Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Cutaneous and Extracutaneous Manifestations of Behçet’s Disease Linked to Its Disease Activity and Prognosis
Authors Limtong P ![]() , Chanprapaph K
, Chanprapaph K ![]() , Vachiramon V
, Vachiramon V ![]() , Ngamjanyaporn P
, Ngamjanyaporn P ![]()
Received 29 May 2020
Accepted for publication 26 July 2020
Published 25 August 2020 Volume 2020:13 Pages 639—647
DOI https://doi.org/10.2147/CCID.S265169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Preeyachat Limtong,1 Kumutnart Chanprapaph,1 Vasanop Vachiramon,1 Pintip Ngamjanyaporn2
1Division of Dermatology, Department of Internal Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Division of Allergy Immunology and Rheumatology, Department of Internal Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Kumutnart Chanprapaph Tel +66-2-2011141
Fax +66-2-2011211
Email [email protected]
Background: Behçet’s disease is a potentially fatal vasculitis disorder involving vessels in both the arterial and venous systems. Cutaneous manifestation is the most common sign in Behçet’s disease, but its relation to disease activity and prognosis is lacking.
Objective: Our study aims to determine the relationship between cutaneous, extracutaneous manifestations with Behçet’s disease activity, morbidity, and mortality.
Materials and Methods: Patients diagnosed with Behçet’s disease were identified by using the 1990 International Study Group for Behçet’s disease criteria and/or the 2014 international criteria for Behçet’s disease. Data regarding patients’ clinical manifestations, laboratory results, disease activity, and prognosis were retrieved and analyzed. Disease activity was evaluated using the 2006 Behçet’s disease current activity form (BDCAF).
Results: Of 119 patients, the mean age at diagnosis was 35.7 ± 10.7 years and 60% were female. Median disease duration was 96 months (IQR 48– 168). Minor oral ulcer at the buccal mucosa was associated with lower median BDCAF score (p = 0.003), whereas minor oral ulcer at the tonsil was related to higher BDCAF score (p = 0.024). Male gender was associated with higher cumulative dose of corticosteroids (p = 0.003) and hospitalization (OR = 2.89 (95% CI [1.10, 7.57]), p = 0.031). Ocular manifestations were related to higher dose of corticosteroids (p = 0.002) and morbidity (OR = 4.39 (95% CI [1.57, 12.29]), p = 0.005).
Conclusion: Our study suggests that different locations of minor oral ulcers help predict disease activity. Male gender and the presence of ocular manifestations resulted in less favorable outcomes for Behçet’s disease.
Keywords: aphthae, Behçet’s syndrome, oral ulcer, stomatitis, vasculitis
Introduction
Behçet’s disease (BD) is a rare but possibly fatal vasculitis disorder which can affect vessels of all sizes in both the arterial and venous systems, resulting in various clinical manifestations.1 Behçet’s disease is highly prevalent along the ancient Silk Road (Eastern Mediterranean, Middle Eastern, and Far Eastern countries). The high prevalence of Behçet’s disease in the Asian population significantly correlates with a predilection for the HLA-B51 allele. The disease onset is usually in the 3rd to 4th decade of life. It is found equally in both genders, with a slight male preponderance among the Middle Eastern and Mediterranean countries and female preponderance in the Far Eastern populations such as Japanese and Koreans.2
The hallmarks of Behçet’s disease are recurrent oral ulcer and genital ulcer as well as ocular involvements.3,4 Behçet’s disease can also present with other cutaneous manifestations such as erythema nodosum (EN)-like lesions, papulopustular eruptions, and small-to-medium-sized cutaneous vasculitis, and positive pathergy test result.2,5,6 Although the natural course of Behçet’s disease is acute with multiple recurrent episodes of attack, different organ involvement results in variable disease activity and outcomes. Unlike the self-limiting nature of oral and genital ulcers, extracutaneous manifestations can lead to potentially significant morbidity and mortality.3,7,8 The mortality rate of Behçet’s disease can vary from 0.9% to 10%, and is mainly determined by major organ vasculitis and neurological involvement.9
Cutaneous manifestation is the earliest, readily visible, and the most common sign found in Behçet’s disease. To date, there is no information on the association between cutaneous manifestation as a prognostic indicator for Behçet’s disease. The aims of our study were to find the associations between cutaneous and extracutaneous features and Behçet’s disease activity as well as to identify factors related to the disease morbidity and mortality.
Materials and Methods
Study Design and Setting
This study was a retrospective analytical study conducted at the dermatology and rheumatology clinics of a university-based hospital (Ramathibodi Hospital, Mahidol University, Bangkok, Thailand).
