Back to Journals » International Medical Case Reports Journal » Volume 18
Deep Brain Stimulation Peri Lead Cyst Resolution with Nonoperative Management: Case Report and Review of the Literature
Authors Narayanan SN ![]() , Bick SK
, Bick SK
Received 17 June 2025
Accepted for publication 23 October 2025
Published 7 November 2025 Volume 2025:18 Pages 1429—1438
DOI https://doi.org/10.2147/IMCRJ.S547667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Sujanya N Narayanan,1 Sarah K Bick2
1Vanderbilt University School of Medicine, Nashville, TN, USA; 2Department of Neurological Surgery, Vanderbilt University Medical Center, Nashville, TN, USA
Correspondence: Sarah K Bick, Email [email protected]
Abstract: Deep brain stimulation (DBS) is an effective treatment for medically refractory essential tremor (ET) and Parkinson’s disease. We present the case of a patient treated with thalamic DBS for ET who developed a large right peri-lead cyst with associated edema three months postoperatively, causing symptoms of dysarthria and left-sided weakness. The patient was treated nonoperatively with a course of steroids and serial observation. Over three months, the cyst regressed in size, with resolution of the associated symptoms. The patient was ultimately able to continue bilateral DBS for ET, which provided relief from upper-extremity tremor. By 9 months after the cyst was diagnosed (one year postoperatively from DBS) he was fully recovered back to baseline. We review other cases of peri-lead cysts and edema, of which etiology and presentation remain varied and unclear. Peri-lead cysts are a rare complication of DBS with an estimated incidence of 0.8%. Ultimately, this case shows that appropriately selected peri-lead cysts may be managed nonoperatively, allowing for continued DBS benefit in patients by avoiding lead removal.
Keywords: deep brain stimulation, peri lead cyst, peri lead edema, neurosurgery, post operative complication
Introduction
DBS is an FDA-approved treatment for multiple neurologic disorders, including Parkinson’s disease (PD), essential tremor (ET), dystonia, epilepsy, and obsessive-compulsive disorder (OCD).1 DBS of the thalamic ventral intermediate nucleus (VIM) reduces neuronal firing and improves tremor and quality of life for patients with ET and tremor-dominant PD.2,3 VIM DBS is the standard of care surgical treatment for patients with medically refractory ET.4,5
While DBS is generally well tolerated, it can be associated with complications including intracranial hemorrhage, infection, and stimulation-related side effects. Peri-lead cyst, consisting of a fluid collection around a DBS lead, is a rare complication with an estimated incidence of 0.8%.6 Peri-lead edema, or cerebral edema forming around a DBS lead, is more common. A review of MRIs obtained one day after DBS electrode placement found 22% of patients to have peri-lead edema.7 In another study where MRI was obtained seven days postoperatively, 40% of patients had peri-lead edema but none had neurologic worsening.8 Similar incidence was reported in a third analysis, where symptomatic peri-lead edema had an incidence of 3.1% (8.7% of all peri-lead edema), and asymptomatic peri-lead edema had an incidence of 35.8%.9 Other surgery-related complications include intracerebral hemorrhage (1–8%), wound infection (3–10%), and postoperative seizures (3.1%).10–13 Complications can also occur related to the stimulation itself. In ET, these can include dysarthria (8–75%) and worsening of gait/ataxia (25–37%), both of which can be managed and reduced by adjustment of DBS settings postoperatively.13
Peri-lead edema has recently been appreciated to be a relatively common complication that may present immediately after DBS or with delayed onset. One review found that symptomatic peri-lead edema occurs in 3.1% of patients, and asymptomatic peri-lead edema occurs in 35.8% of patients.9 Peri-lead edema can be self-limiting but has been observed in some cases to develop into or occur with a peri-lead cyst. Peri-lead cysts, while sometimes associated with peri-lead edema, are much rarer, occurring in fewer than 1% of cases.6 Likely due to the rarity of peri-lead cysts, there is limited literature on their management and no standardized recommendations for follow up imaging or management. It is therefore useful to examine different management strategies to move towards more standardized recommendations to guide treatment. We describe a case of a patient presenting with a delayed large peri-lead cyst after initial successful implantation of DBS for ET.
Case Presentation
A 69-year-old right-handed man presented for evaluation and treatment of essential tremor (ET) diagnosed at age 48. He had a past medical history notable for hypertension. At the time of evaluation, he had a bilateral postural and action tremor that was greater in the right upper extremity and a no-no predominant head tremor. The patient reported that his tremor impeded his ability to eat, write, and work with tools. Fahn Tolosa Marin (FTM) score was 41 total, 14 on the right, and 13 on the left. His medical management at the time consisted of primidone 50 mg twice daily, propranolol extended release 80 mg once daily, gabapentin 400 mg three times daily, and methazolamide 50 mg twice daily. However, his tremor remained inadequately controlled and his medications had side effects of fatigue and negative cognitive effects. Tapering any individual medication resulted in greater tremor severity. Previously tried and failed medications included topiramate, levetiracetam, and zonisamide. His head tremor was addressed in the past with botulinum toxin injection which provided some relief. Due to the refractory nature of the patient’s upper extremity tremor, he sought out advanced therapy for ET symptom control. After screening by a movement disorders neurologist, neuropsychologist, and neurosurgeon, along with multidisciplinary discussion at our advanced movement disorder therapies conference, he was determined to be a candidate for bilateral VIM DBS.
