Back to Journals » Eye and Brain » Volume 10
Curvilinear, symmetrical, and profound pigment deposition on the posterior lens capsule in a patient with bilateral pigmentary dispersion syndrome
Authors Canestraro J, Sherman J ![]()
Received 28 December 2017
Accepted for publication 4 June 2018
Published 13 September 2018 Volume 2018:10 Pages 79—84
DOI https://doi.org/10.2147/EB.S160999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Margaret Wong-Riley
Julia Canestraro,1 Jerome Sherman2
1SUNY College of Optometry, New York, NY, USA; 2Department of Clinical Education, SUNY College of Optometry, New York, NY, USA
Introduction: The classic presentation of pigmentary dispersion syndrome (PDS) often consists of midperipheral iris transillumination defects, Krukenberg’s spindle, and dense homogeneous trabecular pigmentation. Other subtle, sometimes overlooked features include pigment on the lens zonules, pigment on the anterior lens capsule and pigment along the equator of the posterior lens capsule.
Case: This unique presentation of PDS presented with bilateral, dense, oblique, and symmetrical pigment deposition along the posterior lens capsule that changed in shape, density, and extent over the span of 3 years.
Discussion: There have been few reports in the literature that describe a central accumulation of pigment along the posterior lens capsule associated with PDS. There are reported cases of pigment deposition along the central aspect of the posterior lens capsule, some changing over time, although none were bilateral and symmetrical. There are suggestions that perhaps this central pigment deposition is related to a break in the ligament of Weiger, allowing communication between the posterior chamber and posterior lens capsule. This is a case in which curvilinear, symmetrical, and changing pigment deposition on the posterior lens capsule is suggestive of perhaps another key features of PDS.
Keywords: pigment deposition, ligament of Weiger, space of Berger, zonules, pigmentary glaucoma
Introduction
Pigmentary dispersion syndrome (PDS) has many distinct clinical features that aide in its diagnosis and management. Ritch et al1 estimated the prevalence of PDS to be 2.45% of Caucasian patients in a glaucoma screening. Roberts et al2 estimated the prevalence of PDS to be 0.0015% of African Americans in a primary care setting. These estimates are likely disparate because of the difference in phenotypic expression between the two ethnicities, as noted by Roberts et al.2 Although PDS is autosomal dominant in nature3 for both African American and Caucasian populations, it is thought to have incomplete penetrance in the African American population.4 Myopia has been noted as a significant corollary to PDS. Scheie and Cameron5 reported the incidence of myopia to be 65% in a group of 493 eyes with PDS, regardless of ethnicity. The classic clinical presentation of PDS includes midperipheral iris transillumination defects, Krukenberg’s spindle, and dense homogeneous trabecular pigmentation.6 Other clinical features that are often overlooked may include pigment on the lens zonules7 and pigment on the anterior and posterior lens capsule.8 It is estimated that patients with PDS have a 35%–50% chance of developing pigmentary glaucoma during their lifetime.9 Below is a case in which the patient presented with many of the known features of PDS, along with an uncommon presentation of symmetrical pigment on both posterior lens capsules with changes in morphology and density over time.
