Back to Journals » Patient Preference and Adherence » Volume 16
Dental Anxiety Screening and Management Practices in Dental Practice in Eastern Province, Saudi Arabia
Authors AlMuhaish L, AlArfaj A, AlGhannam M, AlMutiri H, Abuhassan S, Asiri A, Nazir MA ![]()
Received 14 October 2022
Accepted for publication 22 December 2022
Published 29 December 2022 Volume 2022:16 Pages 3429—3439
DOI https://doi.org/10.2147/PPA.S393399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Luba AlMuhaish,1 AlHanoof AlArfaj,1 Maha AlGhannam,1 Hadeel AlMutiri,1 Sarah Abuhassan,1 Amal Asiri,2 Muhammad Ashraf Nazir3
1College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Dental Education, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Department of Preventive Dental Sciences, College of Dentistry Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Muhammad Ashraf Nazir, Tel +966-543569615, Email [email protected]
Purpose: The purpose of the study was to investigate dental anxiety (DA) screening and management practices among dental professionals in Saudi Arabia. The study also evaluated correlation between patients’ self-reported DA and dentists’ ratings of patients’ DA.
Participants and Methods: This cross-sectional observational study included dentist/patient pairs (N = 279) from the Eastern Province of Saudi Arabia. The dentists responded to a questionnaire about their DA screening and management practices and they evaluated patients’ DA using the visual analogue scale (VAS). In addition, patients responded to the Modified Dental Anxiety Scale (MDAS) to measure their DA.
Results: About 15.1% of dentists reported using a published scale for screening DA in dental practice and Corah’s Dental Anxiety Scale and Dental Fear Survey were their main scales. However, 69.2% reported directly asking their patients about DA. The use of DA management technique was reported by 89.6% of the dentists. Approximately half of the participants (53%) reported receiving DA training in their undergraduate dentistry programs and 65.2% expressed their interest in continuing education courses related to DA. In multiple logistic regression analysis, statistically significant factors associated with DA screening practice included gender (AOR = 0.46, P = 0.037), place of work (AOR = 3.68, P = 0.039), and interest in continuing education courses (AOR = 3.21, P = 0.015). Monthly income (AOR = 0.20, P = 0.029) and directly asking patient about DA (AOR = 6.15, P = 0.025) were significant factors associated with management of patients with DA. The study also showed a significant but weak correlation between DA evaluated by the dentists and DA reported by the patients (rho = 0.185, P = 0.002).
Conclusion: The present study showed a low prevalence of DA screening practices among dentists. Dentists’ rating of patients’ DA weakly correlated with patients’ self-reported DA.
Keywords: dental anxiety, dental practice, anxiety screening, visual analog scale, modified dental anxiety scale
Introduction
Dental anxiety (DA) is one of the common problems in dental practice and an important obstacle to patient satisfaction.1 It is a significant risk indicator for poor oral health in terms of decayed, missing, and filled teeth and is associated with low oral health‐related quality of life.2,3 The vicious cycle of DA can lead to delay the dental treatment thus worsening the oral health status which in turn can further increase DA and continued avoidance of dental care.4 Researchers have shown that dentally anxious patients with dental insurance were significantly less likely to perform routine dental visits than non-anxious patients with dental insurance.5 Patients who avoid and skip dental appointments were also found to demonstrate increased DA scores.6
The literature indicates variations in the distribution of dentally anxious patients around the world. A study from Sweden reported that the prevalence of low to severe DA was 19.1% in a nationally representative sample of adult population.7 Other studies showed that 18% of the population in Brazil,8 32% of patients in the U.K,9 and 46% of Indian patients demonstrated DA.10 In Saudi Arabia, DA was observed among 27–51.6% of adult patients.11–13
Gender is among many factors implicated in DA and studies have suggested that females were more likely to report feelings of anxiety compared to males14 and even as children.15 An attempt to explain this gender predilection is the willingness of females to express their feelings of anxiety compared to their male counterparts who may not express their feelings due to social reasons.16 The role of education level was found to affect participants’ DA variably in studies where some researchers suggested an inverse relationship between the level of education and DA17 whereas others concluded the opposite.14,16 The reason of dental visit is also linked with DA as patients who requested appointments due to pain were more likely to experience DA.14 It was also found that low socioeconomic status was implicated in experiencing increased DA.17–19
The identification of patient’s level of DA prior to treatment can help dentists reduce their anxiety and improve them psychologically.20 The reduction in DA can result in effective patient management, improved dental care, and patient satisfaction.1,21 Therefore, dentists should use a standardized and validated DA scale for screening patients with DA for effective management. Validated DA scales should also provide the opportunity for the patients to safely reveal any anxiety they might have.22 It is known that the dentists who are trained in dental anxiety better manage and efficiently treat dentally anxious patients than those with no such training.23 Despite this, a study conducted in Australia stated that only one-third of clinicians reported having undergraduate training related to DA and less than half judged training appropriate.22
Heaton et al in the US reported that the use of dental fear survey or any other suitable scales can help dental clinicians effectively evaluate patient’s DA.24 However, the previous studies reported that only 3.7–20% of dentists in Australia and the UK used DA scale for screening patients’ DA.22,25 Recently, Hoglund et al showed low to moderate correlation between dental clinician and patient assessments of patients’ DA in Sweden.26
There is a high prevalence of DA among patients which negatively affects dental care and patient satisfaction. However, data are scant regarding DA screening practices among dentists in Saudi Arabia. The dental practitioners should use a validated DA scale to accurately identify patients with DA. The use of a validated DA scale can help dental practitioners evaluate levels of DA in their patients and use appropriate approaches to effectively manage these patients in their dental practice. Nevertheless, they should also have the ability to screen their patients with DA without using a validated scale. The study aims to investigate dental anxiety screening and management practices among dental practitioners in the Eastern Province, Saudi Arabia. The study also provided data on dentists’ evaluation of patients’ DA and patients’ self-reported DA.