Study Population
Patients diagnosed with Behçet’s disease by the International Statistical Classification of Disease and Related Health Problems 10th Revision (ICD-10) – World Health Organization Version 2016 from January 2008 to July 2018 were allocated into the study. All patients were diagnosed and followed up by board-certified dermatologists and/or rheumatologists. The inclusion criteria were patients diagnosed with Behçet’s disease according to the 1990 International Study Group for Behçet’s disease (ISG) criteria10 and/or the 2014 international criteria for Behçet’s disease (ICBD).11 ISG criteria were defined by the presence of recurrent oral aphthae for at least 3 times/year with at least two of the following criteria: recurrent genital ulcers, ocular manifestation, skin involvement, and a positive pathergy test result. The ICBD comprises the presence of recurrent oral aphthae, recurrent genital ulcers, ocular manifestations (each equals a score of 2), skin lesions, vascular involvement, central nervous system (CNS) involvement, and positive pathergy test result (each satisfies a score of 1). The score summation of at least 4 was the cut-off value for the diagnosis of Behçet’s disease (4 = probable Behçet’s disease, 5 = highly likely Behçet’s disease, and 6 = almost certainly Behçet’s disease). Patients with a minimal follow-up duration of 3 months were included in the study. The exclusion criteria were patients whose final diagnoses were inconsistent with Behçet’s disease and those with incomplete medical records.
Data Collection and Assessment
Data concerning the age of onset, gender, duration of disease, follow-up time, cutaneous manifestations categorized by types and locations of lesion, pathergy test result, extracutaneous manifestations (ocular, neurological, gastrointestinal, articular, vascular, and cardiac manifestations), laboratory results, treatment modalities, disease activity, and prognosis (evaluated in three aspects: cumulative dose of corticosteroids throughout the disease course, morbidity in terms of hospitalization, and mortality) were retrieved and analyzed.
The Behçet’s disease current activity form 2006 (BDCAF)12 was applied in our study to evaluate the disease activity at the presence of mucocutaneous lesions, incorporating clinical features present within the past 4 weeks prior to assessment. These following clinical features were required for the evaluation: headache, mucocutaneous manifestations, joint involvement, gastrointestinal symptoms, ocular abnormalities, neurological features, and major vascular involvement.
Follow-up duration was calculated by the interval between the first date of visit and the last date of follow-up or death. The presence of clinical manifestations was assessed as “yes" or “no" according to the following definitions. Oral ulcers were categorized as minor oral ulcers (ulcers of 1–5 in number, size < 1 cm, no scarring, healed in 2 weeks), major oral ulcers (ulcers of 1–10 in number, size > 1 cm, scarring, healed in 2–6 weeks), and herpetiform oral ulcers (crops of numerous small 2–3 mm ulcers).6,7 Ocular manifestations were defined as the presence of any of the following diagnoses made by ophthalmologists: uveitis, iridocyclitis, keratitis, episcleritis, scleritis, vitritis, vitreous hemorrhage, retinal vasculitis, retinal vein occlusion, and optic neuritis.7,13 Neurological involvement was determined by the presence of the following abnormalities: parenchymal brain disease (Neuro-Behçet), dural venous sinus thrombosis, arterial vasculitis, and aseptic meningitis.14,15 Gastrointestinal involvement was characterized by the presence of abdominal pain, gastrointestinal ulcers, or vasculitis.7,16 Joint involvement was defined by the presence of arthritis or arthralgia.7 The presence of deep vein thrombosis, arterial thrombosis, or pulmonary aneurysm was defined as vascular manifestations.17 Cardiac involvement included the presence of any of the following: pericarditis, myocarditis, endomyocarditis, valve abnormalities, intracardiac thrombosis, endomyocardial fibrosis, cardiomyopathy, and coronary artery lesions.17 Morbidity was defined by any hospital admission due to Behçet s disease.
Statistical Analysis
All data analyses were performed using Stata Version 14.0 (StataCorp, College Station, TX, USA). Categorical variables were expressed as a percentage, while continuous variables demonstrated as mean ± SD for data with normal distribution and median (interquartile range, IQR) for data with non-normal distribution. Logistic regression analysis and quantile regression analysis were utilized for evaluation of associations between categorical variables and continuous variables, respectively. Moreover, multiple regression analysis was applied to the variables which were found statistically significant. A p-value of less than 0.05 was considered statistically significant.
