Back to Journals » International Journal of Women's Health » Volume 18
Decreased CD8+ T Lymphocytes is an Independent Influencing Factor for Persistent HR-HPV Infection
Authors Huang M, Lei H ![]() , Lin Y, Li W, Guo J, Liu Q, Chen L, Xie F, Weng X, Kang Y
, Lin Y, Li W, Guo J, Liu Q, Chen L, Xie F, Weng X, Kang Y ![]() , Lin H, Sun P
, Lin H, Sun P ![]()
Received 29 January 2026
Accepted for publication 27 May 2026
Published 11 June 2026 Volume 2026:18 599791
DOI https://doi.org/10.2147/IJWH.S599791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
MeiXiu Huang,1,2,* HuiFang Lei,1,* YanHua Lin,1 WeiWei Li,1 JianFeng Guo,3 QingYu Liu,1 LanLan Chen,1 Fang Xie,1 XiuQing Weng,4 YaFang Kang,2 HanFeng Lin,5 PengMing Sun2,6,7
1Department of Gynecology, Ningde Mindong Hospital, Fujian Medical University, Fuan, People’s Republic of China; 2Laboratory of Gynecologic Oncology, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fuzhou, People’s Republic of China; 3Department of Laboratory, Ningde Mindong Hospital, Fujian Medical University, Fuan, People’s Republic of China; 4Department of Pathology, Ningde Mindong Hospital, Fujian Medical University, Fuan, People’s Republic of China; 5Department of Obstetrics, Ningde Mindong Hospital, Fujian Medical University, Fuan, People’s Republic of China; 6Fujian Key Laboratory of Women and Children’s Critical Diseases Research, Fuzhou, People’s Republic of China; 7School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: HanFeng Lin, Department of Obstetrics, Ningde Mindong Hospital, Fujian Medical University, Fuan, People’s Republic of China, Email [email protected] PengMing Sun, Laboratory of Gynecologic Oncology, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, People’s Republic of China, Email [email protected]
Objective: To explore the characteristics of vaginal microecological changes and peripheral blood immune cell subset levels in patients with high-risk human papillomavirus (HR-HPV) infection, and to identify independent risk factors for persistent HR-HPV infection, so as to provide a reference for clinical prevention and treatment of cervical lesions.
Methods: A total of 165 participants admitted to Ningde Mindong Hospital from January 2021 to December 2022 were enrolled in this single-center observational study, including 49 cases with persistent HR-HPV positivity and 116 cases with transient HR-HPV infection. Vaginal microecological indicators (cleanliness, pH, bacterial vaginosis score, hydrogen peroxide, sialidase) and peripheral blood immune cell subsets were detected to analyse.
Results: Compared with the transient HR-HPV infection group, the persistent infection group showed significant vaginal microecological imbalance, including lower proportion of grade I-II vaginal cleanliness, higher BV score ≥ 4, lower proportion of pH ≤ 4.5, and higher positive rates of hydrogen peroxide and sialidase (all P< 0.05). In addition, in the present study, sialidase was also significantly increased in the group with cytological and pathological results ≥HSIL (P< 0.05). The percentages of CD4+ T lymphocytes and CD8+ T lymphocytes in the persistent infection group were significantly decreased (P< 0.05), while there were no significant differences in T lymphocytes, B lymphocytes, and NK cells between the two groups (P> 0.05). Multivariate Logistic regression analysis showed that decreased CD8+ T lymphocytes was an independent risk factor for persistent HR-HPV infection (P< 0.05).
Conclusion: Persistent HR-HPV infection is closely associated with vaginal microecological imbalance and impaired cellular immune function. This exploratory study confirms that decreased CD8+ T lymphocytes is independently associated with persistent HR-HPV infection. Comprehensive assessment of vaginal microecological status and CD8+ T lymphocyte level may help identify high-risk populations, but the clinical predictive value needs to be verified by large-sample prospective studies.
Keywords: vaginal microbiota, lymphocytes, high risk human papillomavirus
Introduction
Cervical cancer (CC) is one of the most common gynecological malignancies.1 The pathogenesis of CC is complex, among which high-risk human papillomavirus persistent infection is considered to be an important inducing factor for the occurrence and development of CC.2 Long-term persistent HR-HPV infection can easily lead to the occurrence of cervical intraepithelial neoplasia (CIN), which may further progress to invasive CC. Nevertheless, not all HR-HPV infections and CIN lesions will eventually develop into CC, indicating that multiple host-related factors are also involved in disease progression. Accumulating evidence has demonstrated that alterations in the vaginal microenvironment exert important regulatory effects on the development and progression of cervical diseases.3–5
The vaginal microecology is composed of vaginal flora and immune mediators. When the vaginal microecology is unbalanced, Lactobacillus is replaced by various anaerobic bacteria, which can induce the generation of pro-inflammatory immune mediators and reactive oxygen species, resulting in genomic changes of epithelial cells, affecting cell proliferation and apoptosis.6 Vaginal microecological imbalance and HPV infection have an interactive effect, which can promote the occurrence and development of cervical diseases together.7 A number of previous clinical studies have found that the detection rate of Prevotella in vaginal secretions of patients with cervical lesions is significantly higher than that of healthy controls.3,4 Increased abundance of Prevotella and Gardnerella was observed in cases of persistent HR-HPV infection and HSIL.3 It has been shown that BV-associated bacteria, including Megasphaera elsdenii and Prevotella, induce maturation of dendritic cells, leading to increased production of proinflammatory cytokines (IL-1β, IL-6, IL-8, IL-12, and TNF-α) and enhanced immune responses.8 Abnormal immune activation and infiltration release oxidative stress factors and potential carcinogens, which may accelerate DNA damage in cervical-vaginal cells and enhance the carcinogenic effect of HR-HPV.
Routine clinical vaginal microecological detection mainly includes the evaluation of vaginal cleanliness, pH value, bacterial vaginosis (BV) score, aerobic vaginitis (AV score), as well as the detection of hydrogen peroxide, leukocyte esterase and sialidase. This approach has the advantages of simple operation, low cost and convenient large-scale clinical screening, and can rapidly evaluate the overall status of vaginal microecological balance. However, its resolution is limited. It cannot accurately identify bacterial species or detect uncultured and low-abundance microorganisms, making it difficult to explore the underlying mechanism at the species level. In contrast, high-throughput 16S rRNA sequencing can precisely characterize vaginal microbial structure, species abundance and community diversity, but it is relatively expensive and time-consuming, and is not suitable for large-sample clinical population studies.
The immune system plays a vital role in tumor initiation and progression. After invading the host, HPV can be effectively eliminated by both cellular and humoral immune responses. However, HPV can survive persistently by escaping host immune surveillance. Impaired immune function reduces the abundance of vaginal lactobacilli, disrupts reproductive tract microecological homeostasis, weakens local immune defense, and subsequently induces excessive proliferation of pathogenic microorganisms, thereby facilitating the development of reproductive tract infections and cervical lesions. It has been confirmed that the progression of cervical lesions is closely related to local immunosuppression.9,10 Studies have found that the expression level of IL-4 is increased in the progression of cervical lesions, which may be due to the increased expression of IL-4, causing the immune escape of the lesion cells, leading to the decrease of the body’s immune response to the tumor, thus accelerating the cervical lesions.10 In addition, significant increases in IL-1β and TNF-α levels have been demonstrated in samples with persistently abnormal vaginal microbiota in vivo.11 In women with high abundance of Prevotella, significant responses to LPS, IFN-γ, and IL-1β were observed, which may reflect an immune response to Gram-negative bacteria.3 From the above results, it can be seen that the local cervical immune function of patients with cervical lesions is significantly altered.
