Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Cutaneous-to-Bronchial Rosai–Dorfman Disease without Lymphadenopathy: A Rare Case Report and Literature Review
Authors Bogomolets O ![]() , Hryshchenko R
, Hryshchenko R ![]() , Berezkin O, Bogomolets-Sheremetieva S, Svystak A
, Berezkin O, Bogomolets-Sheremetieva S, Svystak A
Received 25 October 2025
Accepted for publication 8 February 2026
Published 11 March 2026 Volume 2026:19 576795
DOI https://doi.org/10.2147/CCID.S576795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Olga Bogomolets,1,2 Roman Hryshchenko,3 Oleksandr Berezkin,4 Sofiia Bogomolets-Sheremetieva,3 Anna Svystak3
1Faculty of Medicine, Academy of Silesia in Katowice, Zabrze, Poland; 2Department of Military General Practice – Family Medicine, Ukrainian Military Medical Academy, Kyiv, Ukraine; 3Department of Dermatology, Dr. Bogomolets Institute of Dermatology and Cosmetology, Kyiv, Ukraine; 4Dermpathlab, Bogomolets Medical Laboratories, Kyiv, Ukraine
Correspondence: Olga Bogomolets, Academy of Silesia in Katowice, 43 ul. Rolna, Zabrze, Poland, Tel +380 800 332 500, Email [email protected]
Abstract: Rosai–Dorfman disease (RDD) is a rare non-Langerhans cell histiocytosis that typically presents with massive cervical lymphadenopathy and systemic manifestations. The cutaneous form is usually limited to the skin and rarely progresses to systemic involvement. Timely confirmation of the diagnosis of RDD in cases of progression to systemic involvement is a challenge for the health care system. We report a 23-year-old woman with a history of COVID-19 infection and subsequent mRNA vaccination who developed acneiform eruptions on her face and at the vaccination site on her shoulder. Biopsies confirmed cutaneous RDD without lymphadenopathy. After more than one year of a purely cutaneous course, she developed cough and dyspnea. Imaging revealed an isolated bronchial lesion without lymph node involvement; histology confirmed RDD. The patient responded to local corticosteroid injections and systemic glucocorticoids, with stabilization of the disease. Our report underscores the importance of considering RDD in persistent acneiform eruptions unresponsive to treatment and bronchial masses without lymphadenopathy.
Keywords: rosai–dorfman disease, cutaneous rosai–dorfman disease, bronchial involvement, lymphadenopathy-negative, acneiform presentation, COVID-19 vaccination
Introduction
Rosai–Dorfman disease (RDD) is a rare non–Langerhans cell histiocytosis with an unclear etiology.1 The estimated prevalence of RDD is approximately 1 in 200,000 individuals.2 Classical RDD typically presents with bilateral cervical lymphadenopathy; however, extranodal involvement occurs in approximately 43% of cases.1 Bronchial involvement is among the rarest extranodal localizations. When present, it is usually accompanied by nodal or other systemic disease, whereas isolated airway lesions without lymphadenopathy are exceedingly rare.3
To date, no cases in which purely cutaneous RDD (CRDD) has progressed to bronchial disease in the absence of lymphadenopathy have been reported. The cutaneous form is regarded as a distinct clinicopathologic variant that is typically confined to the skin, without systemic symptoms or lymph node enlargement. CRDD often mimics other dermatologic conditions—such as acne, rosacea, granulomatous dermatoses, or cutaneous lymphoma—which can lead to delayed or incorrect diagnosis.4,5
Because of the potential for RDD to mimic other conditions, skin biopsy remains crucial for an accurate diagnosis. The possible role of COVID-19 infection and vaccination as trigger factors in RDD is currently under discussion.6,7 Up to 10% of patients with Rosai–Dorfman disease die as a result of direct disease-related complications, secondary infections, or amyloidosis.8 Most patients present with nonspecific signs and symptoms to their primary care providers and are often referred to various subspecialists on the basis of their clinical presentation.9 RDD represents an abnormal proliferation of histiocytes and may manifest as an isolated condition or in association with other diseases. Its diagnosis requires an integrated clinical, radiologic, pathologic, and molecular approach. Histopathological examination reveals characteristic features of abnormal S100+, CD68+, and CD1a− histiocytes, often demonstrating variable degrees of emperipolesis.10 Computed tomography (CT) and magnetic resonance imaging (MRI) may assist in the detection of disease involvement; however, histopathological confirmation remains essential for establishing a definitive diagnosis of RDD.11
Manifestations of Rosai–Dorfman disease (RDD) may mimic various other conditions, including lymphomas, myelodysplastic syndrome (MDS), solid tumors, tuberculosis, non-tuberculous mycobacterial (NTM) infections, melanoma, and Sjögren’s syndrome, among others.10,12–16 RDD is not uncommonly associated with other histiocytic neoplasms, benign lymphoproliferative disorders, autoimmune diseases, viral infections, or malignancies.10,17
No standardized treatment protocol has been established for RDD, and therapeutic strategies are best individualized according to clinical presentation. Surgical excision, corticosteroid therapy, and observation are among the most commonly employed approaches.1
The aim of this paper is to present a unique case of transformation from purely cutaneous RDD to multisystem extranodal involvement, discuss COVID-19 infection and vaccination as potential triggering factors, and review diagnostic and therapeutic strategies. We also aim to raise awareness among physicians regarding the potential for purely cutaneous RDD to progress to systemic extranodal disease. Early recognition of this progression may help reduce diagnostic delays, guide the selection of appropriate treatment options, and improve patient outcomes.
