Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
CYP2D6 Predicts Plasma Donepezil Concentrations in a Cohort of Thai Patients with Mild to Moderate Dementia
Authors Chamnanphon M ![]() , Wainipitapong S, Wiwattarangkul T, Chuchuen P, Nissaipan K, Phaisal W, Tangwongchai S, Sukasem C, Wittayalertpanya S, Gaedigk A
, Wainipitapong S, Wiwattarangkul T, Chuchuen P, Nissaipan K, Phaisal W, Tangwongchai S, Sukasem C, Wittayalertpanya S, Gaedigk A ![]() , Aniwattanapong D
, Aniwattanapong D ![]() , Chariyavilaskul P
, Chariyavilaskul P ![]()
Received 12 August 2020
Accepted for publication 6 October 2020
Published 2 November 2020 Volume 2020:13 Pages 543—551
DOI https://doi.org/10.2147/PGPM.S276230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Monpat Chamnanphon,1 Sorawit Wainipitapong,2 Teeravut Wiwattarangkul,3 Phenphichcha Chuchuen,2 Kunathip Nissaipan,1,4 Weeraya Phaisal,1,4 Sookjaroen Tangwongchai,2 Chonlaphat Sukasem,5 Supeecha Wittayalertpanya,1,4 Andrea Gaedigk,6 Daruj Aniwattanapong,2 Pajaree Chariyavilaskul1,4
1Clinical Pharmacokinetics and Pharmacogenomics Research Unit, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 2Department of Psychiatry, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 4Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Division of Pharmacogenomics and Personalized Medicine, Department of Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 6Division of Clinical Pharmacology, Toxicology & Therapeutic Innovation, Children’s Mercy Kansas City and School of Medicine, University of Missouri-Kansas City, Kansas City, Missouri, USA
Correspondence: Daruj Aniwattanapong
Department of Psychiatry, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Tel +66 2 256 4298
Email [email protected]
Pajaree Chariyavilaskul
Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Tel +66 2 256 4481 ext. 3020
Email [email protected]
Purpose: Donepezil, a drug frequently used to treat dementia, is mainly metabolized by cytochrome P450 2D6 (CYP2D6). This study investigated the relationships between CYP2D6 genotype and activity scores as well as predicted phenotype of plasma donepezil concentrations in 86 Thai dementia participants.
Materials and Methods: CYP2D6 was genotyped using bead-chip technology (Luminex xTAG® v.3). Steady-state trough plasma donepezil concentrations were measured using high-performance liquid chromatography.
Results: Sixteen genotypes were found but the most frequent genotypes detected among our participants were CYP2D6*10/*10 (27.9%) and *1/*10 (26.7%). One-third of the participants had an activity score of 1.25 which predicted that they were normal metabolizers. The overall median (interquartile range) of plasma donepezil concentration was 51.20 (32.59– 87.24) ng/mL. Normal metabolizers (NMs) had lower plasma donepezil concentrations compared to intermediate metabolizers (IMs) (41.15 (28.44– 67.65) ng/mL vs 61.95 (35.25– 97.00) ng/mL). Multivariate analysis showed that CYP2D6 activity score (r2 = 0.50) and the predicted phenotype (independent of dose) could predict the plasma donepezil concentration (r2 = 0.49).
Conclusion: Plasma donepezil concentration in NMs was lower compared to IMs. Additional studies with larger sample size and use of next-generation sequencing as well as its outcomes are warranted to confirm the benefit of using pharmacogenetic-guided treatment for donepezil.
Keywords: CYP2D6, Luminex xTAG®, donepezil, dementia, pharmacogenetics
Introduction
Dementia is one of the major health problems worldwide. Alzheimer’s disease (AD), the most common form of dementia, is a progressive neurological disorder characterized by the loss of memory and impaired intellectual abilities. AD is associated with the damage of cholinergic neurons in the brain and the decrease in acetylcholine levels which interferes with the action of neurotransmitters.1–3 AD patients suffer not only from memory loss, but also behavioral, thought, emotion and self-care problems. It has been reported that the total treatment costs for AD were at least nine billion dollars which is a huge burden to families and caregivers.4 Unfortunately, only 10–20% of the patients moderately respond to conventional anti-dementia drugs.5
Acetylcholinesterase is a primary member of the cholinesterase enzyme family. Acetylcholinesterase inhibitors (AChEIs) inhibit acetylcholinesterase from breaking down acetylcholine into choline and acetate. This in turn results in an elevated level of acetylcholine in the central nervous system, autonomic ganglia and neuromuscular junctions for long periods of time. This action compensates for the loss of functioning brain cells in AD, resulting in an improvement in the patient’s cognitive and behavioral functions.6,7 To date, AChEIs are the main drug class for the treatment of dementia.5,8
Donepezil is one of the AChEIs currently approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of cognitive manifestations of dementia. Donepezil is mainly metabolized through cytochrome P450 2D6 (CYP2D6) enzyme in the liver.9 CYP2D6 gene locus is highly polymorphic10 and affects the pharmacokinetic properties of donepezil, resulting in interindividual variability of the plasma concentrations of donepezil.7,9 There are four phenotype groups that are commonly used to classify individuals as ultra-rapid metabolizers (UMs), normal metabolizers (NMs), intermediate metabolizers (IMs), and poor metabolizers (PMs). The Clinical Pharmacogenetic Consortium (CPIC) has recently published recommendations for standardized translation of genotype into phenotype which we have adopted for this study.11
Genetic variability of CYP2D6 differs considerably among various ethnic groups.12–15 CYP2D6 allele is frequently found in the Thai population.14–16 A study reported the effects of CYP2D6*10 on plasma donepezil concentration in Thai16 and Chinese17 patients with dementia. However, those studies measured only CYP2D6*2 and *10. As CYP2D6 is highly polymorphic,10 it is unknown if other variations of CYP2D6 can affect the dose and/or plasma concentration of AChEIs, especially donepezil, in dementia patients. Also, the calculation of the CYP2D6 activity score has not been explored. These data are crucial in establishing a specific guideline for the use of pre-emptive CYP2D6 genotyping to estimate AChEIs dose adjustment in this specific group of patients.