Results
A total 139 patients were diagnosed with Behçet’s disease. Twenty were excluded due to insufficient score on the diagnostic criteria (ICBD score ≤ 3) (n = 11) and incomplete medical records (n = 9), leaving 119 remaining patients eligible for the study. Sixty-two patients (52.1%) met both the ISG and ICBD criteria. Fifty-seven patients (47.9%) met the ICBD but did not meet the ISG criteria. Details regarding the study protocol are provided in Figure 1. Patients’ demographics, cutaneous manifestations, extracutaneous manifestations, morbidity, and mortality are shown in Tables 1–2.
 |
Table 1 Demographic and Clinical Data of Patients with Behçet’s Disease |
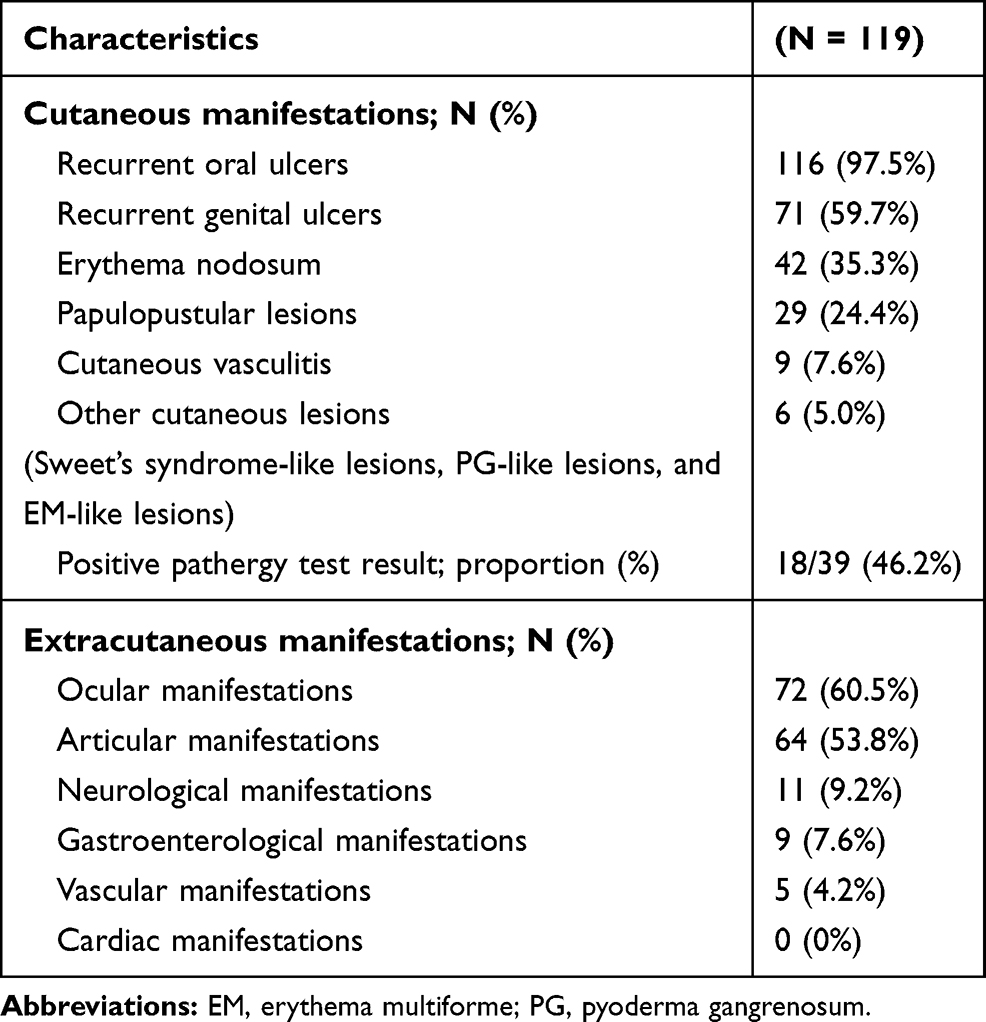 |
Table 2 Frequency of Cutaneous and Extracutaneous Manifestations of the Patients with Behçet’s Disease |
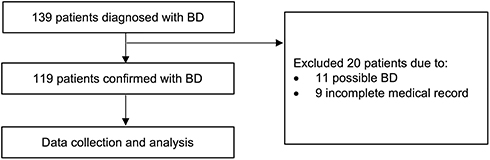 |
Figure 1 Recruitment process and the study flow diagram. |
Cutaneous Manifestations
Of 119 patients, 116 patients (97.5%) had recurrent oral ulcers (Figures 2–3). Seventy-one (59.7%) had recurrent genital ulcers (Figures 4–5), and 42 (35.3%) had EN-like lesions (Figure 6). Among 93 patients with a definitive type of oral ulcers, minor oral ulcers were present in 89 patients (95.7%) and were most commonly located on the tongue (60.0%), buccal mucosa (53.9%), and lips (41.5%). While major oral ulcers were reported less frequently in 11 patients (11.8%), mainly found on the tongue (54.6%), buccal mucosa (45.5%), and lips (36.4%). Both types of oral ulcer occurred simultaneously in 7 patients (7.5%). No herpetiform lesions were reported. Of 8 male patients reporting genital ulcers, 6 (75.0%) had involvement on the scrotum and 4 (50.0%) on the penis. Among 12 female patients with genital ulcer, all had lesions on the vulva and 1 (8.3%) had concomitant vaginal involvement.