Therefore, this study aimed to observe the changes of vaginal microecological indicators and peripheral blood immune cell subsets in patients with cervical lesions, and to explore their relationships with HR-HPV infection and lesion progression, so as to provide theoretical reference for clinical prevention and treatment of cervical lesions.
Methods
Study Subjects
This was a single-center observational study. A total of 165 participants admitted to Ningde Mindong Hospital from January 2021 to December 2022 were enrolled, including 49 cases with persistent HR-HPV positivity and 116 cases with transient HR-HPV infection. All subjects were diagnosed with HR-HPV positivity by HPV testing, voluntarily signed the informed consent form, and cooperated with the entire process of testing and follow-up. Persistent HPV infection is defined as detection of the same HPV genotype at ≥6 month intervals in cervical specimens, which has been used in previous exploratory studies on HPV persistence.12,13 The Ethics Committee of Mindong Hospital in Ningde City approved this study (Ethics No.2021081306H), and all individuals in this study signed an informed consent form. This study was conducted in accordance with the Declaration of Helsinki.
Inclusion Criteria
1) history of sexual activity; 2) no previous treatment or chemoradiotherapy for cervical lesions; 3) no severe immune system diseases.
Exclusion Criteria
1) vaginal cleaning within 48h, vaginal medication, or sexual intercourse within the last 3 days; 2) Oral antibiotics or immunosuppressive agents for 1 month.
Grouping Basis
Subjects were grouped according to the duration of HR-HPV infection. Those with persistent HR-HPV positivity for ≥6 months (positive in two or more consecutive tests with an interval of ≥3 months) were included in the persistent infection group (49 cases); those who turned negative within 6 months after HR-HPV positivity and had no recurrence during subsequent follow-up were included in the transient infection group (116 cases).
Subject Recruitment Process
The recruitment of subjects strictly followed the principles of “voluntary participation, informed consent, random inclusion, and strict screening”, and the specific process was as follows:
The recruitment sources were patients who visited the gynecology outpatient department and the cervical disease specialty department of Ningde Min Dong Hospital for colposcopy. The specific process is shown in Figure 1. Trained medical staff explained the purpose, process, potential risks and benefits of the study in detail to the subjects who met the preliminary conditions. After the subjects voluntarily signed the informed consent form, general demographic data (age, reproductive history, sexual history, past medical history, etc.) were collected, and vaginal microecological testing, peripheral blood immune cell subset testing, cervical cytology and pathological examination were completed. Finally, the study subjects were determined and included in the statistics according to the inclusion criteria, exclusion criteria and grouping basis.
 |
Figure 1 Flow chart of study participants. Abbreviations: HR-HPV, High risk human papillomavirus; TCT, Thinprep cytologic test; LSIL, Low-grade squamous intraepithelial lesion; HSIL, High-grade squamous intraepithelial lesion. |
Detection Indicators and Methods
Cytological Samples Were Collected
Cervical cells were collected from the cervix of all participants using a plastic brush, identified in TinPrep preservation cell solution (Hologic Inc., Madison, Wisconsin), and specimens were immediately stored in the laboratory at 4°C.
Detection of Vaginal Microbial Metabolites
Vaginal secretions from the side of the vagina, on a clean slide, were examined microscopically for triconads, hyphae, cue cells. Hydrogen peroxide, leukocyte esterase and sialidase in secretions were detected by vaginitis automatic detector and matching detection kits. Vaginal PH was determined using the color strip method. If the PH value was no greater than 4.5 (pH≤ 4.5), the result was considered to be normal. Conversely, a pH> 4.5 was considered abnormal. Vaginal cleaning was diagnosed according to the criteria of the National Clinical Laboratory Practice Guideline: I–II was defined as normal vaginal cleaning and III–IV as abnormal vaginal cleaning. AV, BV, CV, TV and VVC were all negative or positive. BV was diagnosed by Nugent scoring method. Nugent scores were calculated by assessing Lactobacillus morphology (score 0–4), vaginal Lactobacillus morphology (score 0–4), and mobile bacilli morphology (score 0–2). A Nugent score of 7–10 is consistent with BV, 4–6 is considered moderate, and 0–3 is considered negative for BV. Colorless SNA was defined as normal (−) and red or purple as positive (+). LE colorless was defined as normal (−) and green or blue as positive (+). Hydrogen peroxide (H2O2): >2 mmol/L was negative (−), <2 mmol/L was positive (+), reflecting the functional status of Lactobacillus. All laboratory procedures were performed according to the manufacturer’s instructions.
Flow Cytometric Analysis of PBLs
Fresh peripheral blood samples (5 mL) were collected from patients using EDTA anticoagulant tubes. Twenty microliters of BD Multitest 6-color TBNK reagent (BD catalog number 337,166) was placed into the bottom of a BD Trucount tube, and 50 µL of heparinized whole blood was added to the tube, mixed with vortex, and incubated for 15 min protected from light. Then, 450 µL of 1X BD FACS lysing solution was added and incubated again for 15 min protected from light. Finally, with a BD Canto II, we analyzed fresh blood samples for total Lym subset distributions, including T lymphocytes, B lymphocytes, NK cells, CD4+T lymphocytes, and CD8+ T lymphocytes. All manipulations were carried out at room temperature (20°C-25°C).
Liquid-Based Cytology
Cytological samples were blinded, independently assessed by two experienced cytopathologists, and reassessed until a consensus diagnosis was reached. Cytological diagnoses were classified as NILM, atypical squamous cells (ASCUS), low grade squamous intraepithelial lesion (LSIL), high grade squamous intraepithelial lesion (HSIL), atypical squamous cells, and it was impossible to exclude high grade squamous intraepithelial lesion (ASC-H), squamous cervical cancer (SCC), and atypical glandular cells (AGC).
Histology
According to the cervical cancer screening program, women with HR-HPV infection or abnormal cytological results can be referred for colposcopy or biopsy. When ≥HSIL was diagnosed by biopsy, patients underwent loop electrosurgical excision cone or cold knife cone biopsy. Formalin (10%) was used for pathological specimens, and 10,4µm thick histological sections were cut and stained with hematoxylin and eosin using standard methods. Cervical biopsy specimens were examined and diagnosed according to the CIN system. If the examination reading was inconsistent, a second histology was performed. If two-thirds of the diagnoses were identical, the result was considered final.
Follow-Up Plan
To dynamically observe the changes of HR-HPV infection status, vaginal microecology and immune cell subsets, and clarify the outcome of infection, a full-course standardized follow-up plan was formulated:
Follow-Up Time Points
1) Baseline follow-up (at recruitment and enrollment): Complete all baseline tests (vaginal microecology, peripheral blood immune cell subsets, cervical cytology, pathological examination) and data collection; 2) Endpoint follow-up (6 months after enrollment): Recheck HR-HPV, vaginal microecology, peripheral blood immune cell subsets, and cervical cytology to clarify the outcome of HR-HPV infection (persistent positivity/negative conversion), and collect the subjects’ clinical outcome data.
Follow-Up Methods
A combination of “outpatient follow-up + telephone follow-up” was adopted. Subjects were preferentially arranged to receive outpatient follow-up in the hospital to complete relevant tests; for those who could not go to the hospital, telephone follow-up was used to understand their health status and medication situation, and remind them to go to the hospital in time to complete the tests to ensure the completeness of follow-up data.
Follow-Up Content
1) General situation: Record the changes of the subjects’ age, weight, living habits (smoking, drinking, etc.), medication history (antibiotics, hormones, etc.), and reproductive status; 2) Laboratory tests: HR-HPV detection (clarify the infection subtype and negative conversion status), vaginal microecological indicators (cleanliness, pH value, BV score, hydrogen peroxide, sialidase), peripheral blood immune cell subsets (CD4+T lymphocytes, CD8+T lymphocytes, total T lymphocytes, B lymphocytes, NK cells); 3) Clinical outcomes: The progression of cervical lesions (such as changes in CIN grade, whether it progresses to HSIL, etc.) and the occurrence of adverse reactions.