This study investigated the relationship between CYP2D6 genotype, activity score and genotype-predicted phenotype on the steady-state of plasma donepezil concentrations in a cohort of Thai patients suffering from mild to moderate degrees of dementia.
Materials and Methods
This was a cross-sectional study conducted during the maintenance phase of donepezil treatment in Thai participants with dementia. The study was approved by the Ethics Committee of the Faculty of Medicine, Chulalongkorn University (IRB number 201/59) and was registered in the Thai Clinical Trial Registry (TCTR20190924003). All participants or their legal guardians gave their informed consent before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki and the guideline of the International Conference on Harmonization in Good Clinical Practice. Experimental work and data analyses were performed at the Clinical Pharmacokinetics and Pharmacogenomics Research Unit, Department of Pharmacology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Participants
A cohort of unrelated participants with mild to moderate dementia who were continuously treated with donepezil for at least 6 months were enrolled in the study. The participants were recruited from the Dementia Outpatient Clinic, King Chulalongkorn Memorial Hospital, Bangkok, Thailand. Patients on other available AChEIs (galantamine and rivastigmine) were excluded. The diagnosis of dementia was done by qualified dementia specialists at the Dementia Outpatient Clinic, King Chulalongkorn Memorial Hospital, Bangkok, Thailand. Comprehensive neuropsychological tests were done to assess the severity of the disease. The validated Thai Mental State Examination (TMSE), Neuropsychiatry Inventory Questionnaire (NPI-Q) and Thai version of Disability Assessment for Dementia scale (DAD-T)18 were used to assess the participant’s cognitive, psychological and behavioral functions. Also, other tests assessed whether the participants were able to carry on with their daily routines or not. All participants provided written informed consent prior to the start of the study.
CYP2D6 Genotyping and Translation into Phenotype
Genomic DNA was isolated from EDTA-treated whole blood samples (3 mL) using a DNA extraction kit according to the manufacturer’s instruction (Invitrogen PureLink® Genomic DNA Mini Kit, Life Technologies, Carlsbad, CA, USA) and adjusted to 20 ng/µL. The Luminex xTAG CYP2D6 kit version 3 (Luminex Molecular Diagnostic, Toronto, ON, Canada) was used to simultaneously detect 19 nucleotide variants of CYP2D6: 1584C>G, 31G>A, 100C>T, 124G>A, 138insT, 883G>C, 1022C>T, 1660G>A, 1662G>C, 1708T>del, 1759G>T/A, 1847G>A, 2550A>del, 2616delAGA, 2851C>T, 2936A>C, 2989G>A, 3184G>A and 4181G>C (positions are numbered using the NG_008376.3 RefSeq as recommended by the Pharmacogene Variation Consortium).19 Gene deletion of CYP2D6*5 and presence of duplications were also detected. Samples were analyzed on a Luminex 200 IS system.
CYP2D6 genotypes were assigned using xTAG® Data Analysis Software (TDAS CYP2D6 1.01) and translated into phenotype using the CYP2D6 activity score system based on the new standardized method that was recently recommended by CPIC.20 Briefly, the CYP2D6*10 allele received a lower value for activity score calculation (ie, 0.25 vs 0.50). CYP2D6 activity scores were then translated into phenotype as follows: UMs (activity score >2.25), NMs (activity score of 1.25 ≤ x ≤ 2.25), IMs (activity score of 0 < x < 1.25), and PMs (activity score of 0).20
Determination of Plasma Donepezil Concentrations
Steady-state trough plasma donepezil concentrations were measured using a fully validated high performance liquid chromatography (HPLC) technique as previously described with some modifications.21,22
Sample preparation was done by liquid-liquid extraction. One mL of plasma was combined with 10 μL of internal standard solution (200 ng/mL rosiglitazone in acetonitrile) and mixed for 1 minute. Then, 5 mL of methyl tert-butyl ether was added and mixed for another 1 minute, followed by centrifugation at 4500 rpm at 25°C for 10 minutes. The organic layer was transferred into a 15 mL conical glass tube. The supernatant was evaporated to dryness and reconstituted with 150 µL of 50% methanol in de-ionized water. The mixture was further centrifuged at 4500 rpm at 25°C for 15 minutes. Subsequently, 90 µL of the final reconstituted solution was injected into the HPLC system (Shimadzu Corporation, Japan). A reversed-phase chromatographic separation was performed using a Luna 5u C18 column (250 mm x 4.6 mm, 5 microns, Phenomenex, USA). The analytes were eluted under gradient conditions using a mobile phase composed of acetonitrile and 20 mM of potassium dihydrogen phosphate with a pH of 5.85. Compounds were detected with a fluorescence detector at an excitation of 330 nm and an emission of 380 nm. A linear calibration curve ranged from 2.5–112 ng/mL (r2 > 0.999). Intra- and inter-day precisions (at concentrations of 7.5, 40 and 80 µg/mL) were 0.59–2.78% and 7.76–10.82%, respectively. The accuracy was 86.44–113.10%. The mean absolute recovery was more than 93.09%. The total runtime was 23 minutes.
Plasma donepezil concentrations were reported as measured concentrations (ng/mL), concentrations/dose per day (ng/mL/mg/day) and concentration/dose per day/weight (ng/mL/mg/kg/day).