Material and Methods
Study Design and Participants
This cross-sectional observational study included dentists and their patients from different cities (Dammam, Khobar, Jubail and Dhahran) of the Eastern Province, Kingdom of Saudi Arabia. The Eastern province is the biggest province by area and the third biggest by population. The population of the province was 5,148,598 with 60.28% of males and 39.72% of females in 2019. According to the Ministry of Health Saudi Arabia, dentist per 10,000 population ratio was 5.5 in the Kingdom.27
A sample of 286 dentist and patient pairs was calculated based on a 95% confidence level, ± 5% precision, size of population (N ≈ 3000), and 0.5 degree of variability in the population. The study included 572 participants (286 dentists and 286 patients). The dental professionals (general dentists, specialists, and consultants) of both gender from public and private clinics in the province participated in the study. Adult male and female patients from the responding dentists also participated in this study. A convenience sampling technique was used for the recruitment of participants.
Measurements of Study Variables
The dental professionals responded to questions regarding the use of DA scale in their dental practice and the types of scales employed for screening patients for DA such as Corah’s Dental Anxiety Scale, Modified Dental Anxiety Scale, Getz Dental Belief Index, Dental Fear Survey, and Spielberger State Trait Anxiety Inventory. The Corah Dental Anxiety Scale (CDAS) is highly used in both epidemiological and clinical research. However, the CDAS lacked an important factor about DA related to receiving dental injections. Therefore, an item about DA related to receiving dental injections was introduced into a modified scale and it was termed as the Modified Dental Anxiety Scale (MDAS). The MDAS scale includes additional question about local anesthetic injections as well as new easier answering options to each question.28
The dental professionals were also inquired about their anxiety management techniques, DA training in their undergraduate programs, and their interest in undertaking continuing education courses related to DA. These questions were taken from previous studies of dentists in the United Kingdom and Australia.20,22 In addition, the dentists evaluated patients’ anxiety using the VAS scale. The Visual analog scale (VAS) consists of 10 items and the score of each item ranges from 0 to 100.24 The questionnaire included information of dentists about gender, nationality, place of work, qualifications, monthly income, and years in dental practice.
The patients also self-reported their DA by responding to the Modified Dental Anxiety Scale (MDAS) in the waiting area before receiving dental treatment. The MDAS is the most commonly used dental anxiety questionnaire and it is highly reliable and valid.28 It is a simple scale and requires less time to be filled by the patients. The MDAS consists of 5 items about DA related to treatment tomorrow, sitting in waiting area, drilling of teeth, scaling and polishing, and local anesthetic injection. Each item uses a 5-options rating scale, ranging from “not anxious” to ‘extremely anxious.29
After returning the completed questionnaires, the patients went to their dentists for dental treatment and dentists evaluated patient’s DA and provided other responses in the questionnaire before providing dental treatment. The questionnaires for dentists and patients (10 dentist and patient pairs) were pretested which helped ensure the ease of understanding the questions by the respondents, evaluate time required to fill the questionnaire, and confirm content validity. No changes were made in the questionnaire as no problems were indicated during pretesting. Data of pre-testing were not included in the final analysis of the study.
Study Procedure and Ethics
The research team members (LA, AA, MA, HA, and SA) visited about 45 dental hospitals and clinics and provided paper copies of questionnaires to dentists and their patients. Permission to conduct the study was taken from the administration of clinics and hospitals. Each dentist was asked to fill one questionnaire for his/her patient who already provided responses about DA in the waiting area. The study participants were ensured about the confidentiality and privacy of their responses. They were informed about their voluntary participation in the study. All details about the procedures of the study including its benefits were discussed with the study participants. Written inform consents were obtained from dentists and patients who agreed to participate in the study. Ethical guidelines of the Declaration of Helsinki were followed during the conduct of the study. The Deanship of Scientific Research at Abdulrahman Bin Faisal University, Dammam provided ethical approval (IRB-2022-340) for the study.
Statistical Analysis
Data of study participants were entered in MS Excel (2010) and then transferred to SPSS Version 22.0 (IBM Corp. Armonk, NY, USA) for statistical analysis. Frequencies and relative frequency distribution were calculated for categorical variables and the means and standard deviations for continuous variables. Bivariate and multiple logistic regression analyses were performed to identify the factors associated with DA screening and management practices. For instance, DA screening and management practices were compared between participants with different monthly income levels. Pearson’s correlation test was performed to evaluate correlation between dentists’ rating of patient DA and patients’ self-reported DA. Statistical testing was performed at a significance level of p˂0.05.
Results
Of the total 286 dental professionals reached, 279 participated in the study with a response rate of 97.5%. Data of seven dentist/patient pairs were discarded due to missing information in their questionnaires. The study population included 64.5% of males and 35.5% of females and with a mean of 35.87 years with SD (±7.55). More than half of the participants (67%) were non-Saudis and general dentists (52.2%), had ≥10 years of dental practice experience (59.1%), and most had monthly income ≥10,000 SAR (70.6%) and worked in the private sector (94.3%). Regarding the practice of DA, 15.1% of participants used using a published scale for screening patients with DA and 89.6% used DA management techniques in their dental practice. Approximately half of the participants (53%) reported receiving DA training in their undergraduate dentistry programs and 65.2% expressed their interest in continuing education courses related to DA (Table 1). In the study, 4.3% of dental professionals reported that Corah’s Dental Anxiety Scale and Dental Fear Survey were their main scales for screening patients for DA (Figure 1). Behavioural management was the most common DA management technique (78.1%) and this was followed by relative analgesia (11.8%), and oral sedation (6.1%). Intravenous sedation (0.7%) and hypnosis (0.7%) were the least frequently used DA management procedures in the study (Figure 2).