Handling of Loss to Follow-Up
For subjects who were lost to follow-up during the follow-up period, the reasons for loss to follow-up (such as relocation, refusal to follow-up, inability to cooperate due to aggravated illness, etc.) were recorded in detail, and attempts were made to track them through telephone, family contact and other methods. If tracking failed, they were included in the lost-to-follow-up cases.
Handling of Missing Data
This study strictly standardized the follow-up and detection processes to minimize data missing. For missing data occurring during the study (such as missing partial detection indicators, incomplete follow-up data, etc.), scientific and reasonable methods were adopted for processing to ensure data integrity and the reliability of statistical analysis.
Adjustment of Confounding Factors
To exclude the interference of confounding factors on the study results and ensure the accuracy of the study conclusions, the following methods were used for adjustment of confounding factors:
Screening of Confounding Factors
Combined with relevant literature reports and the baseline data of this study, the confounding factors that may affect persistent HR-HPV infection were initially screened, mainly including: 1) Demographic factors (age, BMI, educational level); 2) Reproductive and sexual factors (number of pregnancies and deliveries, frequency of sexual activity, number of sexual partners); 3) Clinical factors (status of vaginal microecological imbalance, grade of cervical lesions, past gynecological disease history); 4) Other factors (smoking history, drinking history, hormone use history).
Adjustment Methods
1) Univariate analysis: Chi-square test (for categorical variables) or Mann–Whitney U-test (for continuous variables) was used to analyze the correlation between each confounding factor and persistent HR-HPV infection, and factors with P<0.05 were selected and included in the multivariate adjustment model; 2) Multivariate adjustment: Logistic regression analysis was used, with persistent HR-HPV infection (yes/no) as the dependent variable, the confounding factors screened by univariate analysis as independent variables, and the core observation indicators of this study (vaginal microecological indicators, CD8+T lymphocyte levels) were included for multivariate adjustment. The adjusted OR value and 95% confidence interval (95% CI) were calculated to exclude the interference of confounding factors and clarify the independent association between core indicators and persistent HR-HPV infection.
Explanation of Adjustment
In the statistical analysis section of the paper, the confounding factors included in the adjustment were clearly listed, the adjustment methods and processes were detailedly explained, and the possible impact of confounding factors on the study results was analyzed in the discussion section to ensure the scientificity and reliability of the study conclusions.
Statistical Analysis
Continuous variables were analyzed by t-test or Mann–Whitney U-test. Categorical variables were analyzed by χ2 test or Fisher’s exact test. Receiver operating characteristic (ROC) curves were used to determine cut-off points for continuous data. Risk factors associated with HR-HPV infection were obtained by univariate and multivariate binary logistic regression analysis. Variables with P<0.05 in univariate analysis were included in multivariate regression. Data were calculated in this study using the IBM SPSS statistical package version 22.0 (IBM, Inc., Armonk, USA). The significance level was set at p-value<0.05.
Results
Baseline Characteristics of Participants
A total of 165 patients were finally enrolled in this study, including 49 cases with persistent HR-HPV positivity and 116 cases with transient HR-HPV infection (Figure 1). Group analysis was performed based on whether HR-HPV was persistently positive, and Table 1 presents the baseline characteristics of the two groups. No statistically significant differences were observed between the transient and persistent HPV infection groups in terms of age, menopausal status, reproductive history, history of diabetes mellitus, history of hypertension, or condom use (all P>0.05, Table 1). However, significant differences existed between the two groups in smoking history, drinking history, oral contraceptive use, and number of sexual partners in the past 5 years (all P<0.05, Table 1). Specifically, the proportions of smokers (15.52% vs 4.08%) and drinkers (12.07% vs 10.20%) were lower in the persistent HPV infection group, while the proportions of oral contraceptive users (10.20% vs 1.72%) and those with ≥3 sexual partners in the past 5 years (14.29% vs 4.31%) were higher. There was no statistically significant difference in the age of first sexual intercourse between the two groups (P>0.05, Table 1).
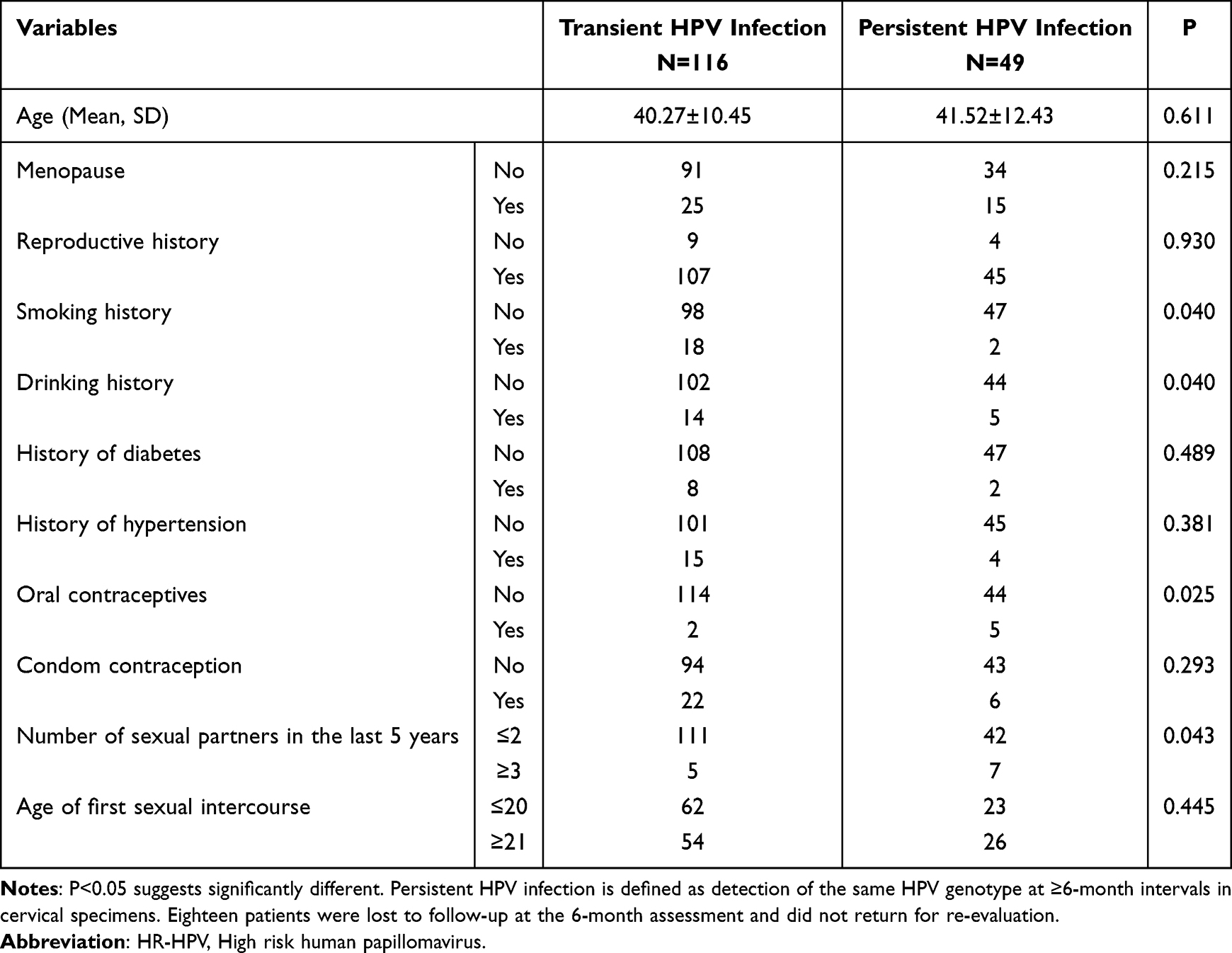 |
Table 1 Baseline Characteristics of Participants |
Relationship Between Vaginal Microenvironment and Persistent HR-HPV Infection
Table 2 shows the comparison of vaginal microecological factors between women with transient and persistent HR-HPV infection, with significant differences in multiple vaginal microecological indicators between the two groups (all P<0.05). Regarding vaginal cleanliness, 58.62% (68/116) of women in the transient HPV infection group had grade I-II cleanliness, compared with only 42.86% (21/49) in the persistent infection group (P<0.05, Table 2). The proportion of participants with a bacterial vaginosis (BV) score ≥4 was significantly higher in the persistent infection group (71.43%, 35/49) than in the transient infection group (44.83%, 52/116) (P<0.05, Table 2). For vaginal pH value, 42.24% (49/116) of participants in the transient infection group had a pH ≤4.5, while this proportion was only 24.49% (12/49) in the persistent infection group (P<0.05, Table 2).