We take a three-stage approach to DBS surgery using a frameless system (STarFix, FHC), with each procedure occurring 1–2 weeks apart. In Stage I, bone fiducials were implanted under general anesthesia and computed tomography (CT) and magnetic resonance imaging (MRI) of the brain were completed with no complications. Subsequently, the surgeon planned the DBS electrode trajectories using T1 post contrast MRI sequence and the frameless stereotactic platform was created using this plan. In Stage II, bilateral directional leads were placed into VIM with the patient awake with intraoperative microelectrode recordings and stimulation testing. On the left, five passes were performed before final electrode implantation (Vercise, Boston Scientific, Marlborough, MA, USA), while on the right three passes were performed. Post-operative CT was obtained, which showed mild bifrontal pneumocephalus (Figure 1A–C). In Stage III, the implantable pulse generator (IPG) was placed subcutaneously in the left chest inferior to the clavicle, while the patient was under general anesthesia and connected to extension wires, which were connected to the DBS electrodes. One month later, the device was turned on and programmed by the patient’s neurologist, with resulting excellent tremor control bilaterally. On the left settings were case positive, level 2 negative (3 80% 2 10% 4 10%), 1.5 milliamps, pulse width 60 microseconds, and frequency 130 Hertz. On the right, settings were case positive, level 2 negative, 2.1 milliamps, pulse width 60 microseconds, and frequency 130 Hertz. Primidone and gabapentin were tapered, and switching from propranolol to a different blood pressure medication was discussed at this appointment.
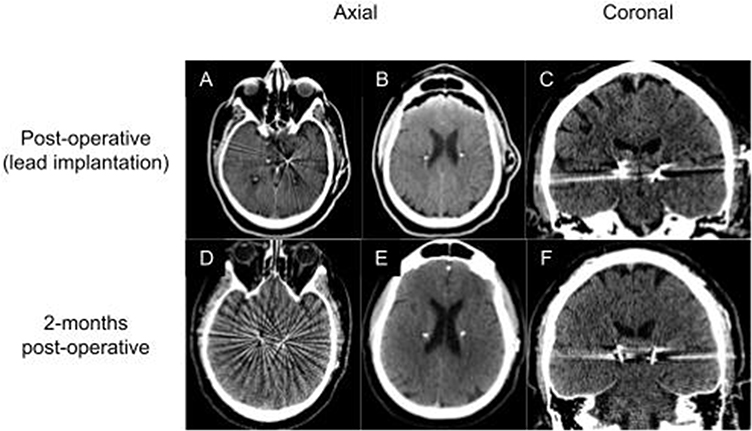 |
Figure 1 CT imaging at different time points after DBS surgery. (A, B, D, E) Axial CT showing DBS hardware with B showing mild bifrontal pneumocephalus resolved on (E, C, F) Coronal CT showing DBS hardware. |
At his scheduled two-month follow-up with his neurologist, the patient reported episodes of acute onset severe vertigo and associated nausea that began 9 days prior. On exam, the patient had mildly dysarthric speech, decreased temperature sensation in his right face and left body, subtle left sided weakness, and left upper extremity ataxia. Symptoms did not change with DBS stimulation turned off. Head CT was obtained that day and was unremarkable (Figure 1D–F). Subsequently, labs, chest x-ray, and CT angiography of the head and neck were negative. Epley maneuvers did not provide relief from vertigo, however, meclizine did. Outpatient MRI was planned, and the patient was started on aspirin 81 mg daily for concern for potential stroke. MRI was performed at an outside facility approximately one month later and demonstrated a fluid-intensity cyst of 2.2 cm in the greatest measured axial dimension around the right DBS electrode tip, with associated edema, but with no diffusion restriction or postcontrast enhancement (Figure 2A and B). The patient was recommended to follow up at our facility. Two weeks after identification of the cyst and edema on MRI, the patient presented to our emergency department with worsening symptoms of left-sided weakness and dysarthria. Incidentally, the patient had completed a seven-day course of prednisone for bronchitis prior to presentation to the emergency room with some improvement in symptoms, although neurologic symptoms began to worsen again on completion. On presentation, the right DBS electrode was turned off without return of tremor, and repeat MRI was planned. As the patient did not have a fever or laboratory tests concerning for infection and had well-healed incisions without appearance suggestive of infection, the patient was admitted and non-surgical treatment was initiated. Dexamethasone taper was started to address cerebral edema, sequentially consisting of 4 mg taken on the first night, 4 mg twice daily for 3 days, 2 mg twice daily for 3 days, 1 mg twice daily for 3 days, and 1 mg daily for 3 days. On the second day of admission, MRI was performed and showed a mild interval decrease in size of the peri-lead cyst from the outpatient MRI to 1.9 cm with near-complete resolution of edema with no contrast enhancement