Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Cutaneous Tuberculous Sinus Tract: A Case Report
Authors Gu J ![]() , Chen S, Ye M, Tian Y
, Chen S, Ye M, Tian Y ![]() , Chen X, Cheng H
, Chen X, Cheng H ![]() , Li T
, Li T ![]()
Received 18 December 2025
Accepted for publication 6 March 2026
Published 16 March 2026 Volume 2026:19 583065
DOI https://doi.org/10.2147/CCID.S583065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Jiefang Gu,1 Siyan Chen,1 Maogen Ye,1 Ye Tian,2 Xian Chen,3 Hongbin Cheng,4 Tianhao Li4
1Department of Dermatology, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Department of Dermatology, Sichuan Second Hospital of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 3Department of Pathology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 4Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
Correspondence: Tianhao Li, Department of Dermatology, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected] Hongbin Cheng, Department of Dermatology, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China, Email [email protected]
Abstract: An 88-year-old female patient presented with a persistent ulcer in the right flank region following incision and drainage of an abscess. After the relevant examinations and debridement procedures, a deep internal sinus tract approximately 2– 3 cm in length was discovered, extending to the lateral border of the external intercostal muscles. Based on local histopathological examination including the tuberculosis PCR, the condition was diagnosed as a cutaneous tuberculous sinus tract caused by Mycobacterium tuberculosis infection. Cutaneous tuberculosis is a relatively uncommon form of extrapulmonary tuberculosis, primarily affecting the skin and subcutaneous soft tissues. The patient has recovered well following an anticipated nine-month course of triple anti-tuberculosis therapy without pyrazinamide. To date, no literature reports have documented persistent deep skin fistulas resulting from this disease.
Keywords: Mycobacterium tuberculosis complex, chronic sinus, deep-seated, skin infection
Introduction
Cutaneous tuberculosis is an infectious skin disease caused by Mycobacterium tuberculosis. Due to its diverse and insidious manifestations, early recognition and diagnosis pose significant challenges for clinicians. Meanwhile, Mycobacterium tuberculosis infection manifesting as deep-seated sinus tracts is even rarer, with no related reports identified. We now report a case of cutaneous Mycobacterium tuberculosis infection involving a deep tuberculous sinus tract that penetrated through the serratus anterior muscle to reach the external intercostal muscle.
Case Report
An 88-year-old woman presented to the dermatology department with a lump on the right flank area for more than a year. Over a year ago, the patient developed a pinhead-sized lump in the right flank area accompanied by mild stabbing pain. Subsequently, the lump gradually enlarged with increasing pain, eventually presenting scattered pustules at its apex. Concurrently, the affected skin area exhibited elevated temperature and marked tenderness. Following incision and drainage of the abscess on the skin lesion, the surgical incision failed to heal and developed into an ulcer. The patient has a history of hypertension spanning over 10 years and a history of cerebral infarction lasting more than one year, denying any other chronic medical conditions, and no relevant family history of infectious disease has been identified.
On physical examination, a deep ulcer of about 3 by 2.5 centimeters with indistinct borders is visible in the right flank area, amounts of curd-like white secretions and necrotic tissue is visible deep within the ulcer, surrounded by dark red edges. During debridement and exploration, multiple deep ulcer cavities were identified, with the deepest measuring approximately 2 to 3 centimeters.
Blood tests showed LYMPH 0.82*109cells/L, LYMPH% 18%, ALB 36.6 g/L, TBA 12.2 μmol/L, HIV-Ag/Ab (-). Color Doppler ultrasound of the superficial mass indicates ulceration extending to the superficial layer of the external intercostal muscles. The plain CT scan image of the upper abdomen reveals the lesions close to the superficial layer of the ribs (Figure 1A). No significant abnormalities were observed in other regular laboratory tests.