Case
A 45-year-old Caucasian male initially presented with reduced acuities in both eyes since childhood. His medical and family history was unremarkable, with best-corrected acuities 20/60 in each eye and correction –8.00–2.00×135 OD and –8.00–1.25×020 OS. External examination was normal, but slit lamp examination revealed midperipheral iris transillumination defects (Figure 1), pigment on the corneal endothelium and dense, and symmetrical pigment on the posterior lens capsules. Gonioscopy revealed angles open to ciliary body with grade 2+ pigment in all quadrants and no evidence of angle recession. Intraocular pressures (IOPs) were 17 and 18 mmHg in each eye. Dilated fundus examination with binocular indirect ophthalmoscopy and scleral depression revealed an intact retina, with no holes or tears and no signs of pigmented cells in the vitreous. The optic nerves were small: ~1 mm ×1 mm as measured with Spectral Domain Optical Coherence Tomography (SD-OCT; © 2017; Carl Zeiss Meditec AG, Jena, Germany). We confirmed optic disc hypoplasia in both eyes as the likely cause of the patient’s decreased vision. Over the course of 3 years, the IOP remained in the 15–19 mmHg range in both eyes. During this time, retinal nerve fiber layer thinning and corresponding visual field defects were evident. Given the presence of optic nerve hypoplasia in addition to PDS, it was difficult to assess the damage solely related to glaucomatous changes. For this reason, glaucoma therapy was initiated using Travatan Z ophthalmic solution once daily in both eyes. IOPs remained stable at 13 mmHg in each eye, and he continues to be monitored for any changes. Of particular interest was the unusual presentation of pigment deposition on the posterior lens capsules of each eye. The pattern of pigment was dense, oblique, and curvilinear and located along the posterior lens capsules (Figure 2). The pigment on the posterior capsule created shadows on the retina, which were best documented with Optos Daytona ultra-widefield imaging (© 2017; Optos plc, Dunfermline, UK), which provides ultra-widefield fundus imaging (Figure 3). Over time, it appeared that there was an increase in pigment deposition along the posterior lens capsule. Comparing photos 1 year apart, one can observe the apparent increase in the size of pigment deposition (Figure 4A and