Back to Journals » Risk Management and Healthcare Policy » Volume 14
Delay in Seeking Institutional Delivery Service Utilization and Associated Factors Among Mothers Attending Jimma Medical Center, Jimma, Ethiopia
Authors Awel S ![]() , Bagilkar VV
, Bagilkar VV ![]() , Fekecha B
, Fekecha B ![]()
Received 8 December 2020
Accepted for publication 6 March 2021
Published 23 March 2021 Volume 2021:14 Pages 1255—1262
DOI https://doi.org/10.2147/RMHP.S295683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Samira Awel, Vinod V Bagilkar, Bekana Fekecha
School of Nursing and Midwifery, College of Health Science, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Samira Awel
School of Nursing and Midwifery, College of Health Science, Institute of Health, Jimma University, P.O. Box: 378, Jimma, Ethiopia
Tel +251 921918489
Email [email protected]
Background: Pregnancy and childbirth-related complications are unpredictable; however, it is preventable by timely care-seeking to obstetric care service.
Objective: To assess delay in seeking institutional delivery service utilization and associated factors among mothers attending Jimma medical center, Southwest Ethiopia.
Methods: Facility-based cross-sectional study design was employed. The sample size was determined by a single population proportion formula. Data were collected from 405 mothers by face-to-face interview and entered using epi-data version 3.1, then exported to SPSS version 23 for analysis. Binary and multivariable logistic regression analysis with 95% CI for odds ratio (OR) was used to identify significant factors.
Results: The prevalence of delay in seeking institutional delivery service utilization was 189 (46.7%). Husbands’ educational status was found to be significantly associated with a maternal delay in seeking care, (AOR= 4.9; 95% CI=2.1– 11.3). Unemployed mothers and mothers with a low income had shown higher odds of delay (AOR= 6.0; 95% CI=1.7– 21.2), (AOR=2.1; 95% CI=1.2– 3.7) respectively. Similarly, mothers who live > 10 kilometers from health facility delayed about 2times, (AOR=1.8; 95% CI= 1.0– 3.2). Moreover, the likelihood of mothers with no antenatal care follow-up was found to have higher delay than mothers who have antenatal care follow-up (AOR =2.8; 95% CI =1.1– 6.7).
Conclusion: Delay in seeking institutional delivery service was high. Factors such as the husband’s educational status, distance from the health facility, income, Antenatal care follow-up, and occupation of the mother were found significant factors of delay in seeking care. Therefore, it is important to reduce delay in seeking care for institutional delivery service utilization by working on barriers, plus empowering women, promoting antenatal care, and education.
Keywords: delay in seeking, institutional delivery service, Ethiopia
Introduction
Maternal mortality is an overwhelming event with bad consequences. The burden of maternal death is high in developing countries.1,2 Worldwide 800 women die every day from these over 99% i.e. 287,000 annual deaths occur in developing countries.3 Every pregnant woman is at risk of obstetric complications.4,5 Though maternal deaths have been declining over the past decades, they remain a concern particularly in the less developed regions.6
Maternal mortality reduction remains a priority and WHO issued strategies toward the termination of preventable maternal deaths under the sustainable development goal (SDG). It is well-known that all of the major causes of maternal death can be treated with effective and timely clinical interventions. However, achieving the SDG requires continual venture in maternal health research programs and policy at the global level and very attentive action in countries. The government cannot achieve a reduction in maternal mortality rate unless works on issues such as maternal delays in seeking care.7,8
Even though the majority of maternal deaths can be prevented, by early recognition and treatment, different factors can hinder women’s access to emergency obstetric services. Several factors were found to delay access and utilization of emergency obstetric care among women in sub-Saharan Africa. These barriers are inter-dependent and occurred at multiple levels either home, on the way to health facilities, or at the facilities.9,10
Maternal health outcomes may also be determined by the time-of-service utilization hence delay in service utilization is an imperative thing in defining maternal wellbeing.11 Despite current increased efforts in Ethiopia including launching many midwifery training programs and comprehensive emergency obstetric and newborn care (CEmONC), much more needs to be accomplished for the reduction of maternal mortality rates. If mothers have early health care seeking behavior and factors which cause delay are reduced, mothers can be saved from preventable deaths as the majority of maternal deaths are preventable by timely care-seeking to obstetric care service.12,13 Though several studies on delivery service utilization were conducted in Ethiopia, little is known about the delay in seeking care for institutional delivery. Therefore, this study aimed to assess delay in seeking institutional delivery service utilization and associated factors among mothers attending JMC, Jimma town southwest Ethiopia.
