Back to Journals » International Medical Case Reports Journal » Volume 19
Delayed Intrathoracic Textile Foreign Body Following Penetrating Shrapnel Injury Presenting with Expectoration of Fabric-Like Material and Chronic Middle-Lobe Destruction: A Case Report
Authors Aldakak MA ![]() , Hdeoa H, Ahmad R, Abbas Y
, Hdeoa H, Ahmad R, Abbas Y ![]() , Al Jabban Y, Dandashy A, Chaban H
, Al Jabban Y, Dandashy A, Chaban H
Received 22 February 2026
Accepted for publication 23 April 2026
Published 27 April 2026 Volume 2026:19 604561
DOI https://doi.org/10.2147/IMCRJ.S604561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Mohammad Alaa Aldakak,1 Hamza Hdeoa,1 Raneem Ahmad,2 Youssef Abbas,2 Yousef Al Jabban,2 Asmaa Dandashy,2 Hussain Chaban2
1Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic; 2National University Hospital, Faculty of Medicine, Damascus University, Damascus, Syrian Arab Republic
Correspondence: Mohammad Alaa Aldakak, Email [email protected]
Background: Retained intrathoracic and tracheobronchial foreign bodies are uncommon but important causes of chronic respiratory symptoms. Diagnosis may be delayed because presentations are nonspecific and retained textile material is often radiolucent. Such material can lead to chronic infection, pleural adhesions, and progressive lung destruction.
Case Presentation: A 31-year-old Syrian male military serviceman and active smoker (20 pack-years) presented with a long-standing intermittent cough that had worsened over one week and become productive of white sputum. He also reported a single episode of expectorating suspected textile material, along with fatigue, weakness, and night sweats, but no fever, dyspnea, hemoptysis, or chest pain. Years earlier, he had sustained a penetrating shrapnel injury complicated by pneumothorax and later purulent pleural effusion requiring tube thoracostomy. On admission, examination suggested right basal involvement; laboratory studies were unremarkable, and tuberculosis testing was negative. Chest CT showed a heterogeneous right-sided lesion with right middle-lobe atelectatic change and tree-in-bud opacities, suggesting chronic inflammatory or infectious disease. Bronchoscopy revealed friable, bleeding mucosa and distortion at the right middle-lobe bronchial orifice.
Case discussion: Due to persistent symptoms and chronic localized abnormalities, right thoracotomy was performed. Dense pleural adhesions were found, and an intrathoracic textile foreign body was removed, most likely implanted during the prior traumatic injury. The right middle lobe was extensively destroyed with purulent change, requiring right middle lobectomy. Histopathology showed fibrosis, architectural destruction, fibroblastic foci, honeycomb change, and chronic inflammation consistent with a UIP pattern; adhesion fragments showed acute-on-chronic foreign body-associated inflammation.
Conclusion: Radiolucent textile foreign bodies may remain undetected for years after penetrating thoracic trauma and later present with chronic respiratory symptoms and localized destructive infection. Once irreversible damage is established, thoracotomy with foreign body removal and lobectomy may be necessary.
Keywords: intrathoracic foreign body, penetrating thoracic trauma, textile foreign body, middle lobectomy, case report
Introduction
Retained intrathoracic and tracheobronchial foreign bodies have been reported after penetrating trauma, aspiration, airway instrumentation, and vascular procedures; however, these entities differ in mechanism, diagnostic approach, and management.1,2 Delayed presentation has been described even after prolonged periods, including a bullet identified a decade after gunshot injury, a dried pepper inhaled seven years earlier, and a fish bone retained for five years.3–5 Clinical manifestations may be atypical, including rhonchus with a “valve-like” chest sensation, intermittent hemoptysis, or pneumothorax with atelectasis.2,5,6 As a result, retained foreign bodies may be misclassified as more common respiratory disorders or neoplasia, as illustrated by reports of a tracheal foreign body initially treated as chronic obstructive pulmonary disease and an airway foreign body mimicking an endobronchial tumor on computed tomography (CT).6,7 Infectious complications are also well described, including lung abscess caused by a retained rusty nail and abscess associated with retained epicardial pacemaker leads after incomplete extraction.8,9 Retained textile material is particularly important because radiolucent fragments may be missed on imaging and can sustain chronic inflammation, dense adhesions, and fistulization, as reported in association with gastropleurobronchial fistula caused by a retained surgical sponge.10 Although bronchoscopy remains central for airway foreign bodies, thoracoscopy or thoracotomy may be required when infection, adhesions, or parenchymal destruction preclude endoscopic management.6,8,9,11 Collectively, these reports indicate that persistent or unusual respiratory symptoms, including expectoration of foreign material, should prompt consideration of a retained foreign body and timely escalation to endoscopic or surgical exploration when appropriate.3,7,12 The work has been reported in line with the SCARE criteria.13
Case Presentation
A 31-year-old Syrian man, a military serviceman and active smoker (20 pack-years), presented with a long-standing intermittent cough that had worsened over the preceding week and become productive of white sputum. He reported a single episode of expectorating suspected textile material, associated with fatigue, generalized weakness, and night sweats, without fever, chills, dyspnea, hemoptysis, or chest pain. His medical history was notable for gastroesophageal reflux disease treated with omeprazole. He denied alcohol consumption, had no known drug allergies, and had no relevant family history.