 |
Figure 2 A recurrent oral ulcer on the buccal mucosa. |
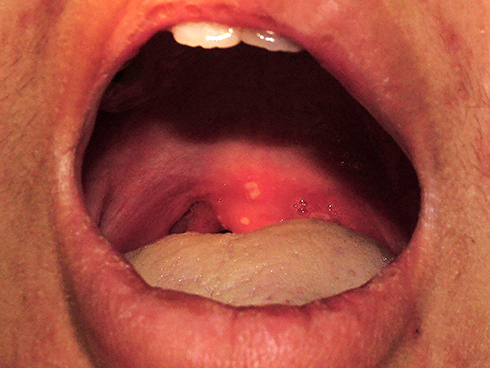 |
Figure 3 Recurrent oral ulcers at the uvula and tonsil. |
 |
Figure 4 A recurrent genital ulcer at the vulva. |
 |
Figure 5 A recurrent genital ulcer on the scrotum. |
 |
Figure 6 Erythema nodosum-like lesions on the lower extremities. |
Other cutaneous manifestations presented in our study were papulopustular lesions found in 29 patients (25.4%) and cutaneous vasculitis in 9 patients (7.6%). Sweet’s syndrome-like lesions, pyoderma gangrenosum (PG)-like lesions, and erythema multiforme (EM)-like lesions were reported equally in 6 patients (5.0%). Pathergy test was positive in 39 (46.2%) patients.
Extracutaneous Manifestations
Ophthalmologic involvement was the most common finding reported in 72 (60.5%) cases, which were mainly panuveitis and retinal vasculitis (65.7% and 55.7%, respectively). Articular manifestations were noted in 64 (53.8%) patients. Neurological involvement was presented in 11 (9.2%) cases, of which 9 had CNS involvement. CNS vasculitis was found in 4 out of 9 patients (44.4%). Gastrointestinal involvement occurred in 9 (7.6%) patients. The most common presentation was gastrointestinal ulceration found in 5 out of 9 (55.6%) patients. Five patients had major vascular involvement, 3 (60.0%) of which had deep vein thrombosis. None had cardiac involvement.
Treatment Modalities
Prednisolone was prescribed to 101 (88.6%) patients. Other immunosuppressive drugs were prescribed to 78 (65.6%) cases. Thirty-five patients (30%) had administration of intravenous pulse methylprednisolone. The median cumulative dose of corticosteroids was 9856.25 mg (IQR 3125–18,350 mg of prednisolone). There was no use of intravenous immunoglobulin or plasmapheresis in any cases.
Cutaneous Manifestations and Disease Activity
Univariate quantile regression analysis demonstrated that features significantly related to a lower median BDCAF score were minor oral ulcer at the buccal mucosa (p < 0.001) and papulopustular lesions on the lower extremities (p = 0.023). While features significantly linked to a higher median BDCAF score were minor oral ulcer at the tonsil (p = 0.045), papulopustular lesions at the neck (p < 0.001), and EN-like lesions (p < 0.001). However, after applying multivariate analysis, only the presence of minor oral ulcer at the buccal mucosa was significantly related to a lower median BDCAF score (median BDCAF score with present vs absent lesion was 5 (IQR 5–7) vs 7 (IQR 5–7) (p = 0.003)), while the presence of minor oral ulcer at tonsil was associated with a higher median BDCAF score (median BDCAF score with present vs absent lesion was 7.5 (IQR 7–8) vs 5 (IQR 5–7) (p = 0.024)) (Table 3 and Supplementary Table S1).