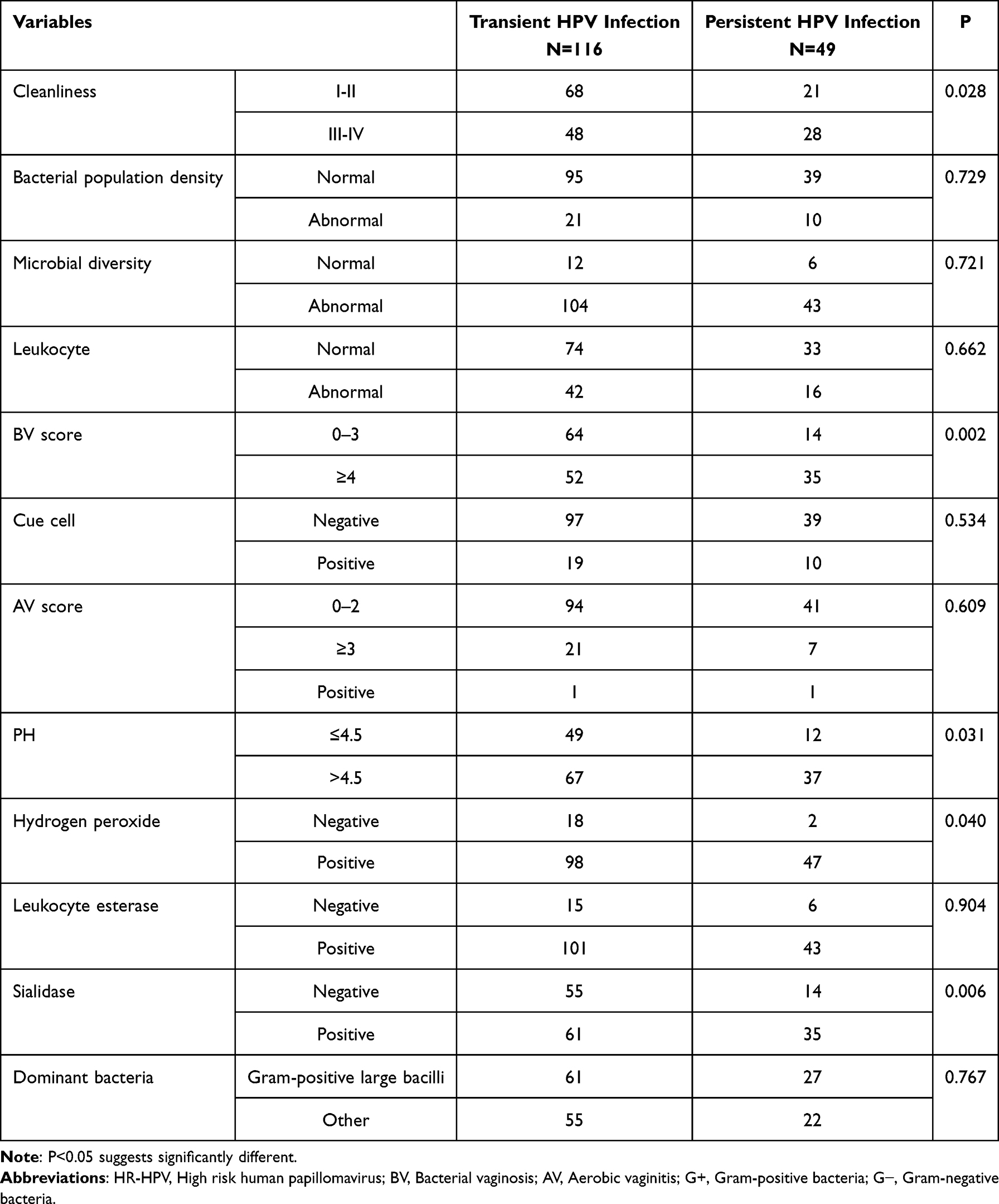 |
Table 2 The Changes of Vaginal Microecological Factors Between Transient and Persistent HPV Infection Women |
Among the microecological functional indicators, the positive rate of hydrogen peroxide in the persistent infection group (95.92%, 47/49) was significantly higher than that in the transient infection group (84.48%, 98/116) (P<0.05, Table 2). In addition, the positive rate of sialidase in the persistent infection group (71.43%, 35/49) was also higher than that in the transient infection group (52.59%, 61/116) (P<0.05, Table 2). No statistically significant differences were found between the two groups in bacterial population density, microbial diversity, leukocyte count, clue cell status, aerobic vaginitis (AV) score, leukocyte esterase, or dominant bacteria (all P>0.05, Table 2).
Furthermore, Table 3 presents the comparison results of vaginal microecological factors between subjects with persistent HR-HPV infection and those with persistent HPV 16/18 subtype infection. There were no statistically significant differences between the two groups in all vaginal microecological indicators (all P>0.05).
