Back to Journals » Research and Reports in Urology » Volume 6
Cystoscopic-assisted partial cystectomy: description of technique and results
Authors Gofrit O, Shapiro A, Katz R, Duvdevani M, Yutkin V, Landau EH, Zorn K, Hidas G, Pode D
Received 26 April 2014
Accepted for publication 4 June 2014
Published 24 October 2014 Volume 2014:6 Pages 139—143
DOI https://doi.org/10.2147/RRU.S66861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Ofer N Gofrit,1 Amos Shapiro,1 Ran Katz,1 Mordechai Duvdevani,1 Vladimir Yutkin,1 Ezekiel H Landau,1 Kevin C Zorn,2 Guy Hidas,1 Dov Pode1
1Department of Urology, Hadassah Hebrew University Hospital, Jerusalem, Israel; 2Department of Surgery, Section of Urology, Montreal, Canada
Background: Partial cystectomy provides oncological results comparable with those of radical cystectomy in selected patients with invasive bladder cancer without the morbidity associated with radical cystectomy and urinary diversion. We describe a novel technique of partial cystectomy that allows accurate identification of tumor margins while minimizing damage to the rest of the bladder.
Methods: During the study period, 30 patients underwent partial cystectomy for invasive high-grade cancer. In 19 patients, the traditional method of tumor identification was used, ie, identifying the tumor by palpation and cystotomy. In eleven patients, after mobilization of the bladder, flexible cystoscopy was done and the light of the cystoscope was pointed toward one edge of the planned resected ellipse around the tumor, thus avoiding cystotomy.
Results: Patients who underwent partial cystectomy using the novel method were similar in all characteristics to patients operated on using the traditional technique except for tumor diameter which was significantly larger in patients operated on using the novel method (4.3±1.5 cm versus 3.11±1.18 cm, P=0.032). Complications were rare in both types of surgery. The 5-year local recurrence-free survival was marginally superior using the novel method (0.8 versus 0.426, P=0.088). Overall, disease-specific and disease-free survival rates were similar.
Conclusion: The use of a flexible cystoscope during partial cystectomy is a simple, low-cost maneuver that assists in planning the bladder incision and minimizes injury to the remaining bladder by avoiding the midline cystotomy. Initial oncological results show a trend toward a lower rate of local recurrence compared with the standard method.
Keywords: bladder cancer, partial cystectomy, cystoscopic-assisted partial cystectomy
Introduction
Partial cystectomy has many theoretical advantages over radical cystectomy, in that it spares the bladder, obviates the need for urinary diversion, maintains erectile function, can be done under regional anesthesia, and is associated with lower morbidity and mortality. Ideal patients for such a procedure have a solitary muscle-invasive tumor that allows complete excision with adequate margins, with reasonable residual bladder volume, and a biopsy-proven absence of carcinoma in situ in the remaining bladder.1 However, using these criteria, only 5%–20% of patients presenting with muscle-invasive bladder cancer are suitable for this surgery, which is more commonly provided in rural, nonteaching hospitals.2,3 Therefore, the literature is limited to retrospective studies reporting 25, 58 and 37 patients.4–6 In appropriately selected patients from leading centers, the overall 5-year survival after partial cystectomy is in the order of 70% and disease-specific survival is around 85%.4–6 The overall oncological results obtained with partial cystectomy are not inferior to radical cystectomy, and approximately three quarters of patients retain a functional bladder.6–8
The classic technique of partial cystectomy involves “cystotomy away from the tumor”, identification of the tumor from the inside of the bladder, and en bloc removal of a full-thickness segment of the tumor-bearing bladder wall.2,9 Making a cystotomy away from the tumor requires either palpation of the tumoral mass or a “smart guess” based on previous knowledge of tumor location. In many cases, most of the tumor bulk has been removed by previous transurethral resection, making it impossible to palpate the tumor. Moreover, in elderly patients, the bladder wall is often thickened by the hypertrophied detrusor, making tumor palpation difficult. Alternatively, midline cystotomy is done and the tumor or its residual crater is identified from inside the bladder. This maneuver can compromise the surgical margins or even go through the tumor itself. Additionally, two suture lines are required for bladder closure.