B). Interestingly, photos taken 2 years later showed a marked decrease in pigment deposition on the posterior lens capsules (Figure 5). There were no changes in the patient’s medical history in that same time span, including a repeated denial of medication changes or incidents of trauma. A search of literature published in the last 15 years did not reveal any cases of bilateral, dense, and symmetrical pigment deposition on the posterior lens capsule with a change in morphology over time.
 | Figure 1 Midperipheral iris transillumination defects of the left eye, seen by direct illumination of the globe via transilluminator applied directly to lower lid in the dark. Note: Transillumination of the fellow eye was almost a mirror image compared to the left. |
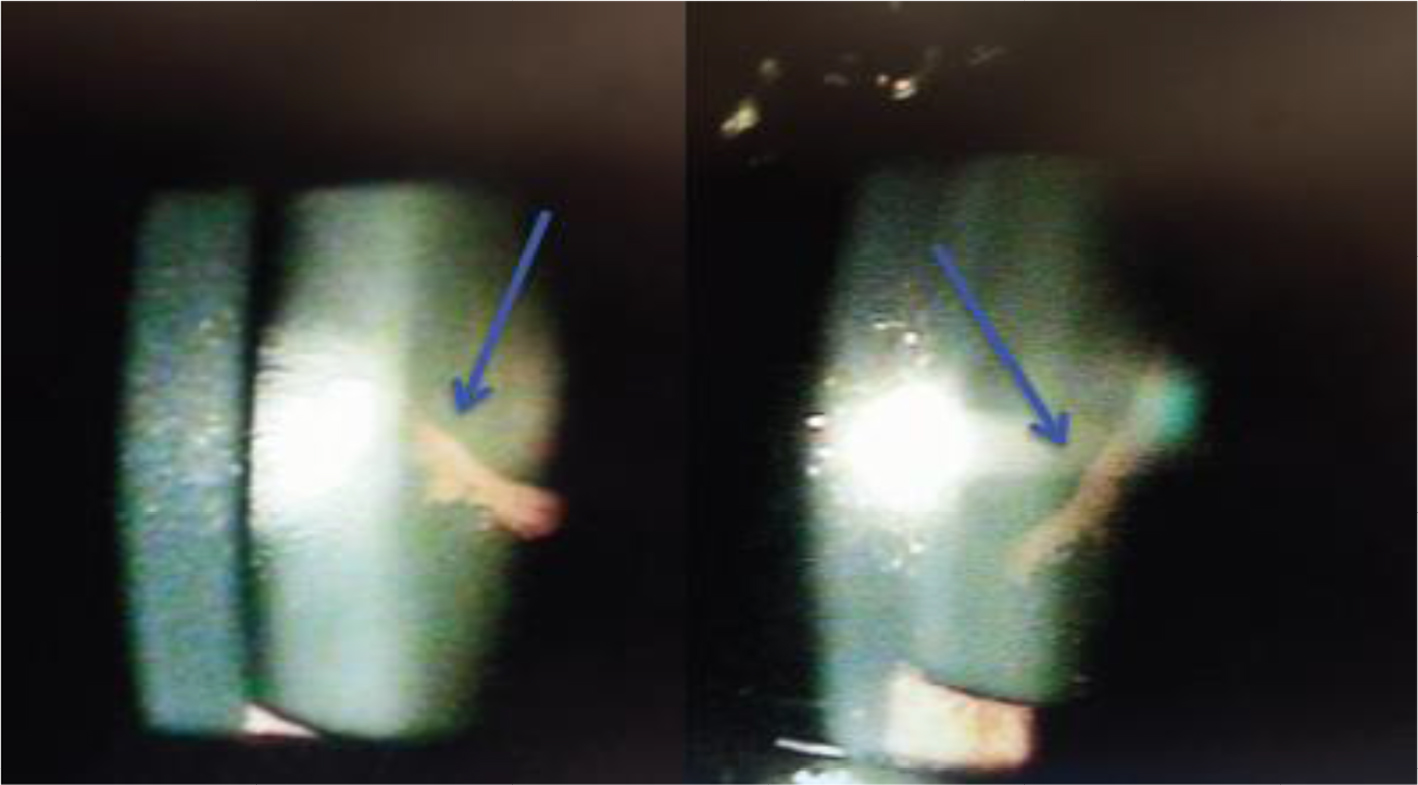 | Figure 2 Circumlinear deposition of dense pigment along the posterior lens capsule of each eye. Notes: The deposition in each eye (arrows) is virtually a mirror image of the other. The view with biomicroscopy of the posterior lens capsule matched the “shadow” seen with ultra-widefield images on each visit as seen in Figures 3–5. |
