Back to Journals » Medical Devices: Evidence and Research » Volume 18
Dedicated Ultrasonography Versus Magnetic Resonance Imaging for Breast Implant Evaluation, Initial Study
Authors De Faria Castro Fleury E ![]() , Junqueira MRDS, Teixeira TSE, Ferreira PA, Matheus e Castro G, Viotti BAP
, Junqueira MRDS, Teixeira TSE, Ferreira PA, Matheus e Castro G, Viotti BAP
Received 1 December 2024
Accepted for publication 7 March 2025
Published 14 March 2025 Volume 2025:18 Pages 177—189
DOI https://doi.org/10.2147/MDER.S503466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eduardo De Faria Castro Fleury,1,2 Michele Rodrigues da Silva Junqueira,2 Tiago Sarmet Esteves Teixeira,2 Pryscilla Alves Ferreira,2 Giulia Matheus e Castro,1 Bruna Aguiar Portugal Viotti2
1Radiology, Faculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo, Brazil; 2Radiology, Instituto Brasileiro de Controle do Câncer – IBCC, São Paulo, Brazil
Correspondence: Eduardo De Faria Castro Fleury, Email [email protected], [email protected]
Aim: Describe the role of dedicated ultrasound in evaluating breast implants compared to breast magnetic resonance.
Materials and Methods: A prospective observational study was conducted in a single center to evaluate breast implant complications in patients referred to breast magnetic resonance (MRI) scan. All patients who had breast implants submitted to MRI scan were invited to a complementary dedicated ultrasound (US) evaluation of the breast implants. The implant changes were classified following a dedicated protocol. The classifiers used to evaluate the implant include evaluation of implant surface (shell), implant internal content homogeneity, fibrous capsule, intracapsular space, pericapsular space, and axillary extension.
Results: Preliminary results included evaluating 29 consecutive patients who underwent MRI. Twenty-nine patients with 49 implants were included in the study. The US showed a superior ability to assess the internal contents of the implants, the implant surface, and the intracapsular contents. There were no significant statistical differences in evaluating macro changes such as implant location, intracapsular collection, and radio-frequency identification (RFID) presence. MRI was superior to the US in classifying the fibrous capsule type.
Conclusion: US of silicone implants can be used as an alternative to MRI to evaluate implant complications.
Keywords: breast implant, anaplastic large cell lymphoma, breast neoplasm, breast ultrasonography, magnetic resonance imaging, silicone gel
Introduction
In September 2021, the Food and Drug Administration (FDA) agency issued a statement with updated recommendations for silicone implants. The report was based on the public consultation held in the same year to discuss the possible relationship between implants and patient complaints. Amidst the reported complications, Breast Implant Illness (BII) and Anaplastic Large Cell Lymphoma associated with implants (BIA-ALCL) stand out.1
Among the report’s final recommendations, the agency recommends screening for possible complications in asymptomatic patients five years after implant placement, followed by biannual follow-up control, while symptomatic patients should be investigated by diagnostic ultrasonography (US) or magnetic resonance imaging (MRI).1
MRI is the gold standard to evaluate silicone implants due to the possibility of performing silicone-sensitive sequences and to its reproducibility. There is no consensus regarding the contribution of dynamic sequences with contrast enhancement techniques, but there seems to be a tendency to use gadolinium.2
The US has a highly questioned role in evaluating implants. US is generally used as a complementary method for screening breast cancer in dense breasts. Most often, when altered, a diagnostic MRI is suggested. Few articles discuss the role of ultrasound for these patients. However, its availability, price, patient acceptance, and non-use of contrast media count in its favor. Operator-dependent results are the main disadvantage in clinical practice.3,4
In recent years, silicone implants have evolved into their 5th generation. The most modern implants are made of cohesive silicone molecules, which diminishes the assessment of shell rupture. Classic findings in the literature have become rare in modern implants, such as the “linguine sign” to describe intracapsular rupture.5,6
Studies also demonstrated a relationship between breast implant illness (BII) and the gel bleeding from intact implants. It is believed that the implant degrades over time, causing silicone particles to spread throughout the body. Untethered silicone particles are toxic to the human body while activating the immune system in the target organs where it is deposited.7
The objective of this study is to assess whether the US has a role in the evaluation of breast implants in comparison with MRI.
