Back to Journals » Clinical Optometry » Volume 14
Daily Variations of Corneal White-to-White Diameter Measured with Different Methods
Authors Bandlitz S ![]() , Nakhoul M, Kotliar K
, Nakhoul M, Kotliar K ![]()
Received 31 January 2022
Accepted for publication 8 July 2022
Published 20 September 2022 Volume 2022:14 Pages 173—181
DOI https://doi.org/10.2147/OPTO.S360651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Stefan Bandlitz,1,2 Makram Nakhoul,3 Konstantin Kotliar3
1Höhere Fachschule für Augenoptik Köln (HFAK), Cologne School of Optometry, Cologne, Germany; 2School of Life and Health Sciences, Aston University, Birmingham, UK; 3Department of Medical Engineering and Technomathematics, FH Aachen University of Applied Sciences, Campus Jülich, Jülich, 52428, Germany
Correspondence: Konstantin Kotliar, Department of Medical Engineering and Technomathematics, FH Aachen University of Applied Sciences, Campus Jülich, Heinrich-Mussmann-Str. 1, Jülich, 52428, Germany, Tel +49 241 6009-53812, Fax +49 241 6009-53222, Email [email protected]
Purpose: A precise determination of the corneal diameter is essential for the diagnosis of various ocular diseases, cataract and refractive surgery as well as for the selection and fitting of contact lenses. The aim of this study was to investigate the agreement between two automatic and one manual method for corneal diameter determination and to evaluate possible diurnal variations in corneal diameter.
Patients and Methods: Horizontal white-to-white corneal diameter of 20 volunteers was measured at three different fixed times of a day with three methods: Scheimpflug method (Pentacam HR, Oculus), placido based topography (Keratograph 5M, Oculus) and manual method using an image analysis software at a slitlamp (BQ900, Haag-Streit).
Results: The two-factorial analysis of variance could not show a significant effect of the different instruments (p = 0.117), the different time points (p = 0.506) and the interaction between instrument and time point (p = 0.182). Very good repeatability (intraclass correlation coefficient ICC, quartile coefficient of dispersion QCD) was found for all three devices. However, manual slitlamp measurements showed a higher QCD than the automatic measurements with the Keratograph 5M and the Pentacam HR at all measurement times.
Conclusion: The manual and automated methods used in the study to determine corneal diameter showed good agreement and repeatability. No significant diurnal variations of corneal diameter were observed during the period of time studied.
Keywords: corneal diameter, white-to-white, diurnal variation, Scheimpflug imaging, placido based topography, slitlamp
Introduction
A precise determination of the corneal diameter is essential for the diagnosis of various ocular diseases, cataract and refractive surgery as well as for the selection and fitting of contact lenses.1–3 In addition to the measurement of the diameter of the visible corneal area from limbus to limbus (white-to-white, WTW) further measuring distances are proposed (Figure 1), especially for the determination of the size of intraocular anterior and posterior chamber lenses. These include the measurement of the topographic transition from the sclera and the cornea, from ciliary sulcus on one side to ciliary sulcus on the opposite side (sulcus-to-sulcus), from scleral spur to scleral spur or from anterior chamber angle to anterior chamber angle (angle-to-angle).4–10
 |
Figure 1 Possible reference points when determining diameters of the cornea and anterior chamber. |
Invasive and non-invasive methods are available to determine WTW diameter of the cornea. Classically, the WTW distance is measured with a calliper gauge, the Castroviejo-Calliper, under local anesthesia.11 However, there are currently numerous non-contact methods that allow the corneal diameter to be determined non-invasively. These include manual methods such as Holladay-Godwin gauge, the reticule or image analysis system at the slitlamp as well as automated methods using Scheimpflug imaging, placido-based topography, optical coherence tomography or Fourier-based profilometry.1,2,12–18
A physiological swelling of the cornea leads to fluctuations in its thickness and its topography. For instance, the physiological nocturnal corneal edema results in small but significant diurnal changes in corneal thickness and shape.19 Diurnal variations in axial eye length, intraocular pressure (IOP), anterior chamber depth, choroidal and retinal thickness were also reported.20–22 It is therefore conceivable that most of anatomical and physiological parameters of the human eye show diurnal variations. To what extent also the corneal diameter is subject to a diurnal rhythm, and to what extent these possible corneal diameter variations can be assessed using modern in vivo measurement methods has not been reported so far.
The objectives of this study were to investigate the agreement between two automatic and one manual method for corneal diameter determination and to evaluate possible diurnal variations in corneal diameter.
Materials and Methods
Participants
A total of 20 participants (age 26.5 (25.0–29.0) years [median (1st quartile – 3rd quartile)]; 12 female, 8 male) of the Höhere Fachschule für Augenoptik Köln (Cologne School of Optometry) were recruited as volunteers for this study. Excluded were volunteers with corneal diseases such as keratoconus, with corneal scars, pannus, ulcers, erosions, as well as patients after ophthalmic surgery including corneal refractive surgery. The test persons were not allowed to wear contact lenses for at least 24 hours before the examination.