and unchanged electrode position (Figure 2C and D). The patient also reported improvement in symptoms, with left lower extremity motor strength improving from 4+/5 to 5/5 and left upper extremity motor strength improving from 4/5 to 4+/5. Given radiologic and clinical improvement continued nonoperative management was planned with close outpatient follow up. At one week follow-up from admission, while the patient was still on dexamethasone taper, he had no dysarthria and showed increased left-sided strength, with left upper extremity strength motor score of 4+/5 proximally and 5/5 distally. Left lower extremity motor score remained at 5/5. MRI obtained one month later showed continued decrease in the size of the cyst, now measuring 1.4 cm in maximum diameter, and complete resolution of edema (Figure 2E and F). Right DBS remained off without recurrence of tremor. Three months later (5.5 months after the cyst was initially imaged and 8.5 months post-operatively), repeat MRI showed further decrease in size of the peri-lead cyst, now measuring 0.7 cm in maximum diameter, and the patient reported substantial improvement in symptoms (Figure 2G and H). At six months postoperatively, left side tremor returned and the patient turned his right side DBS back on. By one year after surgery (9 months after cyst diagnosis), his strength and speech had returned to baseline. At the most recent follow up 2 years after surgery, he continued to experience excellent tremor control with DBS.
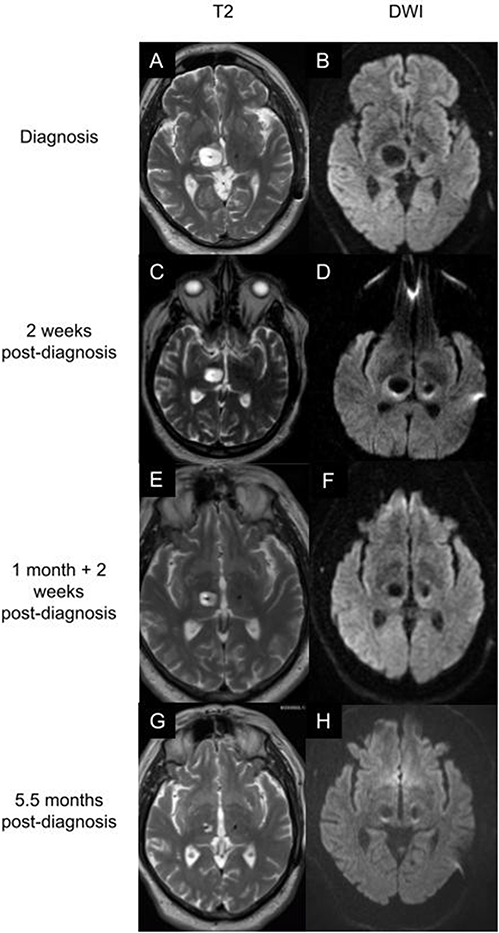 |
Figure 2 MRI imaging of cyst at different time points after diagnosis 3 months after DBS surgery. (A,C,E,G) T2 weighted MRI showing cyst at different time points. (B,D,F,H) diffusion weighted MRI at these same time points. Imaging was performed at diagnosis 3 months after surgery (A and B), 2 weeks after diagnosis (C and D), 1.5 months after diagnosis (E and F), and 5.5 months after diagnosis (G and H) showing gradual improvement over time. |
Discussion
We present the case of a patient who developed a delayed large peri-lead cyst after undergoing VIM DBS for ET, which ultimately resolved with nonoperative management.
Peri-lead cyst is a rare complication of DBS, with one study reporting 0.8% incidence.6 While peri-lead cysts are often accompanied by peri-lead edema, they have also been observed in isolation.6,14 Peri-lead edema is a more common complication following DBS than peri-lead cyst. Reported prevalence rates for peri lead edema vary widely from 0.9% to 100%, likely due to differences in post operative imaging protocols, varying symptoms caused by edema, and whether asymptomatic or only symptomatic edema is considered.6,7,14 The lack of standardized postoperative imaging protocols for DBS surgery is likely due in part to the relatively low complication rates after the procedure.10,11,15 An institutional best surgical practices protocol suggested that MRI be obtained on the same day as electrode implantation and before discharge to screen for acute complications such as ICH.16 However, postoperative CT is also widely used due to accessibility and shorter acquisition time, and is the approach taken at our center.17 While immediate postoperative imaging is relatively standard, follow up imaging protocols are more variable and often utilized only if there is onset of new symptoms.18 We routinely obtain one month follow up head CT to evaluate final lead position after brain shift has resolved. In this patient, MRI was obtained when he presented with weakness and dysarthria 3 months postoperatively and demonstrated large peri-lead cyst. As there are no standardized imaging protocols to monitor peri-lead cysts and the patient was improving at the time of diagnosis, we chose to obtain follow up imaging 1 month after discharge, selecting this as a relatively short interval but still potentially long enough to see change in cyst size. As the cyst was substantially improved at this one month follow up MRI, the next imaging was scheduled for 4 months later. Given the absence of protocols for imaging and management of peri-lead cysts, we present our experience and synthesize existing literature on this rare complication to help guide clinical decision making in the future.