Materials and Methods
This prospective, observational, single-center study, approved by the institutional ethics committee of Instituto Brasileiro de Controle do Câncer- IBCC (São Paulo/ Brazil) and with an informed consent form signed by the patients, was registered on the Brazil Platform under CAAE: 60703822.3.0000.0072
All patients with breast implants referred to MRI examinations between August 2022 and November 2022 were invited to participate, regardless of exam indication. Patients who agreed to participate in the research protocol were included in the study. Patients who refused to undergo additional US were excluded.
Patients were scheduled to have the US scan within one month of the MRI scan. The scheduled patients were examined by the same radiologist who had evaluated the MRI, with 24 years of experience in breast radiology, blinded to the MRI result. We adopted the same parameters for implant evaluation for MRI and US for comparative purposes.
Magnetic Resonance Protocol
All patients underwent routine clinical breast MRI with a 1.5-T (Magnetom Espree, Siemens Healthcare). The protocol used for evaluation was the standard breast protocol, with axial sequences weighted in T1-weighted with fat suppression, axial short-tau inversion recovery (STIR) and each unilateral sagittal sequences in proton density (PD).
The dynamic axial sequences were acquired before and after contrast (gadobenate dimeglumine, MultiHance, Bracco) administration for 4 min. All images were reconstructed in the axial plane with subtraction and maximum intensity-projection (MIP) techniques.
For silicone evaluation, additional silicone-sensitive and silicone-suppressed axial sequences were included.
Ultrasound Protocol
The US was performed following a dedicated evaluation sequence, in which we first evaluated the overall findings of the breast implants, followed by the fibrous capsule, intracapsular contents, pericapsular space, and lymph nodes target evaluations. A linear transducer with a frequency of 15 mHz, Clarius L15 hD3 (Clarius Mobile Health, Vancouver, Canada), was used to assess the overall content, intracapsular collection, and position of the implants. A linear transducer with a frequency of 20 mHz (Clarius L20 hD3) was used for a complimentary evaluation of the implant target evaluation. We used higher-intensity gain curves for the overall investigation. Standard intensity gain curves were opted for evaluating implant surface, pericapsular space, and fibrous capsule.
The reporting system adopted to describe the silicone implant findings in MRI and US followed the descriptors proposed by the authors, which are freely available online on a website (8). The classifier consists of the following evaluations:
Implant
Signal Intensity
Homogeneous or homogeneity loss. Homogeneity loss is considered when the magnetic resonance signal or ultrasound echogenicity is no longer homogeneous, inferring chemical changes in the internal content (Figure 1).
 |
Figure 1 MRI axial STIR with silicone suppression (a), axial silicone sensitive sequence (b), and ultrasonography. RFID near the posterior seal of the implant is shown in the yellow arrow (a, b and d). The green arrow shows the peripheral water droplet sign. The blue asterisk shows the linear beams inside the implant (c). |
Associated findings include central or peripheral “water-droplet” signs or intracapsular rupture. The “water droplet” is the first notable sign to determine changes in the permeability of the implant surface. At the periphery, it usually corresponds to superficial fluid collection (Figure 2). We also evaluated surface vascularization and mass inside the implant content.
 |
Figure 2 Ultrasound with color Doppler and spectral (a and b), sagittal PD (c), and axial post-contrast with fat suppression sequences (d). The green arrow points to the irregularity of the implant surface with peripheral water droplets (a and b). The Orange asterisk shows peripheral water droplets (a–c). The blue arrow points to capsular contracture with increased pericapsular vascularization (a and d). The red arrow shows vascularization inside the implant (a and b). |
Surface Integrity
Evaluation of the implant surface.
Rotation
When present. Assess the location of the posterior seal.
Radio Frequency ID (RFID)
The presence of a magnetic susceptibility artifact in the projection of the implant seal at MRI or an echogenic artifact in the US. Some silicone companies use RFID as a device for identifying breast implants (Figure 1).