Materials and Methods
Examination, treatment, and follow-up of the patient were conducted at the Department of Dermatology of the Dr. Bogomolets Institute of Dermatology and Cosmetology in Kyiv, Ukraine. Clinical history was obtained from medical records and patient interviews.
Ultrasound examination was performed using a LOGIQ E R8 ultrasound scanner (GE HealthCare) with a linear transducer operating at 1–22 MHz. Dermoscopy was conducted with a FotoFinder medicam 1000s digital video dermatoscope (FotoFinder Systems, Germany).
Formalin-fixed, paraffin-embedded (FFPE) tissue samples were processed using standard protocols for diagnostic histological examination. Sections were cut using a Microm HM355S rotary microtome (Thermo Fisher Scientific, US) and mounted on poly-L-lysine-coated adhesive microscopy slides (catalog number TYI01, Nantong Tianye Labware Co., Ltd).
For qualitative evaluation of tissue morphology, Series S Staining Products, including Gill-3 Hematoxylin, Alcoholic Eosin, Bluing Reagent, and Nu-Clear (Epredia, US) were used.
Immunohistochemistry (IHC) was performed using a ready-to-use anti-S100 antibody (clone 4C4.9, Vitro S.A., Spain) on the PT Module platform with Shandon™ Plastic Coverplates (Epredia, US), employing the Master Polymer Plus Detection System with Peroxidase and DAB chromogen (Vitro S.A., Spain). Where applicable, S100 expression was semi-quantitatively assessed using the H-score: strong expression was defined as an H-score of 2 or 3, weak expression was defined as 1, and no expression was defined as 0.
Written informed consent was obtained from the patient for the publication of clinical data and photographs. All procedures complied with the ethical standards of the Declaration of Helsinki.
A literature review was conducted via the PubMed database using the following keyword combinations: “cutaneous Rosai-Dorfman disease”, “facial Rosai-Dorfman disease”, “pulmonary Rosai-Dorfman disease”, “bronchial Rosai-Dorfman disease”, “COVID-19 Rosai-Dorfman disease”, “COVID-19 vaccination Rosai-Dorfman disease”, “diagnostics Rosai-Dorfman disease”, and “treatment Rosai-Dorfman disease”.
Case Presentation
A 24-year-old Caucasian woman presented to the dermatology clinic with nodular lesions on both cheeks and left arm (Figure 1). The patient had no known allergies and no history of acne during adolescence. In October 2020, the patient had a confirmed mild case of COVID-19. In July 2021 and August 2021, she received two doses of the MODERNA COVID-19 vaccine. The post-vaccination period was difficult, particularly after the first dose, with fatigue, fever, nausea, and a brief episode of syncope.
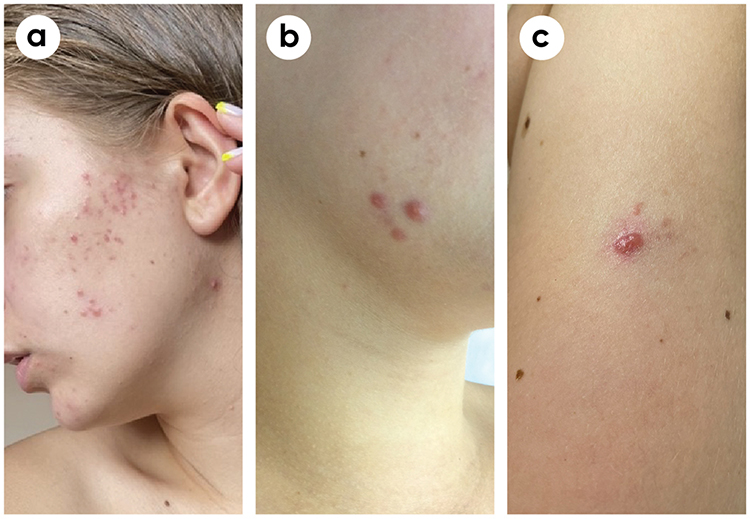 |
Figure 1 Nodular lesions on both cheeks and the left arm. (a) Moderate inflammatory papules and pustules with a few nodules on both cheeks. (b) Inflammatory nodules on the right cheek. (c) Solitary nodular lesion on the left arm. |
The first lesions appeared in October 2022 as small pustules on the cheeks. A diagnosis of acne was made, and the lesions gradually regressed by January 2023 following topical treatment at another clinic. In July 2023, the rash on the cheeks recurred, preceded by itching (Figure 2a). The morphology of the rash changed: the lesions became larger and nodular, particularly on the left cheek. Simultaneously, new lesions appeared on the left shoulder at the site of COVID-19 vaccination. A diagnosis of acne conglobata was made, and local treatment with a combination of topical adapalene and clindamycin was initiated. Despite temporary improvement, the lesions did not resolve. In September 2023, the number and size of nodules on the left cheek increased (up to six lesions) (Figure 2b).
