Back to Journals » Infection and Drug Resistance » Volume 12
Cycloserine for treatment of multidrug-resistant tuberculosis: a retrospective cohort study in China
Authors Li Y, Wang F, Wu L, Zhu M, He G, Chen X, Sun F, Liu Q, Wang X, Zhang W
Received 22 November 2018
Accepted for publication 3 January 2019
Published 29 March 2019 Volume 2019:12 Pages 721—731
DOI https://doi.org/10.2147/IDR.S195555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Yang Li,1,* Fei Wang,2,* Limin Wu,3 Min Zhu,4 Guiqing He,5 Xinchang Chen,1 Feng Sun,1 Qihui Liu,1 Xiaomeng Wang,2 Wenhong Zhang1
1Department of Infectious Diseases, Huashan Hospital, Fudan University, Shanghai 200032, China; 2Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang 310051, China; 3Hangzhou Center for Disease Control and Prevention, Hangzhou, Zhejiang 310021, China; 4Tuberculosis Treatment Center, Hangzhou Red Cross Hospital, Hangzhou 310003, China; 5Department of Infectious Diseases, Wenzhou Center Hospital, Wenzhou 325000, China
*These authors contributed equally to this work
Purpose: Cycloserine has been used in multidrug-resistant tuberculosis (MDR-TB) treatment since the 1950s. We evaluated the efficacy and safety of cycloserine and sought to clarify the role of cycloserine for treatment of simple MDR-TB, pre-extensively drug-resistant tuberculosis (pre-XDR-TB), and extensively drug-resistant tuberculosis (XDR-TB).
Materials and methods: A retrospective observational study was performed in Zhejiang Province, China. We enrolled 144 cycloserine-treated and 181 cycloserine-nontreated patients consecutively and determined the treatment outcome as the primary outcome. The proportion of patients with sputum culture conversion and the frequency of adverse drug reactions were also assessed.
Results: One-hundred (69.4%) out of 144 patients in the cycloserine group successfully completed treatment. The HR of any unfavorable treatment outcome after the introduction of cycloserine was 0.58 (95% CI: 0.38–0.86, P=0.008). Subgroup analysis showed that cycloserine could benefit simple MDR-TB cases reducing the risk of unfavorable treatment outcomes (HR: 0.43, 95% CI: 0.24–0.76, P=0.004), but not pre-XDR-TB (HR: 0.65, 95% CI: 0.30–1.38, P=0.263) or XDR-TB (HR: 0.73, 95% CI: 0.22–2.37, P=0.589). The culture conversion rate at the intensive phase was similar whether cycloserine was administered or not (P=0.703). Of the 144 patients treated with cycloserine, a total of 16 (11.1%) patients experienced side effects attributed to cycloserine.
Conclusion: Cycloserine is an attractive agent for the treatment of MDR-TB, and its safety profile warrants its use in most MDR-TB cases. Cycloserine significantly improved the chance of a favorable outcome for patients with simple MDR-TB but not pre-XDR-TB and XDR-TB. Thus, more aggressive regimens might be required for pre-XDR-TB or XDR-TB patients.
Keywords: cycloserine, multidrug-resistant tuberculosis, efficacy, safety, extensively drug-resistant tuberculosis, treatment outcome
Introduction
Tuberculosis (TB) has been a continuing threat throughout the ages. Since the early 1990s, multiple outbreaks of multidrug-resistant tuberculosis (MDR-TB), defined as TB caused by a strain of Mycobacterium tuberculosis that was resistant to at least isoniazid and rifampicin, have been reported, and it is generally accepted that resistance to these two potent anti-TB agents is associated with an increased probability of catastrophic treatment costs and poorer treatment outcomes. Furthermore, extensively drug-resistant tuberculosis (XDR-TB), defined as MDR-TB plus resistance to a fluoroquinolone and an injectable second-line drug, has recently emerged and threatened public health on a worldwide scale.1 In 2017, there were an estimated 460,000 new cases of MDR-TB, and China is a major contributor of drug-resistant TB (DR-TB). The latest data from the WHO reported a treatment success rate of 55% for MDR-TB and only 34% for XDR-TB.2
Cycloserine, a cyclic analog to D-alanine, could target alanine racemase and D-alanine ligase, thus blocking the formation of the bacterial cell wall.3 Cycloserine has been used in TB therapy since the late 1950s.4 Years later, Somner et al reported its potential for therapeutic intervention in chronic pulmonary TB.5 However, neurological toxicity associated with cycloserine concerns clinicians and limits its use. An earlier report described that symptomatic seizures were encountered in ~10% of patients.6 With the discovery of more effective drugs (eg, rifampicin), cycloserine has been applicable only in the treatment of apparent or proven DR-TB.
To implement TB control, the WHO published treatment guidelines for DR-TB in 1997 and cycloserine has been suggested since then, as it shares no cross-resistance with other agents and might be valuable to prevent resistance to other active drugs.7 In the 2008 recommendations, cycloserine was classified as a Group 4 oral bacteriostatic second-line medication.8 Recently, cycloserine has been recommended as one of the Group B drugs and should be generally included in the starting line-up in the longer regimen for the treatment of MDR-TB.9 However, the clinical studies that focused on cycloserine are scarce, particularly in East Asian patients, as the use of cycloserine was not approved in China until recently. Also, the role of cycloserine in the treatment of XDR-TB or pre-XDR-TB (defined as resistance to isoniazid and rifampicin plus any fluoroquinolone or one of the injectable drugs) is unclear. To address these uncertainties, we evaluated the efficacy, tolerability, and safety of cycloserine in MDR/pre-XDR/XDR-TB treatments using a sizable cohort of patients with MDR-TB from China.