Fibrous Capsule
Classification
The fibrous capsule was described in 4 categories following the silicone involvement grading, where Type I would be the least compromised and Type IV would be the most compromised. The main findings in this classification refer to capsular contracture and silicone-induced granuloma of breast implant capsule (SIGBIC) related to breast implants. In more severe cases (type IV), more significant enhancement of the fibrous capsule with pericapsular swelling is observed.8–10
Silicone-induced granuloma of breast implant capsule (SIGBIC): when present (Figure 3).
 |
Figure 3 Axial post-contrast MRI with fat suppression (a), STIR (b), and ultrasound (c and d). The red arrow shows SIGBIC (a–d). The ultrasound shows irregularity of the implant surface in the same red arrow (c and d), with peripheral water droplets. The blue asterisk shows the thickening and irregularity of the fibrous capsule. |
Integrity of the Fibrous Capsule
Assess whether there are signs of capsule discontinuity.
Intracapsular Collection
Mild, moderate, or large.
Vascular Septae
The presence of a vascular bundle that communicates the fibrous capsule with the implant surface (Figure 4).
 |
Figure 4 Post-contrast axial MRI (a) STIR sequences (b), and color Doppler ultrasound (c). Capsular contracture of the breast implant (yellow arrow) with thickening and contrast enhancement (a) and with peripheral water-droplet demonstrated by the green asterisk (b and c). The blue arrow points to vascularized septae (b and c). The green arrow (a and b) indicates vascularized mass inside the implant. |
Vegetative Lesion
Vegetative lesion from the fibrous capsule’s internal surface.
Associated Findings
Ascertain the contiguity of the fibrous capsule with the skin and subcutaneous tissue, the pectoral muscle, and the chest wall. The involvement of the chest wall is also determined by infiltrative inflammation or swelling, as well as the distance between the fibrous capsule and the parietal pleura.
Pericapsular Space
Silicone Migration
Determine whether silicone migration is into the pericapsular, retro pectoral, or axillary regions.
Associated Lesion
Describe findings related to a mass or non-mass enhancement, following the criteria proposed by the BI-RADSTM lexicon.11
Pericapsular Lymph Node
The presence of a regular or altered pericapsular lymph node and associated findings related to silicone gel bleeding.
Axillary Lymph Node
The presence of a regular or altered pericapsular lymph node and associated findings related to silicone gel bleeding.
Comparison Between MRI and US Findings
All positive findings were scored as 1, and at the end of the exam, we accessed the final score of each report automatically generated in a Google Forms dedicated report system. A comparison of the final scores was performed. We also compared the agreement between MRI and the US using the Kappa-weighted test. The Kappa result is interpreted as follows: values ≤ 0 indicating no agreement, 0.01–0.20 as none to slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement.
MedCalc for Windows software, version 19.4 (MedCalc Software, Ostend, Belgium), was used to analyze the results statistically.
Results
From August to November 2022, 79 patients were invited to participate in the research protocol. Of the 79, 29 accepted the invitation, totaling 49 breast implants evaluated. All patients signed the informed consent form. Patients who refused complimentary US were excluded from the study.
Table 1 shows the patient’s characteristics included in the study and the ultrasonography scan time. All patients referred for MRI scans were diagnostic tests. Regarding location, 25 (53.06%) of the implants were subglandular. 17 (34.69%) implants were exposed to radiotherapy treatment. The average examination time was 19.5 minutes (Table 1).
 |
Table 1 Patient’s Characteristics Included in the Study and the Ultrasonography Scan Time |
Table 2 presents the comparative results of each MRI and US findings. The significance level and the Kappa weighted test were also calculated, where the significance level was p<0.0001 (Table 2).
 |
Table 2 Comparative Results of Each MRI and US Findings |
Substantial or almost perfect agreement was observed for the overall findings, such as implant rotation, RFID presence, intracapsular collection, vascular septae, and silicone in the lymph node. There was no agreement for central and peripheral water droplets, surface discontinuity, linear foci inside the implants, and axillary lymph nodes.