This study was conducted in compliance of principles of good ethical research and in accordance with the requirements of the Declaration of Helsinki (2013) as part of a bachelor thesis under supervision in the FH Aachen. In the study, only CE-certified commercially available non-invasive medical diagnostic devices were used. All the ethical issues of the study were thoroughly controlled and approved by the supervisors. Such bachelor projects do not require formal approval by local ethics committee in the FH Aachen. All participants were thoroughly consulted on the objectives as well as on content of the study and gave written informed consent prior to study commencement. Every participant has given consent to participate as well as consent to publish the data. Patient data were used only in anonymized form.
Procedures
The horizontal white-to-white diameter of the cornea of each right eye was measured at three different times of a day (8 a.m., 11 a.m. and 2 p.m.) with two automated methods: Scheimpflug method (Pentacam HR, Oculus, Wetzlar, Germany) and placido based topography (Keratograph 5M, Oculus, Wetzlar, Germany), as well as semi-automatically using image analysis software at the slitlamp (BQ900 with IM900 Digital Imaging Module, Haag-Streit, Koeniz, Switzerland). Study participants were asked to look straight ahead during the measurement. In order to ensure stability of the tear film, the subjects blinked before the measuring exposure and stopped blinking during the exposure. In the experimental design, the order of measuring stations was randomized. An interval of 5 minutes between each measuring station was set. All measurements were performed by one examiner (MN). Each individual measurement on an instrument was performed three times. The ensuing measurement result was calculated as the statistical median of these three measurements.
Instruments
Pentacam HR
The Pentacam HR uses a rotating Scheimpflug camera (180°) and a monochromatic slit light source (blue light emitting diode at 470 nm), both rotating together around the optical axis in order to create a three-dimensional image of the anterior segment of the eye.23 Within 2 seconds, 50 images with a maximum of 138,000 measured points are taken.12 The Pentacam HR is equipped with an iris camera that automatically calculates the horizontal WTW diameter from the iris photo.
Keratograph 5M
The Keratograph 5M is a placido-based corneal topographer that can also be used for fluid image simulation during contact lens fitting, analysis of the tear film, meibography and determination of the degree of conjunctival redness.24 In addition to manual measuring option with a ruler on the screen, this system also includes an option for automatic measurement of the horizontal WTW diameter. In the present study, the values of the automatic measurements were evaluated.
Haag-Streit LED Slitlamp with Imaging Module
The Haag-Streit BQ 900 is a slitlamp with LED (light emitting diode) light source. The corneal images acquired with diffuse illumination and 10x magnification were stored and then evaluated in the Imaging Module (IM 900). The manually drawn horizontal WTW distance was first specified in pixels and then converted to millimetres. Pixel to mm ratio was calibrated by the help of a stored image of a graticule in advance.
Statistical Analyses
The data was primarily analysed using non-parametric statistical methods. Differences between the measurement series were examined with Friedman test and, if applicable, pairwise using Wilcoxon signed rank test corrected to multiple comparisons according to Holm-Bonferroni. For statistical comparison of independent samples, Mann–Whitney-U-test was applied. The association between the measured values obtained with the different instruments was investigated using Spearman correlation. The agreement of the measurement methods was checked using Bland-Altman plots. The intra-class correlation coefficient (ICC) and the non-parametric coefficient of variation (CV): quartile coefficient of dispersion (QCD), were calculated to determine the repeatability of each measurement method. A p-value <0.05 was assumed to be statistically significant.
For further statistical analysis, the data was examined for normal distribution using the Shapiro–Wilk test. Since there was no significant difference from normal distribution, a two-way repeated measures ANOVA (analysis of variance) was performed to verify the measurement differences between the tested devices at the different measurement points. Statistical analysis of the data was performed with SigmaPlot 12 (Systat Software Inc., Chicago, USA) and SPSS-25 (SPSS Inc., Chicago, USA).
Results
The descriptive data of the corneal diameters measured with the different instruments at different points in time are shown in Table 1. The two-factorial analysis of variance could not show a significant effect of the different instruments (p = 0.117), the different time points (p = 0.506) and the interaction between instrument and time point (p = 0.182) (Figure 2).