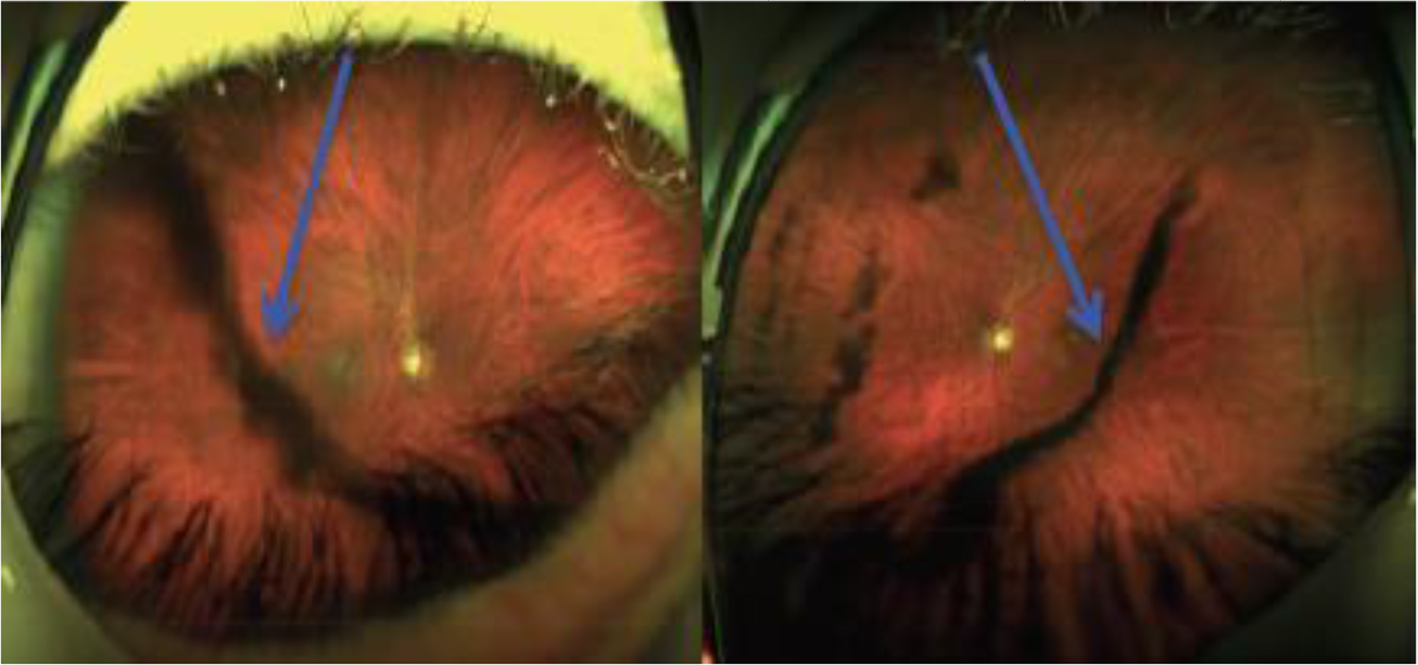 | Figure 3 Optos Daytona ultra-widefield imaging of each eye reveals shadows cast on the fundus from the pigment on the posterior lens capsule. Note: These images also highlight the symmetry of pigment deposition (arrows) in the two eyes. |
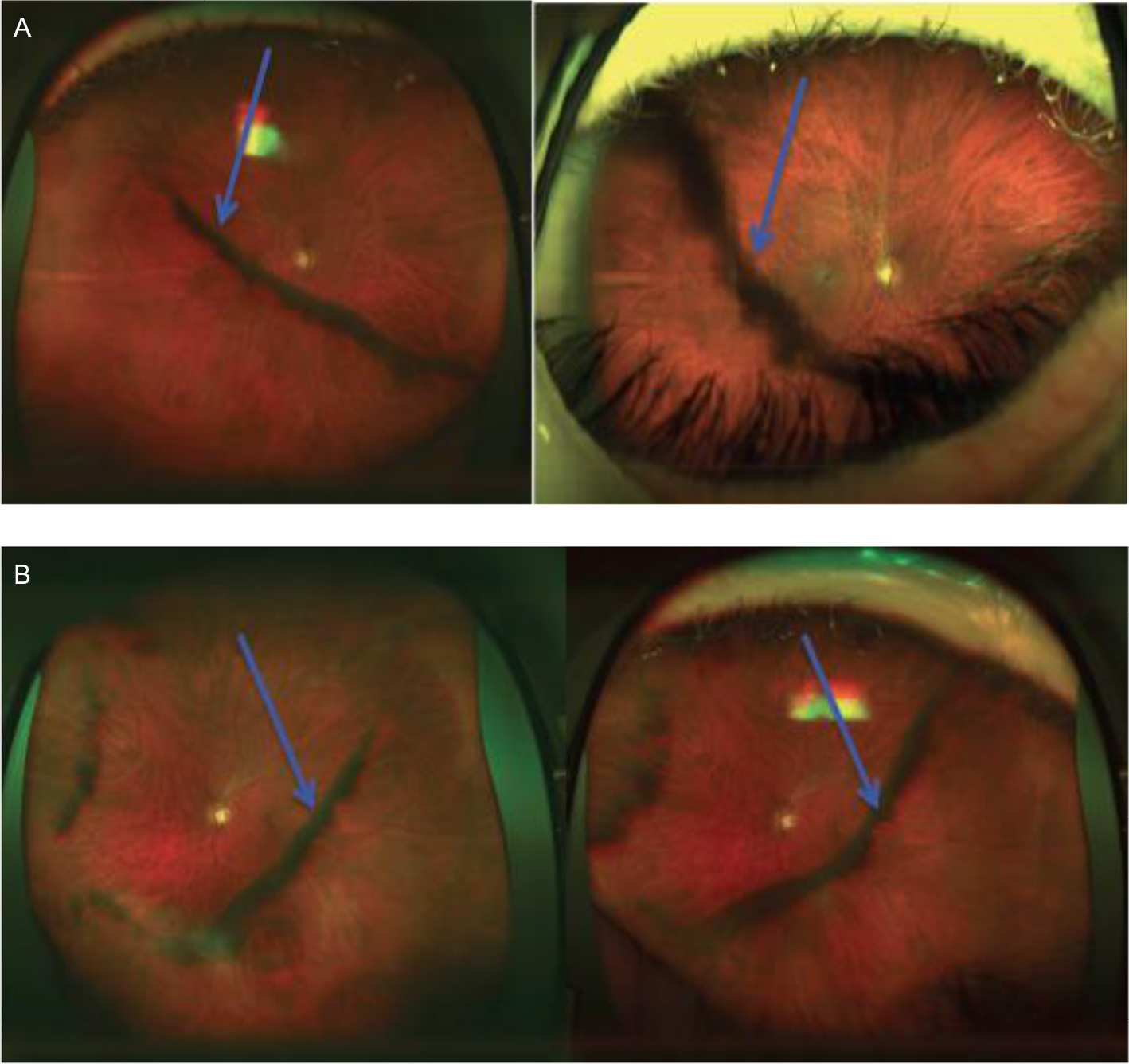 | Figure 4 (A) Optos Daytona ultra-widefield images highlight an increase in pigment over time of the right eye from 2013 (left) to 2014 (right). (B) Optos Daytona ultra-widefield images highlight an increase in pigment over time of the left eye from 2013 (left) to 2014 (right). Note: These are visualized by the shadows cast on the retina (arrows) from the pigment deposition along the posterior lens capsule. |
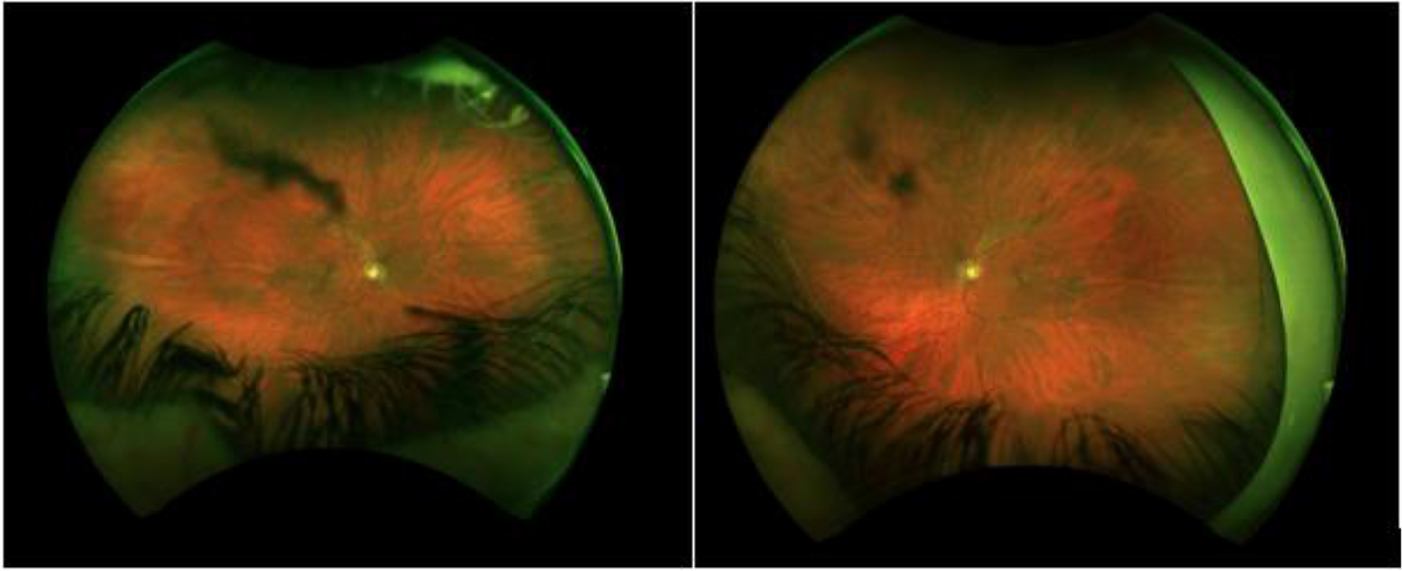 | Figure 5 Optos California images from 2016 reveal a decrease in pigment over time of the right eye (left) and left eye (right) compared to 2013 and 2014 (Figure 4A and B). Notes: These are visualized by the shadows cast on the retina from the pigment deposition along the posterior lens capsule. |
Informed consent
The patient described in this case has given written informed consent to have the case details and accompanying images published.