Statistical Analysis
All analyses were performed using STATA version 14.0 (College Station, TX: StataCorp LP). Descriptive statistics were employed to describe the basic demographic data and CYP2D6 alleles whereas genotype frequencies were presented as median (interquartile range) (median (IQR)). Chi-square test, Fisher’s exact test, Mann–Whitney U-test, or Kruskal Wallis test was performed according to types and distributions of the data. Univariate and multivariate analyses were carried out to explore the relationships between donepezil concentrations as a dependent variable, and CYP2D6 genotype, activity score, predicted phenotype, and other parameters as independent variables. A p-value of <0.05 was considered significant.
Results
The characteristics of the 86 Thai elderly dementia participants were enrolled in the study (Table 1). All participants had a similar degree of mild to moderate dementia based on the comprehensive neuropsychological tests.
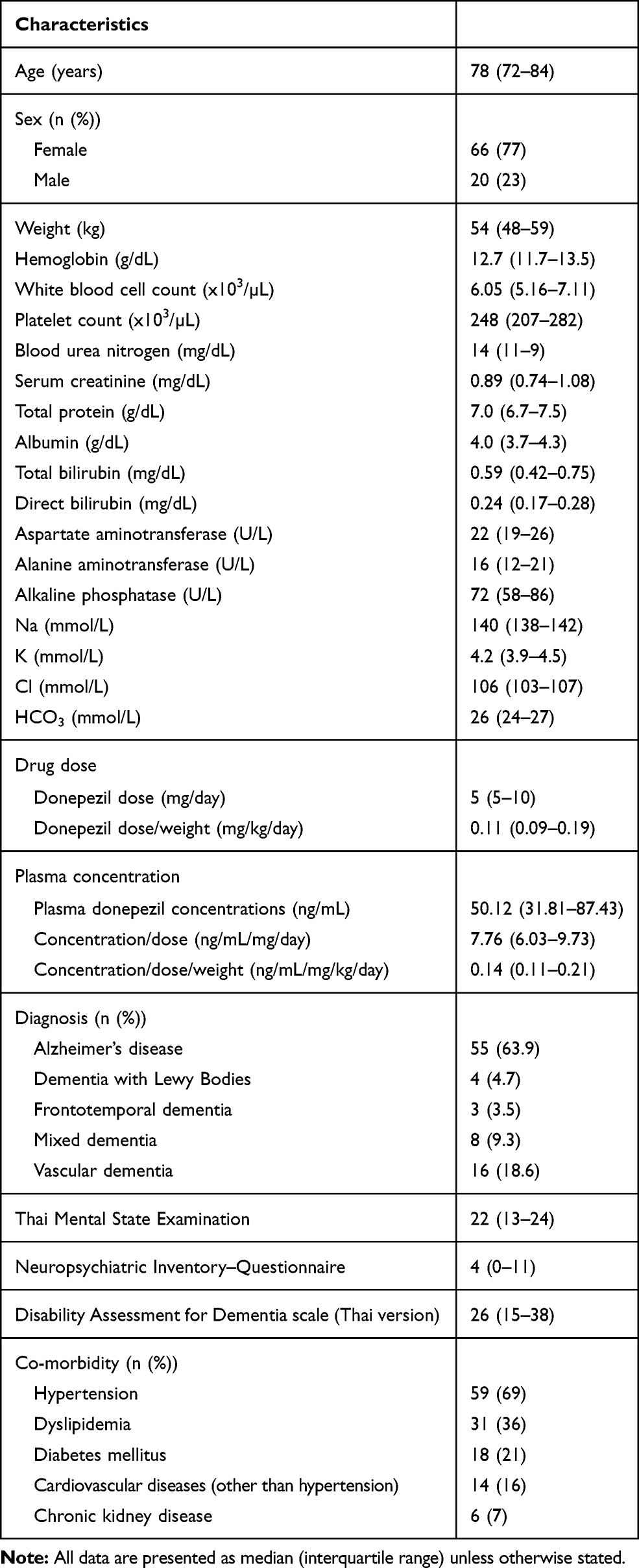 |
Table 1 Patients’ Characteristics (n = 86) |
For all participants, the median donepezil dose was 5 (5–10) mg/day and median donepezil dose per day/weight was 0.11 (0.09–0.19) mg/kg/day. Plasma donepezil concentrations were significantly correlated with dose per day and dose per day/weight (r2 = 0.77 and 0.70, respectively, p < 0.01). The overall median plasma donepezil concentration was 50.12 (31.81–87.43) ng/mL. The median concentration/dose per day was 7.76 (6.03–9.73) ng/mL/mg/day and median concentration/dose per day/weight was 0.14 (0.11–0.21) ng/mL/mg/kg/day (Table 1).
CYP2D6 Genotypes: Relationships to Plasma Donepezil Concentrations and Donepezil Dose
Sixteen different genotypes were detected of which the following CYP2D6 alleles were frequently found in our study: CYP2D6*10 (n = 94, 54.7%), CYP2D6*1 (n = 37, 21.5%), CYP2D6*2 (n = 17, 9.9%), CYP2D6*5 (n = 14, 8.1%), CYP2D6*41 (n = 7, 4.1%), CYP2D6*4 (n = 2, 1.2%), and CYP2D6*14B (n = 1, 0.6%) (Table 2). CYP2D6*10/*10 was the most frequent genotype (27.9%) detected followed by CYP2D6*1/*10 (26.7%), CYP2D6*5/*10 (10.5%) and CYP2D6*2/*10 (7.0%).