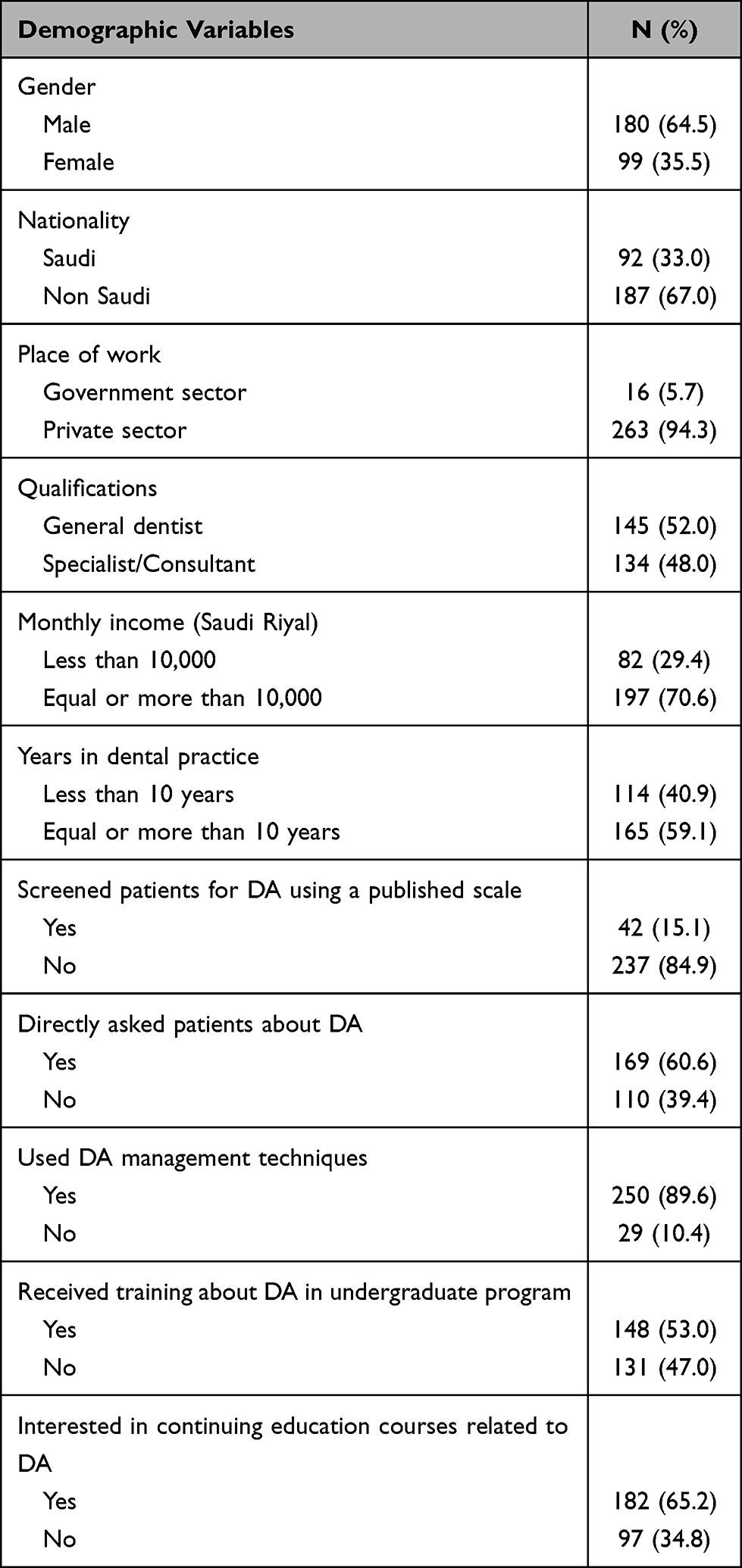 |
Table 1 Descriptive Statistics of Dental Professionals (N = 279) |
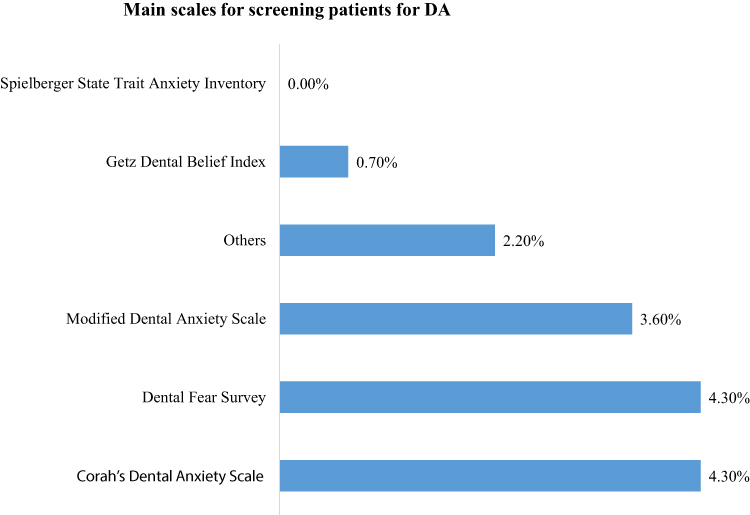 |
Figure 1 Dental professionals’ responses about main scales for screening patient for DA. |
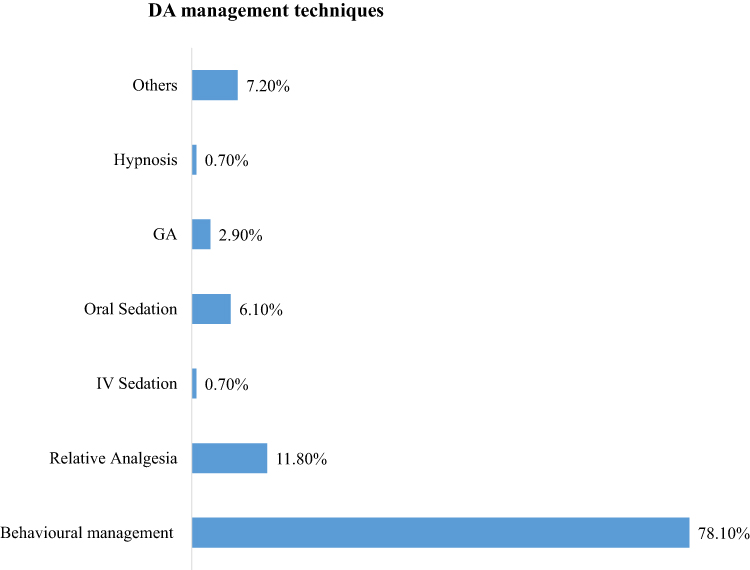 |
Figure 2 Dental professionals’ responses about DA management techniques. |
Table 2 shows results of bivariate analysis with odds ratio (OR), 95% confidence interval (CI), and p-value for each variable. In bivariate analysis, odds ratio statistically significant factors associated with dental professionals’ DA screening practices included gender (OR = 0.49, P = 0.033), directly asked patients about DA (OR = 2.34, P = 0.025), and interest in continuing education courses related to DA (OR = 3.66, P = 0.003). Regarding DA management practices, directly asked patients about DA (OR = 3.95, P = 0.001) and receiving training about DA in undergraduate program (OR = 8.49, P < 0.001) were statistically significant factors (Table 2).