Materials and methods
Study design and procedures
This cohort study was performed at two hospitals located in Zhejiang Province, China, and initiated by the Zhejiang Disease Control and Prevention Center (CDC) which has set up routine drug resistance monitoring for TB since 1999.10 The two clinical studies were completed in both the hospitals: one singer-arm study was supported by the Global Fund MDR-TB Project,11 and another cohort study entitled “Optimization of MDR-TB Treatment Regimen Based on the Molecular Drug Susceptibility Results of Pyrazinamide” was registered on ClinicalTrial.gov with number NCT02120638.12 To acquire complete follow-up information, we screened the patients in the two studies regarding eligibility consecutively. Approval for the collection of data was provided by the ethics committees of Zhejiang CDC. All procedures in this study were performed in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki. All patients provided written informed consent when they were recruited to the Global Fund Project or the clinical trial NCT02120638. The patient would be included if they met all inclusion criteria as follows: (1) male or female aged 18 years or older; (2) diagnosed with active MDR-TB with positive culture for M. tuberculosis and resistance to isoniazid and rifampicin proven by drug-susceptibility testing; and (3) initiating the treatment for MDR-TB between March 2012 and December 2015, and the background treatment regimen including a 6-month intensive phase of five drugs (one second-line injectable drug and four oral drugs) and an 18-month consolidation phase of four oral drugs. A later-generation fluoroquinolone mush be included in the regimen. Pyrazinamide, prothionamide, and an aminoglycoside were considered as priorities. As cycloserine had not been provided in Zhejiang Province until 2013, patients who were diagnosed with MDR-TB after October 2013 were provided with cycloserine (Korea Dong-A ST Co., Ltd.), while the previously diagnosed patients received para-aminosalicylic acid instead. If the standard regimen (fluoroquinolone, aminoglycoside, prothionamide, pyrazinamide, and cycloserine or para-aminosalicylic) could not be made up, ethambutol, high-dose isoniazid, amoxicillin-clavulanate, and clarithromycin were used.
Patients were excluded if they met any of the following exclusion criteria: 1) positive for HIV test; 2) history of seizure disorder, mental depression, or severe anxiety; and 3) declined to participate in this study.
The following information was collected: sociodemographic characteristics, indicators of severity (symptoms and radiologic findings), previous treatment, drug-resistant profiles, and background treatment regimen. Culture and sputum conversion and chest X-rays were performed periodically for the evaluation of treatment outcomes. Moreover, adverse drug reactions (ADRs) were monitored and promptly managed during the entire treatment course.
Definitions
In the present study, we use the term simple MDR-TB to refer to those with resistance to just isoniazid and rifampicin and complicated MDR-TB to refer to those with additional resistance beyond isoniazid and rifampicin, including pre-XDR-TB and XDR-TB.
Standard treatment outcome definitions were applied according to the definitions and reporting framework for TB from WHO in 2013.13 Cured was defined as treatment completed without evidence of failure and three or more consecutive cultures were negative after the intensive phase. If bacteriological results were lacking, the case was defined as treatment completed. Treatment failure was defined as treatment terminated or need for permanent regimen change of at least two anti-TB drugs because of lack of conversion by the end of the intensive phase, or bacteriological reversion in the continuation phase after conversion to negative, or ADR. The default was defined as interruption of treatment for at least 2 months not meeting the criteria for failure. This study used the following brief outcomes: favorable outcome was defined as cured and treatment completion; and unfavorable outcome was defined as any failure, default, or death while on treatment.
When assessing the ADR, we distinguished two types of side effects: major side effects and minor side effects.14 The former refer to any adverse reaction that resulted in temporary or permanent discontinuation of anti-TB drugs, while the latter refer to those that only required a dose adjustment, addition of concomitant treatment, or both.
Drug susceptibility testing
Sputum culture on Löwenstein–Jensen medium or MGIT 960 were applied routinely. Phenotypic drug susceptibility testing to two first-line drugs (rifampicin and isoniazid) and two second-line drugs (ofloxacin and kanamycin) (Baso, Zhuhai, Guangzhou Province, China) was performed from the first positive M. tuberculosis culture with the use of the proportion method, and the result was compared with the standardized strains. The critical drug concentrations of rifampicin, isoniazid, ofloxacin, and kanamycin were 40, 0.2, 2, and 30 µg/mL, respectively.15
Data management and statistical analysis
The clinical data were collected through questionnaires and medical records by trained health workers. For the analysis, patients were divided into two cohorts according to the presence or absence of cycloserine in the background regimen (cycloserine cohort vs non-cycloserine cohort). Continuous variables were calculated as mean with SD and median with IQR and were further compared by the Mann–Whitney U test. Categorical data were presented as numbers (percentage) and were compared using chi-squared test.
The primary outcome was the proportion of favorable treatment in each treatment cohort. All patients’ treatment outcomes were identified according to the definitions described earlier by two clinicians blinded for the background regimen. Considering the potential confounders, we investigated the effect of cycloserine upon the treatment outcome by using a Cox proportional-hazards model among the factors with a P-value less than 0.05 in the univariate Cox regression analysis. Furthermore, we did a specific subgroup analysis of patients with different drug resistance patterns.
Secondary outcome included the efficacy of cycloserine measured by the proportion of conversion within the intensive phase and safety and tolerability of cycloserine measured by the frequency of major and minor reactions.
A two-tailed P-value of less than 0.05 was considered statistically significant. All statistical calculations and analyses in this study were performed using SPSS Statistics, version 22.0 (IBM).
Results
Study population
Between March 2012 and December 2015, a total of 582 patients were recruited to the Global Fund Project and the clinical trial NCT02120638 and then initiated the treatment for MDR-TB. Among 582 patients who were assessed for eligibility, 241 patients were excluded because their background regimens were not adapted to the inclusion criteria. Eleven patients were excluded because the strains from their isolates were identified as nontuberculous mycobacteria. Moreover, three HIV-positive patients and two patients with mental illness in the control group were also excluded. Consequently, 325 patients confirmed to have an organism resistant to both rifampicin and isoniazid were enrolled, of which 144 were treated with cycloserine in their background regimen according to WHO guidelines for designated dosages of 500 mg or 750 mg per day (500 mg for 38 patients weighing less than 50 kg; 750 mg for 96 patients weighing more than 50 kg). All patients’ background regimen included one of the later-generation fluoroquinolones and only two patients in the cycloserine group had not been treated with aminoglycosides as the initial treatment.
Most of the demographic and baseline clinical characteristics were comparable among two treatment cohorts except that fever and TB cavity being more frequent in the cycloserine group. The mean age was 44.0 and 41.7 years in the cycloserine-treated and non-cycloserine-treated group, respectively. Approximately, 70% of patients were male in both groups. More than a quarter (27.4%, 89/325) of patients were treated with at least one of the fluoroquinolones or aminoglycosides more than 30 days before. More details are given in Table 1.
