Back to Journals » Open Access Emergency Medicine » Volume 13
Current Use, Perceived Barriers, and Learning Preference of Point of Care Ultrasound (POCUS) in the Emergency Medicine in Qatar – A Mixed Design
Authors Bashir K ![]() , Azad AM, Hereiz A, Bashir MT
, Azad AM, Hereiz A, Bashir MT ![]() , Masood M, Elmoheen A
, Masood M, Elmoheen A ![]()
Received 31 January 2021
Accepted for publication 19 April 2021
Published 18 May 2021 Volume 2021:13 Pages 177—182
DOI https://doi.org/10.2147/OAEM.S304153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Khalid Bashir,1 Aftab Mohammad Azad,1 Ayman Hereiz,1 Mohammed Talha Bashir,2 Maarij Masood,1 Amr Elmoheen1
1Department of Emergency Medicine, Hamad General Hospital, Doha, Qatar; 2University of Aberdeen School of Medicine and Dentistry, Aberdeen, Scotland, UK
Correspondence: Khalid Bashir Email [email protected]
Introduction: Point of care ultrasound (POCUS) has been a part of emergency medicine (EM) training for almost two decades. EM training program has a very broad and rigorous POCUS curricula which, in several cases, does not translate to routine application in clinical settings. This study therefore sought to compare the indications, utilization, barriers, and preferred POCUS educational method in a large Middle Eastern academic EM.
Methodology: A validated questionnaire was emailed to 50 EM faculties between April and May 2019. Volunteer faculty members partook in a semi-structured interview to better understand the indications, current use, barriers, and preferred learning method. Responses were anonymous, and data were analyzed with descriptive statistics.
Results: This was a mixed design study. 30/50 (60%) of faculty responded to the survey, with a mean age of 39.2 years and a mean number of years in practice, 13.1. 55% (n=28) completed POCUS training in less than five years, while 45% completed more than five years ago and 5% never completed it. Forty percent of EM physicians were trained in Africa, while 55% were qualified in Asia and 5% completed their training in Europe. The indications and frequently performed procedures were consistent with the previous research. The common barrier reported was lack of time, lack of credentialing, lack of quality assurance, and national guidelines. The majority of the faculty preferred a blended learning approach for POCUS.
Conclusion: POCUS perceived barriers to its full use include time constraints, lack of national guidelines, and credentialing (awarding POCUS qualifications) of the faculty. Blended learning appears to be the preferred approach towards acquiring the knowledge and skills of POCUS.
Keywords: point of care ultrasound, POCUS, emergency medicine, learning method, blended learning
Introduction
Point-of-care ultrasound (POCUS) provides a bedside assessment that assists in diagnosis of health conditions, and treatment. If performed appropriately, POCUS contributes to early diagnosis of a wide range of conditions leading to improved outcomes and decreased length of hospital stays.1–3
POCUS allows emergency physicians (EM) to rapidly and in real-time assess cardiac function, central venous pressure, pulmonary edema, pleural effusions, pericardial effusions, ascites, pneumothoraces, and several other underlying pathologies.4–6 Utilization of POCUS enhances the success rate and safety of various bedside procedures such as surgical management of superficial abscesses, insertion of arterial lines, placement of central venous catheters, paracentesis, arthrocentesis, thoracentesis, and other procedures.7–10
POCUS has been incorporated into the academic curriculum in many medical training programs.11,12 POCUS training is now further extended to undergraduate medical education, and medical schools initiated to integrate the bedside ultrasound in their curriculum.13,14 POCUS is recognized as one of the basic and essential skills in the list of emergency procedures approved by The Accreditation Council for Medical Education (ACGME) milestones project.15 This relatively new modality has found application in several disciplines, including emergency medicine. The operator’s skills and competence is key to effective utilization of POCUS; hence, it is recommended that competent physicians perform POCUS. Several studies have been done on the barriers to learning ultrasound,16 with most studies being done in Europe and the USA.