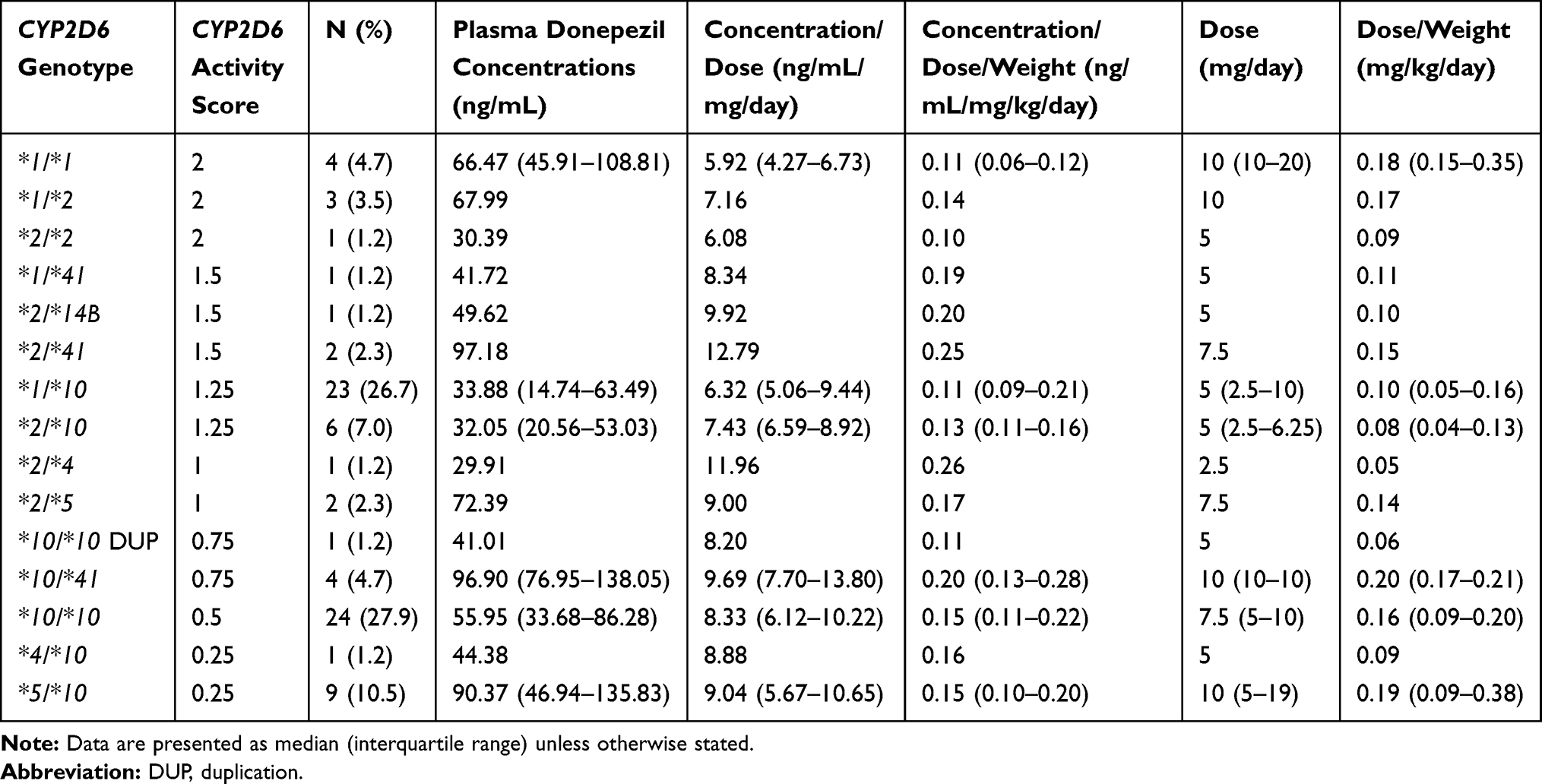 |
Table 2 CYP2D6 Genotype, Plasma Donepezil Concentrations and Dose per Day (n = 86) |
Plasma donepezil concentration, concentration/dose per day and concentration/dose per day/weight were highly variable amongst the CYP2D6 genotypes. However, no statistically significant differences of the plasma donepezil concentration, concentration/dose per day, and concentration/dose per day/weight were seen across the genotype groups (Table 2).
CYP2D6 Activity Scores and Predicted Phenotypes: Relationships to Plasma Donepezil Concentrations and Donepezil Dose
The participants were classified into 7 groups based on their CYP2D6 activity score (Table 3). The three most commonly observed CYP2D6 activity score groups were 1.25 (34%), 0.5 (28%) and 0.25 (12%). Donepezil dose per day was significantly different across the activity score groups (p = 0.029).