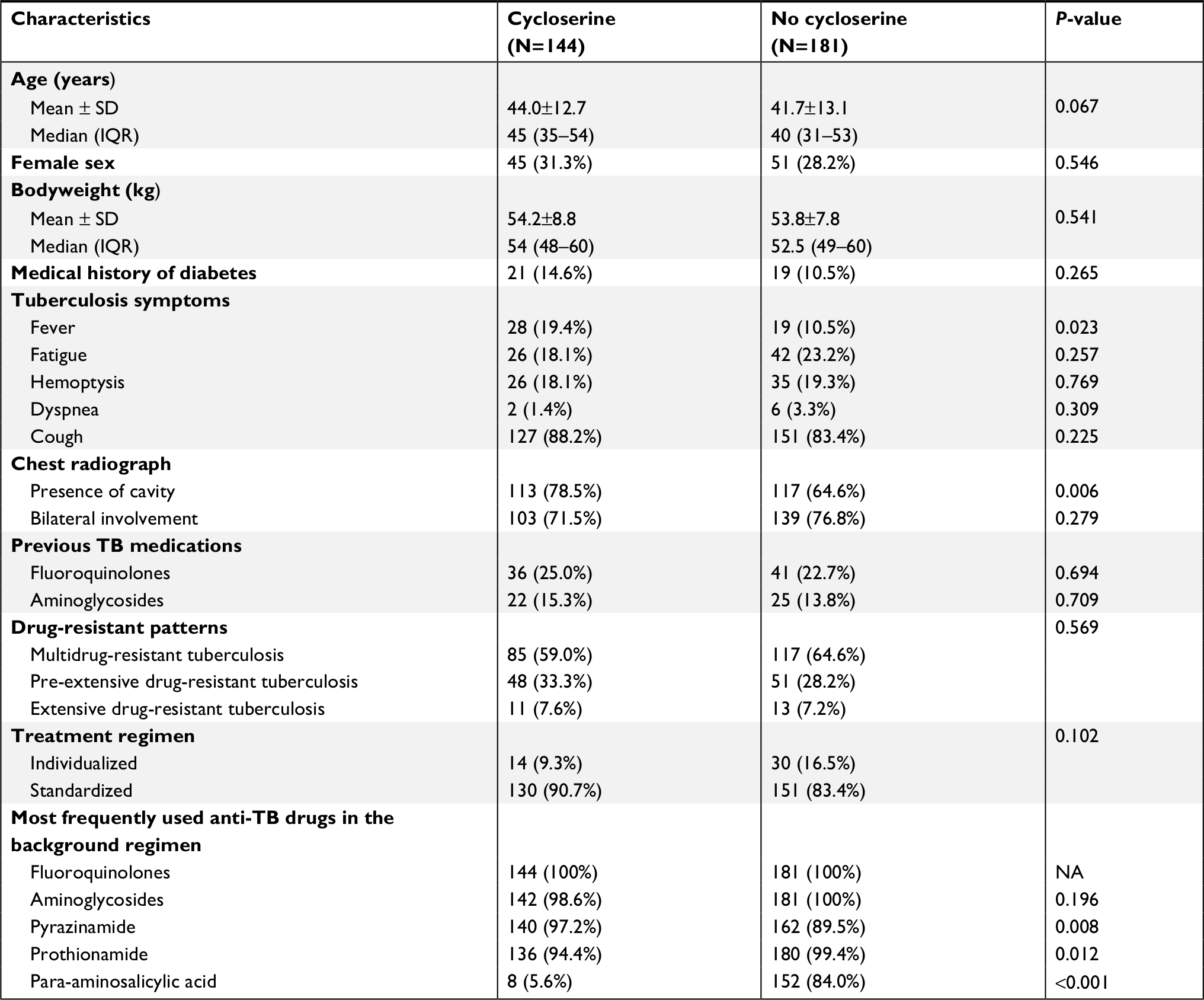 | Table 1 Characteristics of multidrug-resistant tuberculosis cases treated with or without cycloserine Note: Data are presented as n (%), unless otherwise stated. Abbreviations: TB, tuberculosis; NA, not applicable. |
Treatment outcome assessment
The introduction of cycloserine to the standard regimen resulted in significantly less risk of unfavorable treatment outcomes (HR: 0.58, 95% CI: 0.38–0.86, P=0.008). The treatment outcomes are listed in Table 2. One hundred out of 144 (69.4%) cycloserine-treated patients and 108 out of 181 (59.7%) non-cycloserine-treated patients achieved treatment success (P=0.081). The absence to sputum conversion at 6 months and severe ADRs resulting in two or more drug stoppages were the main reasons for treatment failure; the relative responsibilities were 35.1% and 43.2% in the cycloserine group and 43.3% and 41.7% in the non-cycloserine group, respectively. One patient was complicated by pulmonary infection and died in the 18th month of treatment.
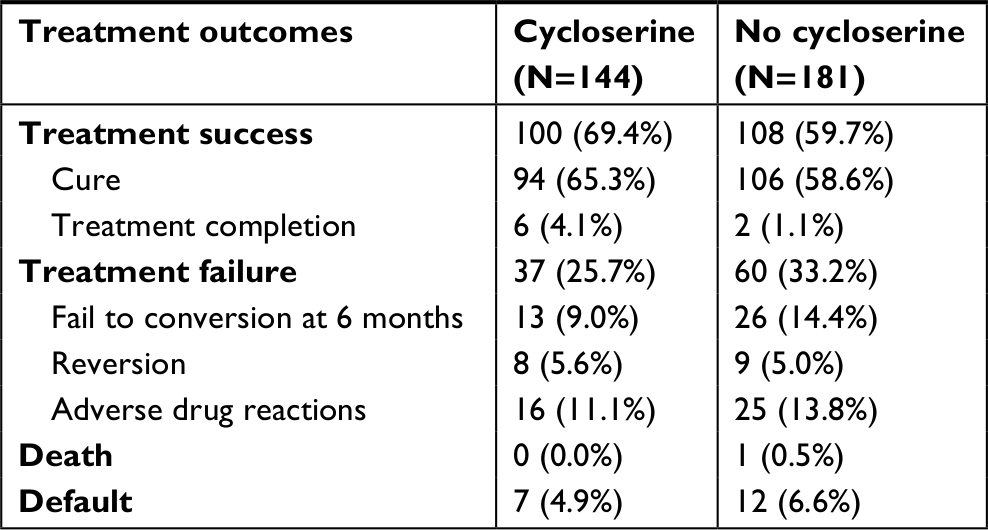 | Table 2 Treatment outcomes of multidrug-resistant/extensively drug resistant tuberculosis cases treated with or without cycloserine |
Treatment outcomes stratified by resistance patterns
The treatment outcomes were further compared between the two groups stratified by resistance patterns (Figure 1). Among simple MDR-TB patients, the proportion of treatment success in the cycloserine group was higher than in the non-cycloserine group, reaching statistical significance (68/85, 80.0% vs 73/117, 62.4%, P=0.007). Cox regression analysis showed that cycloserine could provide benefit to simple MDR-TB patients by reducing the risk of unfavorable treatment outcomes (HR: 0.428, 95% CI: 0.240–0.761, P=0.004). For other strata, the treatment success rate in the cycloserine group was almost similar to patients who were not treated with cycloserine. Or rather, among pre-XDR-TB patients, the proportion achieving favorable outcome was 56.3% (27/48) in those receiving cycloserine vs 56.9% (29/51) in those treated without cycloserine, and among XDR-TB patients, the proportion of favorable outcome was 45.5% (5/11) and 46.2% (6/13), respectively. Cox regression analysis found that cycloserine might fail to improve the treatment outcome for pre-XDR-TB (HR: 0.650, 95% CI: 0.305–1.383, P=0.263) and XDR-TB patients (HR: 0.723, 95% CI: 0.223–2.374, P=0.589). Moreover, a downward trend in favorable treatment outcome rate was observed with the increase in the extent of drug resistance in both groups.