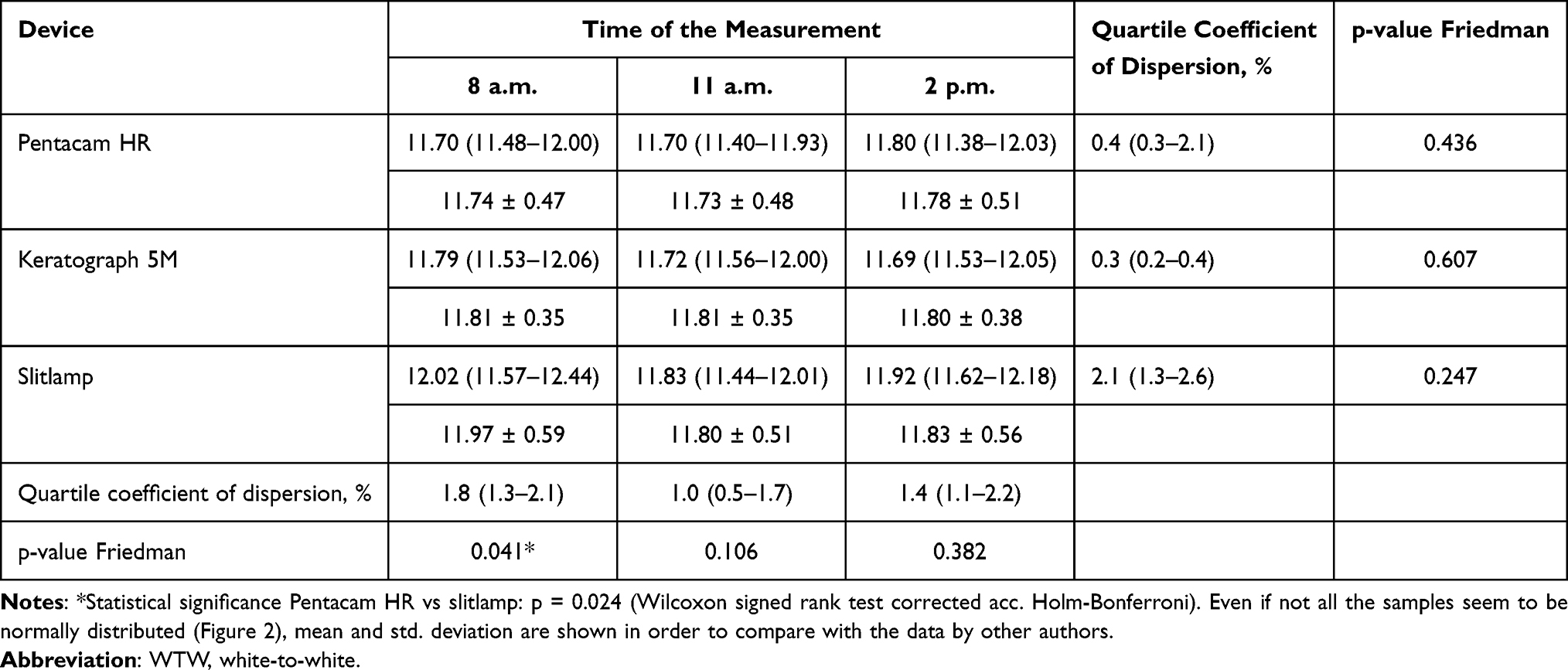 |
Table 1 Descriptive Data of the Average Values of Three WTW Corneal Diameter Measurements at Each Time Point Assessed in mm with Three Different Methods: Median (1st Quartile – 3rd Quartile), Mean ± Std. Deviation, n = 20 |
 |
Figure 2 Boxplots for the horizontal white-to-white corneal diameter values measured with the three different methods at the three different measuring times (n = 20). |
Moreover, there were no significant differences in the corneal diameters measured in male and female with different devices: Keratograph 5M: p = 0.427; Pentacam HR: p = 0.473; slitlamp: p = 0.970 (Mann–Whitney-U-test).
The results showed a very strong correlation of the automatically measured WTW values of the Keratograph 5M and the Pentacam HR (Spearman’s ρ = 0.828; p < 0.001). Additionally, strong correlations between manual measurement with the slitlamp and the automatically measured values of the Keratograph 5M (ρ = 0.767; p < 0.001) as well as of the Pentacam HR (ρ = 0.707; p < 0.001) were shown.
Bland-Altman plots show good agreement between the measurements with different devices (Figure 3). On average, the values measured manually with the slitlamp were higher than the automatically determined values of the Pentacam HR [median (1st quartile – 3rd quartile)]: 0.12 (−0.05–0.35) mm (mean: +0.13 mm; 95% confidence interval: −0.02–0.23 mm) and the Keratograph 5M: 0.07 (−0.13–0.31) mm (mean: +0.06; 95% CI: −0.65–0.77 mm). While the discrepancy between the measurements with slitlamp and Keratograph 5M was not significant (p = 0.15), the difference between the slitlamp and Pentacam results was statistically significant (Wilcoxon signed rank test; p = 0.01 after correction to multiple comparisons). There were no significant differences between the automatically measured values of the Keratograph 5M and the Pentacam HR: 0.03 (−0.09–0.23) mm (mean: 0.05; 95% CI: −0.10–0.12 mm; p = 0.125).