Passive, active, and mixed learning are part of different strategies of effective instructional teaching. Several approaches are used in emergency physicians’ education, including traditional face-to-face lectures, online, or a combination of online and didactics teaching called blended learning (BL).17 Blended learning is an educational method where both traditional face to face and online training are used to improve the learners’ knowledge skills and attitude.18
Each educational method has distinct advantages; for instance, a study involving students of dentistry was conducted, and the outcome was compared using lectures and interactive small group learning. Knowledge retention in both groups was comparable, but skill learning was superior in small group teaching.19 Lecture-based education has been criticized in the past due to its inability to maintain learners’ attention for more than 15 minutes.20
Due to the busy nature of emergency medicine, physicians’ educators need to rely on innovative educational methods and modern technology to fulfill their clinical and educational roles. One of the innovative methods includes blended learning, which is defined as a method where traditional lecture-based education is combined with online education to provide the best outcome. Previous studies have shown that blended learning is equivalent or superior to traditional learning in the education of health professionals.21 There is a paucity of evidence about POCUS education through the BL approach in the emergency department. As far as we are aware, no study has looked at the barriers and educational preferences of POCUS in the Middle East, in particular, Qatar.
This research aimed to examine through a survey and semi-structured interview the indications, utilization, barriers, and preferred method of POCUS learning in the emergency department. The study will help us further improve the POCUS training program at our establishment.
Method
The study had a mixed design and was conducted in a large teaching hospital. The hospital hosts a 4-year-long emergency medicine residency program recognized by the international arm of the accreditation Council of Graduate Medical Education (ACGME-I). The study included semi-structured interviews with the faculty to ensure better understanding of the survey. One study author approached the volunteer faculty to comment on the current usage and future recommendations of POCUS in the emergency department. A validated questionnaire (Figure 1) was used and emailed to all 50 EM consultant faculty trained in different parts of the world with variable POCUS experience.
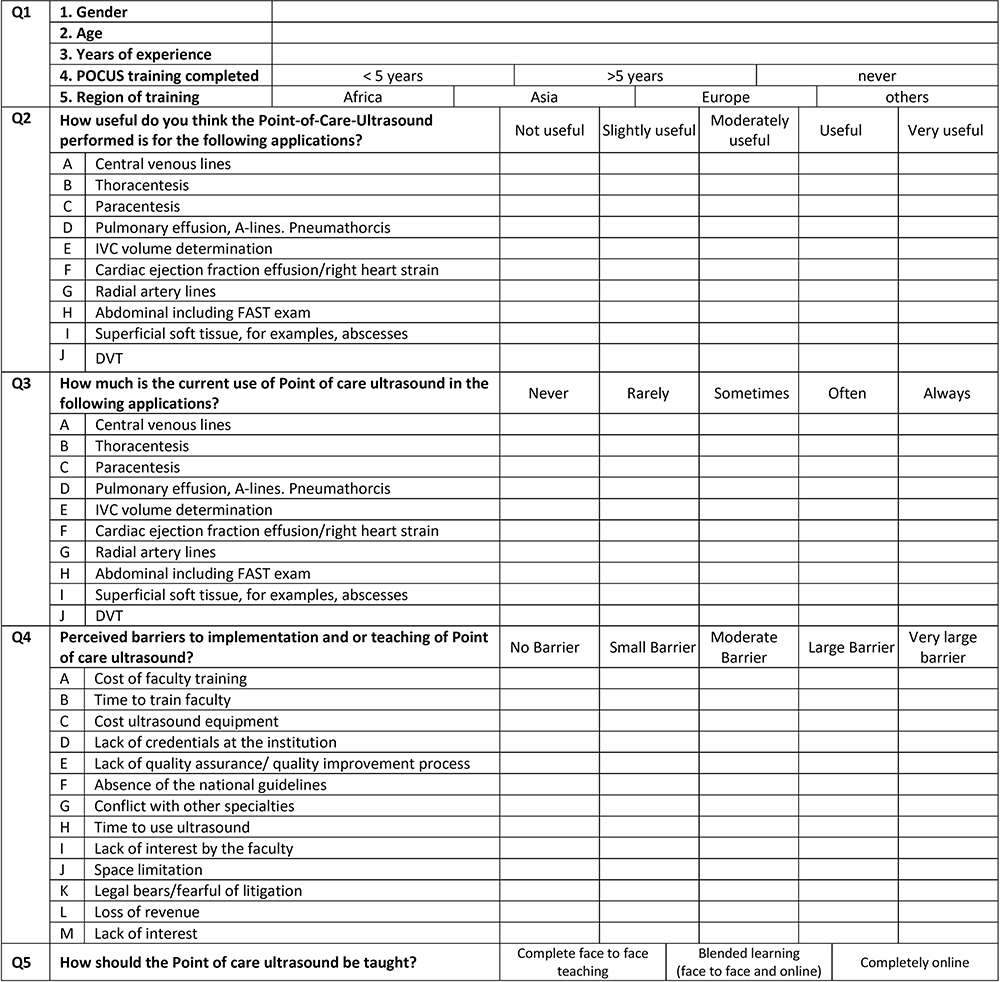 |
Figure 1 Validated questionnaire of the current use, perceived barriers, and learning preference of point-of-care-ultrasound (POCUS) in the emergency medicine. |
In our practice, the terminology used in the rating scale has been defined locally; “always” means POCUS used many times per day, “often” implies POCUS used more than 5–10 times per week, “sometimes” indicates POCUS used 2–5 times per week and “rarely” suggests POCUS used less than 2 times per week.