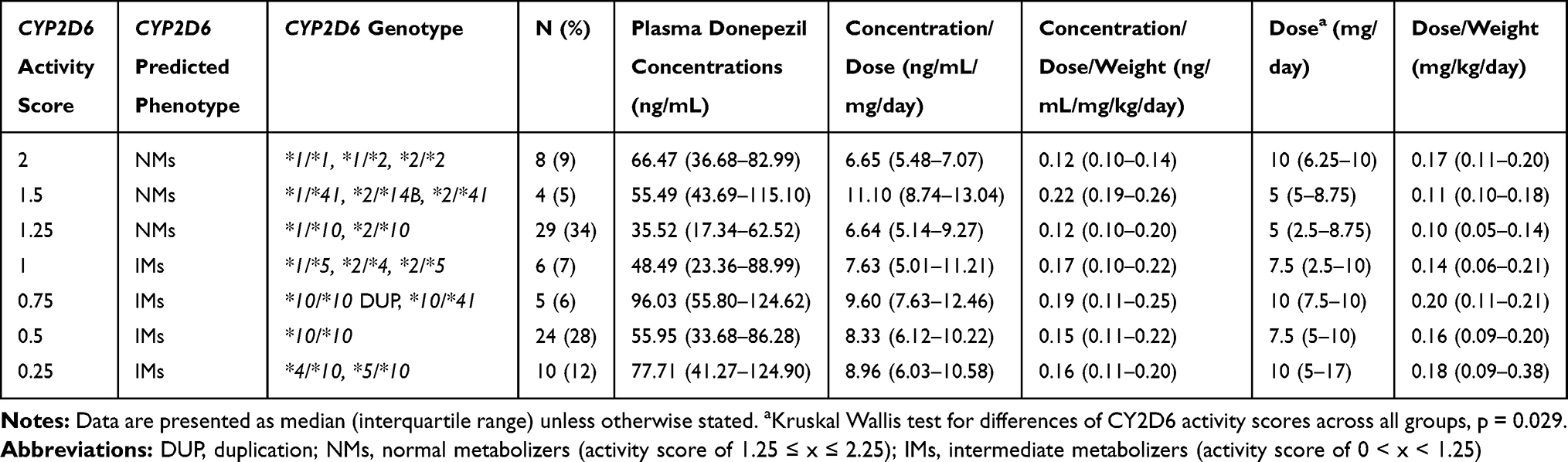 |
Table 3 CYP2D6 Activity Score, Plasma Donepezil Concentrations and Dose per Day (n = 86) |
About half of the participants in this study were predicted to be NMs (n = 41, 48%) and the other half, IMs (n = 45, 52%). NMs had lower plasma donepezil concentrations and donepezil dose per day compared to IMs (41.15 (28.44–67.65) vs 61.95 (35.25–97.00) ng/mL, p = 0.038 and 5 (5–10) vs 10 (5–10) mg/day, p = 0.035, respectively) (Figure 1A and D). There were no significant differences between NMs and IMs for concentration/dose per day (6.78 (5.33–9.27) ng/mL/mg/day vs 8.50 (6.41–10.45) ng/mL/mg/day), concentration/dose per day/weight (0.12 (0.10–0.20) vs 0.15 (0.11–0.21) ng/mL/mg/kg/day), and dose per day/weight (0.10 (0.07–0.18) vs 0.16 (0.09–0.20) mg/kg/day) (Figure 1B, C and E).
 |
Figure 1 Bar charts represent plasma donepezil concentrations and dose per day between CYP2D6 predicted phenotypes. (A) median plasma donepezil concentration (ng/mL) between CYP2D6 normal and intermediate metabolizers (p = 0.038). (B) median plasma donepezil concentration/dose (ng/mL/mg/day) between CYP2D6 normal and intermediate metabolizers (p > 0.05). (C) plasma donepezil concentration/dose/weight (ng/mL/mg/kg/day) between CYP2D6 normal and intermediate metabolizers (p > 0.05). (D) median donepezil dose (mg/day) between CYP2D6 normal and intermediate metabolizers (p = 0.035). (E) median donepezil dose/weight (mg/kg/day) between CYP2D6 normal and intermediate metabolizers (p > 0.05). |
From the multivariate analysis, the CYP2D6 activity score and CYP2D6 predicted phenotype were predictors of plasma donepezil concentration, independent of dose and other factors (Table 4).
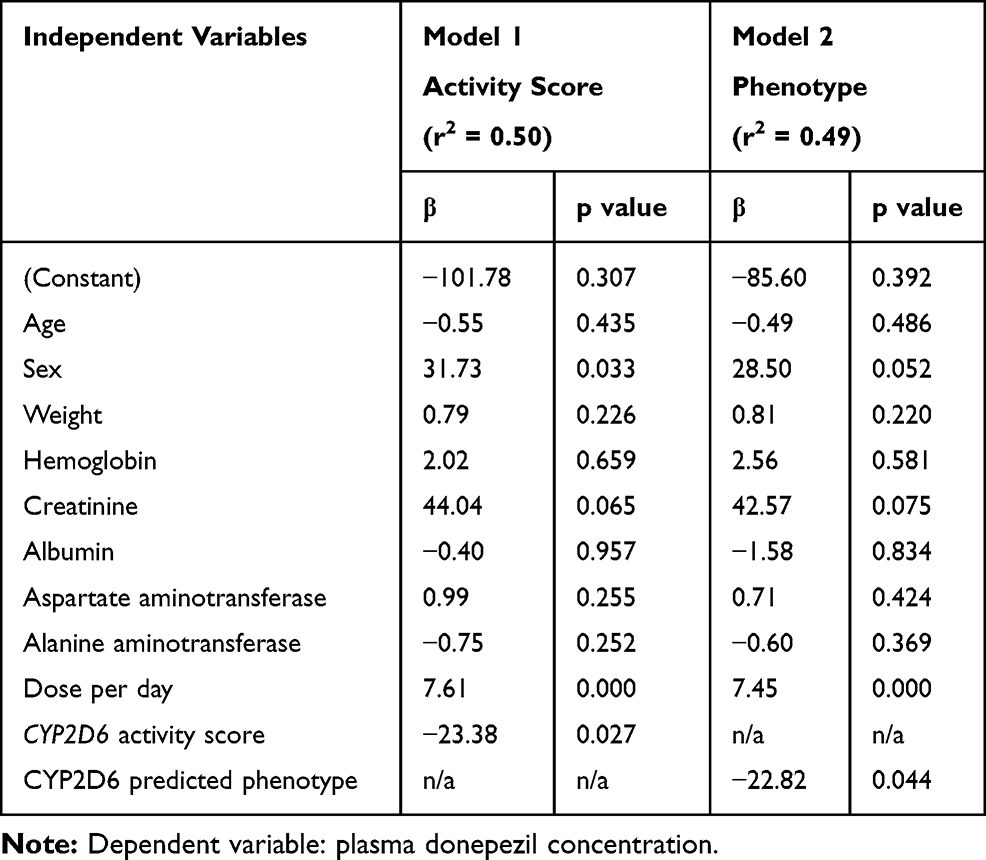 |
Table 4 Multivariate Analysis |
Discussion
This study investigated the relationships between CYP2D6 genotype, activity score, and predicted phenotype to the steady-state plasma donepezil concentrations in Thai participants with mild to moderate dementia.