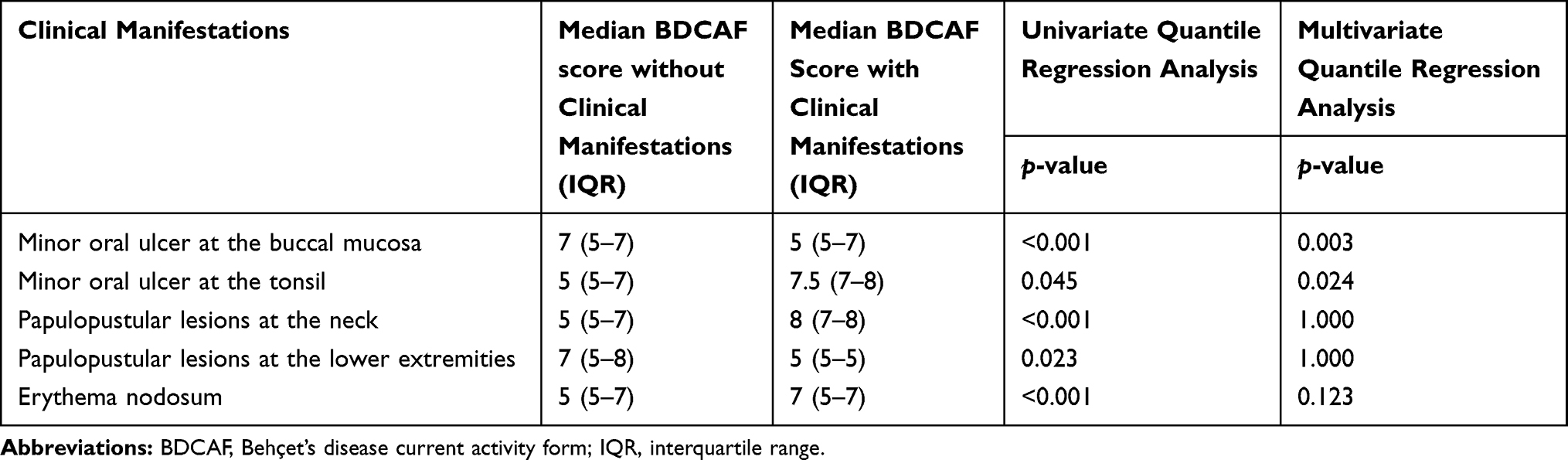 |
Table 3 Cutaneous Manifestations in Relations to Behçet’s Disease Activity |
Cutaneous Manifestations and Disease Prognosis
Multivariate analysis adjusted for follow-up time on cutaneous manifestations in relation to cumulative dose of corticosteroids (Table 4 and Supplementary Table S2) and morbidity (Table 5 and Supplementary Table S3) revealed that patients with recurrent genital ulcers had a significantly lower median cumulative dose of prednisolone compared to those without (7202.5 mg vs 14,405 mg, p = 0.010). However, the presence of recurrent genital ulcer had no association to morbidity. Male gender when compared to their female counterpart was related to significantly higher cumulative dose of prednisolone (14,610 mg vs 6732 mg, p = 0.003) and higher rates of hospitalization (63.2% vs 34.0%, OR = 2.78 (95% CI [1.10, 7.57]) vs 0.35 (95% CI [0.13, 0.91]), p = 0.031). Patients with ocular manifestations also showed a significantly higher median cumulative dose of prednisolone compared to those without (14,210 mg vs 4,903.8 mg, p = 0.002). Moreover, the presence of ocular manifestation was linked to higher morbidity (60.7% vs 22.9%, OR = 4.39 (95% CI [1.57, 12.29])). One patient from our study passed away due to sepsis complication. However, no association was found between clinical manifestations and mortality.
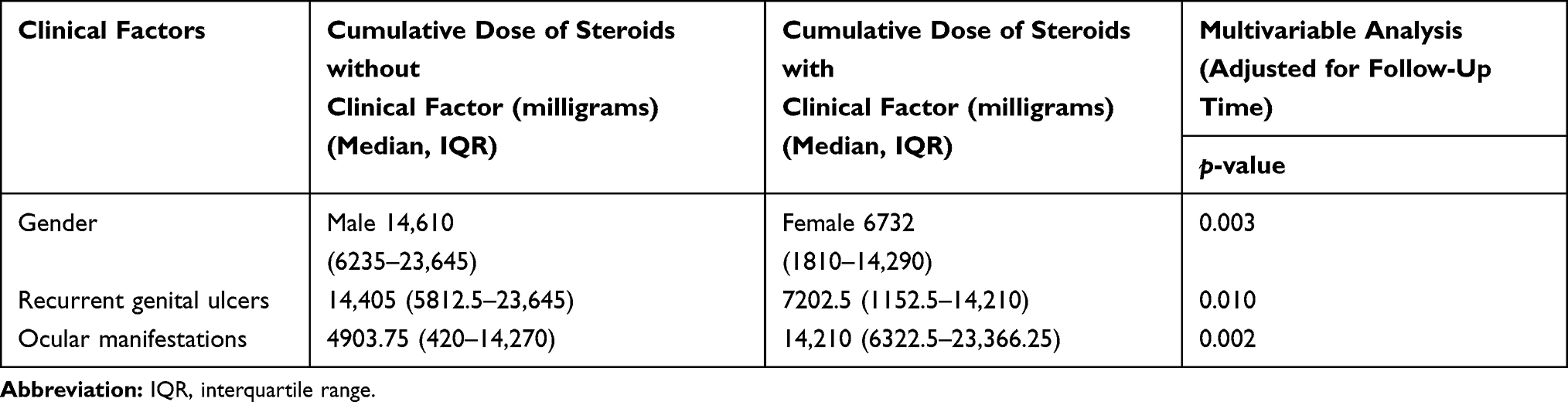 |
Table 4 Clinical Factors in Relations to Cumulative Dose of Corticosteroids |
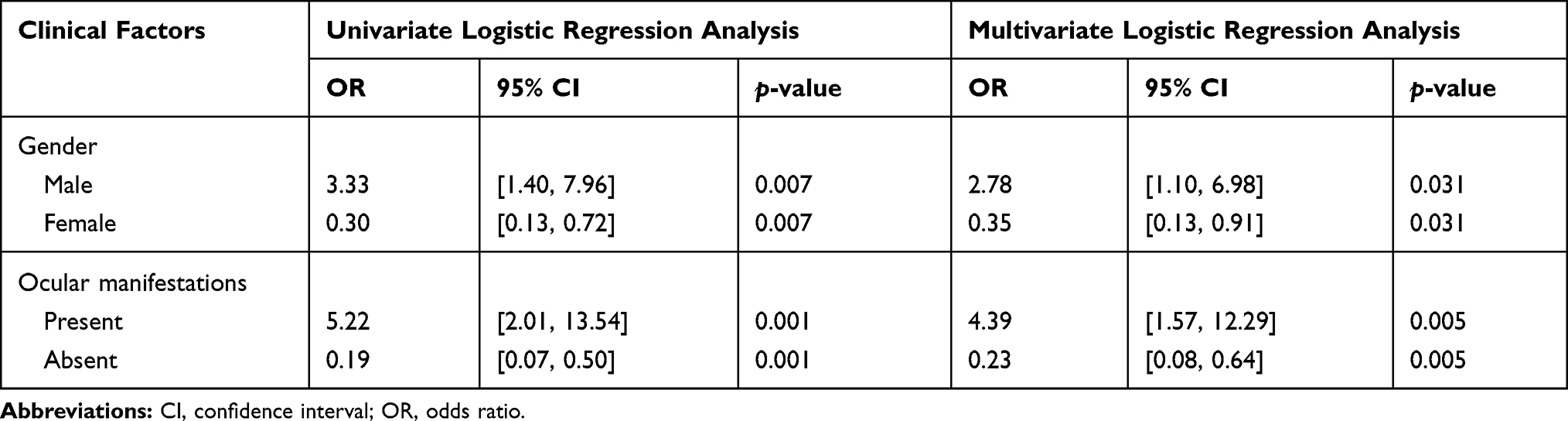 |
Table 5 Clinical Factors in Relations to Behçet’s Disease Morbidity |
Discussion
Mucocutaneous lesions were the hallmarks of Behçet’s disease and the most common findings in our study. Like the previous reports, recurrent oral ulcers were the most prevalent, followed by recurrent genital ulcers and EN-like lesions, respectively.18,19 Our results confirmed that in men the usual locations of genital ulcers were on the scrotum, inguinal area, and penis, whereas in women ulcers were mostly located on the vulva and femoro-inguinal area. There was one patient in our study presenting with vaginal ulcer, which was an extremely rare finding.20