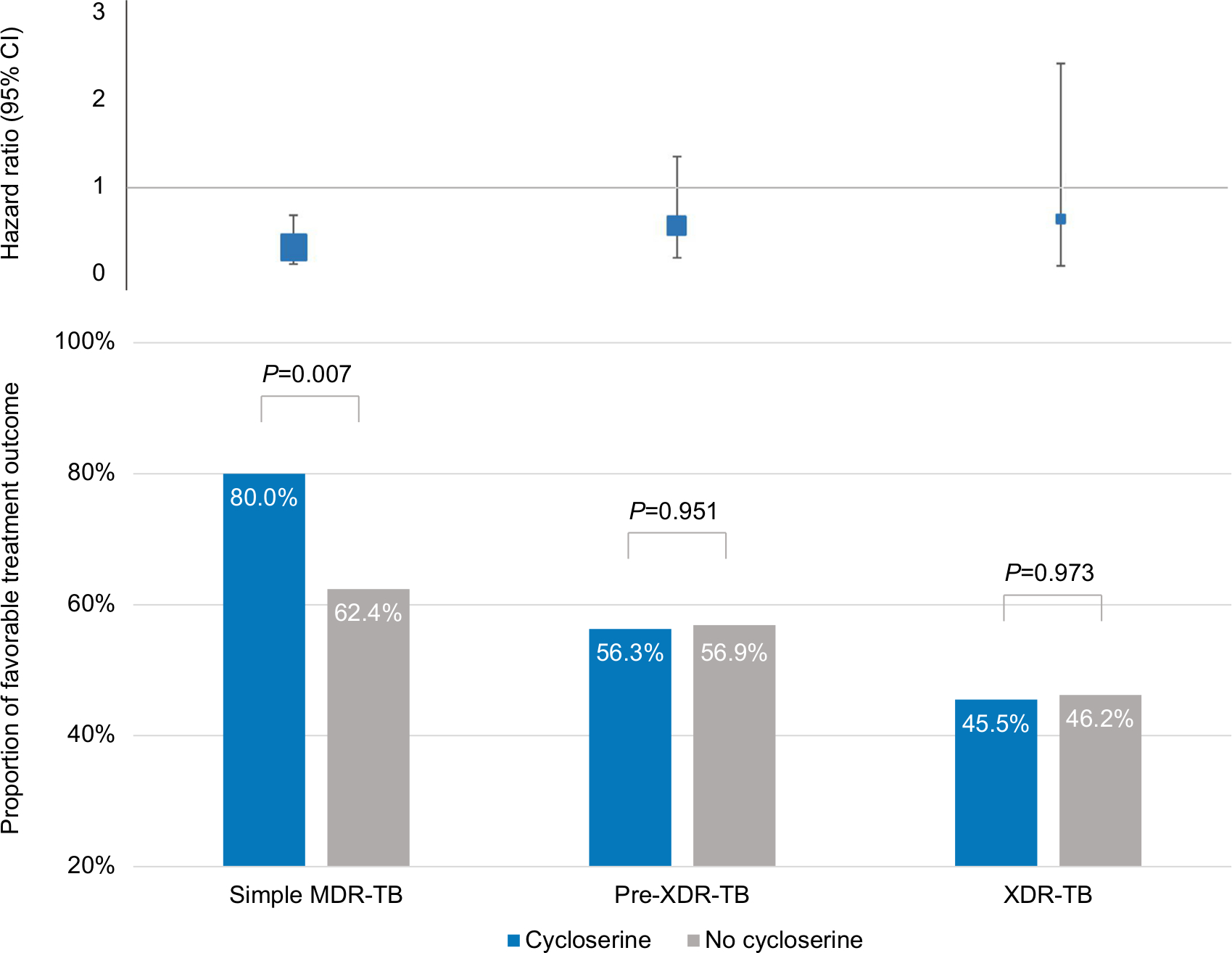 | Figure 1 Proportions of favorable treatment outcome and the HR of any unfavorable treatment outcome after the introduction of cycloserine, according to the resistance pattern among patients treated with and without cycloserine. Abbreviations: MDR-TB, multidrug-resistant tuberculosis; XDR-TB, extensively drug-resistant tuberculosis; pre-XDR-TB, pre-extensively drug-resistant tuberculosis. |
Efficacy of end point assessment
Efficacy was mainly measured by sputum culture conversion and proved to be roughly similar between the two groups. There was no difference in the proportion achieving sputum culture conversion at the end of the intensive phase (117/144, 81.3% vs 144/181, 79.6%, P=0.703) or the end of treatment (127/144, 88.2% vs 149/181, 82.3%, P=0.142) when comparing the cycloserine group and non-cycloserine group. The median (IQR) time to culture conversion was similar between the two groups (31 days vs 61 days), for a HR for conversion in the cycloserine group of 1.057 (95% CI: 0.81–1.37, P=0.679). We also calculated the sputum conversion rate at 6 months and observed no significant difference between the two groups regardless of the resistance patterns (data not shown).
Safety assessment
Overall, 132 of 144 patients (91%) in the cycloserine group and 161 of 181 patients (89%) in the non-cycloserine group had clinically significant ADRs. The most frequent adverse events were gastrointestinal effects (nausea and vomiting), arthralgia, liver injury, and hypokalemia in both treatment groups (Figure 2). Among the 132 patients reporting adverse events in the cycloserine group, 37 (28%) experienced major adverse effects and 95 (72%) patients experienced minor side effects. The adverse events attributed to cycloserine are shown in Table 3. Side effects that were possibly or probably related to cycloserine appeared after a median of 71 days (range 10–331 days) of cycloserine treatment. A total of 16 patients reported 17 episodes related to cycloserine, including nine patients who discontinued cycloserine temporarily or permanently. We observed eight episodes of headache, and cycloserine was permanently withdrawn from the treatment regimen in two patients. Moreover, two cases of seizure, one case of depression, and two cases of anxiety were observed, with these events resulting in cycloserine discontinuation within the first 6 months of treatment. No suicidal ideation was observed.
