ||
El-Amin EI, Al-Ghannam NA, Khan NB. Patients’ assessment of the professional and business aspects of dental practice. Saudi Dental J. 2004;16(3):107–112. | ||
Karydis A, Komboli-Kodovazeniti M, Hatzigeorgiou D, Panis V. Expectations and perceptions of Greek patients regarding the quality of dental health care. Int Soc Qual Health Care. 2001;13(5):409–416. | ||
Mercer E, Mackay-Lyons M, Conway N, Flynn J, Mercer C. Perceptions of outpatients regarding the attire of physiotherapists. Physiother Can. 2008;60(4):349–357. | ||
Mckenna G, Lillywhite GR, Maini N. Patient preferences for dental clinical attire: a cross-sectional survey in a dental hospital. Br Dent J. 2007;203(12):681–685. | ||
Kazory A, Physicians KA. Physicians, their appearance, and the white coat. Am J Med. 2008;121(9):825–828. | ||
Alnasser Y, Alsaeed H, Beeshi NZA. Perception of pediatric physicians’ attire by children and parents within general pediatrics practice in Saudi Arabia. J Health Educ Res Dev. 2016;04(04):1–5. | ||
Taibah S. The Development of a Guideline for Teaching Professionalism in Dentistry in the Kingdom of Saudi Arabia. Bart and The London School of Medicine of Dentistry, University of London; 2011. | ||
GDC. Standards for dental professionals booklet [cited 2010 December]; 2005. Available from: https://www.google.com.sa/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=2ahUKEwiu2pyR2ofdAhURtRoKHVTFAY8QFjAAegQICBAC&url=https%3A%2F%2Fwww.gdc-uk.org%2Fapi%2Ffiles%2FOLD%2520Standards%2520for%2520Dental%2520Professionals.pdf&usg=AOvVaw2bsgWd7gdHGfxxI2kjscfh. Accessed August 29, 2018. | ||
ABIM. American Board of Internal Medicine Foundation [cited 2010 December]. Available from: http://abimfoundation.org/what-we-do/physician-charter. Accessed August 29, 2018. | ||
Ayoub F, Fares Y, Fares J. The psychological attitude of patients toward health practitioners in Lebanon. N Am J Med Sci. 2015;7(10):452–458. | ||
Katić M, Budak A, Ivanković D, et al. Patients’ views on the professional behaviour of family physicians. Fam Pract. 2001;18(1):42–47. | ||
Birhanu Z, Assefa T, Woldie M, Morankar S. Determinants of satisfaction with health care provider interactions at health centres in central Ethiopia: a cross sectional study. BMC Health Serv Res. 2010;10(10):78. | ||
Wiggins MN, Coker K, Hicks EK. Patient perceptions of professionalism: implications for residency education. Med Educ. 2009;43(1):28–33. | ||
Stern DT. Measuring Medical Professionalism. Oxford: Oxford University Press, Inc; 2006. | ||
Alnasser Y, Bin Nafisah H, Almubarakblama Z, Aleisa L, El Sarrag AB. Communication skills between physicians’ insights and parents’ perceptions in a teaching hospital in KSA. J Taibah Univ Med Sci. 2017;12(1):34–40. | ||
Kee W, Khoo H, Lim I, Koh M. Communication skills in patient-doctor interactions: learning from patient complaints health professions education [Internet]; 2017. Available from: https://doi.org/10.1016/j.hpe.2017.03.006. Accessed August 17, 2018. | ||
Sbaraini A, Carter SM, Evans RW, Blinkhorn A. Experiences of dental care: what do patients value? BMC Health Serv Res. 2012;12:177. | ||
Chen D, Lew R, Hershman W, Orlander J. A cross-sectional measurement of medical student empathy. J Gen Intern Med. 2007;22(10):1434–1438. | ||
Hojat M, Vergare MJ, Maxwell K, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Acad Med. 2009;84(9):1182–1191. | ||
ADEA. American Dental Education Association statement on professionalism in dental education [cited 2011 March]; 2009. Available from: http://www.adea.org/policy_advocacy/ethics_professionalism/Documents/ADEA_Statement_on_Professionalism_in_DentEd.pdf. Accessed August 17, 2018. | ||
Nomura K, Ohno M, Fujinuma Y, Ishikawa H. Patient autonomy preferences among hypertensive outpatients in a primary care setting in Japan. Intern Med. 2007;46(17):1403–1408. | ||
Lesser CS, Lucey CR, Egener B, Braddock CH, Linas SL, Levinson W. A behavioral and systems view of professionalism. JAMA. 2010;304(24):2732–2737. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.