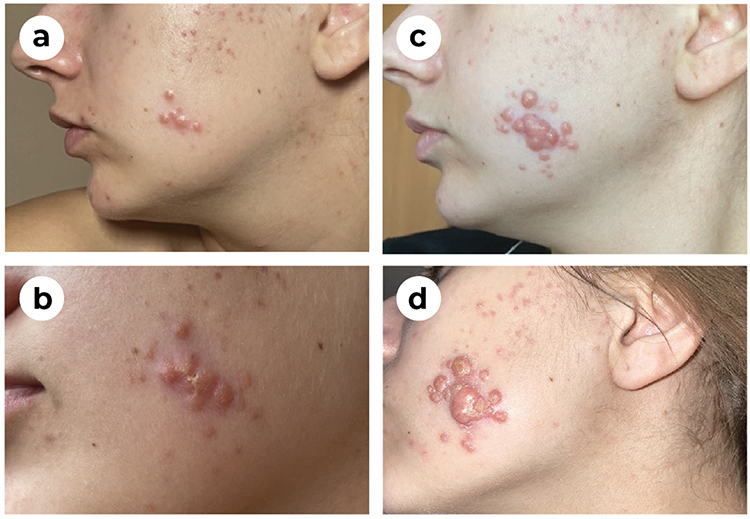 |
Figure 2 Progression of lesions on the right cheek. (a) Progression of lesions with multiple papules and pustules showing a tendency to merge. (b) The formation of painful nodular lesions indicates a transition to a nodulocystic form. (c) Persistence of nodules with dense infiltration and a reduction in small pustules. (d) Active deep nodules with pronounced swelling and conglobation on the left cheek. |
The patient sought care at a different clinic, where a dermatologist prescribed oral doxycycline at a dose of 100 mg per day for one month. Concurrently, a topical combination of azelaic acid and adapalene was also prescribed.
In October 2023, the patient developed spontaneous onset of cough and wheezing. Otherwise, she remained generally well, with no fever or lymphadenopathy. A punch biopsy was obtained from the lesion on the left cheek. Histopathological examination confirmed the diagnosis of Rosai–Dorfman disease (Figure 3). Despite the histological confirmation of RDD, treatment targeting acne has continued in the same clinic. The patient was prescribed systemic clindamycin hydrochloride 355.03 mg daily for 10 days and a combination of ethinylestradiol 0.035 mg with cyproterone acetate 2 mg for three subsequent menstrual cycles.
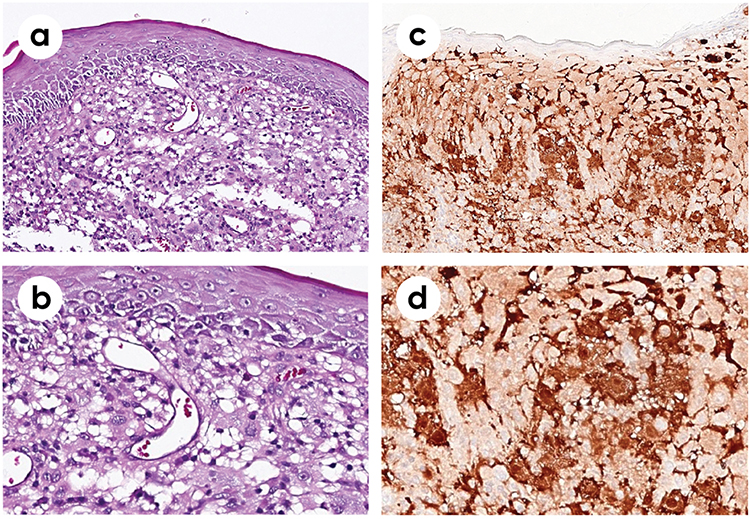 |
Figure 3 Histopathological findings. (a) Epidermotropic and intradermal epithelioid cells (H&E stain, ×20 magnification). (b) Epidermotropic and intradermal epithelioid cells (H&E stain, ×40 magnification). (c) S100 protein (clone 4C4.9) positivity in epidermotropic and intradermal epithelioid cells (×20 magnification). (d) S100 protein (clone 4C4.9) positivity in epidermotropic and intradermal epithelioid cells (×40 magnification). |
In December 2023, following a chemical peeling procedure, lesion exacerbation occurred with crust formation (Figure 2c). Serological tests for IgM antibodies to cytomegalovirus, herpes simplex virus types 1 and 2, and varicella-zoster virus were negative. IgM and IgG antibodies against Epstein–Barr virus were also negative.
Inflammatory and endocrine markers, including C-reactive protein, total IgE, dehydroepiandrosterone sulfate, prolactin, progesterone, thyroid-stimulating hormone, thyroxine, and triiodothyronine, were within normal ranges. An elevated erythrocyte sedimentation rate of 24 mm/h was noted. Other laboratory parameters were unremarkable.
In January 2024, the patient developed allergic dermatitis affecting the axillary and inguinal regions. Oral suprastin 25 mg was prescribed for three days, resulting in complete resolution of the lesions. In five days, physical examination, dermoscopy, and ultrasound evaluation were performed at the Dr. Bogomolets Clinic (Figures 4 and 5). An intralesional injection of triamcinolone acetonide (0.01 mL) was administered, and topical mometasone furoate ointment was prescribed for one month. A second intralesional injection of triamcinolone acetonide (0.5 mL) was performed on January 23, 2024, and it targeted the lesion on the left cheek. The third injection (1 mL) was administered in February 2024.