CYP2D6 allele frequencies in this study were in line with previous studies conducted in Thai, East Asian and Chinese populations.16,17,23,24 The distribution of CYP2D6 genotype in this study was similar to those observed in Thai16 and Chinese patients24 with approximately half of them had CYP2D6*1/*10 and CYP2D6*10/*10. On the other hand, our findings were different to those found in other ethnic groups including South/Central Asian, Middle East, Oceanian, African American, African, Caucasian and American23 (Table 5). However, only CYP2D6*10 was focused in those previous studies16,24 and no consideration in regard to CYP2D6 activity score was noted. Our study used a higher resolution technique which simultaneously detects 19 nucleotide variants of CYP2D6 and genotype data was translated into phenotype using the CYP2D6 activity score system. Hence, the predicted phenotypes reported in our study were highly accurate compared to the previous ones.
 |
Table 5 CYP2D6 Allele Frequencies in Different Populations |
The majority of the participants in our Thai cohort had CYP2D6 activity scores of 1.25 (34%), 0.5 (28%) and 0.25 (12%). When the activity scores were translated into phenotypes, the participants were classified into NMs and IMs. There were no UMs or PMs in this study which was different from previous studies conducted in Italians,25 Indian26 and Japanese.27
The average trough plasma donepezil concentrations for therapeutic doses of 5 or 10 mg donepezil were 25.9 and 50.6 ng/mL, respectively.9 Hefner et al also suggested that plasma donepezil concentrations need to reach at least 50 ng/mL for maximum clinical efficacy at therapeutic dosage of 5 and 10 mg/day.28 The overall median plasma donepezil concentration in this study was 50.12 ng/mL which is consistent with the suggested therapeutic level.
A high degree of variability in plasma donepezil concentrations across genotypes and activity scores were seen but these did not reach statistical difference. Regardless, NMs showed significantly lower plasma donepezil concentrations compared to those observed for IMs (41.15 vs 61.95 ng/mL, p = 0.038). These findings were in line with those reported by Zhong et al that plasma donepezil concentrations were 40 ng/mL and 60 ng/mL in NMs and IMs, respectively.24 Taken together, these results suggest that CYP2D6 enzyme activity influences the metabolism of donepezil.
However, it remains controversial whether CYP2D6 activity impacts the efficacy of donepezil treatment or not.16,24,25,27,29–31,33 For example, a study by Varsaldi et al conducted in 42 AD patients evaluated the impact of CYP2D6 polymorphisms (CYP2D6*1, *2xN, *3, *4, *5 and *6) on steady state plasma donepezil concentrations and its clinical outcomes. They reported that CYP2D6 genotype influenced the metabolism of the drug and the treatment outcomes.25 A larger study was carried out in a group of Thai (n = 85)16 and Chinese (n = 110)24 patients; however, the patients in these studies were only genotyped for CYP2D6*10 (100C>T, rs1065852) variant. Despite this limitation, the investigators showed that the responders had a higher prevalence of CYP2D6*1/*10 and *10/*10 genotypes and higher levels of plasma donepezil concentrations. The decreased function of the genotypes and increased plasma drug levels were associated with improved cognitive score.
On the other hand, a study conducted by Chianella et al assessed the effects of CYP2D6 genetic variation (ie, CYP2D6*1, *1xN, *2, *2xN, *3, *4, *6, *9, *10, and *41) on the metabolism of donepezil and galantamine in 171 Italian patients with AD. They also assessed the genetic variation of butyrylcholine esterase (BCHE) which metabolizes and also is targeted by rivastigmine. The frequency of decreased and nonfunctional CYP2D6 alleles was higher in non-responders compared to responders. Genetic variation in either gene, CYP2D6 or BCHE, predicted clinical response in AD patients treated with AChEIs.29 Another study by Miranda et al also showed that the dose of AChEIs (donepezil, rivastigmine and galantamine), the absence of the apolipoprotein E (ApoE) ξ4 allele as a risk marker for AD, and CYP2D6 polymorphisms were not correlated with clinical response.34 A more recent study by Coin et al showed that increased plasma donepezil concentration at 9 months, but not drug metabolizing enzyme activity, were associated with better cognitive outcomes in AD patients. CYP2D6 and CYP3A4 activities were measured using probe drugs but no direct genotyping was performed.30
Based on the above conflicting reports,24,25,27,29–31,33 the current study was selectively conducted in dementia participants with the same degree of disease severity with no other major co-morbidities aiming to substantiate the effects of CYP2D6 genetic variation on drug dose and plasma levels. We demonstrated the relationships between genotype-predicted phenotype with donepezil dose and plasma concentrations in the univariate analysis. However, the multivariate analysis showed that dose has no effect on plasma concentration of donepezil. On the other hand, CYP2D6 activity score and phenotype groups significantly predicted plasma donepezil concentration (r2 = 0.50 and 0.49, respectively, Table 4). In contrast, Mori et al reported that dose and age, but not CYP2D6 predicted phenotype, predicted the plasma donepezil concentration.27 This finding is different to our study due to the difference of the study population. Mori et al’s study was conducted in patients with dementia with Lewy bodies.