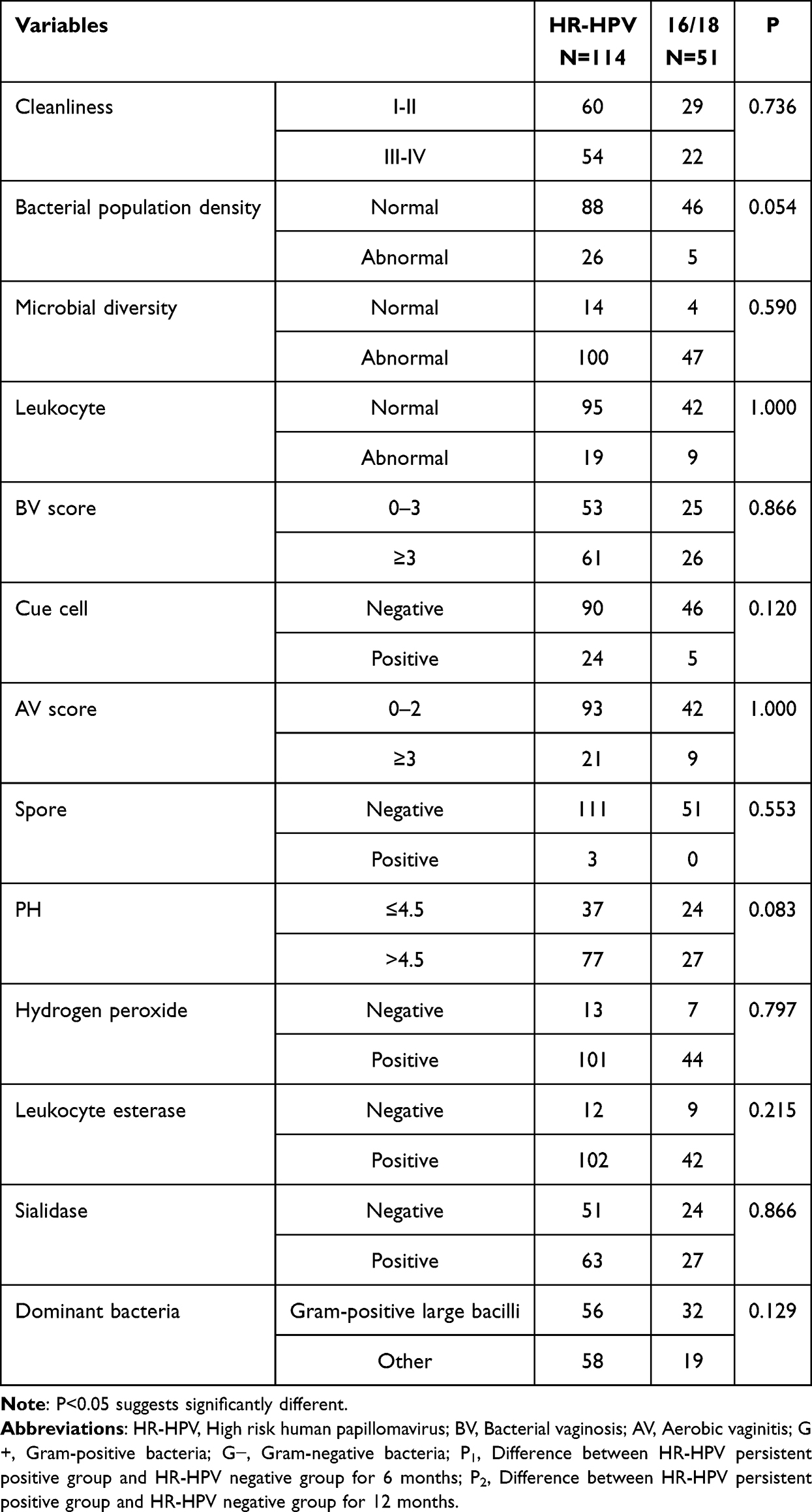 |
Table 3 The Changes of Vaginal Microecological Factors Between Different Persistent HPV Infection Women |
Correlation Between Cervical Cytology/Pathology and Persistent HPV Infection
Table 4 shows the correlation between cervical cytological/pathological results and persistent HR-HPV infection. There was no significant difference in cytological results between the two groups (P>0.05, Table 4): the proportion of cytology ≥ high-grade squamous intraepithelial lesion (HSIL) was 30.17% (35/116) in the transient group and 26.53% (13/49) in the persistent group. However, the pathological results differed significantly between the two groups (P<0.05, Table 4): the proportion of pathology ≥HSIL was 48.28% (56/116) in the transient group, which was higher than 48.98% (24/49) in the persistent group. No significant difference was observed in HR-HPV genotyping (including subtypes 16/18) between the two groups (P>0.05, Table 4).
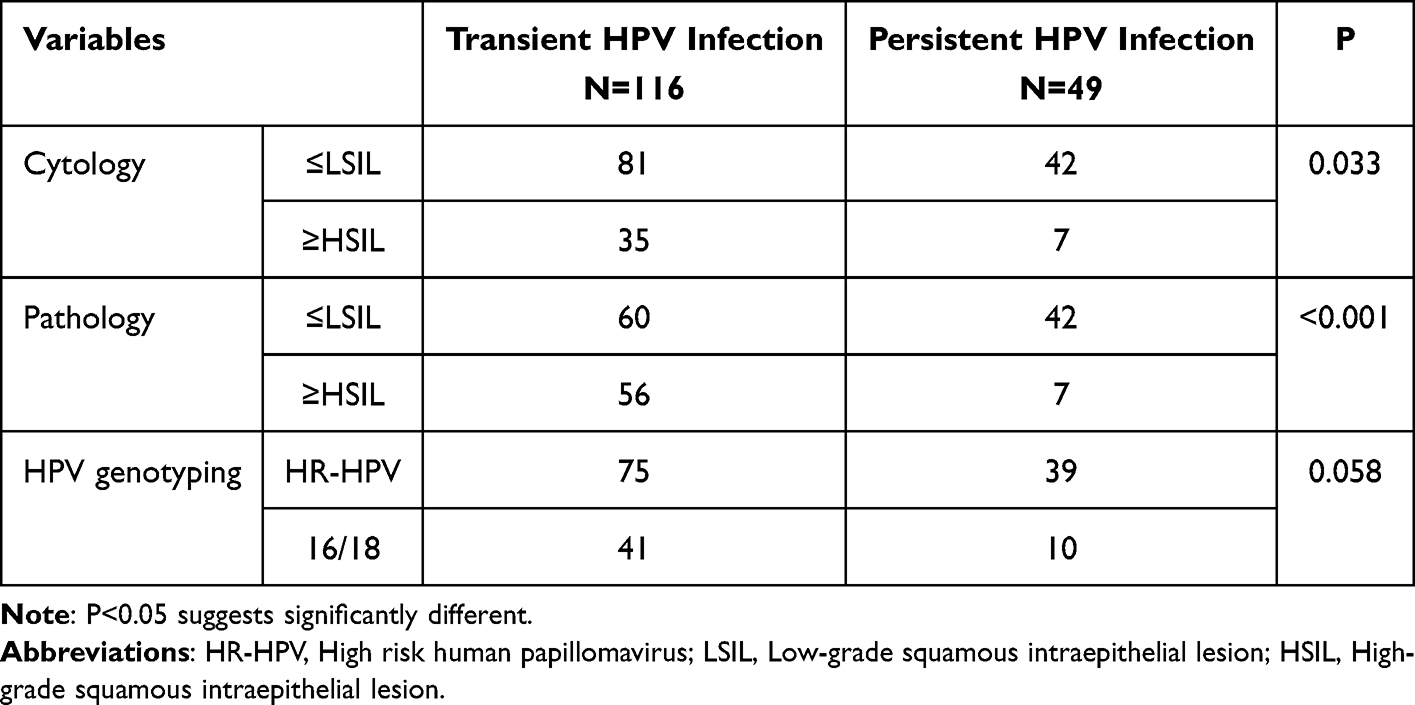 |
Table 4 The Correlation Between Pathology and Persistent HPV Infection |
Relationship Between Vaginal Microenvironment and Cervical Lesions
Subgroup analysis was also performed based on the results of cytology and colposcopic cervical biopsy. The results of the study showed that patients with cytological results ≥HSIL had a higher positive rate of sialidase (P < 0.05, Table 5). The positive rate of sialidase was higher in patients with pathological biopsy results ≥HSIL (P < 0.05, Table 5).