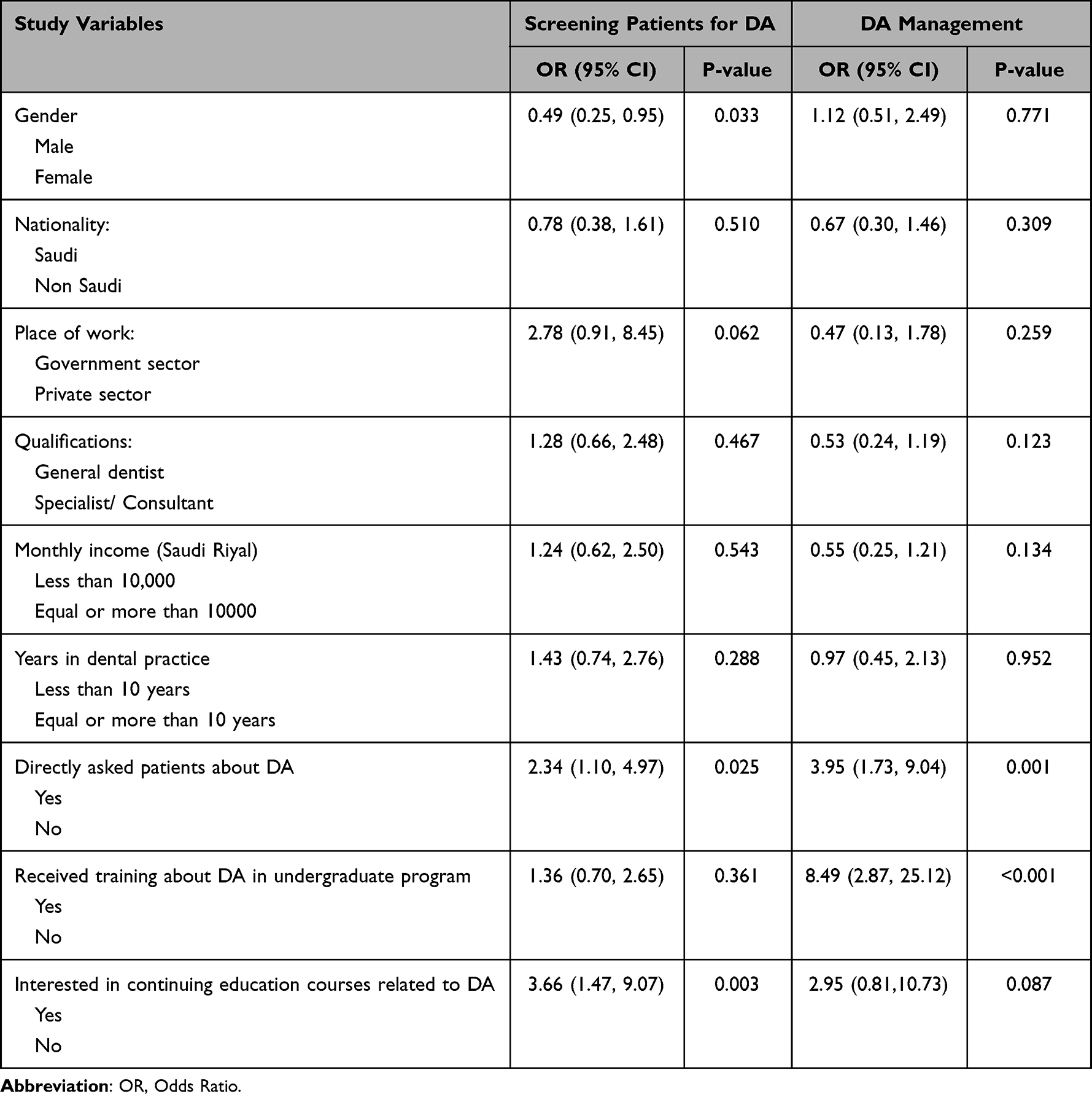 |
Table 2 Bivariate Analyses: Factors Associated with Screening and Managing Patients with DA Among Dental Professionals (N = 279) |
Tables 3 and 4 show the results of multiple logistic regression analyses with adjusted odds ratio (AOR), 95% confidence interval, and p-value. Multiple logistic regression backward selection final models removed unimportant independent variables such as nationality, qualification, etc. and retained important independent variables such as directly asking patients about DA etc.