Thirteen barriers have been identified in our local setting; with 10 barriers being considered as very large; 7–10 barriers as large category, 4–6 barriers as moderate category, and 1–3 barriers in the small category.
We prepared the questionnaire using Survey Monkey, an online survey development cloud-based software. The survey link was sent to participants’ work email. The survey results did not give us a detailed explanation of the POCUS barrier, we conducted interviews to understand better about the barriers. One study author contacted five volunteered faculty for a semi-structured interview to explain more about the current POCUS barriers and their recommendation for the future. The answers were transcribed and agreed upon with the faculty before the end of the interview. Themes were generated from the written list. The survey was analyzed, and descriptive data were acquired through semi-structural interviews. All participants provided informed consent and ethical approval was obtained by the Hamad General hospital (MRC -01-20-314)
Results
Of the 50 faculties invited, 30 partook (response rate 60%). They were 27 male (90%) and 3(10%) females, mean age was 39.2 years (24–54), the mean number of years in practice was 13.1 (3 −26), 55% completed POCUS training within the last five years, while 45% completed more than 5 years, and 5% never completed. Regarding training of the faculty, 40% trained in Africa, 55% in Asia, while 5% were trained in the Europe. The top 5 indications identified were central line insertion, thoracentesis, paracentesis, inferior vena cava (IVC) volume determination, and cardiac ejection fraction/effusion. The most frequently performed procedures included central line insertion, IVC volume determination, cardiac ejection fraction effusions/right heart strain, paracentesis, and thoracentesis. Common barriers identified included training time, lack of credentialing at the institution, lack of quality assurance, and lack of national guidelines. The least common barrier identified was space limitation, lack of interest by the faculty, fear of litigation, and ultrasound and training costs. 16/30 (53.30%) preferred the blended learning approach to learning POCUS, while 10/30 (33.3%) favored a complete face-to-face approach and 4/30 (13.3%) preferred a completely online method.
Volunteer faculties participated in the semi-structured interview. They agreed that the focused, free of cost training provided by the Canadian Emergency Ultrasound Society (CEUS training) and POCUS machines’ availability has helped improve learning and compliance. They recommended that “on the job supervision,” feedback about the images acquisition and interpretation, “future research to assess the benefits to the patients and organization” will help retain the POCUS skills (Table 1).