Approximately six years earlier, he sustained a war-related penetrating shrapnel injury with an entry wound in the right upper arm and an exit wound through the right fifth intercostal space along the mid-axillary line, complicated by a right pneumothorax. At that time, he underwent removal of superficial chest wall shrapnel and right-sided tube thoracostomy for 4 days, after which he was discharged in good condition. Approximately one week later, he developed fever, chills, productive cough, vomiting, marked fatigue, and weakness. Diagnostic thoracentesis revealed a right-sided purulent pleural effusion, and a right chest tube was reinserted and maintained for approximately 2 weeks until drainage ceased. Thereafter, owing to irregular follow-up, he experienced intermittent dry cough that gradually progressed over time.
On admission, he was hemodynamically stable, with a blood pressure of 130/70 mmHg, heart rate of 75 beats/min, temperature of 37°C, and oxygen saturation of 95% on room air. There was no pallor, jaundice, lymphadenopathy, or digital clubbing. Chest examination revealed increased tactile vocal fremitus, dullness to percussion, and reduced breath sounds over the lower half of the right lung field. Cardiovascular, abdominal, neurologic, and musculoskeletal examinations were otherwise unremarkable. A chest radiograph demonstrated a right-sided basal opacity (Figure 1). Laboratory testing, including complete blood count and C-reactive protein, was within normal ranges. Electrocardiography and transthoracic echocardiography were normal. Tuberculosis evaluation showed negative sputum smears for acid-fast bacilli on three separate occasions, and bronchoscopy lavage testing, including Xpert MTB/RIF, was negative. Pulmonary function testing demonstrated preserved spirometry (FEV1 3.30 L; FVC 4.48 L). Chest computed tomography revealed a heterogeneous right-sided lesion with segmental atelectatic change involving the right middle lobe and associated inflammatory changes, including branching nodular opacities demonstrating a tree-in-bud pattern (Figures 2 and 3), suggestive of a chronic inflammatory/infectious process on an inflammatory background. Flexible bronchoscopy demonstrated normal findings in the larynx, trachea, and left bronchial tree. In the right bronchial tree, congestion and bleeding were observed at the orifice of the right middle lobe bronchus with mucosal distortion (Figure 4), and bronchial lavage was obtained.