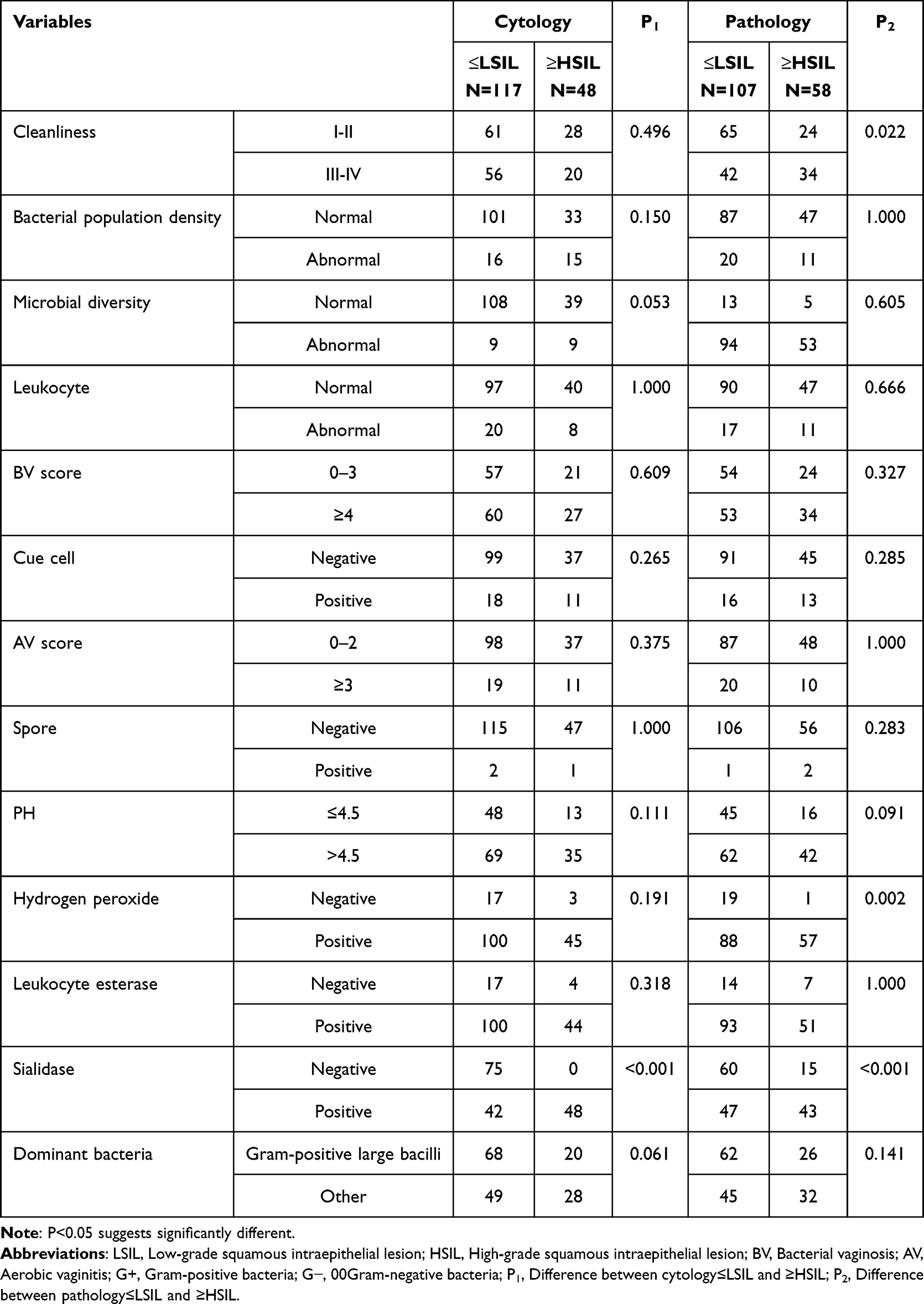 |
Table 5 The Changes of Vaginal Microecological Factors Between Different Cervical Lesions |
Relationship Between Peripheral Immune Cells and HR-HPV Infection and Cervical Lesions
The results of this study showed that compared with the serum immune cell levels of patients with transient HR-HPV infection, the percentages of CD4+ T lymphocytes and CD8+ T lymphocytes in patients with persistent HR-HPV positivity were significantly decreased (Figure 2, P < 0.05). No statistically significant differences were found in the percentages of T lymphocytes, B lymphocytes, or natural killer (NK) cells between the transient HR-HPV infection group and the persistent HR-HPV positivity group (Figure 2, P > 0.05).
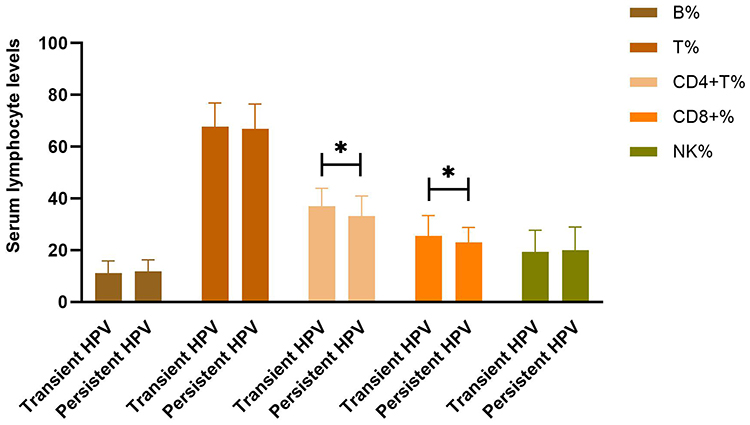 |
Figure 2 Expression of peripheral blood immune cells. The expressions of B lymphocytes, T lymphocytes, CD4+T lymphocytes, CD8+T lymphocytes and NK cells were compared between HR-HPV persistent positive group and transient HR-HPV group. *Means P<0.05, which suggests significantly different. Abbreviation: HR-HPV, High risk human papillomavirus. |
Independent Risk Factors Associated with Persistent HR-HPV Infection
Based on the results of Tables 1, 2, and Figure 2, further Logistic regression analysis was performed to include factors significantly associated with persistent HR-HPV infection and explore the independent risk factors related to persistent HR-HPV infection. Receiver operating characteristic (ROC) curve analysis was conducted to determine the cut-off values of CD4+ T lymphocytes and CD8+ T lymphocytes (Figure 3), and they were grouped according to the cut-off values. Univariate regression analysis showed that the number of sexual partners, oral contraceptive use, vaginal cleanliness, BV, sialidase, and CD8+ T lymphocytes were significantly associated with persistent HR-HPV infection (Figure 4a, P < 0.05). Further multivariate Logistic regression analysis revealed that decreased CD8+ T lymphocytes was an independent risk factor for persistent HR-HPV infection (Figure 4b, P < 0.05).
