Back to Journals » International Medical Case Reports Journal » Volume 19
Delayed Union of a Distal Tibia–Fibula Fracture Following Traditional Bone Setter Management: A Case Report from Rural Uganda
Authors Olwit G ![]() , Mugisha AI
, Mugisha AI ![]()
Received 8 February 2026
Accepted for publication 3 April 2026
Published 9 April 2026 Volume 2026:19 602138
DOI https://doi.org/10.2147/IMCRJ.S602138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Gerald Olwit,1 Aime Ishimwe Mugisha2
1Department of Orthopaedic Surgery, Kabale University School of Medicine, Kabale, Uganda; 2Department of Orthopaedic Surgery, University of Rwanda, College of Medicine and Health Sciences, School of Medicine and Pharmacy, Kigali, Rwanda
Correspondence: Gerald Olwit, Department of Orthopaedic Surgery, Kabale University School of Medicine, P.O.Box 317, Kabale, Uganda, Tel +256 776822110, Email [email protected] Aime Ishimwe Mugisha, Department of Orthopaedic Surgery, University of Rwanda, College of Medicine and Health Sciences, School of Medicine and Pharmacy, Kigali, Rwanda, Tel +250 783 360 199, Email [email protected]
Background: Among the most common fractures involving the long bones of the body are those occurring in the tibia, and they are often associated with substantial morbidity, especially in instances where healing takes a long time to occur. Delayed union has been recognized as a complication of fractures, and it has been attributed to improper stabilization of the fracture, late referral to a specialist, and improper treatment. In low- and middle-income countries, traditional bone setters (TBS) are often the first port of call for musculoskeletal injuries, and this has been linked to adverse outcomes in fractures.
Case Presentation: A 28-year-old male was found to have a fractured tibia and fibula as a result of a football injury. The patient was first seen and treated by a TBS and presented to the orthopedic clinic three months later with pain, deformity, and inability to bear weight. He was found to have a fracture gap with minimal callus and cortical bone, indicating delayed union. The patient was taken to surgery, where an intramedullary nail was inserted to treat the fracture. At four weeks post-surgery, radiographs demonstrated early callus formation along the tibial cortex and maintenance of fracture alignment. Functionally, the patient tolerated partial weight-bearing with improved limb mobility and reduced pain.
Conclusion: This case highlights the orthopedic and public health implications of delayed presentation after traditional fracture care and demonstrates that timely intramedullary nailing can achieve favorable early radiographic and functional outcomes. Early presentation to an orthopedic facility is crucial in avoiding complications in the management of fractures.
Keywords: tibial fractures, intramedullary nailing, delayed union, traditional bone setter, fracture management
Introduction
Amongst the most common long bone injuries in humans worldwide, tibial fractures are at the top, especially in young and active individuals. Most tibial fractures have been known to unite in as short a time usually three to six months if promptly treated with appropriate reduction and fixation.1 Delayed union, which is a condition of prolonged fracture healing with persistent fracture lines, inadequate callus formation, and incomplete bone bridging, is an important condition in the management of tibial fractures. Factors contributing to delayed union include instability of the fracture, inadequate immobilization, compromise of soft tissues, infection, and late presentation to specialized care.2
While intramedullary nailing is the standard treatment for unstable tibia–fibula fractures globally, this case highlights the consequences of prior non-standard management by a TBS, resulting in delayed union and functional impairment.
In developing and middle-income countries, TBS are usually the first source of management for patients with musculoskeletal injuries because of their accessibility, acceptability, and cost-effectiveness.3 However, TBS management has been known to cause several complications associated with delayed union, malunion, nonunion, chronic infection, and functional disability.3 Such complications have resulted in increased disability and may require complex surgical procedures.4
Despite the high incidence of TBS utilization, there is a scarcity of documented cases from sub-Saharan Africa on delayed union of tibia–fibula fractures, followed by surgical treatment. Documenting such cases is highly valuable in terms of the orthopedic and public health significance of delayed treatment of such fractures. Secondly, such cases provide a platform to generate evidence on the need for timely intervention in such cases. This case report of delayed union of a tibia–fibula fracture, following TBS treatment of a young adult male, serves to highlight various lessons on the therapeutic, social, and cultural significance of such cases.