Peri-lead cysts are a rare, delayed complication of DBS. One proposed etiology is that peri-lead cysts may be a rare end result of peri-lead edema.6,9 Due to the absence of standardized imaging guidelines for DBS follow-up, it is difficult to fully characterize the relationship between peri-lead edema and cyst formation. Several authors have suggested that cysts may occur as a part of the natural course of untreated or persistent peri-lead edema, and both share a proposed etiology of cerebrospinal fluid (CSF) tracking.6,9,19–21 With CSF tracking, fluid may accumulate from the subarachnoid space along the lead due to electrode puncture or disruption of ependymal integrity.20,22,23 Other proposed etiologies for peri lead cysts include infection, microhemorrhage, venous infarct, and inflammatory reaction to DBS hardware.20 DBS devices and material seem to be well-tolerated in the long-term at the tissue level, with limited immune reaction around electrodes in a post-mortem analysis of tissue from a patient treated with DBS for 12 years, although multinucleated giant cells and lymphocytic infiltration were observed due to low-grade inflammation.24 As our patient did not have fever or other symptoms and MRI was reassuring, we felt that infection was unlikely and elected to nonoperatively manage. Edema was limited to the right lead tip, making an allergic response less likely due to the unilateral nature.7 Postoperative CT was normal, so microhemorrhage and venous infarct were also less likely to be the cause of his edema.
Peri-lead cysts can cause a variety of symptoms including neurologic deficit and loss of therapeutic effect. In some cases, peri-lead cysts may be asymptomatic.25 Cysts may produce mass effect, leading to motor symptoms such as imbalance and weakness contralateral to the affected lead.14 For our patient, a right peri-lead cyst resulted in left sided motor symptoms due to mass effect and edema. One case reported that peri-lead cyst led to loss of DBS therapeutic effect and intracranial hypertension.26 The loss of DBS therapeutic effect may be attributed to lower electrode impedance, as cystic fluid conductivity is higher than parenchymal conductivity, in turn lowering local field potential.22 Peri-lead cysts may present acutely or with delayed onset. Peri-lead cysts have been reported as soon as 6 hours or 1 day postoperatively.23,27 Conversely, peri-lead cyst has also been diagnosed as long as 59 months postoperatively, with retrospective MRI analysis showing peri-lead edema without cyst at six and 12 months.6
Treatment of peri-lead cyst varies depending on acuity and severity of patient symptoms on presentation. We performed a literature review and identified 22 previously reported cases of peri-lead cysts and their management (Table 1). Patients underwent DBS surgery for PD (n = 10), ET (n = 4), Tourette’s Syndrome (n = 1), dystonia (n = 1), mixed type tremor (n = 1), major depressive disorder/anorexia nervosa (n = 1), and unspecified conditions (n = 3). Bilateral leads were placed in 16 cases and unilateral leads were placed in 2 cases, while the rest were unspecified. Cysts were unilateral in all but one case. Out of these 22 cases, 9 cases explicitly mentioned concurrent or previous peri lead edema. Leads were removed in 10 cases, cysts were stereotactically aspirated in 4 cases, steroid therapy was initiated in 5 cases, and patients were followed with observation only in 5 cases. Across cases, symptoms, presentation, and management varied.