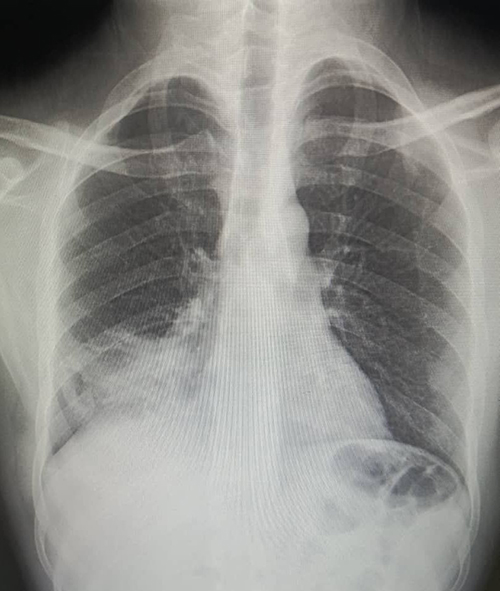 |
Figure 1 Chest radiograph at presentation demonstrating a right-sided basal opacity consistent with chronic inflammatory/infectious involvement of the right lung. |
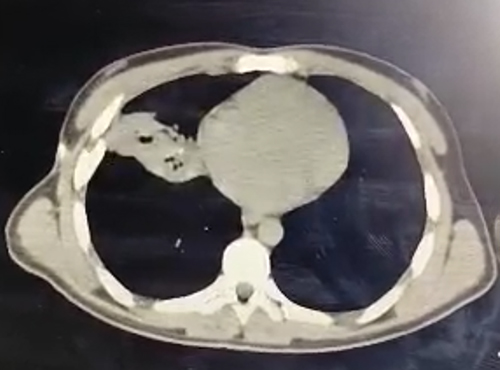 |
Figure 2 Axial chest CT (mediastinal window) demonstrating a heterogeneous right-sided parenchymal lesion adjacent to the cardiac silhouette, corresponding to right middle-lobe involvement in the clinical setting. |
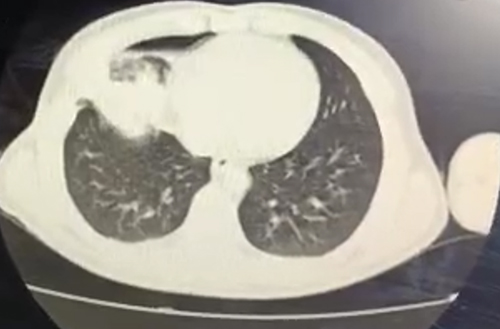 |
Figure 3 Axial chest CT (lung window) demonstrating right middle-lobe atelectasis/consolidation with associated inflammatory changes; branching nodular opacities are compatible with an endobronchial spread pattern (“tree-in-bud”). |
 |
Figure 4 Flexible bronchoscopy image showing congested, friable mucosa with bleeding and distortion at the orifice of the right middle-lobe bronchus. |
Because of persistent symptoms, chronic radiologic abnormalities, and bronchoscopic findings localizing disease to the right middle lobe without identification of a removable endobronchial foreign body, surgical management was undertaken. Under general anesthesia with double-lumen endotracheal intubation and left lateral decubitus positioning, a right thoracotomy was performed through the sixth intercostal space. Dense pleural adhesions were encountered, including firm adhesions between the right middle lobe and the diaphragm. During adhesiolysis, an intrathoracic textile foreign body was identified and removed; based on the clinical context and gross appearance, it was considered most consistent with an implanted fragment of clothing material introduced at the time of the penetrating injury. Thorough pleural lavage was subsequently performed. The right middle lobe appeared extensively destroyed with purulent changes, and a right middle lobectomy was performed. The hilar structures were isolated, ligated, and divided, and the lobar bronchus was transected and closed. Lung re-expansion was satisfactory and intraoperative air-leak testing was negative; a chest tube was placed.
Gross pathological examination of the resected right middle lobe measured approximately 15×10 × 2.5 cm and showed a poorly circumscribed hemorrhagic beige focus measuring approximately 3.3 cm near the hilum. Histopathological examination, showed subpleural and paraseptal fibrosis with architectural destruction, dense fibrosis, marked fibroblastic foci, honeycomb change, and chronic inflammatory infiltrate, consistent with a usual interstitial pneumonia (UIP) pattern; three hilar lymph nodes showed reactive changes (Figure 5). Examination of pleural adhesion fragments revealed acute-on-chronic inflammation with neutrophils and hemosiderin-laden macrophages, vascular congestion, and fibrosis, consistent with a chronic foreign body–associated inflammatory reaction. The postoperative course was uneventful, with marked symptomatic improvement, and the patient was discharged in good general condition after chest tube removal.