Knowing delay in seeking care and factors associated with the delay in seeking institutional delivery service utilization among mothers are important to aid the planning of action to reduce and control the mortality and morbidity rate. It is hoped that the provision of such vital information would inform better strategy in the bridging and/or elimination of the barriers that stand in the way of accessing institutional delivery. Furthermore, this study will be used for policymakers, patients as well as health care providers to take precautions by showing the level of maternal delay in seeking care for delivery service utilization and its associated factors at Jimma medical center (JMC).
Methods and Materials
Study Setting and Period
The study was conducted at Jimma medical center (JMC) from April 1 to April 30, 2019. JMC is one of the oldest public hospitals in the country. It is located in Jimma town 352 km southwest of Addis Ababa the capital of Ethiopia. JMC is the only teaching and referral hospital in the southwestern part of the country which serves as a referral hospital for nearly 15 million populations from Oromia, Gambella, SNNPR, and Benishangul regional states.
Study Design
A facility-based cross-sectional study design was employed.
Population
All mothers delivered at JMC were a source of population. Those mothers available to utilize delivery service at JMC during the data collection period were considered.
Eligibility Criteria
Mothers who present at JMC for delivery service during the data collection period and giving consent to participate were included. Mothers who were on severe medical condition, unable to respond, women who utilized maternal waiting home, those who were admitted in the ward before labor and stayed until delivery were excluded.
Sample Size Determination and Participants
The sample size was determined by using the single population proportion formula (n=(Zα/2)2p(1-p)/d2). Considering the prevalence of maternal delay for utilizing institutional delivery 40.1% (P=0.401) that is taken from a facility-based cross-sectional study conducted in Hadiya southern Ethiopia.14 Standard normal distribution of the Z-value at 95% confidence interval (CI) =1.96, and 5% margin of error become 369 and by adding none respondents’ rate 10% of sample size, the final sample size was 406. All mothers who present to receive the services of delivery at JMC during the data collection period were included consecutively until the required sample size was obtained.
Study Variables
Dependent Variable
The time interval between recognition of the labor and decide to seek institutional delivery service. Time taken ≥1 hr to decide to seek care is considered as delay and less than an hour considered no delay.
Independent Variables
Maternal age, educational status of the mother, educational status of the husband, decision-making power, place of residence, monthly income, mothers, and husband’s occupation.
Obstetric Related Factors
Parity, ANC follow up, ANC frequency, history of chronic illness during pregnancy, history of abortion, maternal knowledge on danger sign and birth preparedness.
Accessibility of the Health Facility
Distance, cost of transportation, transportation availability, accessibility of road.
Data Collection Instrument and Procedure
A structured questionnaire was adapted from a similar study conducted in southern Ethiopia and the survey tools developed by JHPIEGO maternal and neonatal health program.14,20 The adapted English questionnaire was translated into Afaan Oromo and Amharic then it was retranslated back into English by two independent language experts, to check its consistency.
Data Analysis and Presentation
The collected data were entered, cleaned, coded into Epi-Data version 3.1 statistical software, and then exported to SPSS windows version 23 for further analyses. Descriptive statistics, binary and multivariable logistic regressions analyses were performed. All the variables were entered into binary logistic regression and those explanatory variables with a p-value ≤ of 0.25 were considered as a candidate for multivariable logistic regression, multi-collinearity between the candidate variables was checked and odds ratios with 95% CI were computed and variables having a p-value less than 0.05 in the multivariable logistic regression model were considered as significantly associated with the dependent variable.Model fitness was checked using Hosmer and Lemeshow goodness of fitness test.Finally, the result of the analyses was presented in texts, tables, and charts accordingly.
Data Quality Assurance
To check the clarity of the tool pretest was done at Agaro general hospital among 5% of the total sample size that is on 20 women and modifications were done on unclear questions. Data were collected through a face-to-face interview by four diploma midwives and one BSC nurse was recruited for supervision. The training was given for both data collectors and supervisor for two days on the objective of the study, data collection procedures, and handling ethical issues (privacy, confidentiality, cultural sensitivity, etc.). Besides, the investigators were also closely followed the data collection procedures.