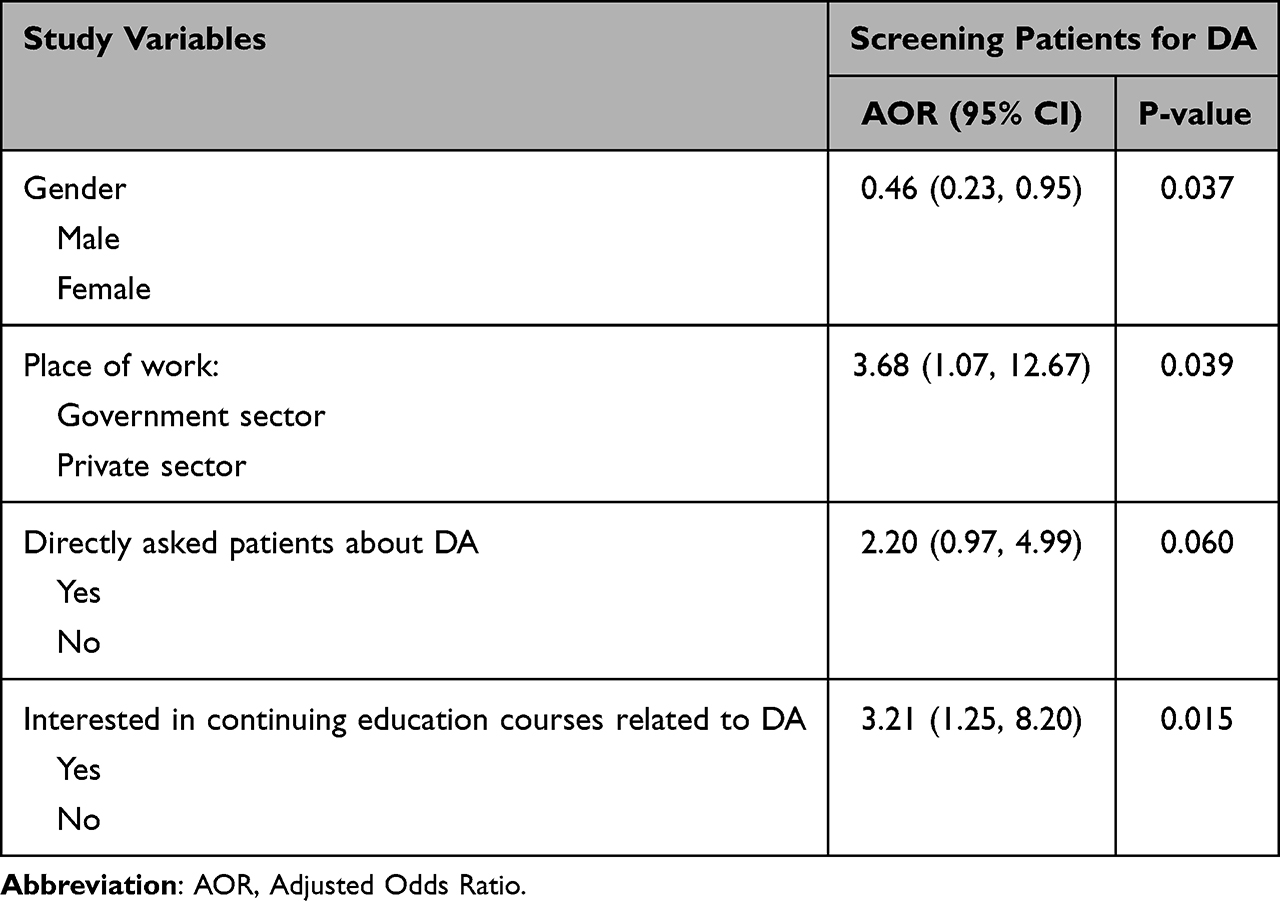 |
Table 3 Multiple Logistic Regression Analyses (Backward Selection Final Models): Factors Associated with Screening of DA Among Dental Professionals (N = 279) |
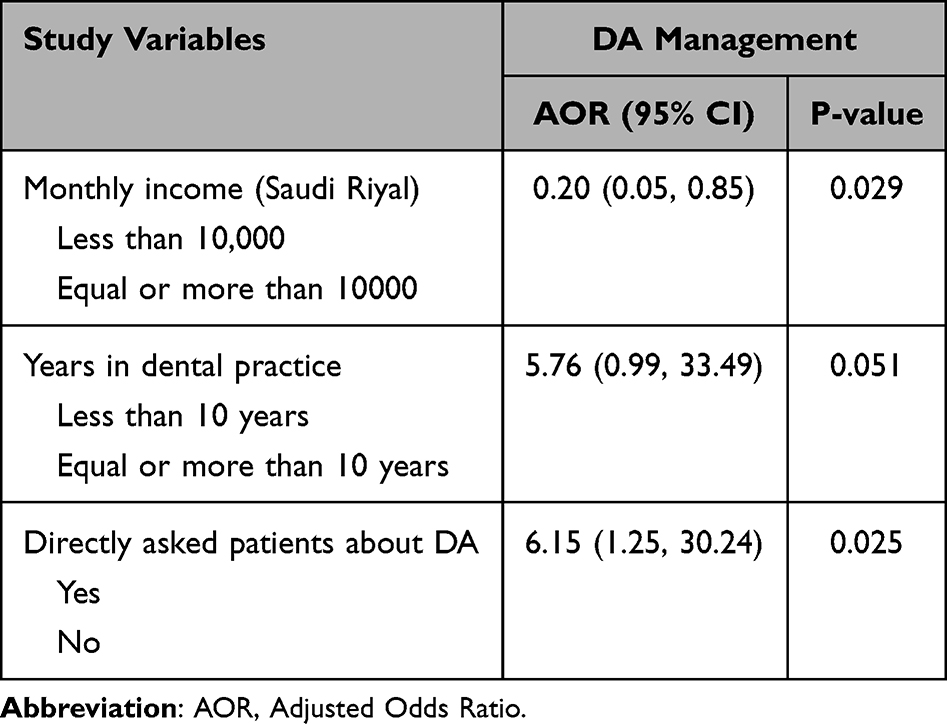 |
Table 4 Multiple Logistic Regression Analyses (Backward Selection Final Models): Factors Associated with Managing Patients with DA Among Dental Professionals (N = 279) |
DA screening practice was significantly associated with gender (AOR = 0.46, P = 0.037), place of work (AOR = 3.68, P = 0.039), and interest in continuing education courses (AOR = 3.21, P = 0.015) whereas directly asking patient about DA was a marginally significant factor in the study (AOR = 2.20, P = 0.060) (Table 3). On the other hand, monthly income (AOR = 0.20, P = 0.029) and directly asking patient about DA (AOR = 6.15, P = 0.025) were significant factors associated with management of patients with DA. Years in dental practice (AOR = 5.76, P = 0.051) was a marginally significant factor (Table 4).
Mean VAS score of patients was 19.92±18.87 and the score ranged from 0 to 83. Descriptive statistics of VAS used for the evaluation of patients’ DA by the dental professionals are shown in Table 5. Among items of VAS, the highest mean score (37.18±33.24) was related to patient asking question. This was followed by patient telling about his/her nervousness, anxiety, or scaredness (27.99±31.12), and patient showing increased muscle tension (24.38±26.40).