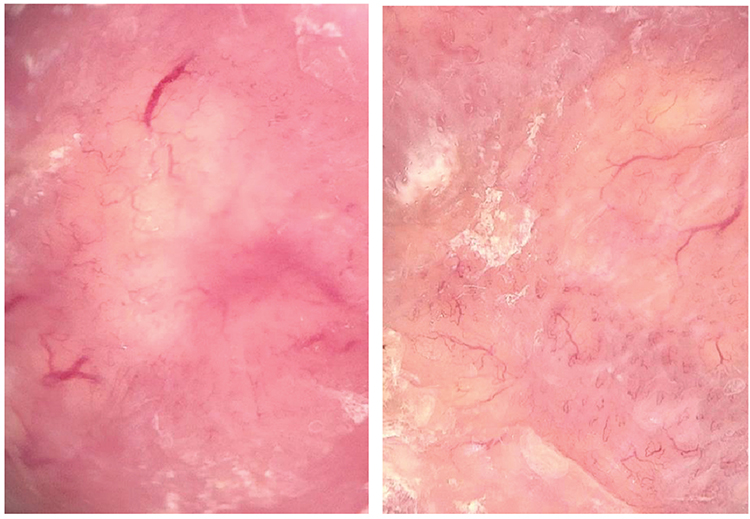 |
Figure 4 Dermoscopic findings. Erythematous background with multiple polymorphic vessels of varying caliber. Rounded yellow structures are visible both centrally and peripherally, along with faint white ribbon-like structures distributed throughout the lesion. |
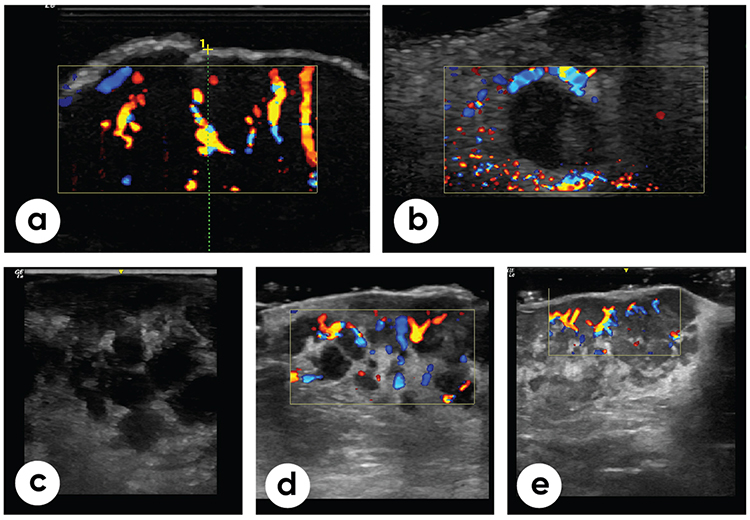 |
Figure 5 Ultrasound examination findings. (a and b) Lesion (infiltrate) of irregular or rounded shape with well-defined margins; anechoic. Color Doppler mode revealed increased diffuse vascularization (January 2024). The yellow frame delineates the region of interest activated in the color Doppler imaging mode, within which the vascularization of the lesion is assessed. The green dotted line and numeric markers indicate linear measurements and are used to determine the dimensions of the lesion. (c) The lesion (infiltrate) was irregular in shape and hypoechoic. Anechoic rounded or irregular structures resembling cysts are present, with clear contours, and are separated by hyperechoic strands. Diffuse vascularization was observed in color Doppler mode (May 2024). (d) The lesion (infiltrate) was irregular in shape and heteroechoic. Anechoic rounded or irregular cyst-like structures with clear contours were demarcated by hyperechoic strands. Increased diffuse vascularization was observed in color Doppler mode (November 2024). The yellow frame delineates the region of interest activated in the color Doppler imaging mode, within which the vascularization of the lesion is assessed. (e) The lesion (infiltrate) was irregular in shape, heteroechoic and had ill-defined borders. Hypoechoic irregular structures with clear contours, demarcated by hyperechoic strands. Color Doppler mode shows increased diffuse vascularization (December 2024). The yellow frame delineates the region of interest activated in the color Doppler imaging mode, within which the vascularization of the lesion is assessed. |
A repeated biopsy with immunohistochemical analysis (S100+, CD68+, and CD1a–) confirmed the diagnosis of Rosai–Dorfman disease. Imaging, including contrast-enhanced computed tomography (CT) and positron emission tomography-computed tomography (PET-CT), revealed a bronchial mass measuring 72×51 × 56 mm in the absence of lymphadenopathy. A second episode of allergic dermatitis, which is clinically similar to the previous episode, occurred. This time, the patient suspected parsley as a potential allergen.
In May 2024, an intralesional injection of triamcinolone acetonide (0.3 mL) was administered to the lesion on the left arm, and radiowave excision of the cheek lesions was performed. Topical tacrolimus 0.1% ointment was prescribed for three months.
In September 2024, the patient experienced a severe allergic reaction to ambrosia pollen, presenting with coughing, sneezing, and conjunctivitis. Antihistamines were ineffective, but the symptoms resolved spontaneously after the patient’s emigration. A follow-up multislice computed tomography (MSCT) scan revealed progression of the bronchial lesion, which remained histologically consistent with Rosai–Dorfman disease.
According to the hematologist’s recommendation, systemic treatment with methylprednisolone was initiated as follows: 64 mg daily for 25 days, then 48 mg for 14 days, 32 mg for 14 days, 16 mg for 14 days, 8 mg for 14 days, and 4 mg for 7 days.
By May 2025, no disease progression or emergence of new lesions was observed (Figure 2d). Follow-up PET-CT revealed a single persistent bronchial lesion that was unchanged in size or location since initial detection, with no evidence of systemic involvement.