Ethical Approval and Consent to Participate
Ethical clearance obtained from the institutional review board (IRB) of Jimma University, institute of health science with the reference number of THRPGD/502/2019. An official letter was written from the school of nursing and midwifery. Written informed consent was obtained from study participant for those aged 18 and above. For those participants, less than18 years of age written informed consent was obtained from a parent or guardian. Participation in the study was voluntary. All interviewers were instructed on how to comply with confidentiality practices for all clients both during and after data collection by using coded questionnaires. Participants were informed of the option to stay out of the study at any point during the interview. All responses were kept confidential and anonymous. This study was conducted in accordance with the Declaration of Helsinki.
Results
Sociodemographic Characteristics of the Study
A total of 405 mothers participated; making the response rate 99.7%. The majority of respondents or 234 (57.8%) of mothers reside in urban. 129 (31.9%) of them were in the age range of 25 to 29 and the mean age (±SD) was 25.58 (±5.34) (Table 1).
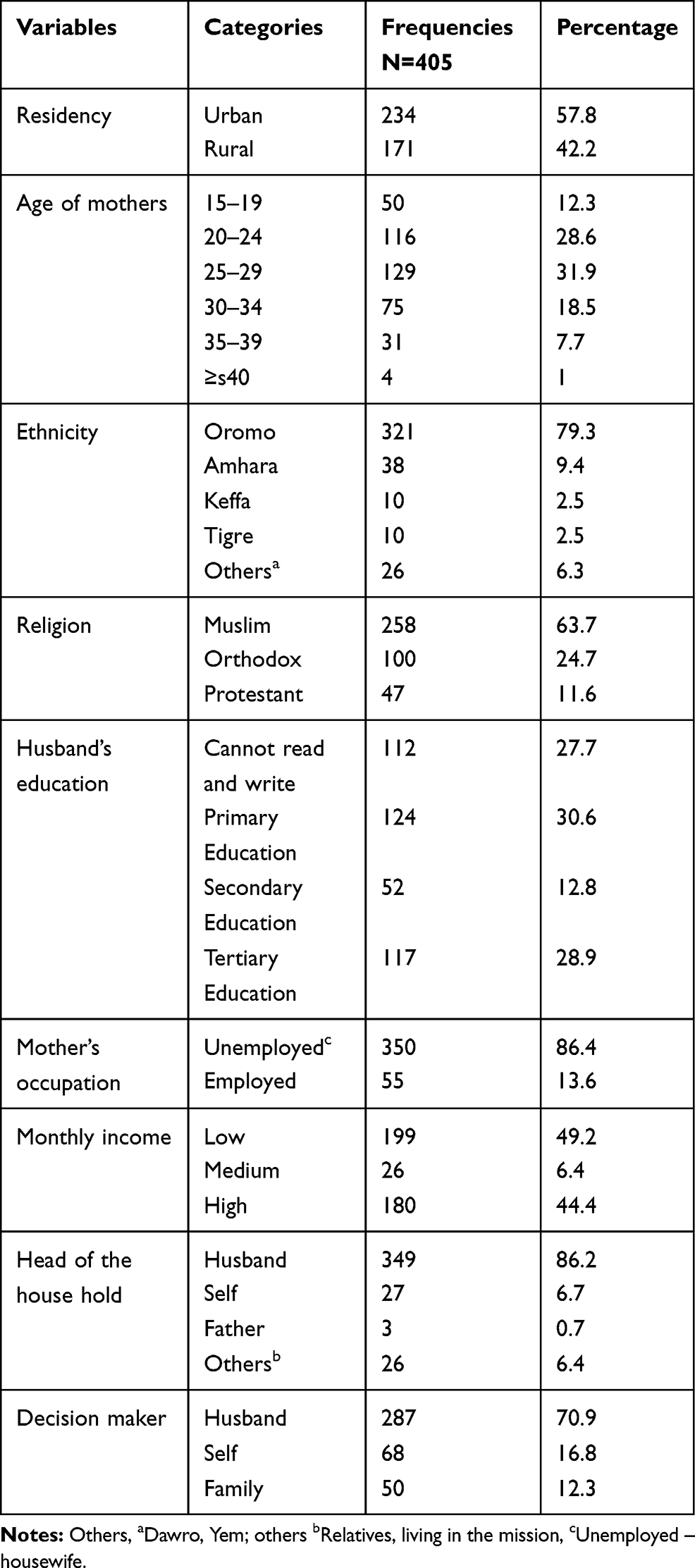 |
Table 1 Sociodemographic Characteristics of Respondents at JMC, Ethiopia, 2019, (N=405) |
Prevalence of Delay in Seeking Institutional Delivery Service Utilization
The prevalence of delay in seeking institutional delivery service utilization among mothers attending JMC was 189 (46.7%) (Figure 1).