Ultrasound showed more findings related to changes in silicone implants. However, MRI was superior for assessing vascularization on the surface of the implants.
Concerning the fibrous capsule, MRI was better at classifying the fibrous capsule type, while ultrasound was better at evaluating the target changes. MRI was superior for assessing associated findings, such as contiguity with the skin, subcutaneous tissue, and chest wall.
Changes in the pericapsular space were also more present in the US, such as extracapsular silicone.
Finally, the MRI detected more axillary lymph nodes than the US did.
Figure 5 show the distribution of the scores by MRI and US. The average score for the US was 8.04 (3–12) (Figure 5), while for MRI 4.0 (0–10).
 |
Figure 5 Distribution of MRI (a) and US (b) scores, with mean, median, and standard deviation. |
Discussion
Silicone breast implants are increasingly noticeable in daily routine, whether through scientific articles discussing the relationship between silicone and breast implant illness, social media-dedicated groups of women discussing their clinical symptoms, or silicone-related academic/scientific discussion.12–14 Over the last five years, the debate has intensified, especially after the FDA issued a report stating new recommendations for silicone, which introduced the “black-box warning” (1). However, the number of aesthetic plastic surgeries for implant placement has increased, which may signal a public health alert for women who report these complications.15
According to the most recent recommendations from the American regulatory agency, some warnings are highlighted: (i) silicone implants are not lifetime devices, with an average lifetime of 10 years; (ii) after changing the silicone implant, the chance of complications doubles compared to the first; (iii) after 5 years of implant placement, asymptomatic patients must undergo preventive screening exams; (iv) MRI is the gold standard for evaluating implants; and (v) implants may be related to systemic diseases known as breast implant illness, and a specific disease called BIA-ALCL (Breast Implant-Associated Anaplastic Large Cell Lymphoma).1
Many of these patients do not have access to information about silicone-related complications, nor do they have access to exams that should screen these changes early. Another difficulty encountered, especially in the United States of America, is the lack of insurance coverage or public health systems to cover expenses related to diagnosis. Currently, MRI remains the gold standard exam for diagnosing silicone complications.1
Our study shows that dedicated US can be a sensitive method for characterizing changes related to device complications, the fibrous capsule, and the pericapsular space. These changes are associated with the chemical reaction inside the breast implants resulting from changes in surface permeability.16 The dedicated US allows a more minimalist evaluation, especially when evaluating more discreet changes, such as implant surface. Higher-frequency probes with better image resolution can also be used for this purpose. MRI, conversely, can show changes in overall access in a less focused way than ultrasound. Generally, the macro changes evaluation criteria were equivalent for both methods, while the minor changes were better evaluated by ultrasonography.
Our results demonstrated that dedicated US to evaluate silicone implants has greater sensitivity for detecting changes in relation to magnetic resonance imaging, with an average of 8/25 scores for US and 4/25 scores for magnetic resonance imaging (Figure 5).
One of the unpublished findings observed in this study was the relationship between an intracapsular superficial fluid layer in the periphery of the implant surface in MRI. These findings were reported as peripheral water droplets inferring signs of surface discontinuity. Subcapsular snowstorm artifacts were observed following MRI findings at the dedicated ultrasound. In these cases, an increase in vascularization in the fibrous capsule is generally associated. These findings indicate a diseased fibrous capsule (Figure 6).