Clinically, the patient remained stable under ongoing steroid tapering and local therapy. Respiratory symptoms were absent, and the patient reported noticeable improvement within the first few days of methylprednisolone treatment.
Discussion
Our patient was diagnosed with extranodal multisystem Rosai–Dorfman disease (RDD) involving both the skin and the intrathoracic region. Extranodal involvement is reported in approximately 43% of RDD patients, whereas multisystem disease is observed in approximately 19%, with a prognosis closely linked to the number of extranodal sites affected. Cutaneous involvement occurs in approximately 10% of extranodal RDD presentations. Intrathoracic RDD is exceedingly rare, reported in only 2% of patients, and typically presents alongside lymphadenopathy.1 These data underscore the exceptional rarity of our case, particularly given the isolated bronchial localization without nodal involvement.
Cutaneous Rosai–Dorfman disease (CRDD) is typically indolent, confined to the skin, and only rarely progresses to systemic involvement.8 Our case therefore represents an unprecedented trajectory: more than a year of purely cutaneous disease followed by isolated bronchial involvement.
Several aspects make this case unique. First, the persistent absence of lymphadenopathy distinguishes it from classical systemic RDD, which almost invariably presents with massive, painless cervical lymphadenopathy. Second, the sequential coexistence of two rare localizations — cutaneous and bronchial — has not been previously reported. Third, the acneiform onset initially mimicked acne conglobata, underscoring the importance of early biopsy in atypical or treatment-resistant eruptions.4,5
Bronchial involvement in RDD is exceedingly rare. When present, it typically manifests with chronic cough, wheezing, and airway obstruction and is often misdiagnosed as a malignancy. The development of an isolated bronchial lesion without nodal involvement after a prolonged cutaneous course, as observed in our patient, expands the recognized clinical spectrum of RDD and highlights the necessity for long-term systemic monitoring in CRDD patients.
It remains unclear whether the initial episode of disseminated acneiform lesions in our patient was related to RDD. Several published cases have described RDD presenting with numerous disseminated acneiform eruptions across different body regions.4,18,19 It is plausible that the initial lesions in our patient — which spontaneously resolved — may also have represented cutaneous RDD. Spontaneous resolution of CRDD lesions has been previously documented.20
Although psychological stress is not an established etiological factor in RDD, it may influence immune regulation and histiocytic behavior, potentially contributing to disease onset or progression.
Likewise, both COVID-19 infection — with its associated cytokine storm — and mRNA vaccination may modulate immune and histiocytic responses.21,22
The authors of two previously published cases hypothesized that COVID-19 infection was a potential trigger for RDD development.6,23 In the first case, the patient presented with generalized lymphadenopathy, with the inguinal node being the largest.6 In the second case, a 54-year-old woman developed a scleral nodule and lymphadenopathy following COVID-19.23
Another case described a 62-year-old man who developed pruritic papules on his legs after the first dose of COVID-19 vaccination. Following the second dose, the lesions gradually spread to the trunk and upper limbs, and RDD was subsequently confirmed. The patient had no enlarged lymph nodes throughout the disease course.24 Another published case described a patient who developed RDD following COVID-19 mRNA vaccination and subsequent COVID-19 infection. This patient presented with bilateral cervical, axillary, and inguinal lymphadenopathy, accompanied by fatigue and weight loss.7
The differences and similarities between the two cases are summarized in Table 1.
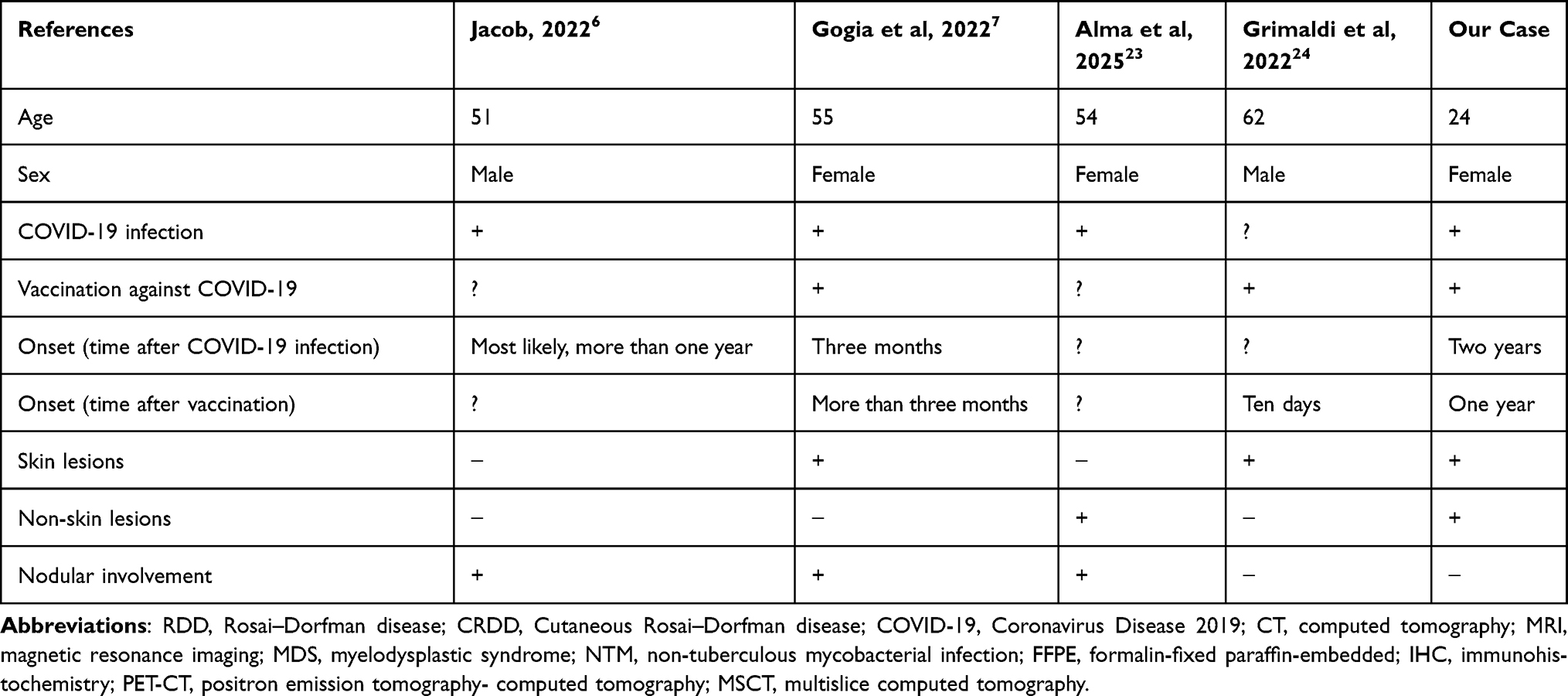 |
Table 1 Comparison of Age, Sex, History of COVID-19 Infection and Vaccination, Onset of Rosai–Dorfman Disease Following COVID-19 Infection and/or Vaccination, Presence of Cutaneous and Extracutaneous Lesions, and Nodal Involvement in Our Case and Previously Published Cases Presumably Related to COVID-19 Infection and/or Vaccination |