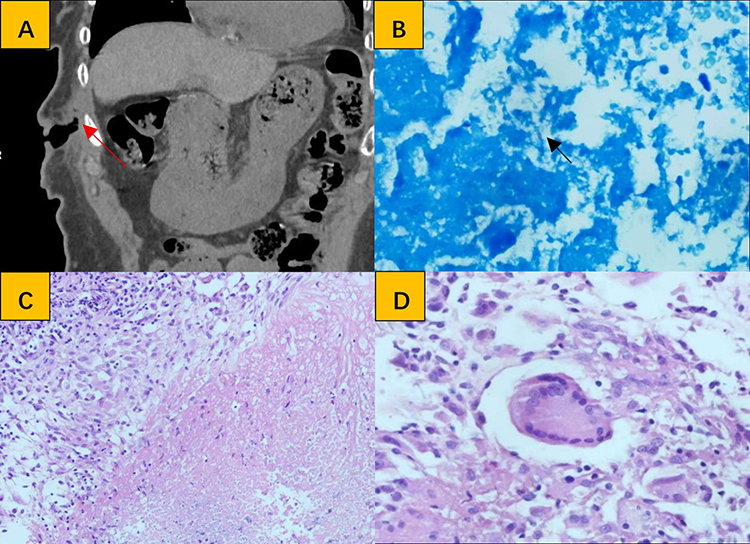 |
Figure 1 Imaging examinations and histological features. (A) Abdominal CT scan in the coronal plane. A deep sinus tract extending to the external intercostal muscles (red arrow). (B) Acid-fast staining shows a suspected positive result (black arrow) (FAB×600). (C) Clearly uniform areas of eosinophilic caseous necrosis and proliferating granulation tissue, with epithelioid cells in the surrounding areas can be seen (HE×200). (D) Multinucleated clusters of foreign-body reactive inflammatory giant cells (HE×400). |
Initial treatment involves intravenous infusion of cefuroxime sodium for anti-infection, supplemented by regular dressing changes with saline solution and povidone-iodine. Secretions and necrotic tissue were collected for acid-fast staining and histopathological examination, and the acid-fast staining indicates a suspicious positive finding (Figure 1B). Pathology findings revealed chronic inflammation (predominantly caseous necrosis, epithelioid cells, and foreign body reaction) (Figures 1C and Figures 1D). Pending TB-DNA testing to rule out tuberculosis. Final Report: Tuberculosis. PCR: Mycobacterium tuberculosis complex (MTBC-DNA) positive (reference value: CT value: 24.86). Final diagnosis: Cutaneous tuberculous sinus tract. We continue to refine chest CT and tuberculosis infection T-cell testing to rule out pulmonary tuberculosis and systemic tuberculosis infection. Considering the potential occurrence of related adverse reactions and the patient’s advanced age, we modified the standard anti-tuberculosis regimen to a 9-month course of lower-dose triple anti-tuberculosis therapy. This consists of oral administration of 200 mg isoniazid tablets, 300 mg rifampicin capsules, and 500 mg ethambutol hydrochloride tablets once daily, while continuing the treatment of dressing change.
The patient presented at our hospital on September 2, 2025, and received a definitive diagnosis of the disease via pathological examination on September 5 (Figure 2A). Following several days of initial treatment and our careful consideration of treatment options, the patient ultimately commenced the aforementioned definitive treatment regimen on September 11 and was discharged after experiencing clinical improvement. The patient returned for follow-up appointments on October 19, 2025, and January 4, 2026, showing significantly reduced pain and a shallower sinus tract with healing of the wound surface, indicating favorable recovery (Figure 2B and C).
 |
Figure 2 Clinical Features. (A) Dermatological lesion in the right flank region. (B) The patient returned for a follow-up visit 1 month later, showing a shallower sinus tract and reduced inflammation. (C) Approximately 4 months later, the wound had largely healed, with only minor residual erythema and hyperpigmentation remaining. And the pain sensation had disappeared. |
Discussion
Lungs are the most common site of infection for Mycobacterium tuberculosis. Extrapulmonary tuberculosis accounts for approximately 8% to 24% of all tuberculosis cases, with cutaneous tuberculosis representing 1.5% to 3% of these cases.1 Tuberculosis infection of the skin typically presents with insidious and diverse manifestations, making it prone to being overlooked or misdiagnosed, and this contributes to the diagnostic challenges associated with the disease.2 Cutaneous tuberculosis can be classified into endogenous and exogenous forms based on the route of infection. This infection can occur in individuals of any age or gender. Cutaneous infections caused by Mycobacterium tuberculosis can manifest in any form on any part of the human body surface, commonly presenting as cutaneous lupus vulgaris, verrucous cutaneous tuberculosis, tuberculous chancroid, and other skin manifestations. Relevant literature indicates that a very small proportion of Mycobacterium tuberculosis skin infections may manifest as persistent, difficult-to-heal ulcers and superficial tract fistulas occurring in locations such as the perineum, scalp, fingers, and soles of the feet.3–6 These conditions have been controlled through treatment with oral anti-tuberculosis treatment alone or in combination with surgical excision. However, no reports have been published regarding the formation of such deep-seated skin fistulas resulting from this kind of infections.
We speculate that in this case, the initial skin infection of the patient with Mycobacterium tuberculosis was localized and had not yet penetrated deeper layers. However, the elderly patient’s compromised immune system was unable to effectively control the pathogen. Concurrently, the repetitive back-and-forth displacement of the chest wall during respiration may have facilitated the gradual invasion of the subcutaneous lesion toward deeper layers. Combined with delayed diagnosis and treatment, these factors ultimately led to the lesion reaching the superficial layer of the external intercostal muscles. This demonstrates the deep extent of the lesion’s invasion and the significant challenges in managing this case.