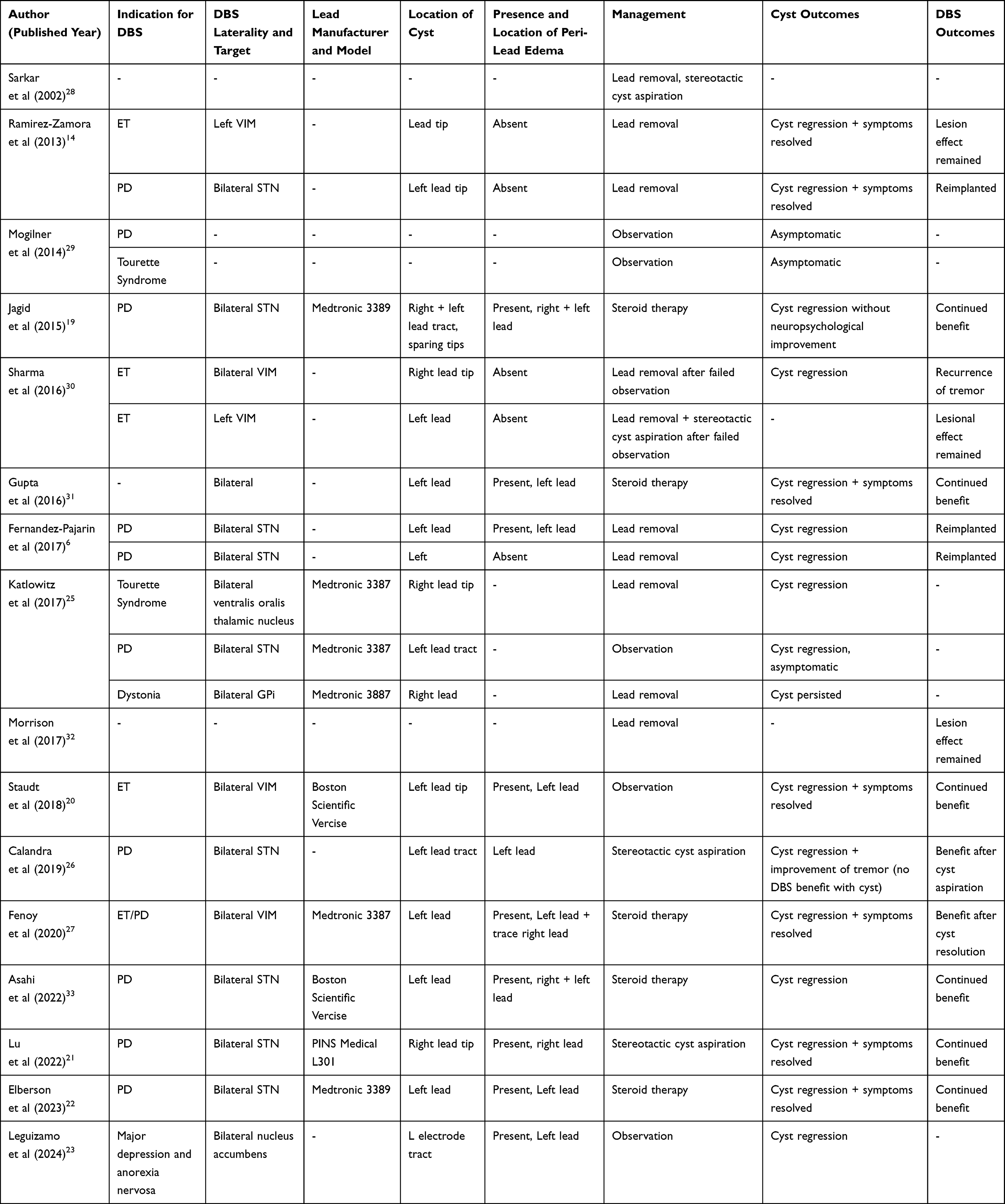 |
Table 1 Reported Cases of Peri-Lead Cyst Post-DBS Surgery |
Lead removal can directly address cyst mass effect and may be indicated in cases where patients are symptomatic.6,14,25,30 Ten of the published cases identified in our literature review were treated with lead removal.6,14,25,28,30,32 This treatment option is often chosen in cases of significant symptoms or concern for infection. For example, in one case lead removal was performed emergently due to acute hydrocephalus.25 Lead removal has also been performed in several cases after peri-lead cyst and associated symptoms worsened after initial nonoperative management and observation.25,30 Overall with lead removal, in 6 cases cysts regressed, in 1 case the cyst persisted, and in 3 cases cyst outcomes were not available.6,14,25,28,30,32 One downside of lead removal is that it can lead to loss of DBS therapeutic effect. However, in some cases, peri-lead cyst may cause a lesion like effect that can provide symptomatic benefit. In one patient who underwent unilateral VIM DBS for ET, lead removal was performed due to cyst formation and associated imbalance, dizziness, numbness, and weakness. Following removal, a lesion effect remained providing tremor relief for several months.14 For our patient, right DBS was initially turned off when cyst was diagnosed, and for four months, the patient did not experience left-sided tremor. As such, turning off DBS as edema and cysts resolve may not be detrimental in the short-term due to residual lesion effects.