Our patient was vaccinated nine months after a mild COVID-19 infection and experienced post-vaccination reactions, particularly after the first dose, followed by the appearance of rashes on the left shoulder at the injection site. However, her first cutaneous lesions appeared approximately two years after the initial infection and more than one year after vaccination.
Therefore, although a causal relationship between COVID-19 infection or vaccination and RDD in our patient remains uncertain, it cannot be excluded. This long latency makes a direct causal link difficult to prove.
Notably, the first episodes of allergic reactions in our patient were also reported after COVID-19 infection and subsequent vaccination. While some studies have shown no significant changes in the overall prevalence or diagnosis rates of chronic allergic diseases before and after the pandemic,25 other data suggest that the risk of developing allergic diseases beyond the first 30 days after COVID-19 diagnosis significantly increases. Although this risk gradually decreases over time, it may persist for at least 6 months and correlates with disease severity.
In contrast, two doses of the COVID-19 vaccine have been shown to have a protective effect against the development of allergic diseases.26 Similar findings have been reported in the context of autoimmune diseases: Peng et al demonstrated that COVID-19 infection is associated with an increased risk of various autoimmune disorders, and that COVID-19 vaccination may attenuate this risk.27 Nearly all patients with allergic skin diseases can be vaccinated with the registered COVID‐19 vaccines available today. Precautionary measures should be taken in a very small subgroup of patients, especially in those with possible severe allergy to ingredients of the vaccine.28
On the basis of the above-mentioned literature, and despite the patient reporting a mild course of COVID-19 and more pronounced reactions to vaccination, it appears that COVID-19 infection was the most likely triggering factor, potentially initiating immune dysregulation that contributed to RDD development in this case.
A published case report described a patient initially suspected of having COVID-19 pneumonia, who was ultimately diagnosed with RDD presenting as a pulmonary artery mass.29 In contrast, the bronchial RDD lesion in our patient was identified almost incidentally by imaging, as the only symptoms reported were cough and wheezing.
Although respiratory tract involvement in RDD is rare, it poses a significant diagnostic challenge.12 An analysis of 15 patients with pulmonary RDD revealed that the median interval between symptom onset and diagnosis was 24 months.3 Nevertheless, both cough and wheezing—present in our patient—are among the most commonly reported respiratory symptoms in RDD.30
Boissière et al31 described a case of RDD with pulmonary involvement and no lymphadenopathy in a 77-year-old female who presented with cough, but without cutaneous manifestations. Similarly, Wu et al32 reported a case of an 18-year-old male with cough and pulmonary RDD in the absence of both lymphadenopathy and skin lesions.
Our case is distinct in that it began as purely cutaneous RDD and subsequently progressed to systemic extranodal RDD involving the bronchial mucosa—without any lymph node involvement. The absence of lymphadenopathy, despite simultaneous cutaneous and bronchial involvement, suggests an atypical immune response pattern.
Notably, the skin and bronchial mucosa share structural and immunological features, which may facilitate localized histiocyte infiltration without lymphatic dissemination.33 Non-nodal variants of RDD have been previously described in the literature. In our case, localized immune activation—potentially triggered by prior COVID-19 infection or vaccination—may have contributed to directed histiocyte migration toward mucosal tissues.10,21
Altered chemokine and cytokine profiles (eg, CCL2, and IL-6) may promote bronchial involvement independently of the lymphatic system. These findings support the hypothesis that cutaneous RDD can, in rare cases, evolve into mucosal or systemic extranodal forms without concomitant lymphadenopathy.