To the best of our knowledge, this is the first study focusing on the association between cutaneous manifestations and disease activity of Behçet’s disease. We demonstrated that different locations of minor oral ulcers resulted in differences in the median BDCAF scores. Minor oral ulcers at the buccal mucosa were significantly associated with lower disease activity, whereas ulcers located at the tonsils were linked to higher disease activity. A prior report has shown that patients with Behçet’s disease had significantly more oral health impairment compared to healthy controls and this was related to higher disease activity.21 Existing evidence has also shown a significantly higher proportion of Streptococcus sanguinis (S. sanguis) in the normal oral flora of Behçet’s disease patients compared to healthy controls,22 and skin hypersensitivity reactions stimulated by streptococcal antigens were remarkably more prominent than those of other antigens in Behçet’s disease patients.23 Interestingly, a study by Seoudi et al has demonstrated the increment of S. sanguinis levels in orally active Behçet’s disease patients and different patterns of bacterial colonization were demonstrated between ulcerated and non-ulcerated oral mucosa in these patients.24 Furthermore, there was a distinct variation of plaque ecology at different intraoral sites.25 Thus, our data showing the distinct location of oral ulcer correlated to an alteration in the disease activity may be related to the diverse levels of bacterial oral flora and S. sanguinis between the buccal mucosa and tonsillar areas. However, further studies are required to validate this hypothesis. Our study retrospectively evaluated cutaneous manifestation at one point in time. As oral ulcer is the most common sign in Behçet’s disease, its number, size, and site can be highly presented at different times/stages of disease. Moreover, it may also be influenced by many factors, particularly the pharmacological therapy.26 Therefore, prospective studies with follow-up of changes in the characteristics of oral ulcers are suggested.