We describe a simple, low-cost method, ie, cystoscopic-assisted partial cystectomy (CAPC), which requires only one incision in the bladder and can potentially provide optimal surgical margins. We compare the results of this method with the results of standard partial cystectomy.
Materials and methods
Study population
A prospectively maintained database holding data on 760 patients diagnosed with bladder cancer between June 1998 and December 2008 was surveyed. Pathological staging was performed according to the 1997 TNM (tumor, node, metastasis) system and grading according to the 1998 International Society of Urologic Pathologists consensus classification. Carcinoma in situ was not considered an absolute contraindication for partial cystectomy. The study was approved by the Helsinki institutional review board committee (approval number 207.08). A total of 30 patients (mean age 67.7±12.1 years), including 28 men and two women, underwent partial cystectomy for high-grade invasive cancer. Median postoperative follow-up was 43 months. Nineteen patients underwent a standard partial cystectomy with cystotomy “away from the tumor” for tumor identification.2,9 In eleven patients, a flexible cystoscope was used intraoperatively for identification of the tumor and for planning the incision in the bladder. All CAPC cases were performed by a single surgeon (ONG). Oncological results of the new technique were compared with the classic method.
Surgical technique
Under general or regional anesthesia, the abdomen and penis are scrubbed and draped. A catheter is inserted in the sterile field. Midline laparotomy is then performed. In most cases, this requires opening of the peritoneum. The transperitoneal approach permits wider excision of the bladder dome with its perivesical fat and the peritoneal covering. The bladder is then mobilized. The overhead operative lights are then turned off and the catheter is removed. Flexible cystoscopy is performed by the senior surgeon. The tumor or its crater are identified and the surgeon plans an elliptic incision around the tumor, thereby leaving 1–2 cm of normal bladder mucosa around it. The surgeon points the cystoscope toward one of the poles of the planned ellipse (Figure 1A). The assistant identifies the transillumination in the operative field and marks this point with a cautery. The cystoscope is removed and a catheter reinserted. The overhead lights are turned on, the bladder around the marked incision is packed with lap pads, and the mark is deepened to the mucosa. The bladder edge is lifted with Allis clamps and the tumor is identified (Figure 1B). The incision around the tumor is completed (Figure 1C and D). The specimen is submitted for frozen section examination to confirm the absence of microscopic disease at the margin. The bladder is then closed in the usual manner with two-layer closure and standard pelvic lymphadenectomy (including the external iliac and obturator nodes) is performed.
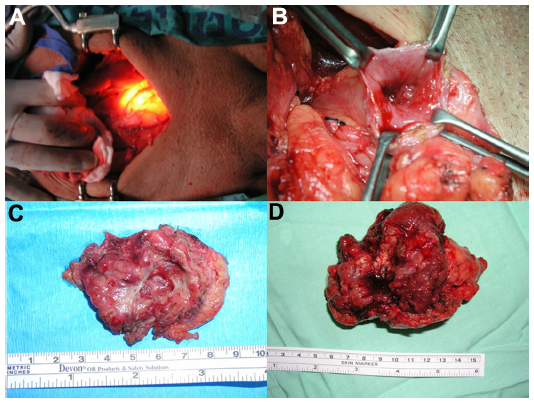 | Figure 1 (A) An intraoperative view. A midline lapartomy was performed and the bladder isolated. The lights in the operating room were turned off. The surgeon pointed the cystoscope toward one of the poles of the planned ellipse around the tumor. The assistant marks this point with a cautery. (B) The marked incision was deepened, the bladder edge lifted with Allis clamps, and the tumor identified. (C) A removed specimen showing only a crater. (D) A removed specimen showing a bulky (pT3) tumor. This patient was operated on at the age of 54 years and is disease-free 85 months after surgery. |
Postoperative management
Adjuvant therapy was given according to the final pathological result. Intravesical instillations of bacillus Calmette-Guerin were provided to patients with carcinoma in situ (induction of six instillations and maintenance of 2–3 instillations every 3 months for 1 year and then every 6 months for an additional 2 years). Systemic chemotherapy was considered in patients with pT3 or node-positive disease. The follow-up protocol included cystoscopy and urinary cytology every 3 months for 2 years and then every 6 months for an additional 3 years. Computed tomography was done every 6 months for 2 years and then annually for a further 3 years.