A recent systematic review proposed a management algorithm for cutaneous Rosai–Dorfman disease (CRDD), in which surgical excision, observation, and topical corticosteroids are considered first-line options for solitary lesions. In contrast, systemic corticosteroids and/or methotrexate are preferred in cases of multifocal disease.20 The same review reported that surgical excision was the most frequently employed intervention (51 patients), achieving complete response in 48 patients. Systemic corticosteroids were administered in 32 patients, with 20 patients achieving complete or partial response.
The optimal duration of systemic therapy for RDD remains undefined. A treatment course of 6 to 12 months followed by observation—assuming good tolerance and a good clinical response—is generally considered reasonable. Upon initiation of systemic therapy, the first assessment of treatment response should occur within 4 months; if the disease remains stable or in remission, the surveillance interval may be extended to 12 months.1
For our patient, a combination approach was employed. Radiowave excision, cryodestruction, and intralesional corticosteroid injections were used to treat the cutaneous lesions. Among these, intralesional corticosteroid injections are the most effective. Local corticosteroid therapy combined with systemic glucocorticoids led to stabilization of both cutaneous and bronchial lesions. These findings suggest suggests that individualized immunosuppressive regimens may be effective even in rare and complex cases of CRDD.
Absence of molecular testing in our patient may be considered as a limitation of this case.
Conclusion
We report an atypical case of progression from purely cutaneous Rosai–Dorfman disease (RDD) to extranodal multisystem involvement. Unlike the classical systemic form, which typically presents with nodal disease, our patient initially presented with acneiform cutaneous lesions without lymphadenopathy, followed by the development of isolated bronchial involvement as the only internal manifestation. This rare clinical course expands the known spectrum of Rosai–Dorfman disease and highlights the importance of long-term monitoring in patients with persistent cutaneous lesions unresponsive to standard dermatologic treatments. This case is important because it raises awareness not only among physicians but also among relevant healthcare officials and affected individuals.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Approval
The need for additional ethical approval was waived by the Local Ethics Committee of the Dr. Bogomolets Institute of Dermatology and Cosmetology, Kyiv, Ukraine (Approval No.: 280825/1; Date: August 28, 2025). No experimental treatment was involved, and all clinical data were obtained in the course of routine diagnostic and therapeutic procedures.
Informed Consent
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abla O, Jacobsen E, Picarsic J, et al. Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Blood. 2018;131(26):2877–10. doi:10.1182/blood-2018-03-839753
2. Werneck Rodrigues DO, Wolp Diniz R, Dentz LC, et al. Case study: Rosai-Dorfman disease and its multifaceted aspects. J Blood Med. 2024;15:123–128. doi:10.2147/JBM.S436720
3. Moyon Q, Boussouar S, Maksud P, et al. Lung Involvement in Destombes-Rosai-Dorfman disease: clinical and radiological features and response to the MEK inhibitor cobimetinib. Chest. 2020;157(2):323–333. doi:10.1016/j.chest.2019.09.036
4. Shen HP, Lu ZF, Zhu JW. Granulomatous rosacea-like skin rash: extranodal Rosai-Dorfman disease. Int J Clin Exp Pathol. 2020;13(3):556–558.
5. Wongrat T, Sangmala S. Facial cutaneous Rosai-Dorfman disease: a case report. J Med Case Rep. 2024;18(1):182. doi:10.1186/s13256-024-04410-9
6. Jacob SSK. Atypical presentation of a sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman disease) with granulomas - post COVID-19 infection. IP Archiv Cytol Histopathol Res. 2022;7(2):139–141. doi:10.18231/j.achr.2022.030
7. Gogia P, Tanni F, Coca-Guzman J, et al. Case report: a rare case of Rosai-Dorfman-Destombes disease after the COVID-19 infection. Front Med. 2022;9:1073767. doi:10.3389/fmed.2022.1073767
8. Bruce-Brand C, Schneider JW, Schubert P. Rosai-Dorfman disease: an overview. J Clin Pathol. 2020;73(11):697–705. doi:10.1136/jclinpath-2020-206733
9. Goyal G, Young JR, Koster MJ, et al. The mayo clinic histiocytosis working group consensus statement for the diagnosis and evaluation of adult patients with histiocytic neoplasms: erdheim-chester disease, langerhans cell histiocytosis, and rosai-dorfman disease. Mayo Clin Proc. 2019;94(10):2054–2071. doi:10.1016/j.mayocp.2019.02.023
10. Elbaz Younes I, Sokol L, Zhang L. Rosai-Dorfman disease between proliferation and neoplasia. Cancers. 2022;14(21):5271. doi:10.3390/cancers14215271