Discussion
A ring-shaped deposition of pigment on the equator of the posterior lens capsule along the zonular attachments can be found in patients with PDS.7 Proximal to the zonules is the ligament of Weiger, which is the ring-like attachment of the anterior limiting membrane of the vitreous to the posterior lens capsule. Another ring of pigment, known as Scheie’s line, can deposit at the juncture of the ligament of Weiger.8 The ligament of Weiger encircles the space of Berger, which is located between the posterior lens capsule and the vitreous.10 This space is located centrally through the visual axis and is typically void of debris assuming that the ligament of Weiger remains intact.11 In our patient, we observed an unusual and dramatic deposition of pigment on the central aspect of the posterior lens capsule, which was remarkably symmetrical when comparing one eye with the other. Theoretically, if the ligament of Weiger is intact, there should not be communication between the posterior chamber and the potential space of Berger.10 In our case, the pigment on the central aspect of the posterior lens capsule appeared to increase and then to decrease in size over time (Figures 4A and B vs Figure 5). A possible explanation for this points to a break in the ligament of Weiger. If there was a break in the ligament of Weiger and the anterior hyaloid remained intact, it would allow aqueous to traverse from the posterior chamber to the space of Berger. The constant flow of aqueous through this space could bring loose iris pigment to deposit on the central aspect of the posterior lens capsule and then over time displace this same pigment to a different location. Given there was no pigment visualized in the vitreous and there were no retinal breaks noted on fundus examination, we believe the pigment cells in our patient originated from the iris, rather than the retina. Roberts et al11suggested that a disruption in this natural barrier, such as with trauma, may allow pigment to enter the potential space of Berger. However, a bilateral break in the ligament of Weiger is rare without trauma and, therefore, remains to be explained. It should be noted that the commencement of travoprost drops after the first 3 years of observation could have had an effect on the change in pigment. We do not feel that this change is significant, given that pigment deposition also decreased over time while on the same medication. Additionally, photos in Figure 4A and B were taken by the Optos Daytona and those in Figure 5 were taken by Optos California Daytona ultra-widefield imaging (© 2017; Optos plc). We do not believe that this would have a significant impact on imaging the pigment on the posterior lens capsule.
There are few cases in the literature that describe findings of bilateral and symmetrical pigment deposition on the posterior lens capsule with changes in morphology over time. Al-Mezaine12 reported a case of unilateral pigment deposition with a history of trauma in that same eye. Nagarajaiah and Shun-Shin,13 Lin et al,14 and Turgut et al15 describe cases of unilateral pigment deposition on the posterior lens capsule without a history of trauma. Nagarajaiah’s case is similar to ours in that the pigment was noted to change over time. Roberts et al11 reported a case of bilateral pigment deposition with the history of trauma in only one eye and a second case of unilateral pigment deposition without trauma. His first case is most similar to ours in that there was bilateral pigment deposition; however, his patient did not present with symmetry between the two eyes, nor was it noted to change over time.
As hypothesized earlier, a break in the ligament of Weiger is the only way in which pigment can reach the space of Berger. Since cases of spontaneous breaks in the ligament of Weiger are rare,16 we propose another mechanism for this break. Bernal et al17 were able to describe and document the precise insertion of the anterior and posterior zonules to the lens capsule. Traditionally, it was thought that both the anterior and posterior zonules began at the ciliary body and inserted directly to the lens. Bernal confirmed that the anterior zonules have a straight path from the ciliary body to the lens. However, the majority of the posterior zonules first inserted into the anterior hyaloid membrane proximal to the ciliary body and then to the lens capsule. Some of these fibers inserted into areas close to Weiger’s ligament before adhering to the posterior lens capsule.17 If one could imagine the posterior bowing of the iris in a patient with PDS and its relationship to the anterior zonules, it could be perceived that such rubbing against the anterior zonules could also affect the posterior zonules, especially those which are directly adherent to the ligament of Weiger. After years of chronic contact, this would promote detachment of the ligament of Weiger, thereby allowing pigment to enter the space of Berger. Given that central posterior lens capsule pigmentation is not common in all patients with PDS, we propose that the amount of iris bowing may be related to this mechanical break in the ligament and perhaps a more concave iris would be more likely to cause a break in the ligament. The degree of iris concavity was not measured in our case but perhaps opens an area for future research.