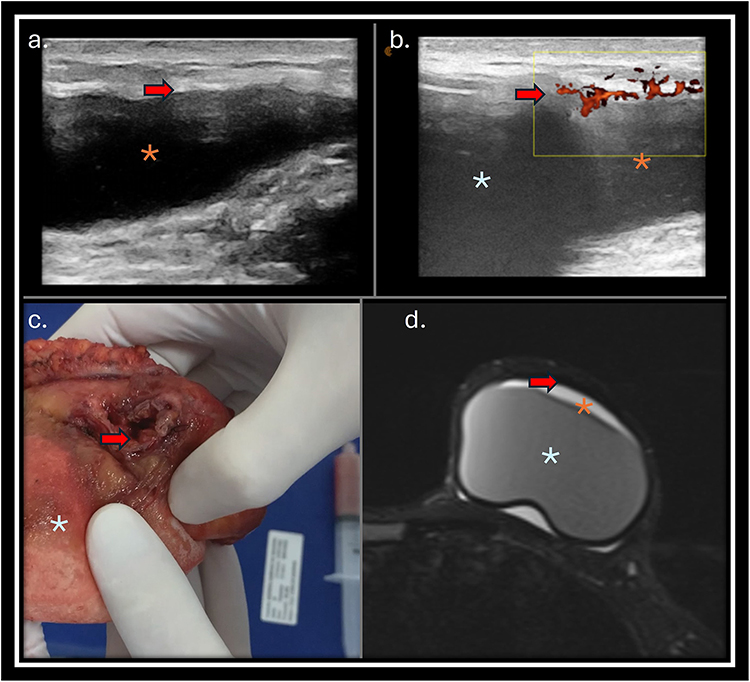 |
Figure 6 Ultrasonography (a) and with color Doppler (b), breast implant macroscopy (c), and MRI axial Stir sequence (d). Capsular contracture of the breast implant with thickening and irregularity of the fibrous capsule shown by the red arrow (a–c). There is also peripheral water droplet in Figures (a and b) and increased flow in the fibrous capsule on the color Doppler study (b). The blue asterisk (b and c) represents the implant, and the Orange asterisk intracapsular collection (a, b, and d). |
The silicone-related changes proposed in this study indicate implant surface degradation, gel bleeding, and chemical reaction of the implant and the fibrous capsule. A description of these findings may help diagnose implant-related complications in patients suffering from BII complaints. The earlier the diagnosis and therapeutic intervention, the lower the patient’s exposure to these toxic particles.15,16
The advent of cohesive gel, introduced in new-generation cohesive silicone implants, makes it difficult to evaluate the internal content of implants using MRI and following the BI-RADSTM recommendation. Descriptors recognized in the literature, such as “linguine sign”, seem increasingly scarce in our practice. While radiologists ignored these new findings presented in this manuscript, the absence of these signs in the report was justifiable. However, when the discussion is open, omission or neglect of these findings may implicate in sub diagnostics or false negative results, directly affecting the proper management of these patients.
This study has some limitations. First is the small number of cases presented and the fact that it was a study carried out in a single center with a single observer. As ultrasound is operator-dependent, studies evaluating inter-observer agreement will be necessary. However, the public health relevance of these findings because of the increase in newly reported cases of silicone implant complications and the constant increase in plastic surgeries using these devices make it imperative to discuss these findings and the role of ultrasonography in silicone implant screening complications. Further studies evaluating more patients and with more observers could validate our initial findings.
Currently, there is no published manuscript or guideline dedicated to silicone implant evaluation. The aim of the study is to propose a dedicated protocol and descriptors for this evaluation. We showed that ultrasonography can be used as an alternative diagnostic tool for implant impairment diagnosis. It is cheaper and more accessible than MRI, but operator-dependent.
Our study proposes that silicone implant evaluation should be performed independently of the descriptors proposed by the BI-RADSTM lexicon. The purpose of creating the BI-RADSTM lexicon was to standardize and audit breast cancer screening and diagnosis. In the case of implant-dedicated US, the presets adopted are dedicated to implants, which impairs the evaluation of breast parenchyma due to the increased gain needed. In addition, a detailed US investigation of silicone implants is time-consuming. Screening of breast parenchyma lesions should be performed after the evaluation of the implants, with an appropriate gain curve.
Conclusions
Ultrasonography showed an excellent ability to detect complications related to breast implants when compared to magnetic resonance imaging, straightforward changes to the surface and content of the implant device, and fibrous capsule impairment.
Abbreviations
FDA, Food and Drug Administration; BII, Breast Implant Illness; BIA-ALCL, Breast Implant-Associated Anaplastic Large Cell Lymphoma; US, Ultrasonography; MRI, Magnetic Resonance Imaging; RFID, Radio Frequency ID; SIGBIC, Silicone-Induced Granuloma of Breast Implant Capsule; BI-RADSTM, Breast Imaging Reporting and Data System.