Regarding the prognosis of Behçet’s disease, male gender and presence of ocular manifestations were poor prognostic factors related to higher cumulative corticosteroid dosage in the course of treatment and higher hospital admission rates. While the presence of genital ulcers was a protective indicator determined by lower cumulative corticosteroid dosage required for disease control. The fact that male gender correlated with higher disease activity has been confirmed by the prior studies.18,19,27-29 Ocular symptoms were more frequently found in male Behçet’s disease patients and were associated with higher disease activity and overall mortality.28,30 Therefore, both the male gender and the presence of ocular manifestations are speculated to be linked to disease morbidity. On the contrary, females of reproductive age had a higher tendency to develop genital ulcers and a lower tendency to present with ocular manifestations, and resulted in a more favorable prognosis.30,31 To date, the underlying mechanisms of gender influence on the diverse clinical outcome and variable disease activity remain unclear. A study by Yavuz et al showed that in patients with Behçet’s disease, testosterone increased neutrophil activity and level of Th1-proinflammatory cytokine (IL-12 and IL-2) production. Moreover, testosterone decreased the gene expression and level of the IL-10 inhibitory cytokine, especially in males. Testosterone also altered the expression levels of Toll-like receptor 4 (TLR4), endoplasmic reticulum amino peptidase 1 (ERAP1), and chemokine receptor 1 (CCR1) genes which may play important roles in the immune response system.32,33 These findings emphasize the possible role of testosterone on the pathogenesis of Behçet’s disease particularly in males. However, further studies are essential to validate the association between gender difference and whether sex hormones are implicated for the pathogenesis of Behçet’s disease.
The present study may be subjected to a few limitations. Our sample size was relatively small. The retrospective nature of the study may result in missing data and the possibility of ascertainment bias. It may also lead to the difficulty in determining the evolution of cutaneous lesions over time. Moreover, all patients were collected from a single center at a tertiary institution which may represent a more severe subgroup of Behçet’s disease. Finally, the BDCAF score used to evaluate the disease activity may not represent the disease severity. Nevertheless, as there have been limited data on the mucocutaneous manifestations as a predictor of disease activity, morbidity, and mortality of Behçet’s disease, especially in the Thai population, our data will be informative to clinicians dealing with these patients as it may enable them to set appropriate counseling and optimize the treatment strategy among patients with poor prognostic indicators.
Conclusion
Our study suggests that the locations of minor oral ulcers were important predictors of disease activity. Male gender and ocular manifestations were associated with hospitalization and poorer prognoses, while the presence of genital ulcers may be associated with more favorable outcome. Future prospective studies in various geographical areas are suggested to confirm these results.
Abbreviations
CI, confidence interval; IQR, interquartile range; OR, odds ratio.
Data Sharing Statement
The data sets used or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Aspect
This study was approved by the Ramathibodi Hospital Institutional Review Board for Ethics in Human Research, according to Good Clinical Practice Guidelines and the provisions of the World Medical Association Declaration of Helsinki (Protocol number: MURA2018/826). As this study’s nature was a retrospective study, informed consent was exempted by the board. All authors confirm that all data accessed complied with relevant data protection and privacy regulations.
Funding
None.
Disclosure
All authors report no conflict of interest in this work.
References
1. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):
2. Alpsoy E. Behçet’s disease: a comprehensive review with a focus on epidemiology, etiology and clinical features, and management of mucocutaneous lesions. J Dermatol. 2016;43(6):
3. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. N Engl J Med. 1999;341(17):
4. Onder M, Gürer MA. The multiple faces of Behçet’s disease and its aetiological factors. J Eur Acad Dermatol Venereol. 2001;15(2):
5. Lee ES, Bang D, Lee S. Dermatologic manifestation of Behçet’s disease. Yonsei Med J. 1997;38(6):
6. Alpsoy E, Zouboulis CC, Ehrlich GE. Mucocutaneous lesions of Behcet’s disease. Yonsei Med J. 2007;48(4):
7. Mendes D, Correia M, Barbedo M, et al. Behçet’s disease–a contemporary review. J Autoimmun. 2009;32(3–4):
8. Uva L, Miguel D, Pinheiro C, Filipe P, Freitas JP. Mucocutaneous manifestations of Behçet’s disease. Acta Reumatol Port. 2013;38(2):
9. Kural-Seyahi E, Fresko I, Seyahi N, et al. The long-term mortality and morbidity of Behçet syndrome: a 2-decade outcome survey of 387 patients followed at a dedicated center. Medicine (Baltimore). 2003;82(1):
10. International Study Group for Behcet’s Disease. Criteria for diagnosis of Behcet’s disease. Lancet. 1990;335(8697):1078–1080.