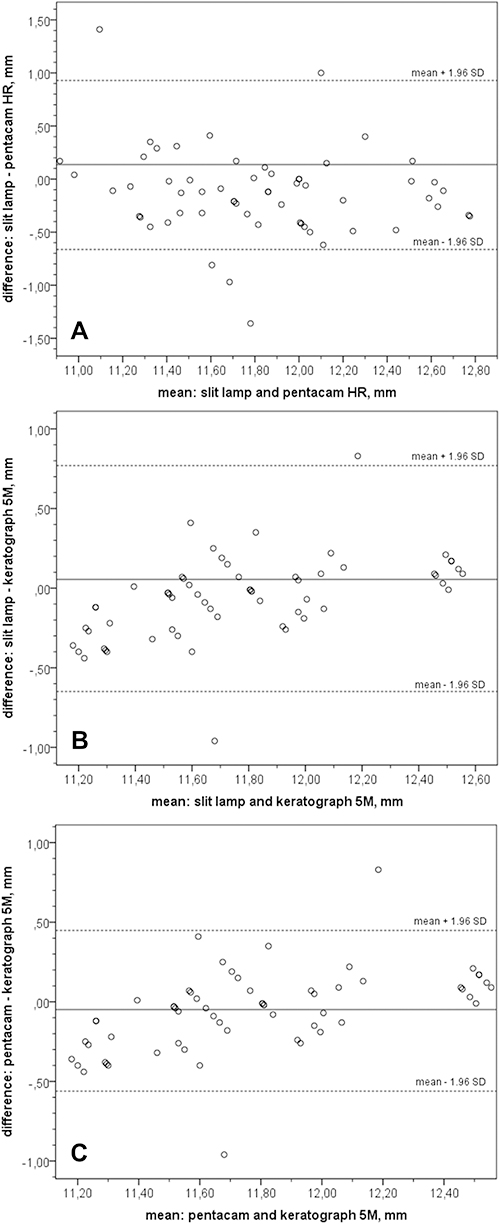 |
Figure 3 Bland Altman plots to describe the agreement between the measurements with the different devices (n = 20): (A) between slitlamp and Pentacam HR; (B) between slitlamp and Keratograph 5M; (C) between Pentacam HR and Keratograph 5M. |
The absolute differences between the measurements with different devices amounted to: Pentacam HR vs slitlamp: 0.24 (0.11–0.41) mm; Keratograph 5M vs slitlamp: 0.28 (0.08–0.41) and Pentacam HR vs Keratograph 5M: 0.13 (0.07–0.26) mm.
Very good repeatability (ICC, QCD) was found for all three devices used (Table 2). However, manual slitlamp measurements showed a higher quartile coefficient of dispersion than the automatic measurements with the Keratograph 5M and the Pentacam HR at all measurement times. Here, the differences of slitlamp measurements’ variability vs. those of Pentacam HR were statistically significant (p < 0.05).
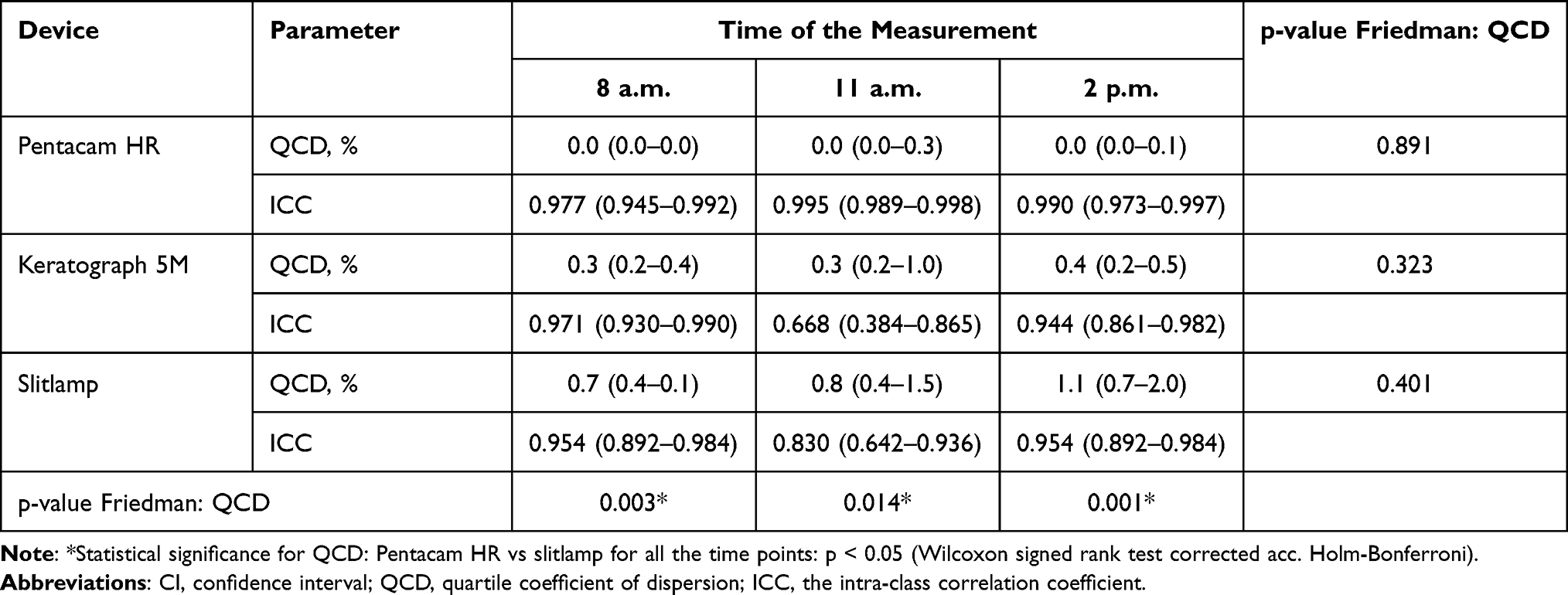 |