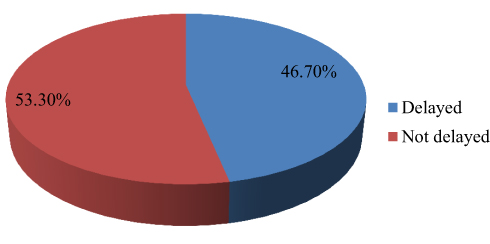 |
Figure 1 Prevalence of delay in seeking institutional delivery utilization at JMC, (n=405), 2019. |
Participants who were delayed to seek care in institutional delivery utilization were asked the reason for time not seeking care. The major reasons reported for the maternal delay in seeking care were:- not recognizing the labor which accounts for 97 (51.3%), a good outcome of previous labor 30 (16.1%), and lack of money 29 (15.1%) (Figure 2).
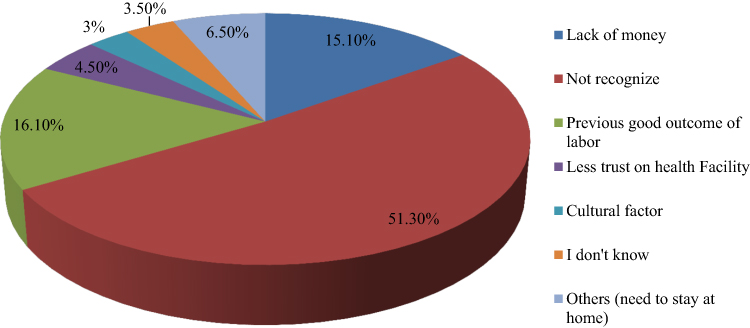 |
Figure 2 Reasons of respondents for the delay in seeking care at JMC, (n=189), 2019. |
Obstetric Characteristics of Mothers
Of 405 mothers who were participated, 264 (65.3) were multi-para. Of all respondents 355 (87.4%) had ANC follow up and the majority 260 (56.8%) of mothers made ANC follow-up at the health center (Table 2).
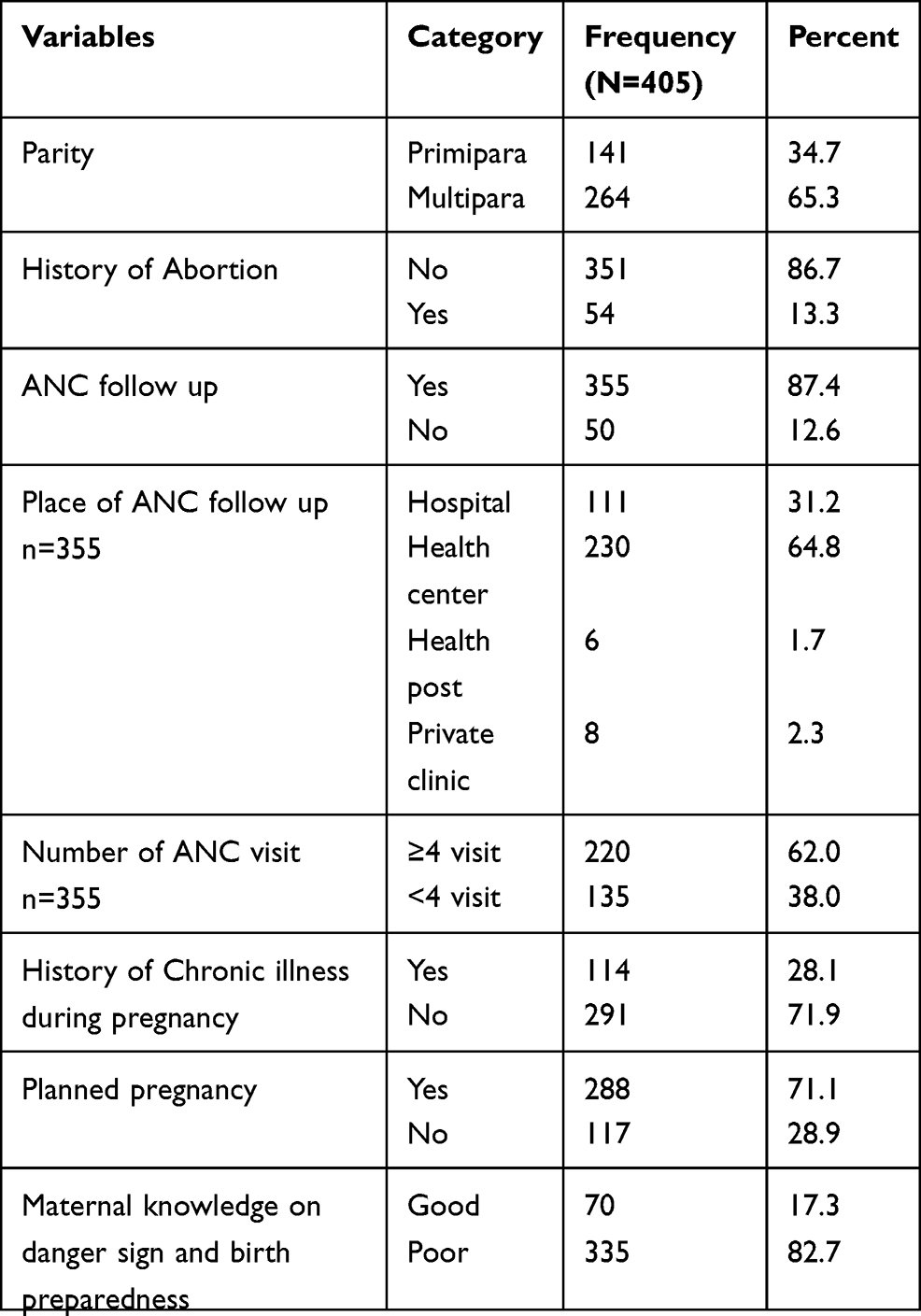 |
Table 2 Obstetric Characteristics of Respondents at JMC, 2019 |
Factors Associated with a Delay in Seeking Care for Institutional Delivery Service Utilization Among Mothers at JMC
Binary logistic regression was done accordingly and Multivariable logistic regression analysis adjusted for potential confounders. Those variables with a p-value ≤of 0.25 were taken to multivariable logistic regression, Residence, education of mother, education of husband, occupation of mother, occupation of husband, monthly income, decision-maker, parity, ANC, labor start time, chronic illness during pregnancy, the status of pregnancy plan, distance, knowledge of mothers on danger sign and birth preparedness, were variables candidate for multivariable logistic regression analysis. Multivariable logistic regression was done after identifying those candidate variables with a P-value ≤ of 0.25. The results are shown in Table 3.