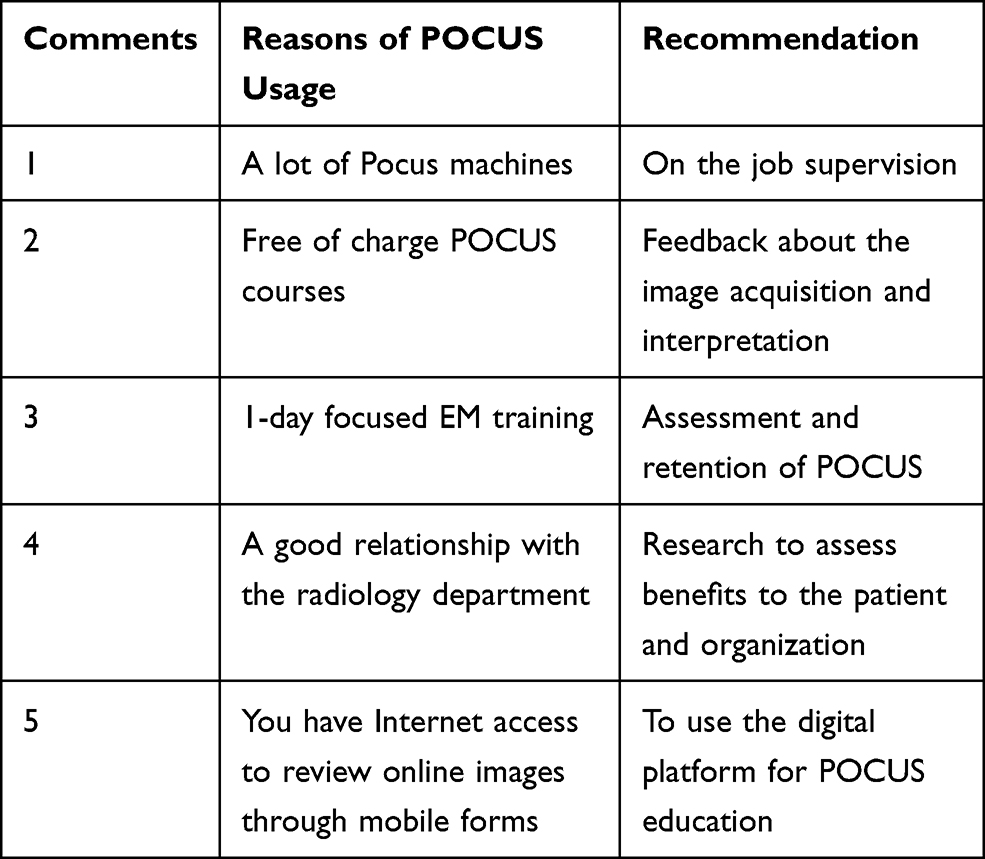 |
Table 1 Comments from the Faculty After the Semi-Structured Interview |
Discussion
The aim of this study was to assess the indications, perceived barriers, and preferred POCUS education method among the faculty in the emergency department of a large teaching hospital. The results from this research shows that POCUS has a wide application among ED consultants in spite of its perceived barriers.
The barriers to POCUS usage have been cited in previous studies. EM physicians must acquire POCUS proficiency skills through appropriate training, supervised practice, and quality assurance. There is need for local availability of theoretical and practical capabilities as well as observation to enhance quality assurance. The barriers could be overcome by organizing specific courses relevant to EM physicians and utilizing technology, such as real-time video conferencing.22
The top 5 indications identified were central line insertion, thoracentesis, paracentesis, inferior vena cava (IVC) volume determination, and cardiac ejection fraction effusions/right heart strain. Similarly, a previous study illustrated that the highest use of POCUS by the residents is for central venous catheter (99%), followed by thoracentesis (61%) and paracentesis (58%). Our findings are similar to the previously published research.16
The most perceived barriers as found by our study included time constraints, lack of national guidelines, lack of quality assurance, and faculty credentialing. A previous study identified the lack of POCUS machine availability and training, lack of formal curriculum, and lack of time to train faculty members as a severe barrier in the POCUS training and learning.23 The study also advocated the time and cost for training faculty members as the highest barrier in POCUS implementation.23
Another study indicated that lack of POCUS training, high cost of the ultrasound, and unavailability of the ultrasound machine constitutes a barrier in the use of POCUS in practice.24
The least barriers identified in our study were space limitation, lack of interest by the faculty, fear of litigation, and cost of ultrasound and training. The cost of ultrasound equipment and training appeared to be insignificant. In contrast, other studies have identified cost as a significant barrier to POCUS learning.25 Our study revealed that funding was not a major barrier. Qatar is one of the world’s wealthiest countries; the government spends around 2.7% of GDP on education and research; hence, not surprisingly, this was not regarded as a major barrier. In our study, only 5 (16.7%) identified litigation concerns, as compared to other studies.16 In Qatar, the indemnity is provided by Hamad Medical Corporation. Litigation is very rare concerning POCUS usage; there has been only one lawsuit against emergency physicians due to the inability to perform ultrasound, due to lack of training, in the last 20 years.25,26
Our study illustrated that blended learning, including face-to-face and online learning, appeared as the preferred method towards acquiring the knowledge and skills of POCUS. Our study results are in accord with a previous study, where blended learning led to statistically improved retention of knowledge both immediately and at two months.27 Another study revealed that the BL approach had a positive impact on the preclinical curriculum in clinical epidemiology and biostatistics.28 A working group was established after the study, with the mandate to enhance the education of POCUS in the department. The curriculum agreed with the Canadian ultrasound society, to run one-day course using blended learning approach. At present, there is a growing interest among physicians from internal medicine, intensive care, surgery and family medicine, all applying to attend the course. We are in the process of developing national guidelines and a 1 year POCUS fellowship training program.