Table 2 Repeatability of the Three Measurement Methods Described by the Non-Parametric Coefficient of Variation, QCD and the Intra-Class Correlation Coefficient (ICC): Median (1st Quartile – 3rd Quartile) for QCD and Mean (95% CI) for ICC, n = 20. Three Measurements Were Performed at Each Time Point with Each Device. Their Average Values are Shown in Table 1 |
Average values of further corneal biometric parameters measured in the study are represented in Table 3. While the central corneal radius (CCR) did not change significantly to different measurement sessions, central corneal thickness (CCT) was significantly reduced to the afternoon session compared to both morning sessions (p < 0.05).
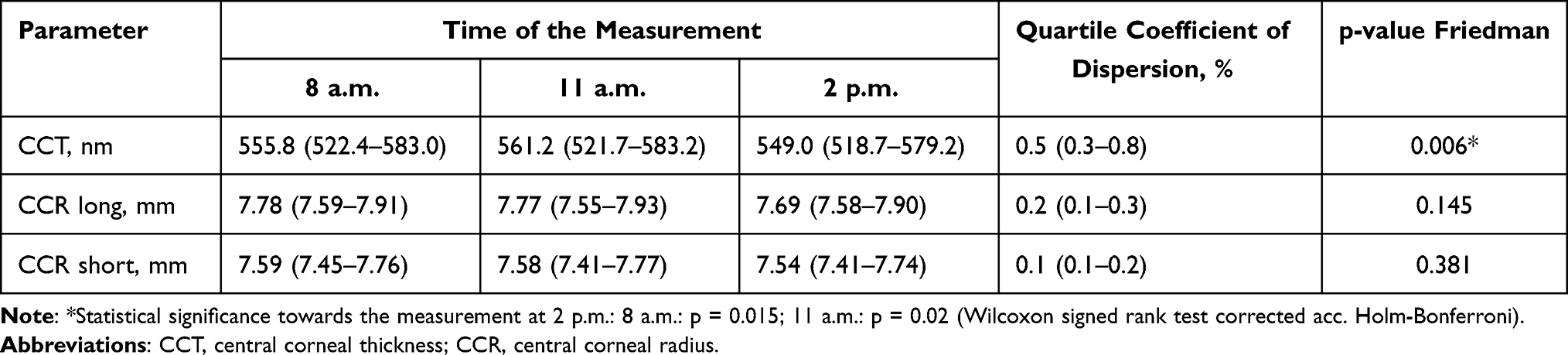 |
Table 3 Descriptive Data of the Average Values (Statistical Median) of Further Corneal Biometric Parameters Measured in the Study: Median (1st Quartile – 3rd Quartile), n = 20 |
Corneal WTW diameters measured with Pentacam HR, Keratograph 5M and slitlamp show no correlation to CCT and a significant moderate to weak correlation to CCR parameters: CCR long: Spearman’s ρ = 0.434; 0.458, p < 0.001 and 0.336, p = 0.009 correspondingly; CCR short: ρ = 0.409; 0.416, p < 0.001 and 0.274, p = 0.034 correspondingly.