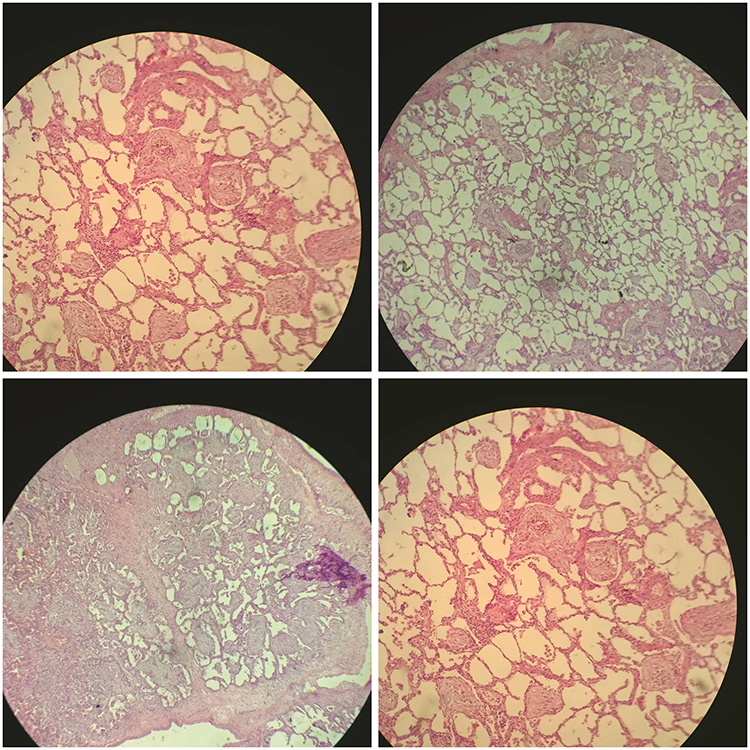 |
Figure 5 Representative H&E-stained histopathology from the resected right middle lobe showing a UIP pattern with architectural distortion and dense fibrosis, fibroblastic foci, and honeycomb change, accompanied by chronic inflammatory infiltrates (composite panel). |
Discussion
This case highlights the potential for delayed and clinically significant complications of retained intrathoracic foreign bodies after penetrating thoracic trauma. Previous reports show that foreign material introduced during trauma may remain unrecognized for prolonged periods before causing chronic pulmonary sequelae.1,8 Delayed presentation after long-term foreign-body retention has also been described, supporting the plausibility of a prolonged silent interval before reevaluation.3
One of the most unusual features in our patient was the expectoration of suspected textile material. Although no fistulous tract was directly demonstrated intraoperatively, this finding raises the possibility that chronic inflammation and infection around the retained textile fragment led to erosion or communication with the bronchial tree, allowing intermittent shedding of material into the airway. A similar pathophysiologic concept has been described in retained textile foreign bodies associated with persistent inflammation, adhesions, and fistulization.10 In our case, bronchoscopy showed congestion, bleeding, and mucosal distortion at the orifice of the right middle lobe bronchus, further localizing the disease to that region, but did not identify a removable endobronchial foreign body.
The delayed diagnosis in this case was likely facilitated by the radiolucent nature of textile material and by the nonspecific clinical presentation. Retained textiles may be missed on imaging when no radiopaque marker is present and may instead present through secondary complications such as chronic infection, adhesions, and parenchymal destruction.10 Our patient ultimately required thoracotomy because of persistent symptoms, chronic radiologic abnormalities, dense pleural adhesions, and extensive destruction of the right middle lobe. This is consistent with prior reports showing that surgical intervention, including pulmonary resection, may be necessary when foreign-body retention is associated with suppuration, abscess formation, or irreversible parenchymal damage.8,9
The histopathological findings in the resected lobe were reported as subpleural and paraseptal fibrosis with architectural destruction, dense fibrosis, marked fibroblastic foci, honeycomb change, and chronic inflammatory infiltrate, consistent with a UIP pattern. In this clinical setting, these findings were identified within a chronically infected and structurally destroyed lobe adjacent to a retained textile foreign body. Although a foreign body-associated chronic inflammatory process likely contributed substantially to the local tissue damage, the patient’s 20 pack-year smoking history may also have contributed to chronic parenchymal injury and may have influenced the fibrotic changes observed. Given the localized nature of the surgical specimen, the respective contributions of smoking-related injury and foreign body-associated inflammation cannot be determined with certainty.
This case emphasizes that radiolucent intrathoracic textile foreign bodies should be considered in patients with atypical chronic respiratory symptoms and a history of penetrating thoracic trauma, particularly when the clinical course is prolonged and imaging suggests localized destructive inflammatory disease. Early recognition may help reduce diagnostic delay, but once chronic suppuration and irreversible lobar destruction are established, thoracotomy with foreign body removal and anatomic resection may be required for definitive source control.9,10
Limitations
We were unable to perform material characterization or fiber analysis of the extracted textile fragment, and no direct intraoperative proof of a bronchopleural or bronchial fistulous tract was identified. Accordingly, the origin of the textile material and the precise mechanism of expectoration are presented as the most plausible interpretation based on the clinical history, operative findings, and pathology rather than as definitive proof.10,14
Conclusion
This case highlights that radiolucent intrathoracic textile foreign bodies may remain undetected for years after penetrating thoracic trauma and later present with atypical chronic respiratory symptoms, including expectoration of suspected textile material, together with localized destructive pulmonary infection. In patients with a relevant trauma history and persistent focal thoracic abnormalities, retained foreign material should be considered early to reduce diagnostic delay. Once chronic suppuration, dense adhesions, and irreversible lobar destruction are established, thoracotomy with foreign body removal and lobectomy may be required for definitive source control.