Case Presentation
A 28-year-old male presented to the orthopedic clinic in Kabale, Uganda, in November 2025 with persistent right leg pain, visible deformity, and inability to bear weight following a football-related injury sustained three months earlier. Initial evaluation at the time of injury included radiographic imaging, which demonstrated an oblique fracture involving the distal tibia and fibula (Figure 1).
 |
Figure 1 Initial radiographs of the right leg demonstrating an oblique distal tibia–fibula fracture with preserved joint alignment. Despite limitations in image annotation clarity, the fracture configuration and alignment are adequately visualized. |
He has BMI of 22.5 kg/m2, non-smoker, and no significant comorbidities. Neurovascular status was intact, soft tissues were preserved, and ankle range of motion was limited by pain. The fracture was classified as AO 43-A2 (oblique distal tibia–fibula fracture).
The patient was initially managed by a TBS, who applied a crude splint without proper immobilization. No specific weight-bearing restrictions were advised, and no follow-up imaging was performed during this period. However, over the subsequent three months, he experienced no clinical improvement and continued to report pain, functional limitation, and progressive deformity of the affected limb, prompting presentation to our facility for further assessment and management.
On physical examination, the right leg exhibited an obvious deformity with intact distal neurovascular status. The soft tissues were intact, without open wounds or signs of infection. Range of motion at the knee was preserved, but ankle dorsiflexion and plantarflexion were limited due to pain and deformity (Figure 2). Repeat radiographs obtained at presentation revealed a persistent fracture gap with minimal callus formation and poor cortical bridging at the fracture site (Figure 3), findings consistent with impaired fracture healing.
 |
Figure 2 Clinical photograph of the right lower limb at presentation, showing an obvious deformity of the distal leg consistent with inadequate fracture reduction and stabilization following initial traditional bone setter management. |
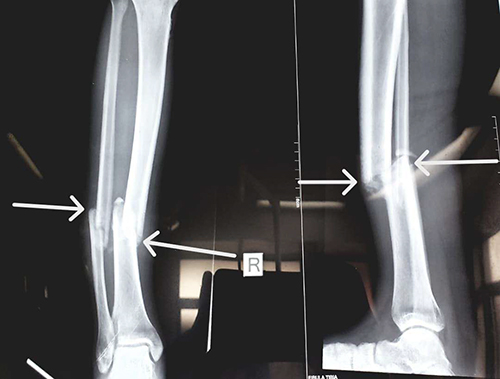 |
Figure 3 Follow-up radiographs of the right leg obtained three months post-injury, revealing a persistent fracture gap, minimal callus formation, and poor cortical bridging of the distal tibia and fibula, consistent with delayed union. |
In view of the prolonged healing duration and radiographic features, a diagnosis of delayed union was established. Open reduction and internal fixation were performed via a standard anterior approach. Two proximal and two distal interlocking screws were placed. Fibrous tissue at the fracture site was debrided to enhance healing. Reaming of the medullary canal was performed prior to nail insertion. Perioperative analgesia included intravenous paracetamol (1 g every 8 hours) and morphine (2 mg every 6 hours) for the first 24 hours.
At the fourth week follow-up, the patient demonstrated notable clinical improvement, including reduced pain, healed surgical incisions without evidence of infection, improved limb alignment, and tolerance to partial weight bearing. Follow-up radiographs confirmed satisfactory positioning of the intramedullary nail with intact interlocking screws and maintained fracture alignment. Early signs of fracture healing were observed, including a less distinct fracture line and early callus formation, particularly along the tibial cortex, although complete cortical bridging had not yet been achieved.