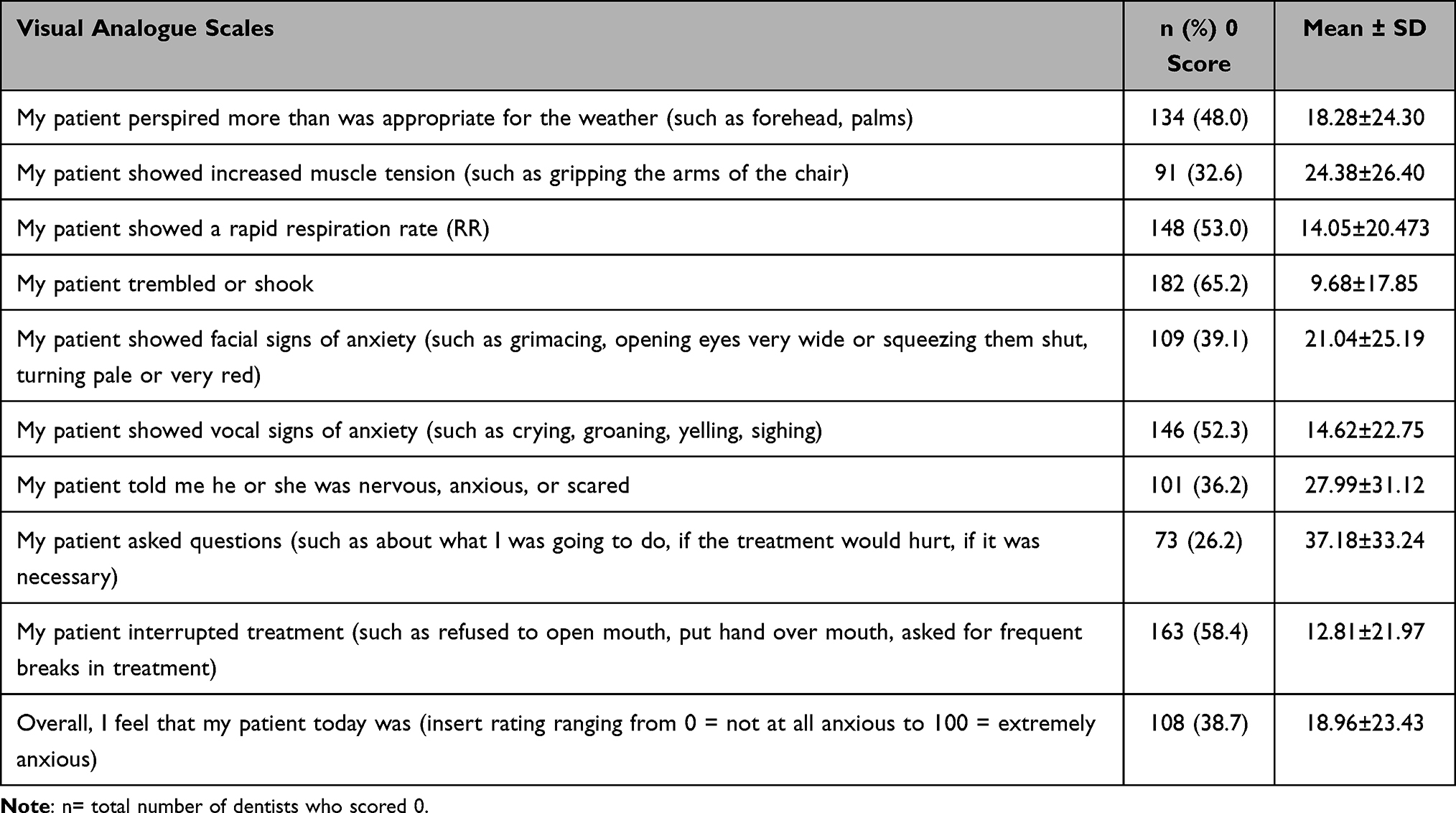 |
Table 5 Descriptive Statistics of VAS Used for the Evaluation of Patients’ DA by Dental Professionals (N = 279) |
The sample of patients consisted of 41.6% of males and 58.4% of females with a mean age of 32.31 years with SD (±10.75). According to self-reported DA of patients, the mean MDAS score was 10.68±4.73. MDAS score was calculated by adding the scores of five items (1 to 5) and the score ranged from 5 to 25. The relationship between dental professionals’ rating of patients’ DA (VAS score) and patients’ self-reported DA (MDAS score) was investigated by calculating Spearman correlation coefficients (rho) which measured the strength of association between VAS and MDAS. The study found a statistically significant correlation (rho = 0.185) between VAS and MDAS scores (P = 0.002).
Discussion
To the best of our knowledge, this is the first study that assessed the screening and management practices related to DA among dental professionals in Saudi Arabia. The finding from the present study showed that less than one-sixth of dental professionals (15.1%) diagnosed patient’s DA using a valid scale. This prevalence is higher than reported by Armfield et al, who demonstrated that only 3.7% of dentists used a validated DA scale for screening patients with DA in Australia.22 In a recent study by Ogawa et al 9.7% of dental practitioners were shown to use questionnaires to measure DA among patients in Japan.30 On the other hand, the findings of a study by Dailey et al observed the use of a valid screening tool among 20% of dentists in the U.K.25 The differences in study participants, methods of screening for DA including non-accessibility of validated instruments, and knowledge and undergraduate training regarding the use of anxiety assessment questionnaires may account for variations in prevalence estimates in different countries.
In the literature, DA is linked to cognitive elements which consist of subjective factors in the processing of dental-related stimuli such as the patient’s personal perceptions of the dentist communication ability, professionalism, and control or command during dental appointment. It is also related to perceptions related to the types of dental procedures and invasiveness or difficulty that the patient may undergo.31 Non cognitive elements mainly pertain to previous traumatic experiences within a dental setting.32 However, not all respondents with high levels of DA report traumatic dental experiences as numerous pathways exist in the development of DA.33 Future studies should therefore carefully examine how both traumatic and non-traumatic negative situations contribute to the emergence of DA.