Statistical analysis
The preoperative and postoperative characteristics of the patients who underwent partial cystectomy using the two methods were compared, as were the oncological results. Continuous variables were compared using the Student’s t-test and categorical variables using Fisher’s Exact test. All statistical tests were two-tailed and a P-value <0.05 was considered to be statistically significant. Local recurrence-free survival, overall (local and systemic) recurrence-free survival, disease-specific survival, and overall mortality were analyzed using the Kaplan–Meier method.
Results
The characteristics of the patients who underwent standard partial cystectomy and CAPC are presented in Table 1. The groups were similar in age, preoperative and postoperative pathological stages, frequency of Tis, frequency of variant histology, positive surgical margin rate, ratio of “first-time bladder tumors”, and duration of follow-up. However, tumor diameter was significantly larger in patients operated on using CAPC (4.3±1.5 cm versus 3.11±1.18 cm, respectively, P=0.032). No patient had metastatic pelvic lymph nodes.
 | Table 1 Characteristics of patients who underwent partial cystectomy using traditional and novel methods |
Both types of surgery were tolerated well, with a low rate of complications. A total of three complications (15.7%) were recorded in the standard partial cystectomy group (two Clavien grade 2 and one Clavien grade 1) compared with the CAPC group, in which two complications were observed (one Clavien grade 2 and one Clavien grade 3b eventration).
The oncological results for the entire cohort are presented in Figure 2. The 5-year overall, disease-specific, and recurrence (local and systemic)-free survival rates were 55%, 67%, and 42%, respectively. Local (intravesical) recurrence was treated with repeated transurethral resection with or without adjuvant bacillus Calmette-Guerin (six patients in the standard partial cystectomy group and none in the CAPC group) or by radical cystectomy (one patient in each group). Systemic recurrence was treated by chemotherapy in three patients in the standard partial cystectomy group and by supportive care in a total of three patients. Table 2 compares the oncological results obtained using the traditional and novel methods. Overall, disease-specific and disease-free survival rates were similar. Local recurrence-free survival was marginally better using CAPC, which resulted in only one local failure 9 months after partial cystectomy. Using standard partial cystectomy, there were seven local failures. This translates to a 5-year local recurrence-free survival of 0.8 for the patients treated using CAPC and 0.426 for those treated using standard partial cystectomy (P=0.088).
 | Figure 2 Kaplan–Meier survival curves. |
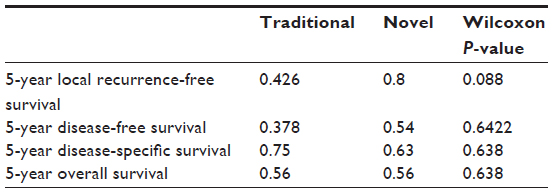 | Table 2 Survival rates after partial cystectomy using the traditional and novel methods |
Discussion
When strict criteria are used for patient selection, partial cystectomy provides survival rates comparable with those of radical cystectomy, with lower morbidity and mortality.7,8 Five-year cancer-specific survival after partial cystectomy is 58%–87% in modern series.4,6,8 There is of course a risk of local recurrence in up to 50% of patients,6 especially when Tis is present, and lifelong follow-up is required. Ultimately, three quarters of patients retain their bladder in the long-term.6,8
The standard technique of partial cystectomy that involves mobilization of the bladder, ie, “cystotomy away from the tumor”, and removal of the tumor-bearing segment has not changed over the last century. It requires either palpation of the tumor or “smart guess” based on previous knowledge of tumor location. Using this method, it is often necessary to close two incisions in the bladder (that of the initial cystotomy and that of the tumor) and, importantly, the initial blind cystotomy can go through the tumor itself or compromise the surgical margins. Two incisions also increase the risk of urinary leakage and subsequent complications.
In this paper we describe a simple and precise method for partial cystectomy. Using a flexible cystoscope, the surgeon identifies the tumor and plans the incision around it. The light of the cystoscope is used to mark one of the poles of the planned incision. The result is a single and accurate incision around the tumor. As such, the CAPC method has two theoretical advantages. Local cancer control is expected to be better and damage to the bladder decreased. Additionally, using the flexible cystoscope is a common practice among urologists and there should not be any learning curve.