Data Sharing Statement
Available from the corresponding author upon reasonable request.
Ethics Approval Statement
Institutional Review Board (IRB) approval is not required for de-identified single case reports or case histories, in accordance with institutional policies.
Patient Consent Statement
Written informed consent was obtained from the patient for publication and any accompanying images.
Funding
There is no funding to report.
Disclosure
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
References
1. Zhao W, Chu M, Ma L, et al. Penetrating chest trauma caused by a falling metallic bar: a case report. J Thorac Dis. 2023;15(7):4027–7. doi:10.21037/jtd-23-767
2. Cherrez-Ojeda I, Felix M, Vanegas E, Mata VL, Jimenez FM, Ugarte Fornell LG. Rhonchus and valve-like sensation as initial manifestations of long-standing foreign body aspiration: a case report. Am J Case Rep. 2019;20:70–73. doi:10.12659/AJCR.913405
3. Ahmed AA, Warsame AM, Özdamir H, Yilmaz Y, Salad NM, Mohamed YG. Spontaneous expulsion of 10 years retained intrathoracic foreign body (bullet) from left main bronchus: a case report. Ann Med Surg. 2022;83:104640. doi:10.1016/j.amsu.2022.104640
4. Lei W, Gan ZY, Liang YF, et al. Airway foreign body caused by pepper inhalation 7 years previously retrieved under conscious sedation with spontaneous respiration: a case report. J Int Med Res. 2022;50(3):3000605221086146. doi:10.1177/03000605221086146
5. Nakatsukasa T, Kamohara R, Tanaka Y, et al. Thoracoscopic removal of a fish bone retained in the lung for five years without the need for lung resection: a case report. Surg Case Rep. 2025;11(1):cr.25–0467. doi:10.70352/scrj.cr.25-0467
6. Ha JH, Jeong BH. Airway foreign body mimicking an endobronchial tumor presenting with pneumothorax in an adult: a case report. Medicina. 2021;57(1):50. doi:10.3390/medicina57010050
7. Zhong LJ, Yan M, Wang Y, Zhou DQ, Tang JM, Xiang SH. An unusual tracheal foreign body in a middle-aged male with a 15-year history of coal use: a case report. BMC Med Imaging. 2021;21(1):35. doi:10.1186/s12880-021-00561-z
8. Kawamoto N, Okita R, Furukawa M, et al. Penetrating pulmonary injury due to a thrown rusty nail while using a lawn mower: a case report. AME Case Rep. 2020;4:35. doi:10.21037/acr-20-87
9. Bahar AR, Jawadi MH, Cardozo S, Kumar K, Baciewicz FA Jr. Retained permanent epicardial pacemaker leads and lung abscess: a diagnostic and surgical challenge. JACC Case Rep. 2025;31:106318. doi:10.1016/j.jaccas.2025.106318
10. Warsame AM, Ali AM, Ekim T, Salad AA, Mohamed YG. Gastropleurobronchial fistula: lessons learned from delayed diagnosis of retained surgical sponge after abdominal surgery—a case report and review of the literature. J Med Case Rep. 2025;20(1):2. doi:10.1186/s13256-025-05055-y
11. Louis M, Tapia R, Grabill N, Bongu N, Singh H, Hastings JC. Missed foreign body aspiration: fentanyl patch leading to severe pneumonia and empyema. Cureus. 2025;17(1):e77931. doi:10.7759/cureus.77931
12. Eliçora A, Sezer HF, Topçu S, Çardaközü T. Tracheobronchial tooth and dental prosthesis aspirations: 15 cases. J Cardiothorac Surg. 2023;18(1):78. doi:10.1186/s13019-023-02178-5
13. Kerwan A, Al-Jabir A, Mathew G, et al. Revised Surgical CAse REport (SCARE) guideline: an update for the age of artificial intelligence. Premier J Sci. 2025;10:100079.
14. Dogan K, Kaptanoglu M, Onen A, Saba T. Unusual sites of uncommon endobronchial foreign bodies: reports of four cases. Scand Cardiovasc J. 1999;33(5):309–311. doi:10.1080/14017439950141588
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.