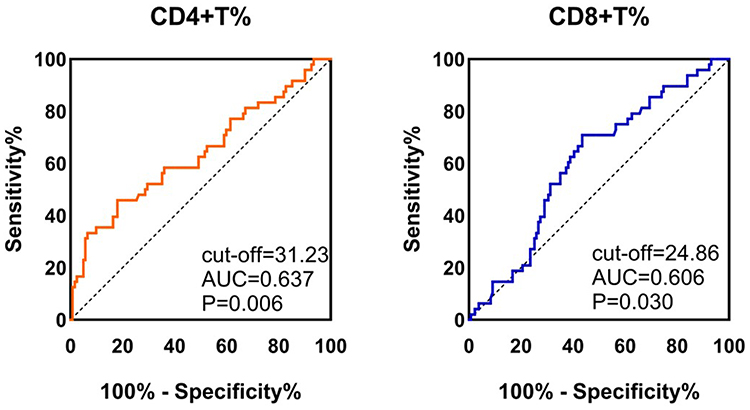 |
Figure 3 The ROC curve. The ROC curve for CD4+T lymphocytes and CD8+T lymphocytes cells. The cut-off values for these indicators were identified. P<0.05 suggests significantly different. |
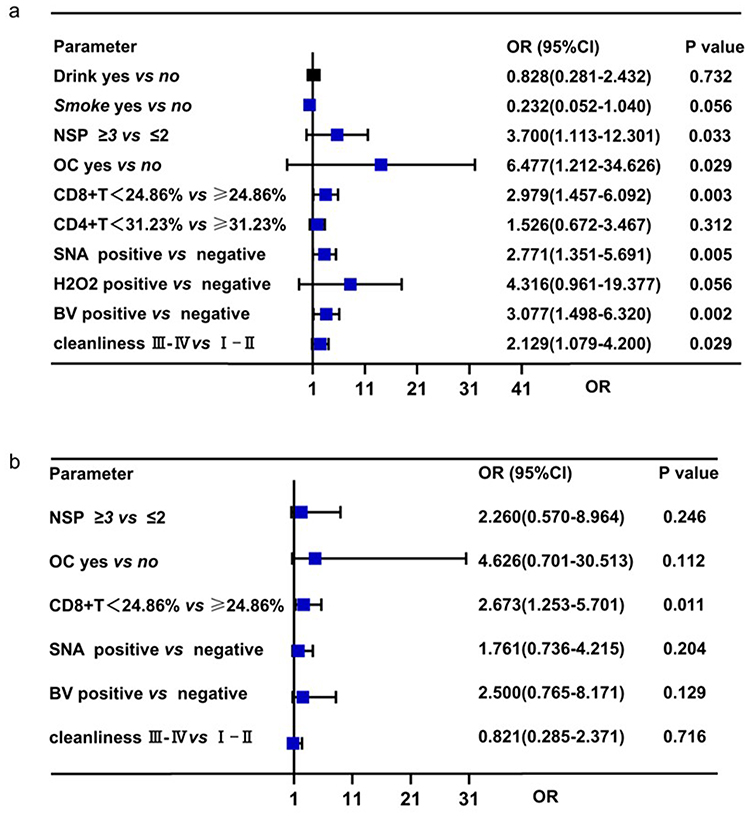 |
Figure 4 The logistic regression analyses. (a) The univariate Logistic regression analyses for persistent HR-HPV(+). (b) The multivariate logistic regression analyses for persistent HR-HPV(+). P<0.05 suggests significantly different. Abbreviations: SNA, Sialidase; H2O2, Hydrogen peroxide; BV, Bacterial vaginosis; OC, oral contraceptives; NSP, Number of sexual partners in the last 5 years. |
Discussion
In the process of cervical and vaginal carcinogenesis induced by HPV infection, microbiota plays a pathogenic or protective role mainly by regulating inflammatory and immune responses in the lower genital tract, affecting HR-HPV oncogene expression and oncoprotein production, regulating oxidative stress and DNA damage, and affecting tumor metabolism.14 This study comprehensively analyzed the characteristics of vaginal microecology changes and the expression of peripheral blood immune cells in patients with HR-HPV infection, and combined the data of lower genital tract microecology and peripheral blood immune cells to predict the risk of HR-HPV infection, which was innovative. This is a single-center observational study with a small sample size, and the results are exploratory and hypothesis-generating, which cannot confirm a causal relationship. The research results provide insights into the multi-factorial regulatory mechanism of persistent HR-HPV infection for clinical intervention and management of HR-HPV infected patients.
The vaginal microenvironment plays a crucial role in maintaining the integrity of the cervical mucosa and resisting pathogen invasion. Its imbalance is closely related to HPV infection and persistence. The results of this study show that persistent HR-HPV infection is associated with poor vaginal cleanliness, bacterial vaginosis, elevated vaginal pH, and increased positive rates of hydrogen peroxide and sialidase, suggesting a severe state of vaginal microecological disorder. A healthy vaginal microecology is dominated by Lactobacillus, which maintains the vaginal acidic environment (pH 3.8–4.5) by producing lactic acid and secretes hydrogen peroxide to inhibit the growth of pathogenic bacteria. The proportion of pH ≤ 4.5 decreased while the positive rate of hydrogen peroxide increased in the persistent infection group, suggesting dysfunction of Lactobacillus.15–17 Hydrogen peroxide can kill and inhibit pathogenic microorganisms, while catalase can decompose hydrogen peroxide, inhibit its killing effect of pathogenic microorganisms, and make pathogenic microorganisms survive and reproduce in the vagina, which will increase the susceptibility to HPV.15 Reproductive system infection can further reduce vaginal cleanliness, leading to abnormal levels of proline aminopeptidase, catalase and other enzymes, forming a vicious cycle and aggravating the disorder of vaginal microecological environment. A variety of bacterial species in the female vagina are interdependent and mutually restricted. Certain species of bacteria can maintain the vaginal microecological balance, but too few or too many species of bacteria may destroy the vaginal microecological balance and increase the chance of HR-HPV infection. BV is mainly due to the reduction of Lactobacillus and the imbalance of vaginal flora. In this study, BV positivity is a risk factor for HR-HPV infection. The analysis of the reason is that BV-associated anaerobic bacteria can release ammonia substances, cause vaginal microecological environment disorder, destroy the protective mucosal barrier, damage or change epithelial cells, and increase the susceptibility to HPV. In addition, in the present study, sialidase was also significantly increased in the group with cytological and pathological results ≥HSIL. SNA is an enzyme that cleans terminal sialic acid residues and is associated with tissue destruction, immune response evasion, bacterial invasion, and access to nutrients associated with bacteria. In addition to Gardnerella, such as Prevotella, Bacteroides, and Mobile bacteria also produce SNAs.18 Previous studies have shown that SNA is closely related to HPV infection and cervical lesions.4
Our study also showed that the percentage of serum CD4+T lymphocytes, CD8+T lymphocytes was significantly decreased in patients with persistent HR-HPV infection. The decreased percentage of CD8+T lymphocytes in serum are independent risk factors for persistent HR-HPV infection. The immune system plays an important role in the occurrence and development of tumors. When HPV virus invases the human body, it can be effectively eliminated by the immune system, which includes cellular immunity and humoral immunity. CD4 + T lymphocytes are an extremely important part of the host immune defense. When the body is in an immunosuppressed state, the chance of HPV infection is significantly increased. Results of previous studies have shown that lower CD4 + T lymphocytes are associated with a higher risk of HR-HPV infection, and lower T and CD8 + T lymphocytes and higher NK lymphocytes are unfavorable factors for natural HPV clearance.19 In addition, Reeves et al proposed that CD8 + T lymphocytes can recognize the epitopes of E6/E7 oncogenes expressed by HPV and that persistent HPV infection may be related to the limited ability of CD8 + T lymphocytes to produce and present peptide epitopes derived from viral proteins20 The regression of cervical squamous intraepithelial lesions and the negative conversion of HPV are closely related to the presence of CD8 + T lymphocytes.21 NK cells have the ability to recognize and kill virus-infected and transformed cells.22 Previous studies reported that cervical tissues infected with HPV16 had more NK cell infiltration than those infected with HPV18.23 In addition, HPV can reduce NK cell cytotoxicity by reducing the expression of NKG2D ligands, which helps the virus to evade the surveillance of the host immune system and establish and maintain persistent infection.24 All of the above support the conclusions of this study. Notably, this study only detected peripheral blood immune cell subsets, and there may be differences between peripheral immune indicators and cervical local immune microenvironment, which is one of the limitations of this study.
Consistent with existing research evidence, this study found that the use of oral contraceptives and a higher number of sexual partners were associated with an increased risk of persistent HR-HPV infection. Oral contraceptives can alter the vaginal mucosal microenvironment by regulating estrogen levels, weakening the local defense barrier, and thus promoting viral colonization.25 On the other hand, multiple sexual partners increase the risk of co-infection with multiple HPV subtypes and the invasion of pathogenic bacteria, disrupting the vaginal microecological balance and reducing the body’s ability to clear the virus.
This study comprehensively analyzed the correlations between clinical characteristics, vaginal microecology, immune cells and the persistence of high-risk HPV infection, providing a multi-dimensional research perspective. Through regression analysis, independent risk factors were identified, enhancing the clinical relevance of the research results. However, this study still has limitations. Firstly, the sample size is relatively small, especially the number of persistent infection cases is limited, which may restrict the statistical power and generalizability of the results. Secondly, the detection of vaginal microecology and immune cells adopts traditional methods, lacking high-resolution data at the species level and subcellular level. Thirdly, potential confounding factors such as immune checkpoint expression and local immune microenvironment of the cervix were not evaluated.