Based on the patient’s condition and physical status, the final treatment plan confirmed to be a 9-month course of oral triple anti-tuberculosis therapy (excluding pyrazinamide), combined with regularly dressing change to thoroughly clear pus and necrotic tissue from the sinus tract. Given that this patient is 88 years old and has underlying conditions such as hypertension, simultaneously refer to the 2023 expert consensus on diagnosis and treatment of elderly pulmonary tuberculosis published in the Chinese Journal of Tuberculosis and Respiratory Diseases,7 we opted for a 9-month triple anti-tuberculosis regimen without pyrazinamide as the primary treatment, which based on the long-term and prudent considerations. Additionally, considering of the deep nature of the sinus tract, we combined oral anti-tuberculosis medications with regular dressing changes which involves thorough saline irrigation and pus drainage of the deep sinus tract to reduce the accumulation of necrotic material that impedes skin lesion repair. After 1 month of the above treatment, the patient’s pain and cutaneous condition showed significant improvement. And we will continue to monitor the patient’s subsequent recovery progress until the full recovery.
Conclusion
Our patient has had a lump in the right flank region for over a year, yet the condition has not received the attention it deserves, which caused the delay of diagnosis and expansion of the infection site which is deep to the lateral border of the external intercostal muscle without regular and standardized treatment. Due to the deep location of the site of lesion, incomplete drainage and debridement, coupled with the failure to identify the cause of infection, the patient’s skin lesion was difficult to heal. After the anti-tuberculosis treatment and regularly dressing changes, the patient’s pain has significantly decreased, and the sinus tract is continuing to heal.
We represented a rare case of deep-seated cutaneous tuberculous sinus tract caused by with the Mycobacterium tuberculosis complex infection. Based on the patient’s medical history and clinical presentation, supplemented by pathological examination, acid-fast staining, and tuberculosis PCR testing, we ultimately confirmed the diagnosis in this case. Early detection and diagnosis are of great benefit to the treatment of this disease and the patients suffering from it. We recommend more clinical training to improve clinicians’ diagnostic capabilities for similar diseases.
Abbreviations
PCR, Polymerase chain reaction; MTBC, Mycobacterium tuberculosis complex.
Ethics Statement
After thorough communication and obtaining the patient’s verbal consent for publication, considering the patient’s physical condition, the patient authorized her legal guardian (i.e., the patient’s daughter) to sign the relevant documents. And written informed consent for publication of the patient’s clinical details and clinical images was obtained from the legal guardian (i.e., the patient’s daughter). Institutional approval is not required for the publication of this case report.
Acknowledgments
I would like to express my sincere gratitude to all those who have contributed to and supported my research, without whose insights, encouragement, and assistance this case report would not have been possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed.
Funding
This work was supported by the Science and Technology Research Special Project of Sichuan Administration of Traditional Chinese Medicine (25MSZX130).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kaul S, Kaur I, Mehta S, et al. Cutaneous tuberculosis. Part I: pathogenesis, classification, and clinical features. J Am Acad Dermatol. 2023;89(4):1091–5. doi:10.1016/j.jaad.2021.12.063
2. Chen Q, Chen W, Hao F. Cutaneous tuberculosis: a great imitator. Clin Dermatol. 2019;37:192–199. doi:10.1016/j.clindermatol.2019.01.008
3. Yu J, Huang W, Zhang G, et al. Vulvar ulcerative cutaneous tuberculosis secondary to genital tract tuberculosis. An Bras Dermatol. 2022;97:786–788. doi:10.1016/j.abd.2021.11.004
4. Hassunuma Carneiro B, Gama Palone A, C ACZ, et al. Cutaneous tuberculosis on the scalp: a case report. Infez Med. 2021;29(2):263–267.
5. Dhar A, Khan UH, Shabir A, et al. Tuberculosis of finger presenting as non-healing ulcer of digit: a case report. Cureus. 2022;14(9). doi:10.7759/cureus.29426
6. Tharun Ganapathy C, George NM, Selvamuthukumaran S, et al. An interesting case report of cutaneous tuberculosis of the foot. Int J Surg Case Rep. 2022;100. doi:10.1016/j.ijscr.2022.107763
7. Chinese Society for Tuberculosis, Chinese Medical Association. Expert consensus on diagnosis and treatment of elderly pulmonary tuberculosis. Chin J Tuberc Respir Dis. 2023;46(11):1068–1084. doi:10.3760/cma.j.cn112147-20230921-00182
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.