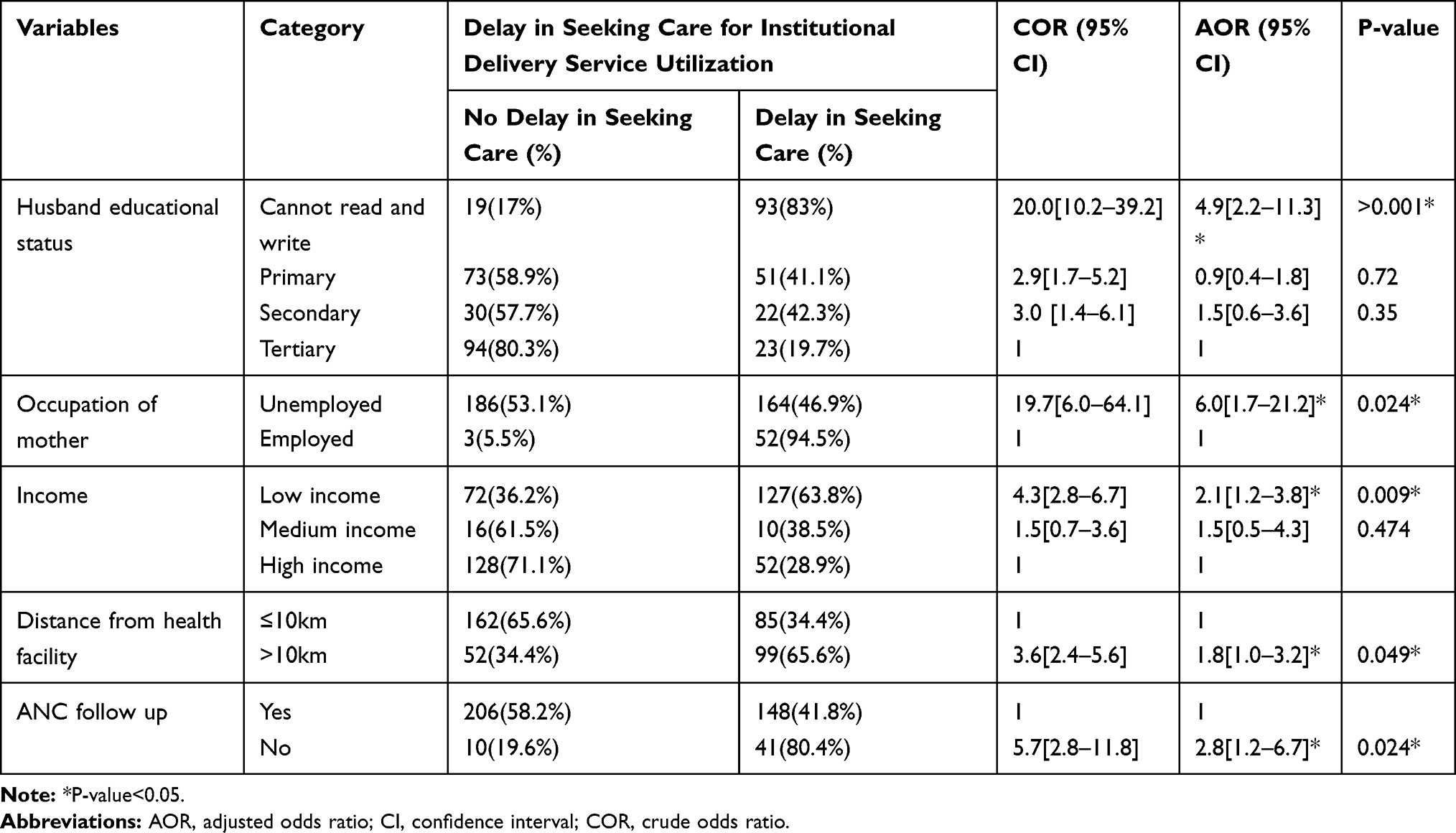 |
Table 3 Factors Associated with a Delay in Seeking Institutional Delivery Service Utilization Among Mothers at JMC, Southwest Ethiopia, 2019 |
Delay in seeking institutional delivery service utilization among whose husband’s cannot read and write was about 5 times higher than those mothers whose husbands education status is in tertiary level (AOR= 4.9; 95% CI=2.1–11.3). Unemployed mothers have been delayed about 6 times than employed ones (AOR= 6.0; 95% CI=1.7–21.2). Mothers with low household income were about 2 times more likely to delay in seeking care than those mothers with high household income (AOR=2.1; 95% CI=1.2–3.8). Mothers who live with a distance from a health facility >10 KM were about 2 times delayed to seek care than those mothers who live ≤ at 10KM from a health facility (AOR=1.8; 95% CI= 1.0–3.2). Mothers with no ANC follow-up were about 3 times more likely to delay in seeking care than those mothers who have ANC follow-up (AOR =2.8; 95% CI =1.1–6.7).