The study has several limitations. The sample size was small; only 30 participants took part in the study from one teaching hospital in spite of several reminders. The busy schedule of the emergency consultant was one of the possible reasons for the low response rate. We believe our hospital faces the same barriers reported by other emergency departments, such as training, lack of time, and credentialing process. The small sample size in a single teaching hospital limits the statistical power of the study, thus necessitating the need to repeat the study in several health facilities across the country. The questionnaire was closed-ended and may introduce response bias; hence, a semi-structured interview was conducted with a selected group of volunteers. Its lack of generalizability restricts the semi-structured interview due to the challenge in analyzing the open-ended questions, difficult to compare answers, and honesty of the participants cannot be guaranteed. However, this was the only pragmatic approach to explore participants’ thoughts and feelings about POCUS usage. Despite the limitations, the study has highlighted important barriers that will improve the utilization of POCUS in the emergency department if addressed appropriately.
Conclusion
Presently, POCUS is moderately used by EM consultants, and the perceived barriers to its full use include time constraints, lack of national guidelines, and credentialing of the faculty. Blended learning appears to be the preferred approach towards acquiring the knowledge and skills of POCUS. POCUS utilization in EM may be further enhanced after addressing the perceived barriers.
Acknowledgment
Open access funding provided by the Qatar National Library.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Diercks DB, Mehrotra A, Nazarian DJ, et al. Clinical policy: critical issues in the evaluation of adult patients presenting to the emergency department with acute blunt abdominal trauma. Ann Emerg Med. 2011;57:387–404. doi:10.1016/j.annemergmed.2011.01.013
2. Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med. 2011;364(8):749–757. doi:10.1056/NEJMra0909487
3. Diprose W, Verster F, Schauer C. Re-examining physical findings with point-of-care ultrasound: a narrative review. NZ Med J. 2017;130(1449):46–51.
4. Lichtenstein D, Mezière G. A lung ultrasound sign allowing bedside distinction between pulmonary edema and COPD: the comet-tail artifact. Intensive Care Med. 1998;24(12):1331–1334. doi:10.1007/s001340050771
5. Sisley AC, Rozycki GS, Ballard RB, Namias N, Salomone JP, Feliciano DV. Rapid detection of traumatic effusion using surgeon-performed ultrasonography. J Trauma Acute Care Surg. 1998;44(2):291–297. doi:10.1097/00005373-199802000-00009
6. Goldberg BB, Goodman GA, Clearfield HR. Evaluation of ascites by ultrasound. Radiology. 1970;96(1):15–22. doi:10.1148/96.1.15
7. Mourad M, Ranji S, Sliwka D. A randomized controlled trial of the impact of a teaching procedure service on the training of internal medicine residents. J Grad Med Educ. 2012;4(2):170–175. doi:10.4300/JGME-D-11-00136.1
8. Nazeer SR, Dewbre H, Miller AH. Ultrasound-assisted paracentesis performed by emergency physicians vs the traditional technique: a prospective, randomized study. Am J Emerg Med. 2005;23(3):363–367. doi:10.1016/j.ajem.2004.11.001
9. Shiloh AL, Savel RH, Paulin LM, Eisen LA. Ultrasound-guided catheterization of the radial artery: a systematic review and meta-analysis of randomized controlled trials. Chest. 2011;139(3):524–529. doi:10.1378/chest.10-0919
10. Sibbitt JW, Kettwich L, Band P, et al. Does ultrasound guidance improve the outcomes of arthrocentesis and corticosteroid injection of the knee? Scand J Rheumatol. 2012;41(1):66–72. doi:10.3109/03009742.2011.599071
11. Atkinson P, Bowra J, Lambert M, Lamprecht H, Noble V, Jarman B. International Federation for Emergency Medicine point of care ultrasound curriculum. Can J Emerg Med. 2015;17(2):161–170. doi:10.1017/cem.2015.8
12. Galusko V, Khanji MY, Bodger O, Weston C, Chambers J, Ionescu A. Hand-held ultrasound scanners in medical education: a systematic review. J Cardiovasc Ultrasound. 2017;25(3):75–83. doi:10.4250/jcu.2017.25.3.75
13. Baltarowich OH, Di Salvo DN, Scoutt LM, et al. National ultrasound curriculum for medical students. Ultrasound Q. 2014;30(1):13–19. doi:10.1097/RUQ.0000000000000066
14. Hoppmann RA, Rao VV, Poston MB, et al. An integrated ultrasound curriculum (iUSC) for medical students: 4-year experience. Crit Ultrasound J. 2011;3(1):1. doi:10.1007/s13089-011-0052-9
15. Boniface KS, Ogle K, Aalam A, et al. Direct observation assessment of ultrasound competency using a mobile standardized direct observation tool application with comparison to asynchronous quality assurance evaluation. AEM Educ Train. 2019;3(2):172–178. doi:10.1002/aet2.10324
16. Care C. Perceived barriers in the use of point of care ultrasound in the WWAMI region. J Emerg Med Crit Care. 2015;1(1):1–4.