11. International Team for the Revision of the International Criteria for Behçet’s Disease (ITR-ICBD). The International Criteria for Behçet’s Disease (ICBD): a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014;28(3):
12. Bhakta BB, Brennan P, James TE, Chamberlain MA, Noble BA, Silman AJ. Behçet’s disease: evaluation of a new instrument to measure clinical activity. Rheumatology (Oxford). 1999;38(8):
13. Kump LI, Moeller KL, Reed GF, Kurup SK, Nussenblatt RB, Levy-Clarke GA. Behçet’s disease: comparing 3 decades of treatment response at the National Eye Institute. Can J Ophthalmol. 2008;43(4):
14. Akman-Demir G, Serdaroglu P, Tasçi B. Clinical patterns of neurological involvement in Behçet’s disease: evaluation of 200 patients. The Neuro-Behçet Study Group. Brain. 1999;122(Pt11):
15. Kalra S, Silman A, Akman-Demir G, et al. Diagnosis and management of Neuro-Behçet’s disease: international consensus recommendations. J Neurol. 2014;261(9):
16. Skef W, Hamilton MJ, Arayssi T. Gastrointestinal Behçet’s disease: a review. World J Gastroenterol. 2015;21(13):
17. Atzeni F, Sarzi-Puttini P, Doria A, Boiardi L, Pipitone N, Salvarani C. Behçet’s disease and cardiovascular involvement. Lupus. 2005;14(9):
18. Yazici H, Tüzün Y, Pazarli H, et al. Influence of age of onset and patient’s sex on the prevalence and severity of manifestations of Behçet’s syndrome. Ann Rheum Dis. 1984;43(6):
19. Alpsoy E, Donmez L, Onder M, et al. Clinical features and natural course of Behçet’s disease in 661 cases: a multicentre study. Br J Dermatol. 2007;157(5):
20. Gürler A, Boyvat A, Türsen U. Clinical manifestations of Behçet’s disease: an analysis of 2147 patients. Yonsei Med J. 1997;38(6):
21. Mumcu G, Inanc N, Ergun T, et al. Oral health related quality of life is affected by disease activity in Behçet’s disease [published correction appears in Oral Dis. 2006 May;12(3):356]. Oral Dis. 2006;12(2):
22. Isogai E, Ohno S, Kotake S, et al. Chemiluminescence of neutrophils from patients with Behçet’s disease and its correlation with an increased proportion of uncommon serotypes of Streptococcus sanguis in the oral flora. Arch Oral Biol. 1990;35(1):
23. Kaneko F, Oyama N, Nishibu A. Streptococcal infection in the pathogenesis of BehÇet’s disease and clinical effects of minocycline on the disease symptoms. Yonsei Med J. 1997;38(6):
24. Seoudi N, Bergmeier LA, Drobniewski F, Paster B, Fortune F. The oral mucosal and salivary microbial community of Behçet’s syndrome and recurrent aphthous stomatitis. J Oral Microbiol. 2015;7:27150. doi:10.3402/jom.v7.27150
25. Theilade E, Theilade J. Formation and ecology of plaque at different locations in the mouth. Scand J Dent Res. 1985;93(2):
26. Mays JW, Sarmadi M, Moutsopoulos NM. Oral manifestations of systemic autoimmune and inflammatory diseases: diagnosis and clinical management. J Evid Based Dent Pract. 2012;12(3 Suppl):265–282. doi:10.1016/S1532-3382(12)70051-9
27. Ugurlu N, Bozkurt S, Bacanli A, Akman-Karakas A, Uzun S, Alpsoy E. The natural course and factors affecting severity of Behçet’s disease: a single-center cohort of 368 patients. Rheumatol Int. 2015;35(12):
28. Bang DS, Oh SH, Lee KH, Lee ES, Lee SN. Influence of sex on patients with Behçet’s disease in Korea. J Korean Med Sci. 2003;18(2):
29. Zouboulis CC, Turnbull JR, Martus P. Univariate and multivariate analyses comparing demographic, genetic, clinical, and serological risk factors for severe Adamantiades-Behçet’s disease. Adv Exp Med Biol. 2003;528:
30. Ucar-Comlekoglu D, Fox A, Sen HN. Gender differences in Behçet’s disease associated uveitis. J Ophthalmol. 2014;2014:820710. doi:10.1155/2014/820710
31. Ishido T, Horita N, Takeuchi M, et al. Clinical manifestations of Behçet’s disease depending on sex and age: results from Japanese nationwide registration. Rheumatology (Oxford). 2017;56(11):
32. Yavuz S, Ozilhan G, Elbir Y, Tolunay A, Eksioglu-Demiralp E, Direskeneli H. Activation of neutrophils by testosterone in Behçet’s disease. Clin Exp Rheumatol. 2007;25(4 Suppl 45):
33. Yavuz S, Akdeniz T, Hancer V, Bicakcigil M, Can M, Yanikkaya-Demirel G. Dual effects of testosterone in Behcet’s disease: implications for a role in disease pathogenesis. Genes Immun. 2016;17(6):
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.