Discussion
One aim of the present study was to investigate the agreement between two automatic and one manual method for determining corneal WTW diameter. Millimetre rulers, measuring eyepieces, diameter gauges, callipers, and manual distance determination with a digital ruler on images belong to manual methods for determining the visible WTW diameter.6 Here, active participation of the observer is required to decide where the cornea begins and ends. In the automatic determination of WTW diameter, the measuring instruments recognize the corneal-limbus transition by comparing grayscales and calculate the diameter from this.13
The values of the corneal diameter (11.75 ± 0.48 mm) measured automatically with the Scheimpflug camera (Pentacam HR) in this study are in a good agreement with previous reports on healthy eyes by Domínguez-Vicent et al12 (11.75 ± 0.40 mm), Salouti et al23 (11.76 ± 0.38 mm) and Shajari et al15 (11.8 ± 0.4 mm) in which the horizontal WTW diameter was also determined with the Pentacam HR.
Ortiz-Toquero et al25 used a placido-based corneal topographer and found an automatically measured horizontal WTW diameter of 11.82 ± 0.49 mm in healthy eyes and 11.76 ± 0.48 mm in eyes with keratoconus. However, the difference between healthy eyes and eyes with keratoconus was not statistically significant (p = 0.45). The present values (11.81 ± 0.34) measured with the Keratograph 5M in healthy eyes are also in a good agreement with the literature.25
Pinero et al6 reported WTW diameters of 12.25 ± 0.49 mm being manually measured with a digital ruler on the camera images of a topographer (CSO Topographer). They concluded that manual measurement with a digital ruler on the topographer images was sometimes difficult because in some cases it was hard to define the end and the beginning of the cornea accurately. In addition, the images used were focused on the corneal centre and not on the limbus, which, according to the authors, made it difficult to recognize the corneal borders. In this study, the focus of high-resolution slitlamp images was placed on the limbus. During the subsequent manual measurement with the digital ruler, slightly larger diameters were determined on average. However, there was no statistically significant difference between the two automatic measurement methods.
In this pilot study only 20 healthy volunteers were examined. Statistically speaking, the statistical tests used, which did not show differences in the measurement parameters either at different measurement times or with different devices, have relatively low sensitivity (power). At a fixed significance level of α = 0.05, for example, the power to find a difference of 0.05 mm with a standard deviation of 0.5 mm, N = 20, and 3 measurement times (Table 1: Pentacam) was less than 0.1. To detect a difference of 0.1 mm at a standard deviation of 0.4 mm in a paired comparison of the measurements of two measuring devices (eg, Keratograph vs Pentacam, Table 1), at least 260 test persons would have been required. Nevertheless, the temporal and device-specific differences in corneal diameter measured in the study are very small. The magnitude of these differences corresponds to the reproducibility of the respective devices and is neither clinically nor physiologically nor application-related relevant in the clinical practice of optometrists (eg, contact lens fitting).
The visible WTW corneal diameter does not necessarily correspond to the corneoscleral topographic transition. In their measurements with the Eye Surface Profiler, Consejo et al4 reported a diameter of the topographic limbus that was in average 0.33 ± 0.24 mm larger than the WTW diameter. Also, the diameters measured from anterior chamber angle to anterior chamber angle and ciliary sulcus to ciliary sulcus appear to be larger than the WTW diameter of the cornea.8 This finding is important for reliable sizing of intraocular lenses.
Both automatic and manual methods showed a very good repeatability (ICC). Kawamorita et al8 also showed very good repeatability for the Orbscan system based on slitlamp technology and placido disks in the measurement of the WTW diameter (ICC = 0.984) as well as in the determination of the angle-to-angle (ICC = 0.938) and sulcus-to-sulcus (ICC = 0.976) diameters. Venkataraman et al16 found an ICC value of 0.89 for the automatic measurement with the Orbscan, while the manual measurement with a digital ruler on the Orbscan images showed an ICC value of 0.940. This value was comparable to the ICC value found in this study for the manual measurement at the slitlamp. For the repeatability of the WTW diameter measured with the Keratograph, Ortiz-Toquero et al25 reported an ICC value of 0.990 and a coefficient of variation value of 0.33%. These values are also in a very good agreement with the repeatability values of ICC = 0.990 and CV = 0.37 ± 0.28% for the Keratograph determined in our study. For the Cassini topography system based on colour LEDs, Pinero et al26 found an ICC of 0.997 for WTW diameter determination in a recently published study.