Discussion
This facility-based cross-sectional study aimed to assess factors associated with a delay in seeking institutional delivery service utilization at Jimma medical center, Ethiopia. Besides, the study tried to indicate the prevalence of delay in seeking care for utilization of institutional delivery. Our study identified maternal delay to seek care was linked with socio-economic factors, accessibility of health facility, and obstetric related factors. This study revealed that the prevalence of delay in seeking institutional delivery service utilization was 46.7%. The finding was higher than the study conducted in Bahir Dar, Northern Ethiopia which was 37.8%.16 Nevertheless, this finding was less than the study conducted in Pakistan, which was 71%.15 The possible reason for the discrepancy might be due to the geographical location difference, sample size variation since the study was conducted in the majority of an urban area of this study participants were living in urban. Whereas the majority of study participants in Pakistan were live in rural area mothers who live in a rural area have poor access to institutional delivery service utilization.15
This study shows that delay in seeking institutional delivery service utilization was higher among mothers whose husbands cannot read and write. The study conducted in Pakistan also suggested that education, gender discrimination, economic and cultural beliefs have a great impact on timely seeking care and utilization of health care system.17 Similar study conducted in Hadiya show that as the maternal delay was high among mothers whose husbands are low in their educational status.14 This implies that, husbands who cannot read and write may have poor awareness in delivery care importance; thus affect maternal delivery service utilization.
Mothers who live with a distance of greater than ten kilometers far away from health facilities have been delayed more than mothers who live with a distance less than or equal to ten kilometers from a health facility. The distance was not the major predictor to delay in seeking care in the study conducted in Bahirdar city, Amhara region. However, this finding was consistent with the study done in rural India mentioned that distance is one of the major barriers for maternal delivery service utilization as women living farther away from the health facilities are less likely to give birth at a health facility.18 The reason behind this might be women who traveled the shortest distance had a high chance of attending and coming early to utilize delivery whereas women who were traveling long distances had less chance to seek treatment as early as possible.
Unemployed mothers were more likely to delay than employed mothers the reason behind this could be, employer mothers can generate income and they are more autonomous subsequently unemployed mothers will be dependent on husbands, therefore, it affects timely seeking delivery care of mothers. Not having ANC follow-up was found a significant contributor to the delay in seeking care. The possible reason might be due to mothers who attend ANC get information about delivery complications and birth preparedness during their follow-up so that they seek care as soon as possible. The major reason that mothers claimed for the delay in seeking care was lack of recognizing the labor and the current practices could not able to provide them with enough counseling information on where to deliver when to return to the facility for the service utilization, and overall on the birth preparedness and complication readiness plan due to different facility problems. This finding was consistent with comprehensive emergency care access in Ethiopia as mentioned that lack of recognition was the predictor for the delay in seeking care.19
Limitations
Since the data were collected through an interviewer-administered questionnaire it might be prone to social desirability bias. Furthermore, this study uses a cross-sectional design which failed to distinction cause and effect relationships. Further research should be conducted at a community level to understand factors that hinder maternal health care seeking behavior, increase its representativeness, strengthen as well- as widen our results in different countries.
Conclusion
The study identified as the prevalence of delay in seeking institutional delivery service utilization was high in JMC. Husband’s educational status, Occupation of the mother, Income, distance from the health facility, ANC follow-ups were found significantly to influence delay in seeking care for institutional delivery service utilization. This finding may contribute more to enhance the practice and quality of ANC services being delivered for pregnant mothers. Thus, efforts should be made to expand health facilities with delivery services and initiate mothers to have ANC follow-up. Need to promote adult education as husband’s educational status was one of the predictors. Empowerment of women to increase women employment through integrated activities including girl’s education is vital.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; COR, Crude Odds Ratio; EDHS, Ethiopian Demographic health survey; OR, Odds Ratio; KM, Kilometer; SPSS, Statistical Package for Social Sciences.
Data Sharing Statement
All the data analyzed in this article are available from the corresponding author and can be obtained upon reasonable request.
Acknowledgments
We would like to thank Jimma University, we are also grateful to Jimma medical center, respective data collectors, and study participants for their valuable contribution to the realization of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Jimma University supported this research financially. The university had no role in the design of the study, collection, analysis, and interpretation of the data, or in writing the manuscript.
Disclosure
The authors declared that they have no conflicts of interest for this work.