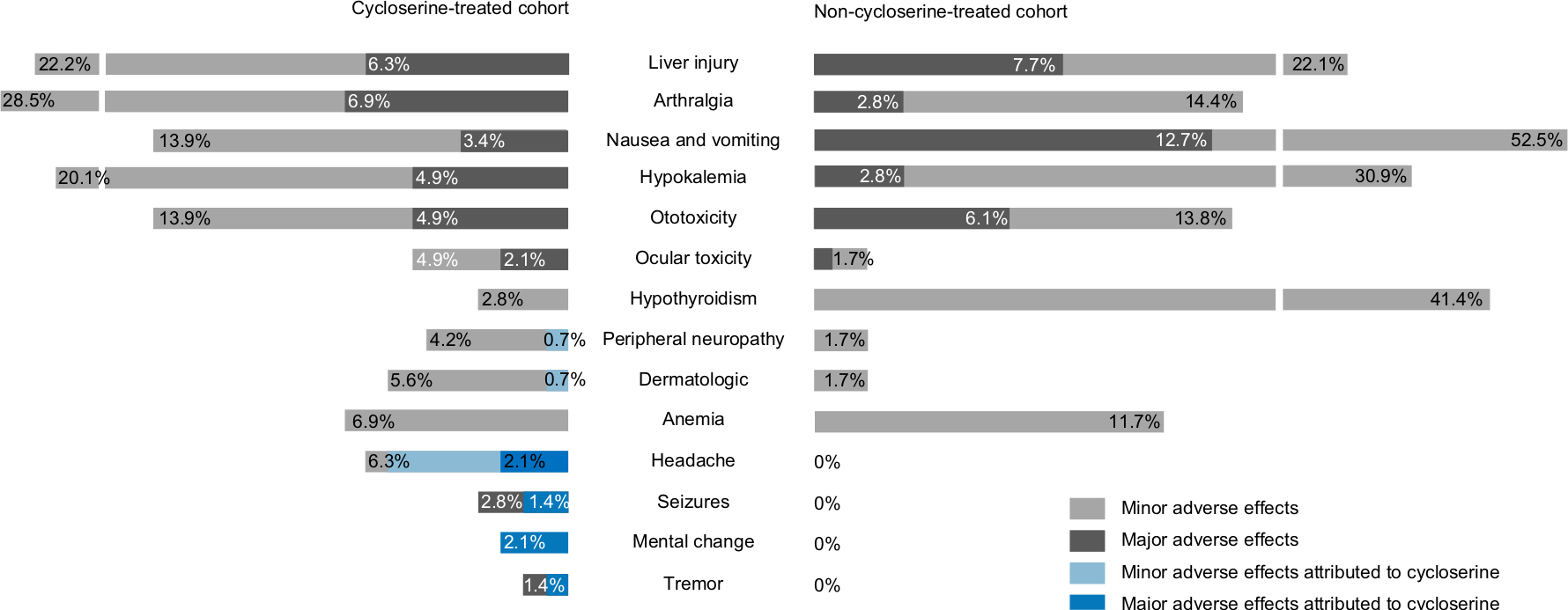 | Figure 2 Adverse drug reactions in patients with and without cycloserine treated for multidrug-resistant tuberculosis in China. Notes: Adverse drug reactions which were associated with cycloserine are marked in sky blue (minor adverse effects) or navy blue (major adverse effects). |
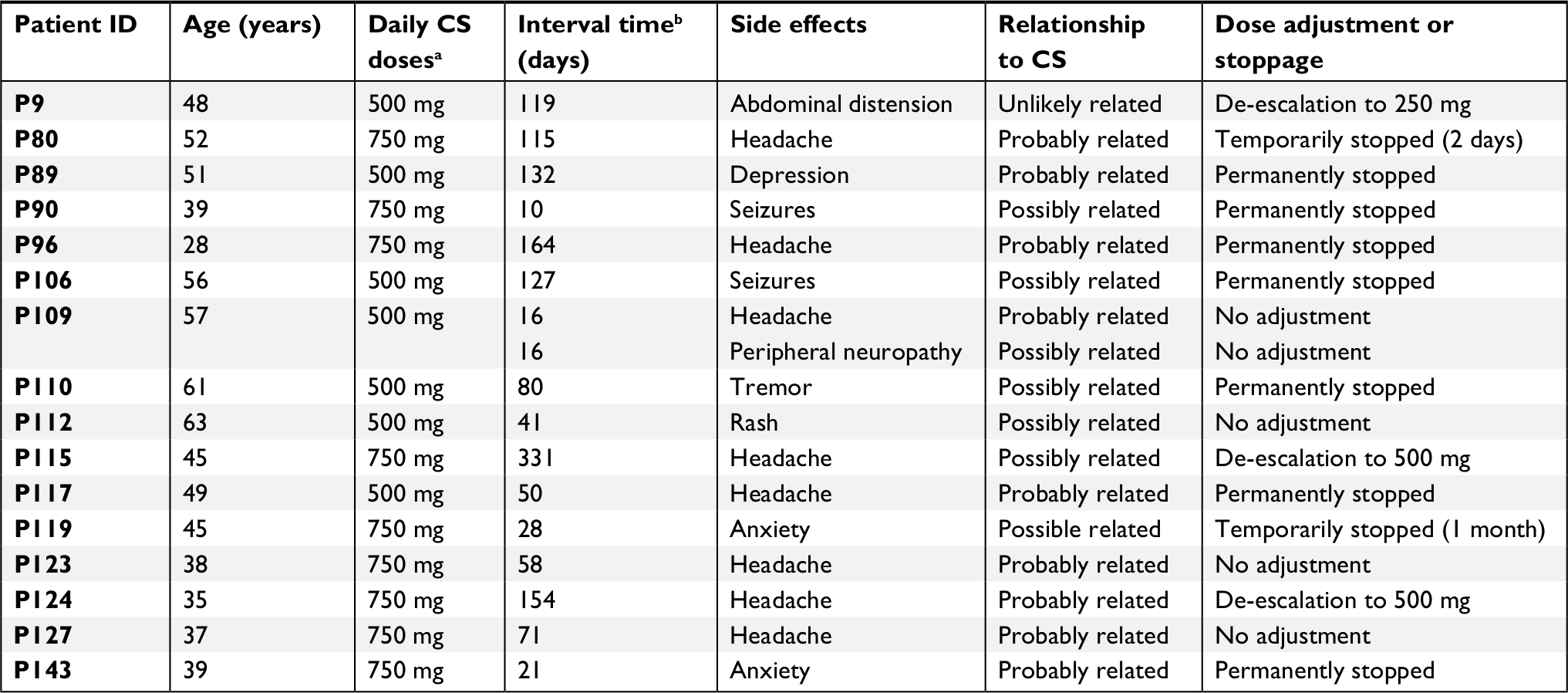 | Table 3 Side effects associated with cycloserine or requiring to withdraw cycloserine Notes: aDaily CS doses refer to the doses in the background regimen. bInterval time from start of therapy to appearance of side effects (days). Abbreviation: CS, cycloserine. |
Risk factors to unfavorable treatment outcomes
The associations between unfavorable treatment outcomes and each baseline variable were first assessed using a univariate Cox regression model (Table S1). Using a Cox regression analysis (Table 4), we found that a significant risk of unfavorable treatment outcomes was related to age greater than 60 years (HR: 2.40, 95% CI: 1.36–4.22; P=0.002), the presence of a cough before starting treatment (HR: 2.48, 95% CI: 1.14–5.11; P=0.022), resistance to fluoroquinolones proven by drug-susceptibility testing (HR: 2.05, 95% CI: 1.24–3.38; P=0.005), and the individualized treatment regimen (HR: 1.66, 95% CI: 1.01–2.63; P=0.048).