Discussion
This case report details a young adult male who underwent successful surgical salvage using intramedullary nailing after developing a delayed union of a distal tibia–fibula fracture after initial management by a traditional bone setter. The main characteristics include radiographic evidence of minimal callus formation and poor cortical bridging, persistent deformity, delayed presentation three months after injury, and early clinical and radiologic improvement following definitive orthopedic intervention. These results demonstrate the efficacy of evidence-based surgical management as well as the orthopedic consequences of postponing fracture care.
Failure to attain progressive fracture healing within the anticipated timeframe, usually three to six months, without fulfilling nonunion criteria, is commonly referred to as delayed union of tibial fractures.1,2 Characteristic radiographic features include insufficient cortical bridging, limited callus formation, and persistent fracture lines. Because of its subcutaneous location, relatively poor soft tissue envelope, susceptibility to instability, and compromised blood supply, the tibia is especially vulnerable to impaired healing.2,5 Inadequate immobilization, fracture instability, infection, soft tissue injury, and improper or delayed initial management are known risk factors.2,5 In this instance, prolonged instability and improper fixation during the early post-injury phase probably played a major role in the observed delayed union.
The learning points from this case include the importance of early presentation to formal orthopedic care, counseling patients on the potential risks of TBS treatment, and ensuring prompt re-evaluation for those who choose TBS care. Additionally, intramedullary nailing can serve as an effective salvage procedure even after delayed presentation, emphasizing the need for timely intervention and education.
In many regions of sub-Saharan Africa, TBS are still heavily involved in the healing process of musculoskeletal trauma. Cultural beliefs, accessibility, affordability, and the scarcity of formal orthopedic services all have an impact on their widespread use.5 High rates of TBS management complications, such as delayed union, malunion, nonunion, chronic infection, compartment syndrome, and permanent disability, have been reported in numerous studies.3,4,6 Following TBS treatment in Nigeria, Odatuwa-Omagbemi et al reported a significant burden of fracture-related complications, with delayed hospital presentation frequently requiring more complicated surgical procedures.3 Similar results have been documented in various African contexts, highlighting the case’s regional significance.4,6
Delayed union in this patient likely resulted from insufficient fracture stability and impaired periosteal blood supply due to improper TBS management. The tibia’s subcutaneous location makes it particularly vulnerable to delayed healing. Controlled micromotion induced by intramedullary nailing promotes callus formation, enabling successful salvage. Similar studies in sub-Saharan Africa have reported high rates of delayed union and malunion following TBS management, emphasizing the challenges of non-standardized fracture care.3,6–8
In this case, the patient initially sought TBS care due to its accessibility, lower cost, and cultural acceptability. Barriers to early hospital presentation may include limited awareness, financial constraints, and geographic accessibility.9,10 This case demonstrates that evidence-based surgical intervention can achieve favorable early outcomes even after delayed presentation.
For the majority of diaphyseal tibial fractures, intramedullary nailing is still the best option. It also works well for delayed union and aseptic nonunion.2,7 Stable internal fixation, early mobilization, periosteal blood supply preservation, and controlled micromotion to promote fracture healing are all provided by this technique.2,7 In this particular case, intramedullary nailing produced stable fixation, satisfactory alignment, and early radiologic healing signs at four weeks, all of which are in line with results documented in the literature.3,8 Early functional improvement and absence of postoperative complications further support its role as an effective salvage procedure in similar contexts.
This case illustrates the orthopedic consequences of delayed presentation following TBS treatment, highlighting the need for early referral, patient counselling, and timely surgical intervention. The successful use of intramedullary nailing despite delayed union emphasizes that evidence-based orthopedic care can still achieve positive outcomes. These observations form the core learning points for both local and international clinicians.3,8 Furthermore, reducing the long-term disability burden linked to musculoskeletal injuries requires increasing access to reasonably priced orthopedic trauma care.
Postoperative and follow-up radiographic images were not available for inclusion, which limits visual documentation of fracture healing despite descriptive reporting of radiological progress. The quality of the initial radiographic image was limited by cropping and overlapping annotations, which could not be fully corrected, potentially affecting visual clarity. However, this case does provide valuable insight into a common yet underreported clinical condition and reiterates valuable lessons in clinical practice.