References
1. Wellington A. Maternal mortality literature review risk management. 2017:1-6. doi:10.13140/RG.2.2.13930.214
2. Lindtj B, Mitiku D, Zidda Z, Yaya Y. Reducing maternal deaths in Ethiopia: results of an intervention programme in Southwest Ethiopia. Plos One. 2017;72(Mmr220):1–18.
3. The World Bank. Indicators; 2021. Available from: http://data.worldbank.org/indicator.
4. World Health Organization. Maintenance break; 2021. Available from:
https://www.who.int/docstore/world-health-day/en/pages1998/whd98_05.html.
5. Goodman DM, Srofenyoh EK, Ramaswamy R, et al. Addressing the third delay: implementing a novel obstetric triage system in Ghana. BMJ Glob Heal. 2018;3(2):1–8.
6. United Nations. Reproductive Health Policies 2017. Available from: https://www.un.org/en/development/desa/population/publications/pdf/policy/reproductive_health_policies_2017_data_booklet.pdf
7. Nyflot L, Sutras V. Strategies to reduce global maternal mortality. Acta Obstetricia et Gynecologica Scandinavica. 2018;97(6):639–640. doi:10.1111/aogs.13356
8. Muchiri WF, Muturi KS, Kariuki NJ, Orare OD, Mwagandi CL, Kyalo MJ. Operation assessment on ambulance services: a case study of Machakos County, Kenya. Int J Trop Dis Heal. 2018;33(1):1–12. doi:10.9734/IJTDH/2018/41879
9. Geleto A, Chojenta C, Mussa A, Loxton D. Barriers to access and utilization of emergency obstetric care at health facilities in sub-Saharan Africa-a systematic review protocol. Syst Rev. 2018;7:Article 60. doi:10.1186/s13643-017-0635-z
10. Thaddeus S, Maine D. Too far to walk maternal mortality in context screen. Soc Sci Med. 1994;38(8):1091–1110. doi:10.1016/0277-9536(94)90226-7
11. Chavane LA, Bailey P, Loquiha O, Dgedge M, Aerts M, Temmerman M. Maternal death and delays in accessing emergency obstetric care in Mozambique. BMC Pregnancy Childbirth. 2018;18(1):1–8. doi:10.1186/s12884-018-1699-z
12. Adegoke A, Utz B, Msuya SE, van den Broek N, van den Broek N. Skilled birth attendants: who is who? A descriptive study of definitions and roles from nine Sub Saharan African countries. PLoS One. 2012;7(7):1–11. doi:10.1371/journal.pone.0040220
13. Hunt P, Mesquita JBDE. Reducing Maternal Mortality the Contribution of the Right to the Highest Attainable Standard of Health. New York, NY: United Nations Popul Fund; 2015:1–16.
14. Lire A, BeyamoMekiso A, Tadele D, Facha W. Delays for utilizing institutional delivery and associated factors among mothers attending public health facility in Hadiya Zone, Southern Ethiopia. Science Journal of Public Health. 2017;5(6):149-157. doi:10.11648/j.sjph.20170506.13
15. Shah N, Hossain N, Shoaib R, Hussain A, Gillani R, Khan NH. Socio-demographic characteristics and the three delays of maternal mortality. J Coll Physicians Surg Pak. 2009;19(2):95–98.
16. Awoke W, Seleshi K. Maternal delays in utilizing institutional delivery services, Bahir Dar, Ethiopia. Health (Irvine Calif). 2013;5(6):1026–1031. doi:10.4236/health.2013.56137
17. Shaikh BT, Hatcher J. Health seeking behavior and health service utilization in Pakistan: challenging the policymakers. J Public Health (Oxford, England). 2005;27(1):49–54. doi:10.1093/pubmed/fdh207
18. Kumar S, Dansereau EA, Murray CJL, Kumar S, Dansereau EA, Does CJLM. Does distance matter for institutional delivery in rural India? Does distance matter for institutional delivery in rural India? Appl Econ. 2014;46(33):4091–4103. doi:10.1080/00036846.2014.950836
19. Federal Democratic Republic Of Ethiopia. Ethiopia: Demographic and Health Survey; 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf.1–551.
20. JHPIEGO. Monitoring birth preparedness and complication readiness. Tools and Indicators for Maternal and Newborn Health: Baltimore,; 2021.
Available from: http://reprolineplus.org/system/files/resources/bpcr_monitoringtools.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.