Regarding the gender, male dental professionals were significantly less likely than female counterparts to use of DA scale in the present study. This finding is supported by a previous study where more female than male dentists were shown to use DA screening tool.22 More females screening patients with DA in our study can be attributed to females’ sensitive nature of identifying the signs of anxiety in their patients. On the contrary, evidence also indicated significant association of gender with the use of DA questionnaire and male dentists were more likely to use DA questionnaire than female dentists.25 Moreover, gender differences regarding the use of DA tool were not observed in a previous study.30
The MDAS questionnaire has many advantages including being concise, practical with high validity and is ubiquitously used in the literature to assess DA. These qualities make it beneficial in comparing results from different studies and in systematic reviewing of the literature.34 The MDAS was the most frequently used dental anxiety questionnaire among a sample of dental practitioners in the U.K.25 The use of the Index of Dental Anxiety and Fear was the most common in a sample of Australian dentists.22 Visual Analog Scale and Modified Dental Anxiety Scale were frequently used scales among those dentists who used questionnaires for the diagnosis of DA among patients in Japan.30 The dental professionals in the present study commonly used Corah’ Dental Anxiety Scale and Dental Fear Survey instruments for the assessment of DA.
More than half of our sample directly asked their patients about DA. Similar results were reported in a previous study where 48.5% of Australian dentists directly asked their patients about DA.22 Although most dentists reported directly asking patients about DA, however, such response may not accurately diagnose and understand the level of patients’ DA. Therefore, use of standardized instruments for the identification of DA and patients’ self-reported DA are critical for effective patient management. The present study also found that dental professionals who directly asked their patients about DA were 2.2 times more likely to use a valid screening tool and 6.15 times more likely to use DA management technique. It is possible that many dentists ask their patients about DA first and then they use a validated instrument to screen them for DA and manage their anxiety accordingly Given increased likelihood of this group of dentists for using valid tool and management, they should be exposed to continuing education activities so that they are better prepared for diagnosis and management of patients with DA.
Findings of the present study showed that most dental professionals (89.6%) used DA management techniques and behavioral management was the most common technique followed by relative analgesia. The study also showed that monthly income and years in dental practice were significantly associated with management of DA. The dentists with low monthly income were less likely to manage patients with DA than those with high income. It is possible that financial situations of dentists affect their decision-making and consequently patient management.35 The dental professionals with less than 10 years of experience were 5.76 times more likely to employ DA management techniques in their dental practice. It is understandable that younger dentists are more likely to receive and retain DA-related knowledge and skills gained in dental school which may account for this phenomenon.22 More than half of dentists in our study reported receiving training about DA in undergraduate dentistry program.
The majority (65.2%) of dental professionals in the present study expressed their interest in continuing education activities related to DA. This is in contrast with the finding of an Australian study which confirmed that 36.9% of dentists showed interest in continuing professional development course in dental anxiety.22 The interest in continuing education course among our sample of dentists remained a statistically significant factor associated with the practice of valid DA assessment tool. This is in line with evidence that indicated that continuing education programs for dentists improved their knowledge, motivation for learning, clinical skills, and quality of patient care.36
Low use of a valid screening tool among dentists can be related to their belief that they accurately identifying patients with DA based on their clinical judgement.25 However, low correlation between DA reported by patients and diagnosed by dentists in the present study show difference in patients’ self-reported DA and dentists’ ratings of patients’ DA. This is consistent with the results of a recent study by Höglund et al who demonstrated that clinicians rated patients’ DA lower than DA reported by the patients in Sweden.26 Similarly, evidence from the US reported low to moderate correlation between dentists’ evaluation of patients’ DA and patients’ self-reported DA.24 This shows that dentists have difficulty in correctly identifying DA among patients which highlights the importance of using a validated tool for the diagnosis of DA before dental treatment. The implementation of DA screening tools requires collaborative and integrated initiatives involving dentists, dental team, patients, decision makers in health-care systems, and dental academia.
The present study has several limitations. The study included dentists and patients from the eastern region of Saudi Arabia, which limited generalizability of results to dentists and patients in other regions of the country. There is also a possibility of selection bias as a convenience sample of participants were recruited for the study. Moreover, cross-sectional study design provides information of study variables at one point in time and cannot be used to infer temporal relationship between variables. The study included MDAS and VAS scales for patients and dentists, respectively. These scales are short and hence are prone to random errors by study participants.
Conclusions
This study showed a low prevalence of DA screening practices among dental professional. However, most dental professionals directly asked patients about DA and used DA management techniques and behavior management was the most common technique. Approximately half of the sample received DA training in their undergraduate programs and the majority expressed their interest in continuing education courses related to DA. Dentists’ rating of patients’ DA weakly correlated with patients’ self-reported DA.
Dental curricula should be updated to provide adequate training to undergraduate dental students about the prevalence, causes, diagnosis including the use of validated tools, and management approaches related to DA. Similarly, health-care organizations should organize continuing education courses to improve knowledge and skills of dentists for effective screening and management of patients with DA.
Acknowledgments
The authors thank Faisal Masud and Abdulrahman Aljeraisy for their help in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Corah NL, O’Shea RM, Ayer WA. Dentists’ management of patients’ fear and anxiety. J Am Dent Assoc. 1985;110(5):734–736. doi:10.14219/jada.archive.1985.0427
2. Carlsson V, Hakeberg M, Wide Boman U. Associations between dental anxiety, sense of coherence, oral health-related quality of life and health behavior--a national Swedish cross-sectional survey. BMC Oral Health. 2015;15:100. doi:10.1186/s12903-015-0088-5
3. Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. 2009;37(3):220–230. doi:10.1111/j.1600-0528.2009.00468.x
4. Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. 2007;7:1. doi:10.1186/1472-6831-7-1
5. Sohn W, Ismail AI. Regular dental visits and dental anxiety in an adult dentate population. J Am Dent Assoc. 2005;136(1):58–66; quiz 90–1. doi:10.14219/jada.archive.2005.0027
6. Nicolas E, Collado V, Faulks D, Bullier B, Hennequin M. A national cross-sectional survey of dental anxiety in the French adult population. BMC Oral Health. 2007;7:12. doi:10.1186/1472-6831-7-12
7. Svensson L, Hakeberg M, Boman UW. Dental anxiety, concomitant factors and change in prevalence over 50 years. Community Dent Health. 2016;33(2):121–126.