11. Li H, Li D, Xia J, et al. Radiological features of Rosai-Dorfman disease: case series and review of the literature. Clin Radiol. 2022;77(11):e799–e805. doi:10.1016/j.crad.2022.07.008
12. Al-Maghrabi H, Elmahrouk A, Feteih M, Jamjoom A, Al-Maghrabi J. Rosai-Dorfman disease with pulmonary involvement mimicking bronchogenic carcinoma. J Cardiothorac Surg. 2020;15(1):37. doi:10.1186/s13019-020-1085-6
13. Al Umairi R, Blunt D, Hana W, Cheung M, Oikonomou A. Rosai-Dorfman disease: rare pulmonary involvement mimicking pulmonary langerhans cell histiocytosis and review of the literature. Case Rep Radiol. 2018;2018:2952084. doi:10.1155/2018/2952084
14. Hur K, Hong JY, Kim KH, et al. Facial Cutaneous Rosai-Dorfman disease: dermoscopic findings with successful surgical treatment. Ann Dermatol. 2023;35(Suppl 2):S287–S291. doi:10.5021/ad.22.071
15. Yousef YA, Al-Hussaini M, Nazzal R, Abdeen G, Alnawaiseh I, Alrawashdeh K. Rosai-Dorfman disease masquerading as uveal melanoma: case report and review of literature. Hematol Oncol Stem Cell Ther. 2020;13(4):238–241. doi:10.1016/j.hemonc.2018.05.005
16. Xu J, Huang M, Dong B, et al. Extranodal Rosai-Dorfman disease manifesting as Sjögren’s syndrome combined with panuveitis and hypertrophic pachymeningitis: a case report and review of literature. J Int Med Res. 2024;52(4):3000605241233141. doi:10.1177/03000605241233141
17. Elshikh M, Schellingerhout D, Rayan J, et al. Disease characteristics, radiologic patterns, comorbid diseases, and ethnic differences in 32 patients with rosai-dorfman disease. J Comput Assist Tomogr. 2020;44(3):450–461. doi:10.1097/RCT.0000000000000983
18. Zhang Y, Chen H. Image gallery: generalized cutaneous Rosai-Dorfman disease presenting as acneiform lesions. Br J Dermatol. 2019;180(2):e36. doi:10.1111/bjd.17260
19. Sampaio R, Silva L, Catorze G, Viana I. Cutaneous Rosai-Dorfman disease: a challenging diagnosis. BMJ Case Rep. 2021;14(2):e239244. doi:10.1136/bcr-2020-239244
20. Dhrif O, Litaiem N, Lahmar W, Fatnassi F, Slouma M, Zeglaoui F. Cutaneous Rosai-Dorfman disease: a systematic review and reappraisal of its treatment and prognosis. Arch Dermatol Res. 2024;316(7):393. doi:10.1007/s00403-024-02982-6
21. Haslbauer JD, Matter MS, Stalder AK, Tzankov A. Histomorphological patterns of regional lymph nodes in COVID-19 lungs. Pathologe. 2021;42(Suppl 1):89–97. doi:10.1007/s00292-021-00945-6
22. Craig JW, Farinha P, Jiang A, Lytle A, Skinnider B, Slack GW. Kikuchi-Fujimoto disease following COVID-19 vaccination: experience at a population-based referral center. Am J Clin Pathol. 2023;160(2):114–118. doi:10.1093/ajcp/aqad032
23. Alma N, Shambu SK, Babu K. Rosai-Dorfman disease presenting as a scleral nodule in a female with multisystem inflammatory syndrome post-COVID-19 infection. Taiwan J Ophthalmol. 2025;15(2):319–322. doi:10.4103/tjo.TJO-D-25-00009
24. Grimaldi M, Perino F, Moretta G, et al. Cutaneous Rosai-Dorfman disease after COVID-19 vaccination treated with thalidomide. Dermatol Ther. 2022;35(11):e15864. doi:10.1111/dth.15864
25. Choi S, Kim B. Comparison of the prevalence and risk factors of chronic allergic diseases before and after COVID-19: using raw data from the Korea National Health and Nutrition Examination Survey in 2019 and 2021. J Asthma. 2023;60(12):2093–2103. doi:10.1080/02770903.2023.2220791
26. Oh J, Lee M, Kim M, et al. Incident allergic diseases in post-COVID-19 condition: multinational cohort studies from South Korea, Japan and the UK. Nat Commun. 2024;15(1):2830. doi:10.1038/s41467-024-47176-w
27. Peng K, Li X, Yang D, et al. Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study. EClinicalMedicine. 2023;63:102154. doi:10.1016/j.eclinm.2023.102154
28. Ring J, Worm M, Wollenberg A, et al. Risk of severe allergic reactions to COVID-19 vaccines among patients with allergic skin diseases - practical recommendations. A position statement of ETFAD with external experts. J Eur Acad Dermatol Venereol. 2021;35(6):e362–e365. doi:10.1111/jdv.17237
29. Dronamraju V, McSurdy K, Graham R, et al. A rare case of Rosai-Dorfman disease presenting as a pulmonary artery mass in a 33-year-old female with hypoxia. Pulm Circ. 2023;13(2):e12214. doi:10.1002/pul2.12214
30. Ahsan SF, Madgy DN, Poulik J. Otolaryngologic manifestations of Rosai-Dorfman disease. Int J Pediatr Otorhinolaryngol. 2001;59(3):221–227. doi:10.1016/s0165-5876(01)00488-8
31. Boissière L, Patey M, Toubas O, et al. Tracheobronchial Involvement of Rosai-Dorfman disease: case report and review of the literature. Medicine. 2016;95(7):e2821. doi:10.1097/MD.0000000000002821
32. Wu L, Zhang Y, Guo X, et al. Primary diffuse Rosai-Dorfman disease in central airway: a case report and literature review. BMC Pulm Med. 2023;23(1):82. doi:10.1186/s12890-023-02363-1
33. Tamari M, Ver Heul AM. Neuroimmune mechanisms of type 2 inflammation in the skin and lung. Allergol Int. 2025;74(2):177–186. doi:10.1016/j.alit.2025.02.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.