This novel technique was performed in eleven patients and the results were compared with those in 19 patients who underwent standard partial cystectomy during the same period. The oncological results of the entire series match the results reported in the literature for overall, disease-specific, and disease-free survival rates.4–6 Patients operated on using CAPC were similar to patients operated on using standard partial cystectomy in all aspects except for tumor diameter, which was significantly larger in the CAPC group (Table 1). The complication rate was low in both groups, matching the reported low rate of complications with this operation.4 The long-term results of the two methods were similar (Table 2). Despite having significantly larger tumors, there was only one local recurrence in the group that underwent CAPC compared with seven local recurrences when standard partial cystectomy was used. However, this difference did not reach statistical significance (P=0.088).
The idea of using cystoscopic light during surgery has been reported in a case report of a patient suffering from endometriosis,10 but not in the context of bladder cancer. It seems that the future of partial cystectomy includes laparoscopy and robot-assisted surgery.11,12 The method described here seems most suitable for these technologies, which involve an inherent loss of tactile perception often used for identification of tumor location during open surgery.
The main drawback of the study is the small number of patients. However, partial cystectomies are rare operations, especially in teaching centers, and it may take years to recruit a larger series.3 An additional drawback of the study is the nonrandomized selection of patients.
Conclusion
The use of flexible cystoscopy during partial cystectomy is a simple maneuver that assists in planning the bladder incision and minimizes damage to the rest of the bladder. Initial oncological results are promising, with a trend toward a low rate of local recurrence compared with the standard method. This method is easy to learn and no significant learning curve is expected. Further follow-up studies are warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
Biagioli MC, Fernandez DC, Spiess PE, et al. Primary bladder preservation treatment for urothelial bladder cancer. Cancer Control. 2013;20:188–199. | |
Sweeney P, Kursh ED, Resnick MI. Partial cystectomy. Urol Clin North Am. 1992;19:701–711. | |
Hollenbeck BK, Taub DA, Dunn RL, et al. Quality of care: partial cystectomy for bladder cancer – a case of inappropriate use? J Urol. 2005;174:1050–1054. | |
Smaldone MC, Jacobs BL, Smaldone AM, et al. Long-term results of selective partial cystectomy for invasive urothelial bladder carcinoma. Urology. 2008;72:613–616. | |
Holzbeierlein JM, Lopez-Corona E, Bochner BH, et al. Partial cystectomy: a contemporary review of the Memorial Sloan-Kettering Cancer Center experience and recommendations for patient selection. J Urol. 2004;172:878–881. | |
Kassouf W, Swanson D, Kamat AM, et al. Partial cystectomy for muscle invasive urothelial carcinoma of the bladder: a contemporary review of the MD Anderson Cancer Center experience. J Urol. 2006;175:2058–2062. | |
Capitanio U, Isbarn H, Shariat SF, et al. Partial cystectomydoes not undermine cancer control in appropriately selected patients with urothelial carcinoma of the bladder: a population-based matched analysist. Urology. 2009;74:858–864. | |
Knoedler JJ, Boorjian SA, Kim SP, et al. Does partial cystectomy compromise oncologic outcomes for patients with bladder cancer compared to radical cystectomy? A matched case-control analysis. J Urol. 2012;188:1115–1119. | |
Berglund RK, Herr HW. Surgery for bladder cancer. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-Walsh Urology. 10th ed. Elsevier: Philadelphia, PA, USA; 2012. | |
Seracchioli R, Mannini D, Colombo FM, et al. Cystoscopy-assisted laparoscopic resection of extramucosal bladder endometriosis. J Endourol. 2002;16:663–666. | |
Tareen BU, Mufarrij PW, Godoy G, et al. Robot-assisted laparoscopic partial cystectomy and diverticulectomy: initial experience of four cases. J Endourol. 2008;22:1497–1500. | |
Allaparthi S, Ramanathan R, Balaji KC. Robotic partial cystectomy for bladder cancer: a single-institutional pilot study. J Endourol. 2010;24:223–227. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.