17. Prober CG, Heath C. Lecture halls without lectures—a proposal for medical education. N Engl J Med. 2012;366(18):1657–1659. doi:10.1056/NEJMp1202451
18. Bashir K, Thomas S. Educational approach of blended learning in teaching benign paroxysmal positional vertigo in an emergency department. J Coll Physicians Surg Pak. 2020;30(3):299–303. doi:10.29271/jcpsp.2020.03.299
19. Arias A, Scott R, Peters OA, McClain E, Gluskin AH. Educational outcomes of small-group discussion versus traditional lecture format in dental students’ learning and skills acquisition. J Dent Educ. 2016;80(4):459–465. doi:10.1002/j.0022-0337.2016.80.4.tb06104.x
20. Stuart J, Rutherford R. Medical student concentration during lectures. Lancet. 1978;312:514–516. doi:10.1016/S0140-6736(78)92233-X
21. Liu Q, Peng W, Zhang F, Hu R, Li Y, Yan W. The effectiveness of blended learning in health professions: systematic review and meta-analysis. J Med Internet Res. 2016;18:e2. doi:10.2196/jmir.4807
22. Rizvi NF, Gulzar S, Nicholas W, Nkoroi B. Barriers in adopting blended learning in a private university of Pakistan and East Africa: faculty members’ perspective. Mhealth. 2017;3:18. doi:10.21037/mhealth.2017.04.04
23. Peh WM, Kang ML. A pilot survey on an understanding of point of care bedside ultrasound (POCUS) among medical doctors in internal medicine: exposure, perceptions, interest and barriers to training. Proc Singapore Healthc. 2018;27(2):85–95. doi:10.1177/2010105817731412
24. Dalai C, Dversdal RK. Perceived barriers and facilitators to the use of point-of-care ultrasound for clinicians in Oregon. POCUS J. 2019;4(2):20–21. doi:10.24908/pocus.v4i2.13691
25. Wong J, Montague S, Wallace P, et al. Barriers to learning and using point-of-care ultrasound: a survey of practicing internists in six North American institutions. Ultrasound J 12, 19 (2020). the WWAMI region. J Emerg Med Critl Care. 2015;1(1).
26. Blaivas M, Pawl R. Analysis of lawsuits filed against emergency physicians for point-of-care emergency ultrasound examination performance and interpretation over a 20-year period. Am J Emerg Med. 2012;30:338–341. doi:10.1016/j.ajem.2010.12.016
27. Bashir K, Azad A, Kaleelullah Saleem Farook M, et al. Emergency medicine residents’ acquisition of point-of-care ultrasound knowledge and their satisfaction with the flipped classroom andragogy. POCUS J. 2018;3(1):2–5. doi:10.24908/pocus.v3i1.13301
28. Evans KH, Thompson AC, O’Brien C, et al. An innovative blended preclinical curriculum in clinical epidemiology and biostatistics: impact on student satisfaction and performance. Acad Med. 2016;91(5):696–700. doi:10.1097/ACM.0000000000001085
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.