Another approach that has been described to treat symptomatic peri-lead cyst is stereotactic cyst aspiration, with or without concurrent lead removal. Stereotactic cyst aspiration without lead removal can provide immediate significant reduction in size of the cystic lesion.21,26 In one case of a 44-year-old man with PD, when DBS failed to have effect at 4 months postoperatively, MRI showed a peri-lead cyst. Although the cyst was asymptomatic, due to radiologic signs of intracranial hypertension the cyst was aspirated without lead removal, and one month later, DBS was turned back on with good control of tremor.26 In another case, a 60-year-old woman with PD was found to have peri-lead edema on MRI 2 months post-operatively when the patient presented with right-sided hypertonia and static tremor. After failing a course of steroids and antibiotics, repeat imaging showed progression to peri-lead cyst, and the decision was made to aspirate the cyst while preserving the lead, after which tremor was well-controlled with DBS.21 These cases demonstrate that in some patients with symptomatic peri-lead cyst without concern for infection, stereotactic cyst aspiration can lead to improvement in symptoms while allowing patients to continue to receive DBS therapy to treat symptoms of their movement disorder.
Several cases have been managed nonoperatively with or without steroid treatment and with follow up to monitor symptoms and cyst radiographic appearance.19,20,22,23,25,27,29,31,33 In some cases, steroids may help treat edema and aid cyst involution, while still preserving DBS therapeutic effects. In one case of a 71-year-old man with PD treated with DBS who experienced postoperative neurocognitive decline, bilateral peri-lead edema was seen on CT 4 months postoperatively, and 5 months later, MRI demonstrated progression to bilateral cysts and edema for which the patient was treated with a course of steroids. Nine months later, peri-lead edema and cysts were radiographically improved and the patient continued to experience motor benefit from DBS.19 In another case, a 66-year-old woman treated with DBS for ED and PT developed aphasia and hemi-neglect 2 days postoperatively, with CT demonstrating peri-lead edema and cyst and dexamethasone was initiated. Edema initially worsened on repeat CT, but by 3 months post-operatively peri-lead cyst and edema had resolved and the IPG was implanted.27 As demonstrated by these cases, steroid effects on cyst size vary and may take longer and require additional adjustment of DBS settings for effective symptom control.19,22,27,31,33 Steroids may be particularly important when peri-lead edema is noted to predate or co-exist with peri-lead cyst. For our patient, symptoms and radiographic appearance both significantly improved with steroid administration for an unrelated issue (bronchitis) at the time of cyst diagnosis. Given the significant observed improvement and absence of infectious signs, we felt it was reasonable to continue steroid regimen with dexamethasone taper as first-line treatment rather than subjecting the patient to the risk of an additional surgical procedure such as cyst aspiration or lead removal and allowing him to maintain his DBS hardware for future therapeutic use. As medical management was attempted rather than definitive surgical treatment, close follow-up was coordinated to verify continued improvement. In the case that symptoms worsened or if the cyst grew larger in size, then cyst aspiration or even lead removal may have been considered. However, after steroid treatment and with time the cyst showed interval decrease with resolution of symptoms, so further intervention was not indicated.
Peri-lead cysts may spontaneously resolve with observation alone and no steroid treatment.19,26,28 A 72-year-old male treated with DBS for ET presented with dysarthria and imbalance three months postoperatively and was found to have left peri-electrode edema and cyst. With clinical observation alone, it was found to have completely resolved at 17 months along with associated symptoms.20 However, observation alone is not successful in all cases. In one case, a cyst was noted 6 weeks post-operatively on MRI when the patient presented with new-onset dysarthria and ataxia. Repeat imaging 2 weeks later demonstrated that the cyst had grown, and the lead was removed. At follow up 6 months later the cyst had regressed but left hand tremor returned.30 In another case, a cyst was diagnosed on MRI 10 months post-operatively when the patient presented with dysarthria and hemiparesis. After 3 months, symptoms progressed and MRI demonstrated the cyst had grown in size, so the lead was removed and the cyst was aspirated.30 These cases demonstrate that while nonoperative management is a reasonable option to initially consider for peri-lead cyst in patients with initially mild or improving symptoms, close follow up is warranted to ensure that symptoms do not worsen and require additional treatment.
Several limitations exist for this case report and literature review. In our case and others managed non-operatively no biopsy was performed, so we do not have histological confirmation of diagnosis and absence of infection. However, improvement of symptoms and radiographic appearance with time and without surgery suggest that no infection was present. There are no standardized follow up imaging protocols for DBS cases or complications such as peri-lead cysts, which likely contributes to the variance in reported incidence rates and outcomes. As peri-lead edema and cyst may both present asymptomatically, there exists a potential underreporting bias of undetected or incidental cases. However, as symptoms may be severe in some circumstances, it is prudent to consider the utility of different management strategies.
Overall, intervention decisions should be made based on patient symptoms and presentation and after discussion of risks and benefits of different approaches. In symptomatic patients with severe presentation or worsening symptoms, cyst aspiration or lead removal are indicated. In patients with asymptomatic or improving symptoms, observation with or without a steroid course is a reasonable management choice.