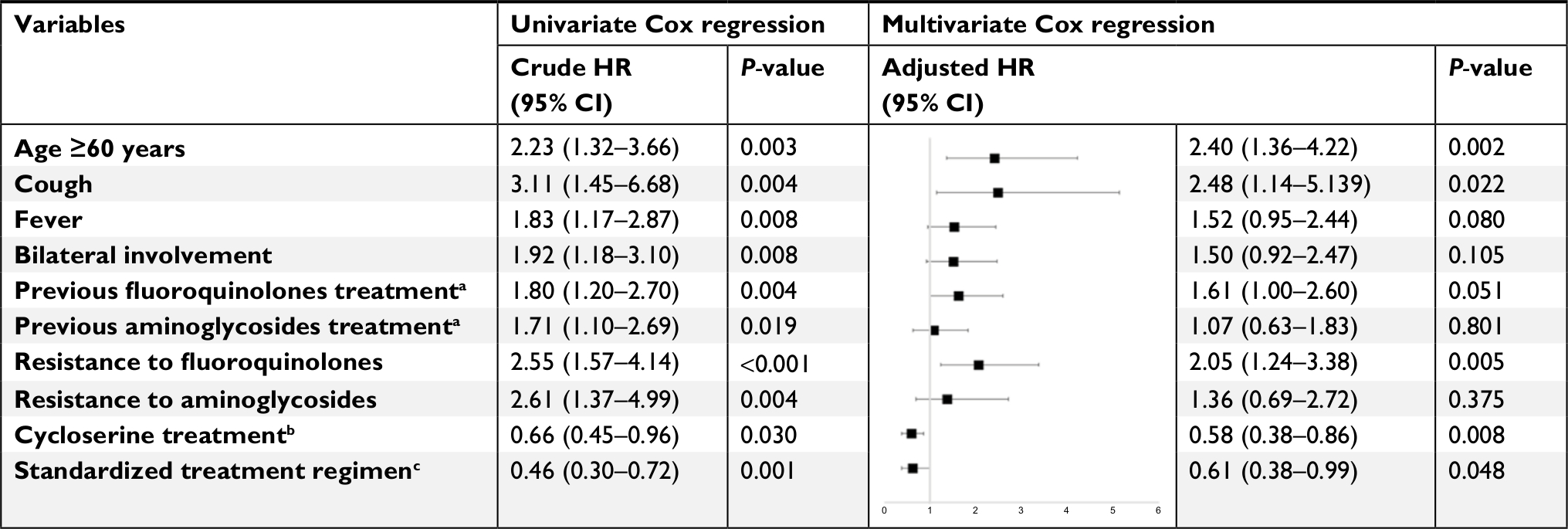 | Table 4 Cox regression analysis of potential independent variables associated with unfavorable treatment outcome in multidrug-resistant tuberculosis cases Notes: aTreated with fluoroquinolones or aminoglycosides more than 30 days before. bTreated with cycloserine, pyrazinamide, clarithromycin, high-dose isoniazid, or amoxicillin-clavulanate as the baseline regimen. cStandardized treatment regimen included a later-generation fluoroquinolone, pyrazinamide, prothionamide, an aminoglycoside, and cycloserine, or else para-aminosalicylic acid. |
Discussion
The weaknesses and intolerability of current regimens brought more than half of DR-TB patients to treatment failure. The arrival of novel drugs such as delamanid and bedaquiline has offered fresh opportunities.16,17 However, up to now, there are insufficient new drugs to compose an entirely new regimen, so that the effective use of existing tools is urgently needed to combat MDR-TB.
The evaluation of cycloserine is greatly hampered by the paucity and weakness of the existing evidence. To our knowledge, this is the first study with a control group aimed at defining or optimizing the role of cycloserine in MDR-TB treatment. Our study suggested a significant trending toward improved treatment outcome after the introduction of cycloserine. When exploring the role of cycloserine for patients with different resistance patterns, we observed a significant improvement in treatment outcomes related to cycloserine in simple MDR-TB patients. However, for complicated MDR-TB patients, cycloserine alone was of less benefit without more effective drugs, such as linezolid and bedaquiline,14,18 indicating the requirement for reprioritization of cycloserine and new or repurposed agents when managing highly resistant forms of TB. Another interesting fact was that no association was found between the resistance to injectable agents and unfavorable treatment outcome, while the resistance to the fluoroquinolones may well give rise to treatment failure, which may suggest that fluoroquinolones are more critical for the treatment of MDR-TB (Table 4).
Our data reported an overall treatment success rate of 69.4% within 24 months in the patients treated with cycloserine. Previous studies reported that the successful outcome rate ranged from 67.5% to 77.0%,19–21 which was in accordance with our findings. There are several possible reasons to explain these subtle differences. First, the definition of treatment outcome has been updated and further emphasizes the tolerability of the regimens which was likely to be underappreciated before. Second, some studies combined adjunctive therapy such as surgical resection, which resulted in improved treatment outcomes.20,21 Moreover, the accelerated development of pre-XDR-TB and XDR-TB probably reduces the treatment success rate.