The knowledge of the natural diurnal variations of the different corneal parameters is relevant for clinical practice as well as for the eye research. The selection of an appropriate contact lens diameter and intraocular lens sizing is based on the corneal WTW diameter determination. Furthermore, the measurement of corneal diameter is relevant in the diagnosis of congenital glaucoma, where an increased corneal diameter is present.27
The anterior corneal surface shows a flattening in the time after waking up in the morning, while the posterior surface shows a slight steepening and a change in astigmatism.19 This change correlates with a simultaneous increase in corneal thickness, which is more pronounced in the periphery of the cornea than in its center.19 A study by Read et al19 showed mean amplitudes of change over a 24-hour period of 0.019±0.008 mm for central and 0.022±0.008 mm for peripheral corneal thickness, 0.36±0.11 D for anterior corneal surface and 0.05±0.03 D for posterior corneal surface. Du Toit et al28 reported that the mean corneal swelling on opening the eyes was 2.9±0.3%, but there were significant individual variations ranging from 1.3% to 7.2%. It is also assumed that the variability of corneal thickness is due to changes in eyelid blink, tear film production, tear film evaporation, and IOP in addition to night-time corneal swelling.28,29
During the course of the day, the radii of the corneal anterior surface seem to become slightly steeper while the cornea becomes thinner.30,31 These variations in corneal radius and thickness are associated with night-time corneal swelling and occur most significantly between morning and midday measurements.32 The measurement of the corneal diameter in a period from 8 a.m. to 2 p.m. showed no significant changes in the present study. Read et al hypothesized that the nocturnal swelling of the cornea leads to a backward movement of the posterior cornea towards the anterior chamber and a slight forward movement of the anterior cornea, which is accompanied by an increase in corneal thickness and a decrease in anterior chamber depth observed upon awakening.19 However, these assumed axial positional changes seem to have no influence on the corneal diameter.
Conclusions
The manual and automated methods used in the study to determine corneal diameter showed good agreement and repeatability. No significant diurnal variations of corneal diameter were observed during the period of time studied.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen Y, Xia X. Comparison of the Orbscan II topographer and the iTrace aberrometer for the measurements of keratometry and corneal diameter in myopic patients. BMC Ophthalmol. 2016;16:33. doi:10.1186/s12886-016-0210-8
2. Salouti R, Nowroozzadeh MH, Tajbakhsh Z, et al. Agreement of corneal diameter measurements obtained by a swept-source biometer and a scheimpflug-based topographer. Cornea. 2017;36(11):1373–1376. doi:10.1097/ICO.0000000000001300
3. Bergmanson JP, Martinez JG. Size does matter: what is the corneo-limbal diameter? Clin Exp Optom. 2017;100(5):522–528. doi:10.1111/cxo.12583
4. Consejo A, Llorens-Quintana C, Radhakrishnan H, Iskander DR. Mean shape of the human limbus. J Cataract Refract Surg. 2017;43(5):667–672. doi:10.1016/j.jcrs.2017.02.027
5. Nemeth G, Hassan Z, Szalai E, Berta A, Modis L. Comparative analysis of white-to-white and angle-to-angle distance measurements with partial coherence interferometry and optical coherence tomography. J Cataract Refract Surg. 2010;36(11):1862–1866. doi:10.1016/j.jcrs.2010.05.017
6. Pinero DP, Plaza Puche AB, Alio JL. Corneal diameter measurements by corneal topography and angle-to-angle measurements by optical coherence tomography: evaluation of equivalence. J Cataract Refract Surg. 2008;34(1):126–131. doi:10.1016/j.jcrs.2007.10.010
7. Bruner C, Skanchy DF, Wooten JP, Chuang AZ, Kim G. Anterior chamber lens sizing: comparison of white-to-white and scleral spur-to-scleral spur methods. J Cataract Refract Surg. 2020;46(1):95–101. doi:10.1016/j.jcrs.2019.08.043
8. Kawamorita T, Uozato H, Kamiya K, Shimizu K. Relationship between ciliary sulcus diameter and anterior chamber diameter and corneal diameter. J Cataract Refract Surg. 2010;36(4):617–624. doi:10.1016/j.jcrs.2009.11.017
9. Ghoreishi M, Abdi-Shahshahani M, Peyman A, Pourazizi M. A model for predicting sulcus-to-sulcus diameter in posterior chamber phakic intraocular lens candidates: correlation between ocular biometric parameters. Int Ophthalmol. 2019;39(3):661–666. doi:10.1007/s10792-018-0859-5
10. Nakhoul M, Kotliar K, Bandlitz S. Untersuchung tageszeitlicher schwankungen des hornhautdurchmessers. DOZ. 2020;10:88–94.