Conclusion
We present a case of a patient with ET who developed peri-lead cyst and associated peri-lead edema observed two months postoperatively from DBS surgery and review the published literature of this rare complication of DBS. Treatment of peri-lead cyst currently lacks standardized guidelines but may include medical management or surgical intervention to address neurologic deficit or loss of DBS therapeutic effect. Our report has several important implications for clinical practice. In cases of new, unexplained neurologic symptoms after DBS, obtaining early neuroimaging can be important for identifying complications such as peri-lead cyst or edema, allowing for early intervention and monitoring. Our case suggests that in selected patients, namely those without symptoms or with improving symptoms and without infectious signs and symptoms, nonoperative treatment with continued monitoring can lead to resolution of peri-lead cyst and may be considered in similar situations in the future.
Abbreviations
ET, Essential tremor; GPi, globus pallidus interna; Lead, unspecified location along lead (may be tip and/or tract); Lead tip, distal lead; Lead tract, proximal lead; PD, Parkinson’s disease; STN, subthalamic nucleus; VIM, ventral intermediate nucleus of the thalamus.
Consent for Publication
All adult participants provided written informed consent to participate in this study. Written informed consent was obtained from the individual for publication of the details of their medical case and any accompanying images. Our institutional policy did not require approval or institutional review board approval to publish case details for a single patient, but patient written informed consent was obtained.
Funding
No funding was received for this research.
Disclosure
Dr Sarah Bick reports personal fees from Varian medical systems, FHC, Inc, and Spark Therapeutics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Youngerman BE, Chan AK, Mikell CB, McKhann GM, Sheth SA. A decade of emerging indications: deep brain stimulation in the United States. J Neurosurg. 2016;125(2):461–471. doi:10.3171/2015.7.JNS142599
2. Milosevic L, Kalia SK, Hodaie M, Lozano AM, Popovic MR, Hutchison WD. Physiological mechanisms of thalamic ventral intermediate nucleus stimulation for tremor suppression. Brain J Neurol. 2018;141(7):2142–2155. doi:10.1093/brain/awy139
3. Wharen RE, Okun MS, Guthrie BL, et al. Thalamic DBS with a constant-current device in essential tremor: a controlled clinical trial. Parkinsonism Relat Disord. 2017;40:18–26. doi:10.1016/j.parkreldis.2017.03.017
4. Hopfner F, Deuschl G. Managing Essential Tremor. Neurother J Am Soc Exp Neurother. 2020;17(4):1603–1621. doi:10.1007/s13311-020-00899-2
5. Zhang J, Yan R, Cui Y, Su D, Feng T. Treatment for essential tremor: a systematic review and bayesian model-based network meta-analysis of RCTs. EClinicalMedicine. 2024;77:102889. doi:10.1016/j.eclinm.2024.102889
6. Fernández-Pajarín G, Sesar A, Ares B, et al. Delayed complications of deep brain stimulation: 16-year experience in 249 patients. Acta Neurochir. 2017;159(9):1713–1719. doi:10.1007/s00701-017-3252-7
7. Succop BS, Zamora C, Roque DA, Hadar E, Kessler B, Quinsey C. Day one postoperative MRI findings following electrode placement for deep brain stimulation: analysis of a large case series. Front Neurol. 2023;14:1253241. doi:10.3389/fneur.2023.1253241
8. Saitoh T, Enatsu R, Mikami T, et al. Peri-electrode edema after deep brain stimulation. J Clin Neurosci off J Neurosurg Soc Australas. 2019;59:29–31. doi:10.1016/j.jocn.2018.11.026
9. Tian Y, Wang J, Jiang L, Feng Z, Shi X, Hao Y. The need to be alert to complications of peri-lead cerebral edema caused by deep brain stimulation implantation: a systematic literature review and meta-analysis study. CNS Neurosci Ther. 2022;28(3):332–342. doi:10.1111/cns.13802
10. Fenoy AJ, Simpson RK. Risks of common complications in deep brain stimulation surgery: management and avoidance. J Neurosurg. 2014;120(1):132–139. doi:10.3171/2013.10.JNS131225
11. Shashkin C. Complications of deep brain stimulation for movement disorders: literature review and personal experience. Acta Neurochir Suppl. 2023;130:121–126. doi:10.1007/978-3-030-12887-6_15
12. Boviatsis EJ, Stavrinou LC, Themistocleous M, Kouyialis AT, Sakas DE. Surgical and hardware complications of deep brain stimulation. A seven-year experience and review of the literature. Acta Neurochir. 2010;152(12):2053–2062. doi:10.1007/s00701-010-0749-8