8. Ferreira CM, Gurgel-Filho ED, Bönecker-Valverde G, et al. Dental anxiety: score, prevalence and behavior. Revista Brasileira em Promocao da Saude. 2004;17(2):51. doi:10.5020/18061230.2004.p51
9. Nuttall NM, Bradnock G, White D, Morris J, Nunn J. Dental attendance in 1998 and implications for the future. Br Dent J. 2001;190(4):177–182. doi:10.1038/sj.bdj.4800918
10. Malvania EA, Ajithkrishnan CG. Prevalence and socio-demographic correlates of dental anxiety among a group of adult patients attending a dental institution in Vadodara city, Gujarat, India. Indian J Dent Res. 2011;22(1):179–180. doi:10.4103/0970-9290.79989
11. Gaffar BO, Alagl AS, Al-Ansari AA. The prevalence, causes, and relativity of dental anxiety in adult patients to irregular dental visits. Saudi Med J. 2014;35(6):598–603.
12. Fayad MI, Elbieh A, Baig MN, Alruwaili SA. Prevalence of dental anxiety among dental patients in Saudi Arabia. J Int Soc Prev Community Dent. 2017;7(2):100–104. doi:10.4103/jispcd.JISPCD_19_17
13. Quteish Taani DS. Dental fear among a young adult Saudian population. Int Dent J. 2001;51(2):62–66. doi:10.1002/j.1875-595X.2001.tb00823.x
14. Jeddy N, Nithya S, Radhika T, Jeddy N. Dental anxiety and influencing factors: a cross-sectional questionnaire-based survey. Indian J Dent Res. 2018;29(1):10–15. doi:10.4103/ijdr.IJDR_33_17
15. Kothari S, Gurunathan D. Factors influencing anxiety levels in children undergoing dental treatment in an undergraduate clinic. J Family Med Prim Care. 2019;8(6):2036–2041. doi:10.4103/jfmpc.jfmpc_229_19
16. Waseem A, Hussain V, Zahid RB, Shahbaz M. Reasons for not seeking early dental care in patients presenting in the exodontia department at a Tertiary Care Hospital in Lahore, Pakistan. Professional Med J. 2021;28(08):1107–1113. doi:10.29309/TPMJ/2021.28.08.5044
17. Khan S, Alqannass NM, Alwadei MM, et al. Assessment of the relationship between dental anxiety and oral health-related quality of life. J Pharm Bioallied Sci. 2021;13(Suppl 1):S359–S62. doi:10.4103/jpbs.JPBS_742_20
18. Sukumaran I, Taylor S, Thomson WM. The prevalence and impact of dental anxiety among adult New Zealanders. Int Dent J. 2020;71(2):122–126. doi:10.1111/idj.12613
19. Bhardwaj SS, Almulhim B, Alghamdi S, Alaasaf A, Bhardwaj A. Effect of age, gender and socioeconomic status on perceived dental anxiety. Revista Argentina de Clínica Psicológica. 2021;30(1):525.
20. Dailey YM, Humphris GM, Lennon MA. Reducing patients’ state anxiety in general dental practice: a randomized controlled trial. J Dent Res. 2002;81(5):319–322. doi:10.1177/154405910208100506
21. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013;58(4):390–407; quiz 531. doi:10.1111/adj.12118
22. Armfield JM, Mohan H, Luzzi L, Chrisopoulos S. Dental anxiety screening practices and self-reported training needs among Australian dentists. Aust Dent J. 2014;59(4):464–472. doi:10.1111/adj.12211
23. Uziel N, Meyerson J, Winocur E, Nabriski O, Eli I. Management of the dentally anxious patient: the dentist’s perspective. Oral Health Prev Dent. 2019;17(1):35–41. doi:10.3290/j.ohpd.a41985
24. Heaton LJ, Carlson CR, Smith TA, Baer RA, de Leeuw R. Predicting anxiety during dental treatment using patients’self-reports: less is more. J Am Dent Assoc. 2007;138(2):188–95; quiz 248–9. doi:10.14219/jada.archive.2007.0135
25. Dailey YM, Humphris GM, Lennon MA. The use of dental anxiety questionnaires: a survey of a group of UK dental practitioners. Br Dent J. 2001;190(8):450–453. doi:10.1038/sj.bdj.4801000
26. Höglund M, Bågesund M, Shahnavaz S, Wårdh I. Evaluation of the ability of dental clinicians to rate dental anxiety. Eur J Oral Sci. 2019;127(5):455–461. doi:10.1111/eos.12648
27. Ministry of Health. Health indicators. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Indicator/Pages/Indicator-1440.aspx.
28. Humphris G, Crawford JR, Hill K, Gilbert A, Freeman R. UK population norms for the modified dental anxiety scale with percentile calculator: adult dental health survey 2009 results. BMC Oral Health. 2013;13:29. doi:10.1186/1472-6831-13-29
29. Caltabiano ML, Croker F, Page L, et al. Dental anxiety in patients attending a student dental clinic. BMC Oral Health. 2018;18(1):48. doi:10.1186/s12903-018-0507-5
30. Ogawa M, Ayuse T, Fujisawa T, Sato S, Ayuse T. The methods and use of questionnaires for the diagnosis of dental phobia by Japanese dental practitioners specializing in special needs dentistry and dental anesthesiology: a cross-sectional study. BMC Oral Health. 2022;22(1):38. doi:10.1186/s12903-022-02071-y
31. Scandurra C, Gasparro R. The role of cognitive and non-cognitive factors in dental anxiety: a mediation model. Eur J Oral Sci. 2021;129(4):e12793. doi:10.1111/eos.12793
32. Scandurra C, Gasparro R, Dolce P, et al. The Italian validation of the level of exposure-dental experiences questionnaire. Applied Sciences. 2020;10(3):1143. doi:10.3390/app10031143
33. De Jongh A, van Eeden A, van Houtem C. Do traumatic events have more impact on the development of dental anxiety than negative, non-traumatic events? Eur J Oral Sci. 2017;125(3):202–207. doi:10.1111/eos.12348
34. Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009;9:20. doi:10.1186/1472-6831-9-20
35. Kateeb ET, McKernan SC, Gaeth GJ, et al. Predicting dentists’ decisions: a choice-based conjoint analysis of Medicaid participation. J Public Health Dent. 2016;76(3):171–178. doi:10.1111/jphd.12126
36. Al-Ansari A, Nazir MA. Dentists’ responses about the effectiveness of continuing education activities. Eur J Dent Educ. 2018;22(4):e737–e44. doi:10.1111/eje.12388
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.