11. Jose RM, Roy DK. Castroviejo caliper: a useful tool in plastic surgery. Plast Reconstr Surg. 2004;114(4):1006. doi:10.1097/01.PRS.0000138699.78046.22
12. Dominguez-Vicent A, Perez-Vives C, Ferrer-Blasco T, Albarran-Diego C, Montes-Mico R. Interchangeability among five devices that measure anterior eye distances. Clin Exp Optom. 2015;98(3):254–262. doi:10.1111/cxo.12247
13. Baumeister M, Terzi E, Ekici Y, Kohnen T. Comparison of manual and automated methods to determine horizontal corneal diameter. J Cataract Refract Surg. 2004;30(2):374–380. doi:10.1016/j.jcrs.2003.06.004
14. Rufer F, Schroder A, Erb C. White-to-white corneal diameter: normal values in healthy humans obtained with the Orbscan II topography system. Cornea. 2005;24(3):259–261. doi:10.1097/01.ico.0000148312.01805.53
15. Shajari M, Lehmann UC, Kohnen T. Comparison of corneal diameter and anterior chamber depth measurements using 4 different devices. Cornea. 2016;35(6):838–842. doi:10.1097/ICO.0000000000000840
16. Venkataraman A, Mardi SK, Pillai S. Comparison of Eyemetrics and Orbscan automated method to determine horizontal corneal diameter. Indian J Ophthalmol. 2010;58(3):219–222. doi:10.4103/0301-4738.62647
17. Ferrer-Blasco T, Esteve-Taboada JJ, Martinez-Albert N, Alfonso JF, Montes-Mico R. Agreement of white-to-white measurements with the IOLMaster 700, Atlas 9000, and Sirius systems. Expert Rev Med Devices. 2018;15(6):453–459. doi:10.1080/17434440.2018.1481745
18. Jesus DA, Kedzia R, Iskander DR. Precise measurement of scleral radius using anterior eye profilometry. Cont Lens Anterior Eye. 2017;40(1):47–52. doi:10.1016/j.clae.2016.11.003
19. Read SA, Collins MJ. Diurnal variation of corneal shape and thickness. Optom Vis Sci. 2009;86(3):170–180. doi:10.1097/OPX.0b013e3181981b7e
20. Chakraborty R, Read SA, Collins MJ. Diurnal variations in axial length, choroidal thickness, intraocular pressure, and ocular biometrics. Invest Ophthalmol Vis Sci. 2011;52(8):5121–5129. doi:10.1167/iovs.11-7364
21. Read SA, Collins MJ, Iskander DR. Diurnal variation of axial length, intraocular pressure, and anterior eye biometrics. Invest Ophthalmol Vis Sci. 2008;49(7):2911–2918. doi:10.1167/iovs.08-1833
22. Burfield HJ, Patel NB, Ostrin LA. Ocular biometric diurnal rhythms in emmetropic and myopic adults. Invest Ophthalmol Vis Sci. 2018;59(12):5176–5187. doi:10.1167/iovs.18-25389
23. Salouti R, Nowroozzadeh MH, Zamani M, Ghoreyshi M, Khodaman AR. Comparison of Horizontal corneal diameter measurements using the Orbscan IIz and Pentacam HR systems. Cornea. 2013;32(11):1460–1464. doi:10.1097/ICO.0b013e3182a40786
24. Fernandez J, Rodriguez-Vallejo M, Martinez J, Tauste A, Hueso E, Pinero DP. Confounding sizing in posterior chamber phakic lens selection due to white-to-white measurement bias. Indian J Ophthalmol. 2019;67(3):344–349. doi:10.4103/ijo.IJO_613_18
25. Ortiz-Toquero S, Zuniga V, Rodriguez G, de Juan V, Martin R. Agreement of corneal measurements between dual rotating Scheimpflug-Placido system and Placido-based topography device in normal and keratoconus eyes. J Cataract Refract Surg. 2016;42(8):1198–1206. doi:10.1016/j.jcrs.2016.04.033
26. Pinero DP, Molina-Martin A, Camps VJ, de Fez D, Caballero MT. Validation of corneal topographic and aberrometric measurements obtained by color light-emitting diode reflection topography in healthy eyes. Graefes Arch Clin Exp Ophthalmol. 2019;257(11):2437–2447. doi:10.1007/s00417-019-04453-5
27. Henriques MJ, Vessani RM, Reis FA, de Almeida GV, Betinjane AJ, Susanna R. Corneal thickness in congenital glaucoma. J Glaucoma. 2004;13:185–188. doi:10.1097/00061198-200406000-00002
28. Du Toit R, Vega JA, Fonn D, Simpson T. Diurnal variation of corneal sensitivity and thickness. Cornea. 2003;22(3):205–209. doi:10.1097/00003226-200304000-00004
29. Odenthal MT, Nieuwendaal CP, Venema HW, Oosting J, Kok JH, Kijlstra A. In vivo human corneal hydration control dynamics: a new model. Invest Ophthalmol Vis Sci. 1999;40(2):312–319.
30. Kiely PM, Carney LG, Smith G. Diurnal variations of corneal topography and thickness. Am J Optom Physiol Opt. 1982;59(12):976–982. doi:10.1097/00006324-198212000-00007
31. Handa T, Mukuno K, Niida T, Uozato H, Tanaka S, Shimizu K. Diurnal variation of human corneal curvature in young adults. J Refract Surg. 2002;18(1):58–62. doi:10.3928/1081-597X-20020101-09
32. Read SA, Collins MJ, Carney LG. The diurnal variation of corneal topography and aberrations. Cornea. 2005;24(6):678–687. doi:10.1097/01.ico.0000154385.43732.6e
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.