Limitations
One limitation of this study relates to the quality of the initial radiographic image. The image had been previously cropped and was originally obtained under suboptimal conditions, which reduced its overall clarity. Additionally, the original, uncropped version is no longer available for verification or further enhancement. These constraints could not be fully corrected and may have affected the visual clarity and, to some extent, the interpretation of the radiographic findings.
Another limitation of this case report is the absence of postoperative radiographic imaging and the relatively short duration of follow-up. Postoperative X-rays were not available for inclusion as they were not retained in the accessible patient records, limiting objective assessment of fracture alignment and healing. In addition, follow-up was restricted to 4 weeks due to loss of the patient to further follow-up, which precluded evaluation of longer-term clinical and functional outcomes. These factors may affect the completeness of outcome assessment and have been acknowledged as important constraints of this report.
Conclusion
In conclusion, delayed union in tibia–fibula fractures is a serious complication of improper initial management. Early detection, referral, patient education on the risks of traditional fracture care, and timely surgical intervention with intramedullary nailing can lead to favorable outcomes. This case reinforces Strengthening health systems and promoting community education are critical to prevent similar complications and improve musculoskeletal care in low-resource settings. It also provides clear learning points: educate patients on the risks of non-standard fracture management, encourage early presentation, and consider surgical salvage promptly if complications arise.
Data Sharing Statement
All data generated or analyzed during this case report are included in the published article.
Ethics Approval and Consent to Participate
Ethical approval was not required for this case report in accordance with local institutional policies. Written informed consent was obtained from the patient for participation and publication of this case.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying data. A copy of the written consent is available for review by the Editor upon request.
Acknowledgments
The authors thank the patient for providing consent and cooperation during the preparation of this case report. We also acknowledge the Department of Orthopedic Surgery of Kabale University School of Medicine under Dr. Rodney Mugarura and Dr. Asaph Owamukamaeli for their significant contributions to this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare no competing interests.
References
1. Bilge O. The epidemiology of adult fractures according to the AO/OTA fracture classification. Turk J Trauma Emerg Surg. 2020. doi:10.14744/tjtes.2020.26374
2. Mukhopadhaya J, Jain AK. AO principles of fracture management. Indian J Orthop. 2019;53(1):217–6. doi:10.4103/ortho.IJOrtho_598_18
3. Odatuwa-Omagbemi DO, Adiki TO, Elachi CI, Bafor A. Complications of traditional bone setters (TBS) treatment of musculoskeletal injuries: experience in a private setting in Warri, South-South Nigeria. Pan Afr Med J. 2018;30. doi:10.11604/pamj.2018.30.189.15730
4. Doumgba Antoine D, Mapouka Pierre Alfred I, Nouganga Emmanuel D, et al. The consequences of traditional treatments on bone fractures. Study about 92 cases recorded in Bangui, Central Africa Republic. Acta Sci Med Sci. 2022;6(4):110–114.
5. Zafari H, Moein SA, Razzaghof M, Mortazavi SMJ. The contributing factors of nonunion bone fractures: a brief review. J Orthop Spine Trauma. 2022. doi:10.18502/jost.v8i2.9309
6. Afsar SS. Frequency of complications among trauma patients treated by traditional bone setters. J Popul Ther Clin Pharmacol. 2023;7966–7971. doi:10.53555/jptcp.v30i1.6997
7. Zelle BA, Boni G. Safe surgical technique: intramedullary nail fixation of tibial shaft fractures. Patient Saf Surg. 2015;9(1):40. doi:10.1186/s13037-015-0086-1
8. Musculoskeletal health [Internet]; 2026. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
9. Njai A, Nak Y, Kah M, et al. Understanding barriers to orthopaedic and trauma care delivery in the gambia utilizing the social ecological model: a scoping review. J Global Surg. 2025;1(2):172–186. doi:10.52648/JoGS.1243
10. Moldovan F, Moldovan L. Assessment of patient matters in healthcare facilities. Healthcare. 2024;12(3):325. doi:10.3390/healthcare12030325
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.