Currently, MDR-TB treatment outcome assessments need to integrate efficacy end points and safety end points. Efficacy end points in this study were mainly measured by time to and proportion of sputum culture conversion. Unlike drug-susceptible TB, failure to sputum conversion rather than relapse or sputum reversion accounted for a greater proportion of treatment failure,23 suggesting that the regimen in this study might not show strong sterilizing activity. Our study did not provide the evidence that cycloserine could confer a benefit to culture conversion. A possible explanation for this finding is that treatment of MDR-TB includes multiple drugs, and an observational study without strict placebo controls hardly assesses the efficacy of a single agent. Furthermore, a recent study has shown that more than half of patients with the recommended dosage of 10 mg/kg of cycloserine prescription had peak serum concentrations lower than the minimum inhibitory concentrations of the strains isolated from the corresponding patients, suggesting the need for adjusting each patient’s dosages depending on the clinical pharmacokinetic and pharmacodynamic assessments.24,25
ADR remains problematic during the treatment course of MDR-TB patients. By contrast with other anti-TB agents, ADR attributed to cycloserine was relatively uncommon, with a frequency of 11.1%. Consistent results were found in a meta-analysis that estimated the frequencies of any ADR from cycloserine at 9.1% (95% CI: 6.4–11.7).26 Neuropsychiatric reactions, as expected, were representative of adverse effects of cycloserine, since its central active mechanism as a partial NMDA-agonist and high brain–blood barrier permeability.27 In this study, headache was one of the most common side effects of cycloserine, although most headaches resolved quickly while seizures were rare, mainly associated with high dosages,28 co-administration of fluoroquinolones, and alcoholism,27 but all led to the withdrawal of cycloserine. Psychiatric disturbances were also described on rare occasions in our study but were more complicated to manage for clinicians. In greater detail, depression or anxiety might be partly attributable to the inadequate social support and lack of confidence owing to previous poor treatment outcomes, such as the patient (P89), who was suffering from depression and had been infected with M. tuberculosis for more than 8 years and suffered complications post-TB destroyed lung and complained of unbearable arthralgia during the treatment. A major challenge is the lack of reference standard against which to evaluate drug-induced psychiatric events. However, the current psychiatric reactions to cycloserine are mainly based on case reports,29 and further controlled studies are now needed.
Limitations
This retrospective study has several limitations. First, the major limitations derive from the observational study design, which precluded us from controlling confounding bias and other drugs in the background regimen and addressing some important topics, especially pharmacokinetic and pharmacodynamic assessments of cycloserine. Second, some strains isolated from patients were missing and thus we did not perform the drug susceptibility testing to cycloserine. Moreover, as cycloserine had not been approved in China until 2014, its availability and affordability require further evaluation.
Conclusion
The introduction of cycloserine improved the overall favorable outcome of MDR-TB patients. Cycloserine is considered a better-tolerated agent with infrequent adverse side effects characterized by neuropsychiatric reactions. For simple MDR-TB patients, we believe our results support the use of cycloserine in the setting of correct patient assessment and monitoring. For complicated MDR-TB patients, more effective treatment options should be considered.
Data availability
Individual participant data after deidentification that underlie the results reported in the article could be shared from 12 months following article publication for 2 years. Study documents could be available immediately after publication. The data set could only be shared with investigators who provide a methodologically sound proposal for individual participant data meta-analysis. Proposals should be directed to [email protected]. Data requestors will need to sign a data access and proposals do not necessarily mean it will be assented.
Acknowledgments
We thank all patients for affording their treatment profiles and all health care workers who participated in this effort. This study is funded by Zhejiang-National Committee of Health and Family Planning Co-Sponsored Project (WKJ-ZJ-07).
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Shah NS, Wright A, Bai GH, et al. Worldwide emergence of extensively drug-resistant tuberculosis. Emerg Infect Dis. 2007;13(3):380–387. | ||
World Health Organization. WHO global tuberculosis report 2017. Geneva: World Health Organization; 2017. | ||