The unusual presentation of the density, symmetry, and changing morphology of pigment has not been described previously in literature. This has clinical significance because if the known and sometimes subtle findings of PDS such as Krukenberg’s spindle, iris transillumination defects, and pigmented trabecular meshwork are initially overlooked by the examiner, observation of pigment on the posterior lens capsule may promote the examiner to check for these features more closely. Additionally, future studies relating the degree of iris bowing to a break in the ligament of Weiger may confirm such a relationship and thereby identify a new subset of patients with this feature of PDS.
Disclosure
The authors report no conflicts of interest in this work.
References
Ritch R, Steinberger D, Liebmann JM. Prevalence of pigment dispersion syndrome in a population undergoing glaucoma screening. Am J Ophthalmol. 1993;115(6):707–710. | ||
Roberts DK, Chaglasian MA, Meetz RE. Clinical signs of the pigment dispersion syndrome in blacks. Optom Vis Sci. 1997;74(12):993–1006. | ||
Andersen JS, Pralea AM, DelBono EA, et al. A gene responsible for pigment dispersion syndrome maps to chromosome 7q35-q36. Arch Ophthalmol. 1997;115(3):384–388. | ||
Roberts DK, Meetz RE, Chaglasian MA. The inheritance of the pigment dispersion syndrome in blacks. J Glaucoma. 1999;8(4):250–256. | ||
Scheie HG, Cameron JD. Pigment dispersion syndrome: a clinical study. Br J Ophthalmol. 1981;65(4):264–269. | ||
Ritch R. A unification hypothesis of pigment dispersion syndrome. Trans Am Ophthalmol Soc. 1996;94:381–409. | ||
Zentmayer W. Association of an annular band of pigment on the posterior capsule of the lens with a Krukenberg spindle. Arch Ophthalmol. 1938;20(1):52–57. | ||
Scheie HG, Fleischhauer HW. Idiopathic atrophy of the epithelial layers of the iris and ciliary body: a clinical study. Trans Am Ophthalmol Soc. 1957;55:369–391. | ||
Ritch R, Mudumbai R, Liebmann JM. Combined exfoliation and pigment dispersion: paradigm of an overlap syndrome. Ophthalmology. 2000;107(5):1004–1008. | ||
Hilding AC. Normal vitreous, its attachments and dynamics during ocular movement. Arch Ophthalmol. 1954;52(4):497–514. | ||
Roberts D, Miller E, Kim L. Pigmentation of the posterior lens capsule central to Weiger’s ligament and the Scheie line: a possible indication of the pigment dispersion syndrome. Optom Vis Sci. 1995;72(10):756–762. | ||
Al-Mezaine HS. Central posterior capsule pigmentation in a patient with pigment dispersion and previous ocular trauma: a case report. Indian J Ophthalmol. 2010;58(4):336–337. | ||
Nagarajaiah S, Shun-Shin G. Pigment deposition on the central aspect of the posterior lens capsule in pigmentary dispersion syndrome. Digital J Ophthalmol. 2011;17(4):69–71. | ||
Lin DY, Volpicelli M, Singh K. Dense pigmentation of the posterior lens capsule associated with pigment dispersion syndrome. J Glaucoma. 2003;12(6):491–493. | ||
Turgut B, Türkçüogˇlu P, Deniz N, Catak O. Annular and central heavy pigment deposition on the posterior lens capsule in the pigment dispersion syndrome: pigment deposition on the posterior lens capsule in the pigment dispersion syndrome. Int Ophthalmol. 2008;28(6):441–445. | ||
Torii H, Takahashi K, Yoshitomi F, Miyata K, Ishii Y, Oshika T. Mechanical detachment of the anterior hyaloid membrane from the posterior lens capsule. Ophthalmology. 2001;108(12):2182–2185. | ||
Bernal A, Parel JM, Manns F. Evidence for posterior zonular fiber attachment on the anterior hyaloid membrane. Invest Ophthalmol Vis Sci. 2006;47(11):4708–4713. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.