This study has some limitations. The cross-sectional design displays associations, not causal relationships. The sample size is relatively small and did not comprise UMs or PMs. This may be due to the relative rarity of these phenotypes in East Asians including Thais. Second, the participants were classified into 16 genotypes but half of the genotype groups had a few subjects so there was not enough power to detect any significant differences in plasma donepezil concentration between the genotype groups. In addition, the participants who could not tolerate donepezil may have been switched to other drugs and thus were excluded from the study. Third, donepezil is also metabolized through CYP3A4 and CYP3A5 pathways and several other genes including ABCB1, POR, NR1/2 have been reported to be involved in donepezil disposition.26,30,35,36 However, a study in Thai population reported that those pathways and drug transporters played minimal roles in donepezil disposition and did not affect treatment outcome.16 Fourth, drug levels may also be affected by co-medications that are enzyme inducers or inhibitors. Although co-medications of the participants were reviewed and no potent enzyme inducers or inhibitors were identified, drug interactions cannot be completely ruled out. Also, a previous study reported that plasma concentrations of S-donepezil influence treatment outcome.17 Here, we measured racemic plasma donepezil concentrations as we would like to implement our findings into the real clinical setting were the measurement of stereoselective form of drug was not available in every hospital. Lastly, only sixteen common CYP2D6 variants were detected. However, undetected rare alleles would likely not have altered our conclusions.
Conclusion
In a cohort of Thai dementia participants with the same disease severity, we observed the relationships between CYP2D6 genotype-predicted phenotype and donepezil dose as well as the plasma concentration. NMs have lower plasma donepezil concentrations compared to IMs. The results from the multivariate analysis showed that independent of dose, CYP2D6 activity score and phenotype significantly predicted plasma donepezil concentration. Additional studies with a larger sample size utilizing next-generation sequencing are needed in order to confirm whether the patients would benefit from pharmacogenetic-guided treatment with donepezil or not.
Acknowledgments
We are grateful to the participants who took part in this study. We thank the staff of the Dementia Outpatient Clinic, King Chulalongkorn Memorial Hospital, Bangkok, Thailand for their support during the study. This research was supported by Ratchadaphisek Somphot Endowment Fund, Faculty of Medicine, Chulalongkorn University (grant number: RA59/090) and Ratchadaphisek Somphot Fund for Postdoctoral Fellowship, Chulalongkorn University.
Disclosure
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results. The data that support the findings of this study are available from the National Research Council of Thailand but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are; however, available from the authors upon a reasonable request and with a permission of the National Research Council of Thailand.
References
1. Eratne D, Loi SM, Farrand S, Kelso W, Velakoulis D, Looi JC. Alzheimer’s disease: clinical update on epidemiology, pathophysiology and diagnosis. Australas Psychiatry. 2018;26(4):347–357. doi:10.1177/1039856218762308
2. Alzheimer's Association Report. 2018 Alzheimer’s disease facts and figures. Alzhiemer's & Dementia. 2018;14(3):367–429.
3. Cummings JL. Alzheimer’s disease. N Engl J Med. 2004;351(1):56–67. doi:10.1056/NEJMra040223
4. Brown L. The economic cost of dementia in Australia 20162056. Report Prepared Alzheimer’s Australia. 2017.
5. Cacabelos R. Pharmacogenomics and therapeutic prospects in dementia. Eur Arch Psychiatry Clin Neurosci. 2008;258(Suppl 1):28–47. doi:10.1007/s00406-007-1006-x
6. McGleenon BM, Dynan KB, Passmore AP. Acetylcholinesterase inhibitors in Alzheimer’s disease. Br J Clin Pharmacol. 1999;48(4):471–480. doi:10.1046/j.1365-2125.1999.00026.x
7. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: part II. Clin Pharmacokinet. 2009;48(12):761–804.
8. Barner EL, Gray SL. Donepezil use in Alzheimer disease. Ann Pharmacother. 1998;32(1):70–77. doi:10.1345/aph.17150
9. Jann MW, Shirley KL, Small GW. Clinical pharmacokinetics and pharmacodynamics of cholinesterase inhibitors. Clin Pharmacokinet. 2002;41(10):719–739. doi:10.2165/00003088-200241100-00003
10. Nofziger C, Turner AJ, Sangkuhl K, et al. PharmVar GeneFocus: CYP2D6. Clin Pharmacol Ther. 2020;107(1):154–170. doi:10.1002/cpt.1643
11. Caudle KE, Sangkuhl K, Whirl-Carrillo M, et al. Standardizing CYP2D6 genotype to phenotype translation: consensus recommendations from the clinical pharmacogenetics implementation consortium and dutch pharmacogenetics working group. Clin Transl Sci. 2020;13(1):116–124. doi:10.1111/cts.12692
12. Goetz MP, Sangkuhl K, Guchelaar HJ, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 and tamoxifen therapy. Clin Pharmacol Ther. 2018;103(5):770–777. doi:10.1002/cpt.1007
13. Gaedigk A, Sangkuhl K, Whirl-Carrillo M, Klein T, Leeder JS. Prediction of CYP2D6 phenotype from genotype across world populations. Genet Med. 2017;19(1):69–76. doi:10.1038/gim.2016.80
14. Chamnanphon M, Gaedigk A, Vanwong N, et al. CYP2D6 genotype analysis of a Thai population: platform comparison. Pharmacogenomics. 2018;19(12):947–960. doi:10.2217/pgs-2018-0075
15. Suwannasri P, Thongnoppakhun W, Pramyothin P, Assawamakin A, Limwongse C. Combination of multiplex PCR and DHPLC-based strategy for CYP2D6 genotyping scheme in Thais. Clin Biochem. 2011;44(13):1144–1152. doi:10.1016/j.clinbiochem.2011.06.985
16. Yaowaluk T, Senanarong V, Limwongse C, Boonprasert R, Kijsanayotin P. Influence of CYP2D6, CYP3A5, ABCB1, APOE polymorphisms and nongenetic factors on donepezil treatment in patients with Alzheimer’s disease and vascular dementia. Pharmgenomics Pers Med. 2019;12:209–224.