Bruning JB, Murillo AC, Chacon O, Barletta RG, Sacchettini JC. Structure of the Mycobacterium tuberculosis D-alanine:D-alanine ligase, a target of the antituberculosis drug D-cycloserine. Antimicrob Agents Chemother. 2011;55(1):291–301. | ||
Epstein IG, Nair KG, Boyd LJ. Cycloserine, a new antibiotic, in the treatment of human pulmonary tuberculosis: a preliminary report. Antibiotic Med Clin Ther. 1955;1(2):80–93. | ||
Somner AR, Brace AA. Ethionamide, pyrazinamide and cycloserine used successfully in the treatment of chronic pulmonary tuberculosis. Tubercle. 1962;43(4):345–360. | ||
Cohen AC. Pyridoxine in the prevention and treatment of convulsions and neurotoxicity due to cycloserine. Ann N Y Acad Sci. 1969;166(1):346–349. | ||
Crofton Sir J, Chaulet P, Maher D. Guidelines for the management of drug-resistant tuberculosis. Trans R Soc Trop Med Hyg. 1997;91:15–17. | ||
World Health Organization. Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis. Geneva: World Health Organization; 2008:12–185. | ||
World Health Organization. Rapid Communication: Key Changes to Treatment of Multidrug-and Rifampicin-Resistant Tuberculosis (MDR/RR-TB). Geneva: World Health Organization; 2018. | ||
Wang X, Fu Q, Li Z, et al. Drug-resistant tuberculosis in Zhejiang Province, China, 1999–2008. Emerg Infect Dis. 2012;18(3):496–498. | ||
Zhang L, Meng Q, Chen S, et al. Treatment outcomes of multidrug-resistant tuberculosis patients in Zhejiang, China, 2009–2013. Clin Microbiol Infect. 2018;24(4):381–388. | ||
Sun F, Li Y, Chen Y, et al. Introducing Molecular Testing of Pyrazinamide Susceptibility Improves MDR-TB Treatment Outcomes: A Prospective Cohort Study. Eur Respir J. 2018: 1801770. | ||
Eurosurveillance editorial team. Revised definitions and reporting framework for tuberculosis. Euro Surveill. 2013;18(16):20455. | ||
Migliori GB, Eker B, Richardson MD, et al. A retrospective TBNET assessment of linezolid safety, tolerability and efficacy in multidrug-resistant tuberculosis. Eur Respir J. 2009;34(2):387–393. | ||
World Health Organization. Policy guidance on drug-susceptibility testing (DST) of second-line antituberculosis drugs. Geneva: World Health Organization; 2008:1–20. | ||
Ferlazzo G, Mohr E, Laxmeshwar C, et al. Early safety and efficacy of the combination of bedaquiline and delamanid for the treatment of patients with drug-resistant tuberculosis in Armenia, India, and South Africa: a retrospective cohort study. Lancet Infect Dis. 2018;18(5):536–544. | ||
Diacon AH, Pym A, Grobusch MP, et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N Engl J Med. 2014;371(8):723–732. | ||
Caminero JA, Piubello A, Scardigli A, Migliori GB. Bedaquiline: how better to use it. Eur Respir J. 2017;50(5):e1701670. | ||
Prasad R, Verma SK, Sahai S, Kumar S, Jain A. Efficacy and safety of kanamycin, ethionamide, PAS and cycloserine in multidrug-resistant pulmonary tuberculosis patients. Indian J Chest Dis Allied Sci. 2006;48:183–186. | ||
Tahaoğlu K, Törün T, Sevim T, et al. The treatment of multidrug-resistant tuberculosis in Turkey. N Engl J Med. 2001;345(3):170–174. | ||
Masjedi MR, Tabarsi P, Chitsaz E, et al. Outcome of treatment of MDR-TB patients with standardised regimens, Iran, 2002–2006. Int J Tuberc Lung Dis. 2008;12:750–755. | ||
Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment of extensively drug-resistant tuberculosis. N Engl J Med. 2008;359(6):563–574. | ||
Cegielski JP, Dalton T, Yagui M, et al. Extensive drug resistance acquired during treatment of multidrug-resistant tuberculosis. Clin Infect Dis. 2014;59(8):1049–1063. | ||
Yu X, Zeng X, Shi W, et al. Validation of cycloserine efficacy in treatment of multidrug-resistant and extensively drug-resistant tuberculosis in Beijing, China. Antimicrob Agents Chemother. 2018;62(3):e01824-17. | ||
Hung WY, Yu MC, Chiang YC, et al. Serum concentrations of cycloserine and outcome of multidrug-resistant tuberculosis in Northern Taiwan. Int J Tuberc Lung Dis. 2014;18(5):601–606. | ||
Hwang TJ, Wares DF, Jafarov A, Jakubowiak W, Nunn P, Keshavjee S. Safety of cycloserine and terizidone for the treatment of drug-resistant tuberculosis: a meta-analysis. Int J Tuberc Lung Dis. 2013;17(10):1257–1266. | ||
Schade S, Paulus W. D-cycloserine in neuropsychiatric diseases: a systematic review. Int J Neuropsychopharmacol. 2016;19(4):pyv102. | ||
Holmes CX, Martin GE, Fetterhoff KI. The role of the cycloserine (seromycin) blood level in the treatment of pulmonary tuberculosis and the prevention and control of cycloserine (seromycin) toxicity. Dis Chest. 1959;36(6):591–593. | ||
Sharma B, Handa R, Nagpal K, Prakash S, Gupta PK, Agrawal R. Cycloserine-induced psychosis in a young female with drug-resistant tuberculosis. Gen Hosp Psychiatry. 2014;36(451):e3–e4. |
Supplementary material
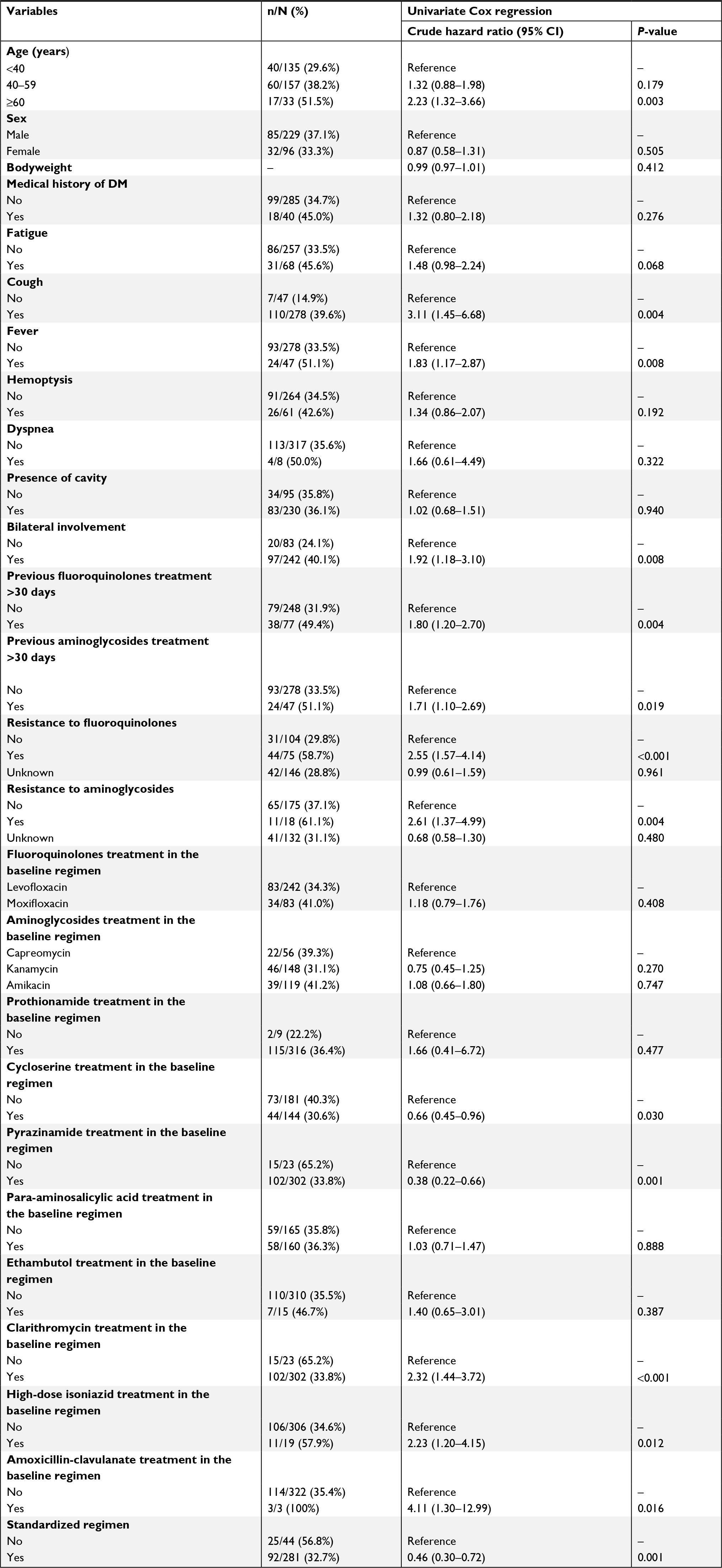 | Table S1 Univariate Cox regression analysis of potential independent variables associated with unfavorable treatment outcome in multidrug-resistant tuberculosis cases Abbreviation: DM, diabetes mellitus. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.