Data Sharing Statement
All datasets generated or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics
The study complies with the Declaration of Helsinki and was performed according to local ethics committee approval. This prospective, observational, single-center study, approved by the institutional ethics committee (Instituto Brasileiro de Controle do Câncer- IBCC (São Paulo/ Brazil) and with an informed consent form signed by the patients, was registered on the Brazil Platform under CAAE: 60703822.3.0000.0072
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The authors affirm that human research participants provided informed consent for publication of the images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors have no conflicts of interest to declare.
References
1. US Food and Drug Administration: risks and complications of breast implants. 2021. Available from: https://www.fda.gov/medical-devices/breast-implants/risks-and-complications-breast-implants.
2. Mazzocconi L, De Lorenzi F, Carbonaro R, et al. Non-contrast MRI and post-mastectomy silicone breast implant rupture: preventing false positive diagnoses. Eur J Cancer Prev. 2024;33:525–532. doi:10.1097/CEJ.0000000000000887
3. Secco GM, Gutierrez PA, Secco VL, Chico MJ, Secco RA, Pesce KA. Is breast ultrasound a good alternative to magnetic resonance imaging for evaluating implant integrity? Radiologia. 2022;1:20–27. doi:10.1016/j.rxeng.2020.10.011
4. Schafer ME. Fundamentals of high-resolution ultrasound in breast implant screening for plastic surgeons. Clin Plast Surg. 2021;48:59–69. doi:10.1016/j.cps.2020.08.001
5. Torres-Zuniga S, Ziade NV, Zambrano JC. Ultrasound criteria and baker scale for breast implant capsular contracture diagnosis. Plast Reconstr Surg Glob Open. 2022;10:4582. doi:10.1097/GOX.0000000000004582
6. de Faria Castro Fleury E. Clear to cloudy II: radiological perspective of silicone breast implants. Eur J Plast Surg. 2020;43:505–508. doi:10.1007/s00238-019-01612-z
7. Mustafá JCR, Fleury EFC, Dijkman HBPM. Case report: evidence of migratory silicone particles arising from cohesive silicone breast implants. Front Glob Womens Health. 2022;3:730276. doi:10.3389/fgwh.2022.730276
8. Implant Lexicon: imaging guide for interpretation, description and classification for silicone breast implant. 2023. Available from: https://www.silicone-lexicon.com.
9. De Faria Castro fleury E, Castro C. Magnetic resonance classification proposal for fibrous capsules in breast silicone implants. Clin Imaging. 2022;91:26–31. doi:10.1016/j.clinimag.2022.08.010
10. De Faria Castro Fleury E. Why is the baker classification inadequate for classifying silicone implant fibrous capsules? Cureus. 2024;16:55776. doi:10.7759/cureus.55776
11. ACR BI-RADS® Mammography: ACR BI-RADS® Mammography. 2013. Available from: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads-ACR-BI-RADS®-Mammography.
12. Lachmansingh DA. Breast implant illness and psychiatric implications. Ir J Psychol Med. 2022;39:435–436. doi:10.1017/ipm.2019.48
13. Tang SY, Israel JS, Afifi AM. Breast implant illness: symptoms, patient concerns, and the power of social media. Plast Reconstr Surg. 2017;140:765–766. doi:10.1097/PRS.0000000000003785
14. Watad A, Rosenberg V, Tiosano S, et al. Silicone breast implants and the risk of autoimmune/rheumatic disorders: a real-world analysis. Int J Epidemiol. 2018;47:1846–1854. doi:10.1093/ije/dyy217
15. Miranda BH, Banwell PE, Sterne GD, Floyd DC. Breast implant illness: a United Kingdom patient-centred approach. J Plast Reconstr Aesthet Surg. 2024;98:201–210. doi:10.1016/j.bjps.2024.07.066
16. Fleury EF. Silicone induced granuloma of breast implant capsule (SIGBIC) diagnosis: breast magnetic resonance (BMR) sensitivity to detect silicone bleeding. PLoS One. 2020;15:0235050. doi:10.1371/journal.pone.0235050
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.