13. Wong JK, Hess CW, Almeida L, et al. Deep brain stimulation in essential tremor: targets, technology, and a comprehensive review of clinical outcomes. Expert Rev Neurother. 2020;20(4):319–331. doi:10.1080/14737175.2020.1737017
14. Ramirez-Zamora A, Levine D, Sommer DB, Dalfino J, Novak P, Pilitsis JG. Intraparenchymal cyst development after deep brain stimulator placement. Stereotact Funct Neurosurg. 2013;91(5):338–341. doi:10.1159/000350021
15. Allert N, Cheeran B, Deuschl G, et al. Postoperative rehabilitation after deep brain stimulation surgery for movement disorders. Clin Neurophysiol. 2018;129(3):592–601. doi:10.1016/j.clinph.2017.12.035
16. Kramer DR, Halpern CH, Buonacore DL, et al. Best surgical practices: a stepwise approach to the University of Pennsylvania deep brain stimulation protocol. Neurosurgical Focus. 2010;29(2):E3. doi:10.3171/2010.4.FOCUS10103
17. Saleh C, Dooms G, Berthold C, Hertel F. Post-operative imaging in deep brain stimulation: a controversial issue. Neuroradiol J. 2016;29(4):244–249. doi:10.1177/1971400916639960
18. Deuschl G, Herzog J, Kleiner-Fisman G, et al. Deep brain stimulation: postoperative issues. Mov Disord. 2006;21(S14):S219–S237. doi:10.1002/mds.20957
19. Jagid J, Madhavan K, Bregy A, et al. Deep brain stimulation complicated by bilateral large cystic cavitation around the leads in a patient with Parkinson’s disease. BMJ Case Rep. 2015;2015:bcr2015211470. doi:10.1136/bcr-2015-211470
20. Staudt MD, MacDougall KW. Spontaneous regression of an intraparenchymal cyst following deep brain stimulator electrode implantation: case report and literature review. World Neurosurg. 2018;117:249–254. doi:10.1016/j.wneu.2018.06.115
21. Lu Y, Qiu C, Chang L, et al. Development of unilateral peri-lead edema into large cystic cavitation after deep brain stimulation: a case report. Front Neurol. 2022;13:886188. doi:10.3389/fneur.2022.886188
22. Elberson B, Scott H, Dhall R, Petersen E. Impedance trend from a symptomatic perielectrode cystic cavity following deep brain stimulation: illustrative case. J Neurosurg Case Lessons. 2023;6(12):CASE23349. doi:10.3171/CASE23349
23. Leguizamo JM, Monsalve Duarte G, Guarnizo A. Hyperacute brain cyst after deep brain stimulation surgery: a case with complete spontaneous resolution. Neurol Sci off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2025;46(2):1023–1025. doi:10.1007/s10072-024-07797-x
24. DiLorenzo DJ, Jankovic J, Simpson RK, Takei H, Powell SZ. Long-term deep brain stimulation for essential tremor: 12-year clinicopathologic follow-up. Mov Disord off J Mov Disord Soc. 2010;25(2):232–238. doi:10.1002/mds.22935
25. Katlowitz K, Pourfar MH, Israel Z, Mogilner AY. Intraparenchymal cysts following deep brain stimulation: variable presentations and clinical courses. Oper Neurosurg Hagerstown Md. 2017;13(5):576–580. doi:10.1093/ons/opx037
26. Calandra CR, García Fernández C, Raina GB, et al. Intraparenchymal cystic lesion after deep brain stimulation surgery: an unusual complication. Parkinsonism Relat Disord. 2019;64:354–355. doi:10.1016/j.parkreldis.2019.05.016
27. Fenoy AJ, Conner CR, Withrow JS, Hocher AW. Case report of hyperacute edema and cavitation following deep brain stimulation lead implantation. Surg Neurol Int. 2020;11:259. doi:10.25259/SNI_527_2019
28. Sarkar A, Wharen REJ, Utti RJ. Novel Cyst Formation After Deep Brain Stimulator Placement: Description of Case and Treatment. Philadelphia, PA; 2002.
29. Mogilner A, Pourfar M, Baxi N. Incidental asymptomatic intraparenchymal cysts following DBS placement. Mov Disord. 2014;29(Suppl 1):431–432. doi:10.1002/mds.25855
30. Sharma VD, Bona AR, Mantovani A, et al. Cystic lesions as a rare complication of deep brain stimulation. Mov Disord Clin Pract. 2016;3(1):87–90. doi:10.1002/mdc3.12230
31. Gupta HV, Lyons MK, Mehta SH. Teaching NEUROIMAGES: noninfectious cyst as an unusual complication of deep brain stimulation. Neurology. 2016;87(18):e223–e224. doi:10.1212/WNL.0000000000003284
32. Morrison P, Richard I. Long Term Tremor Benefit From Cyst Formation as a Complication of DBS Surgery in a Patient with Parkinson’s Disease. Vancouver, BC; 2017.
33. Asahi T, Ikeda K, Yamamoto J, Muro Y, Mori A, Yamamoto N. Cerebrospinal fluid leakage to the chest subcutaneous pocket due to aggressive brain edema around the leads for deep brain stimulation: a case report and literature review. NMC Case Rep J. 2022;9:357–363. doi:10.2176/jns-nmc.2022-0157
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.