Conclusions
In conclusion, this exploratory observational study shows that persistent HR-HPV infection is associated with vaginal microecological imbalance (manifested by poor cleanliness, elevated BV score, abnormal pH value, and increased levels of hydrogen peroxide and sialidase) and impaired cellular immune function (decreased CD4 and CD8+ T lymphocytes). Among them, the reduction of CD8+ T lymphocytes is an independent risk factor for persistent HR-HPV infection. These findings suggest that comprehensive assessment of vaginal microecological status and peripheral CD8+ T lymphocyte levels may help identify individuals at high risk of persistent HR-HPV infection, but the clinical application value needs to be verified by large-sample, multi-center prospective studies. Targeting the regulation of vaginal microecological balance and enhancing cellular immune function may be potential strategies for preventing persistent HR-HPV infection, but intervention studies are needed to confirm its efficacy.
Future studies should expand the sample size, conduct long-term longitudinal follow-up, and verify the causal relationship between the identified factors and persistent HR-HPV infection; use metagenomic sequencing and flow cytometry to clarify the species-specific changes in vaginal microbiota and the detailed alterations in immune cell subsets. In addition, intervention studies are needed to evaluate the efficacy of microecological targeted therapy and immune enhancement therapy in improving the clearance rate of HR-HPV.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The Ethics Committee of Mindong Hospital in Ningde City approved this study (Ethics No.2021081306H). This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
MeiXiu Huang and Huifang Lei contributed equally to this paper and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Fujian Province (grant no. 2022J011519).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rebecca LS, Angela NG, Ahmedin J. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1). doi:10.3322/caac.21820
2. Shiming H, Qingfei M, Huihui S, et al. Human papillomavirus type 16E6promotes cervical cancer proliferation by upregulating transketolase enzymatic activity through the activation of protein kinase B. Mol Carcinog. 2023;63(2). doi:10.1002/mc.23656
3. Binhua D, Yuxuan H, Hongning C, et al. Prevotella as the hub of the cervicovaginal microbiota affects the occurrence of persistent human papillomavirus infection and cervical lesions in women of childbearing age via host NF-κB/C-myc. J Med Virol. 2022;94(11). doi:10.1002/jmv.28001
4. Wenyu L, Qiaoyu Z, Yaojia C, et al. Changes of the vaginal microbiota in HPV infection and cervical intraepithelial neoplasia: a cross-sectional analysis. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-06731-5
5. Irina Livia S, Anca B, Alina F, Ciprian Gavrila I, Demetra Gabriela S. Exploring microbiota diversity in cervical lesion progression and HPV infection through 16S rrna gene metagenomic sequencing. J Clin Med. 2023;12(15). doi:10.3390/jcm12154979
6. Cristina Paula C, Mayara Luciana S, Rafaella Almeida Lima N, Noely Paula Cristina L, Lara T. Microbiome and cervical cancer. Pathobiology. 2020;88(2). doi:10.1159/000511477
7. Kyrgiou M, Moscicki A. Vaginal microbiome and cervical cancer. Semi Cancer Biol. 2022;86:189–16. doi:10.1016/j.semcancer.2022.03.005
8. van Teijlingen N, Helgers L, Zijlstra-Willems E, et al. Vaginal dysbiosis associated-bacteria Megasphaera elsdenii and Prevotella timonensis induce immune activation via dendritic cells. J Reprod Immunol. 2020;138:103085. doi:10.1016/j.jri.2020.103085
9. Tiezzi DG, Andrade JM, Noushmehr H, Carlotti Júnior CG, Tirapelli DP. Integrated genomic and molecular characterization of cervical cancer. Nature. 2017;543(7645). doi:10.1038/nature21386
10. Barros MR Jr, de Melo CM, Barros ML, et al. Activities of stromal and immune cells in HPV-related cancers. J Exp Clin Cancer Res. 2018;37(1). doi:10.1186/s13046-018-0802-7
11. Bing B, Gulixian T, Awahan T, Rexianguli M, Yuping S, Azierguli A. Analysis of vaginal flora diversity and study on the role of Porphyromonas asaccharolytica in promoting IL-1β in regulating cervical cancer. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-73146-9
12. Jesper B, Fabio B, Anna DI, et al. Human papillomavirus same genotype persistence and risk: a systematic review. J Low Genit Tract Dis. 2020;25(1). doi:10.1097/lgt.0000000000000573
13. Unnop J, Xavier C, Suzanne MG, et al. Natural history of progression of HPV infection to cervical lesion or clearance: analysis of the control arm of the large, randomised PATRICIA study. PLoS One. 2013;8(11). doi:10.1371/journal.pone.0079260
14. Yiheng Y, Jufan Z, Renqian F, Mengfei H, Fenghua C, Yan H. Altered vaginal cervical microbiota diversity contributes to HPV-induced cervical cancer via inflammation regulation. PeerJ. 2024;12. doi:10.7717/peerj.17415
15. Cindy C, Alda Pereira DS, Andreia M, et al. Association of myeloperoxidase polymorphism (G463A) with cervix cancer. Mol Cell Biochem. 2015;404. doi:10.1007/s11010-015-2359-5
16. Gootenberg DB, Mitchell CM, Kwon DS. Cervicovaginal microbiota and reproductive health: the virtue of simplicity. Cell Host Microbe. 2018;23(2). doi:10.1016/j.chom.2018.01.013
17. David HM, Jeanne MM. The vaginal microbiome: current understanding and future directions. J Infect Dis. 2016. doi:10.1093/infdis/jiw184
18. Briselden AM, Moncla BJ, Stevens CE, Hillier SL. Sialidases (neuraminidases) in bacterial vaginosis and bacterial vaginosis-associated microflora. J Clin Microbiol. 1992;30(3). doi:10.1128/jcm.30.3.663-666.1992
19. Ye L, Yebin F, Yanlin C, et al. Peripheral blood lymphocytes influence human papillomavirus infection and clearance: a retrospective cohort study. Virol J. 2023;20(1). doi:10.1186/s12985-023-02039-6
20. Emma R, Oliver W, Christian HO, et al. HPV epitope processing differences correlate with ERAP1 allotype and extent of CD8(+) T-cell tumor infiltration in OPSCC. Cancer Immunol Res. 2019;7(7). doi:10.1158/2326-6066.Cir-18-0498
21. W YL, S J, D I, et al. Characterising the local immune responses in cervical intraepithelial neoplasia: a cross-sectional and longitudinal analysis. BJOG. 2008;115(13). doi:10.1111/j.1471-0528.2008.01936.x
22. Shiyuan H, Laimonis AL. Manipulation of the innate immune response by human papillomaviruses. Virus Res. 2016;231. doi:10.1016/j.virusres.2016.11.004
23. Adriana G-H, Isabel S-C. NK Cell Regulation in Cervical Cancer and Strategies for Immunotherapy. Cells. 2021;10(11). doi:10.3390/cells10113104
24. Jimenez-Perez MI, Jave-Suarez LF, Ortiz-Lazareno PC, et al. Cervical cancer cell lines expressing NKG2D-ligands are able to down-modulate the NKG2D receptor on NKL cells with functional implications. BMC Immunol. 2012;13. doi:10.1186/1471-2172-13-7
25. Farah F, Fatemeh D, Marzieh M, Maryam Sadat H, Amir S. Long-term oral contraceptive use as a risk factor for high-grade cervical lesions in women with high-risk human papillomavirus: a retrospective cohort analysis. Int J Gynecol Cancer. 2025;35(11). doi:10.1016/j.ijgc.2025.102650
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.