17. Lu J, Wan L, Zhong Y, et al. Stereoselective metabolism of donepezil and steady-state plasma concentrations of S-donepezil based on CYP2D6 polymorphisms in the therapeutic responses of Han Chinese patients with Alzheimer’s disease. J Pharmacol Sci. 2015;129(3):188–195. doi:10.1016/j.jphs.2015.10.010
18. Charernboon TL,T. Functional disability in dementia: a validation study of the Thai version of disability assessment for dementia scale. J Clin Gerontol Geriatrics. 2015;6(4):133–136. doi:10.1016/j.jcgg.2015.04.001
19. https://www.pharmavar.org/gene/CYP2D6.
20. CYP2D6 genotypes to phenotype standardization project. https://cpicpgx.org/resources/cyp2d6-genotype-to-phenotype-standardization-project/. 2019.
21. Xie Z, Liao Q, Xu X, Yao M, Wan J, Liu D. Rapid and sensitive determination of donepezil in human plasma by liquid chromatography/tandem mass spectrometry: application to a pharmacokinetic study. Rapid Commun Mass Spectrom. 2006;20(21):3193–3198. doi:10.1002/rcm.2718
22. Abonassif MA, Hefnawy MM, Kassem MG, Mostafa GA. Determination of donepezil hydrochloride in human plasma and pharmaceutical formulations by HPLC with fluorescence detection. Acta Pharm. 2011;61(4):403–413. doi:10.2478/V10007-011-0035-1
23. CYP2D6 allele frequency table on PharmGKB. www.pharmgkb.org/page/cyp2d6RefMaterials.
24. Zhong Y, Zheng X, Miao Y, Wan L, Yan H, Wang B. Effect of CYP2D6*10 and APOE polymorphisms on the efficacy of donepezil in patients with Alzheimer’s disease. Am J Med Sci. 2013;345(3):222–226. doi:10.1097/MAJ.0b013e318255a8f9
25. Varsaldi F, Miglio G, Scordo MG, et al. Impact of the CYP2D6 polymorphism on steady-state plasma concentrations and clinical outcome of donepezil in Alzheimer’s disease patients. Eur J Clin Pharmacol. 2006;62(9):721–726. doi:10.1007/s00228-006-0168-1
26. Sonali N, Tripathi M, Sagar R, Velpandian T, Subbiah V. Impact of CYP2D6 and CYP3A4 genetic polymorphism on combined cholinesterase inhibitors and memantine treatment in mild to moderate Alzheimer’s disease. Dement Geriatr Cogn Disord. 2014;37(12):58–70. doi:10.1159/000350050
27. Mori E, Ikeda M, Nakai K, Miyagishi H, Nakagawa M, Kosaka K. Increased plasma donepezil concentration improves cognitive function in patients with dementia with Lewy bodies: an exploratory pharmacokinetic/pharmacodynamic analysis in a Phase 3 randomized controlled trial. J Neurol Sci. 2016;366:184–190. doi:10.1016/j.jns.2016.05.001
28. Hefner G, Brueckner A, Hiemke C, Fellgiebel A. Therapeutic drug monitoring for patients with Alzheimer dementia to improve treatment with donepezil. Ther Drug Monit. 2015;37(3):353–361. doi:10.1097/FTD.0000000000000152
29. Chianella C, Gragnaniello D, Maisano Delser P, et al. BCHE and CYP2D6 genetic variation in Alzheimer’s disease patients treated with cholinesterase inhibitors. Eur J Clin Pharmacol. 2011;67(11):1147–1157. doi:10.1007/s00228-011-1064-x
30. Coin A, Pamio MV, Alexopoulos C, et al. Donepezil plasma concentrations, CYP2D6 and CYP3A4 phenotypes, and cognitive outcome in Alzheimer’s disease. Eur J Clin Pharmacol. 2016;72(6):711–717. doi:10.1007/s00228-016-2033-1
31. Miranda LF, Gomes KB, Tito PA, et al. Clinical response to donepezil in mild and moderate dementia: relationship to drug plasma concentration and CYP2D6 and APOE genetic polymorphisms. J Alzheimers Dis. 2017;55(2):539–549. doi:10.3233/JAD-160164
32. Yang YH, Wu SL, Chou MC, Lai CL, Chen SH, Liu CK. Plasma concentration of donepezil to the therapeutic response of Alzheimer’s disease in Taiwanese. J Alzheimers Dis. 2011;23(3):391–397. doi:10.3233/JAD-2010-100936
33. Yang YH, Chen CH, Chou MC, Li CH, Liu CK, Chen SH. Concentration of donepezil to the cognitive response in Alzheimer disease. J Clin Psychopharmacol. 2013;33(3):351–355. doi:10.1097/JCP.0b013e31828b5087
34. Miranda LF, Gomes KB, Silveira JN, et al. Predictive factors of clinical response to cholinesterase inhibitors in mild and moderate Alzheimer’s disease and mixed dementia: a one-year naturalistic study. J Alzheimers Dis. 2015;45(2):609–620. doi:10.3233/JAD-142148
35. Magliulo L, Dahl ML, Lombardi G, et al. Do CYP3A and ABCB1 genotypes influence the plasma concentration and clinical outcome of donepezil treatment? Eur J Clin Pharmacol. 2011;67(1):47–54. doi:10.1007/s00228-010-0883-5
36. Noetzli M, Guidi M, Ebbing K, et al. Population pharmacokinetic approach to evaluate the effect of CYP2D6, CYP3A, ABCB1, POR and NR1I2 genotypes on donepezil clearance. Br J Clin Pharmacol. 2014;78(1):135–144. doi:10.1111/bcp.12325
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.