Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Current Perspectives on Photodynamic Therapy for Skin Diseases: A Narrative Review
Authors Beutler K, Nowicka D, Chilicka-Hebel K ![]()
Received 5 April 2026
Accepted for publication 13 June 2026
Published 16 June 2026 Volume 2026:19 614649
DOI https://doi.org/10.2147/CCID.S614649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Katarzyna Beutler,1 Danuta Nowicka,2 Karolina Chilicka-Hebel3
1University Centre of General Dermatology and Oncodermatology, Wroclaw Medical University, Wroclaw, Poland; 2Division of Aesthetic Dermatology and Regenerative Medicine of the Skin, Wroclaw Medical University, Wroclaw, Poland; 3Department of Health Sciences, Institute of Health Sciences, University of Opole, Opole, Poland
Correspondence: Karolina Chilicka-Hebel, Email [email protected]
Abstract: Photodynamic therapy (PDT) is a minimally invasive treatment widely used in dermatology for various skin diseases. It works through the interaction of a photosensitizer, light, and oxygen, producing reactive oxygen species that selectively destroy abnormal cells. PDT is well established in treating conditions such as actinic keratosis, Bowen’s disease, and superficial basal cell carcinoma, with good cosmetic outcomes. Increasing evidence also supports its use in non-cancerous conditions, including acne, photoaging, and certain infections. Despite its advantages, limitations such as treatment-related pain and reduced effectiveness in thicker lesions remain challenges. Ongoing research aims to improve photosensitizers, delivery methods, and light technologies to enhance its clinical effectiveness.
Keywords: photodynamic therapy, skin diseases, acne vulgaris, photorejuvenation, warts
Introduction
Photodynamic therapy (PDT) is a modern, minimally invasive treatment method in which a light-sensitive substance (photosensitiser) is selectively accumulated in diseased tissues and then activated by light of a specific wavelength. Activation produces reactive oxygen species (mainly singlet oxygen and other reactive oxygen species), which destroy target cells through apoptosis or necrosis, while limiting damage to healthy tissue. Additionally, the PDT process has immunomodulatory effects that may aid in the removal of skin lesions. These effects include the stimulation of immune system cells and the production of a local inflammatory response. Photodynamic therapy in dermatology is used for registered indications, but also off-label. Apart from dermatology, PDT is utilized in urology, surgery, gynecology, microbiology and dentistry.1–6 The use of light in conjunction with photosensitizing substances for therapeutic purposes has a long history. For thousands of years, different civilizations realized that they could cure a variety of skin conditions by combining sunlight with different plants. However, the phrase “photodynamic action” was first used around a century ago by Hermann von Tappeiner to characterize an oxygen-dependent response after photosensitization, which laid the scientific basis for PDT. He observed that dye and light by themselves did not result in cell death in the absence of oxygen. Using eosin as the photosensitizer to treat a variety of skin disorders, such as condyloma lata and non-melanoma skin cancer, he finally documented the first human cases of PDT. Hematoporphyrin was the most thoroughly researched photosensitizer throughout the ensuing decades. However, hematoporphyrin’s extended phototoxicity limited its therapeutic value because it had to be given intravenously and removed from tissue extremely slowly. Kennedy’s 1990 study on the use of visible light and 5-aminolevulinic acid (5-ALA) for topical PDT therapy of the skin was a groundbreaking development. Because ALA quickly removed itself from the body and readily entered damaged or aberrant stratum corneum, it was revolutionary. Kennedy and colleagues achieved a 90% full response rate while treating basal cell carcinoma with a single treatment. PDT procedures have changed extensively since they were first introduced in terms of improving patient safety and technique effectiveness.3,7
Mechanism of Action of Photodynamic Therapy
In photodynamic treatment, a photosensitizer is excited by absorbing photons of light at a suitable wavelength, which starts a sequence of photophysical reactions that produce reactive oxygen species. When a photosensitizer molecule in its ground state (S0) absorbs a photon of light at a wavelength that matches its absorption spectrum, the excitation process starts. The energy difference between the photosensitizer’s ground state and excited state must be equal to the photon energy. An excited singlet state (S1) is created when an electron in the photosensitizer molecule is moved to a higher molecular orbital upon photon absorption. The endogenously generated protoporphyrin IX (PpIX) has distinctive absorption peaks at 400–410 nm (Soret band) and at 635 nm in the case of the most widely used photosensitizers in dermatology based on 5-aminolevulinic acid (5-ALA) or its methyl ester (MAL). When PpIX is exposed to light at these wavelengths, the molecule is excited and light energy is absorbed.The excited singlet state (S1) can experience many deactivation processes and is comparatively short-lived. Intersystem crossover (ISC), which occurs when an excited photosensitizer in the singlet state changes into a long-lived triplet state (T1), is the most crucial mechanism for PDT. One of the electrons’ spins is inverted in the triplet state, creating two unpaired electrons with parallel spins. With a lifespan of microseconds to milliseconds as opposed to nanoseconds for the singlet state, this state is far more stable than the latter. Because it allows the excited photosensitizer to interact with molecular oxygen or other biological substrates, the triplet state’s extended lifespan is essential for PDT efficiency.8,9
The main photosensitizing drugs in dermatological photodynamic treatment are 5-aminolevulinic acid (5-ALA) and its derivative, methyl aminolevulinate (MAL). Both substances work as prodrugs; when applied topically to the skin, they are absorbed by cells and metabolized via the heme biosynthesis pathway to create protoporphyrin IX (PpIX), the actual photoactive photosensitizer, which is then triggered by visible light. The porphyrin-heme biosynthesis pathway’s first committed intermediate is ALA. ALA synthase strictly controls the synthesis of ALA under physiological conditions through a negative feedback process that is controlled by the intracellular concentration of free heme. Applying exogenous ALA topically circumvents this rate-limiting enzymatic step and overwhelms the cell’s ability to use ferrochelatase, the pathway’s last enzyme, to convert PpIX into heme. As a result, photosensitizing PpIX concentrations build up inside cells. Crucially, PpIX accumulates preferentially in malignant and precancerous cells for a number of reasons, including a compromised epidermal barrier that allows ALA penetration, altered heme pathway enzyme activity (including decreased ferrochelatase activity), and a slower conversion of PpIX to heme. By limiting photodynamic damage to sick tissue while protecting nearby healthy cells, this differential accumulation guarantees the therapy’s selectivity. Because of its low molecular weight, ALA may readily pass through the stratum corneum. It has been demonstrated that the maximum PpIX concentration occurs about 6 hours after the conclusion of a 4-hour incubation period, and the skin clears it within 24 to 50 hours.3,10
The methyl ester derivative of ALA is called methyl aminolevulinate (MAL). The methyl ester group increases the molecule’s lipophilicity and improves its ability to pass through the skin barrier. After topical administration, intracellular esterases must first demethylate MAL back to ALA before it can enter the heme biosynthesis pathway and be converted to PpIX. MAL has been demonstrated to quickly attain peak intracellular concentrations of PpIX, allowing for a shorter incubation period than ALA, even though this extra enzymatic step may theoretically reduce the availability of free ALA. Similar to ALA, PpIX produced from MAL ensures therapeutic selectivity by preferentially accumulating in malignant and precancerous cells. After PpIX has accumulated in target cells, it is activated by exposure to visible light at wavelengths that match its absorption spectra, which contains maxima at 635 nm and 400–410 nm (the Soret band). PpIX molecules undergo intersystem crossing to reach a longer-lived triplet state after being stimulated from their ground state to an excited singlet state by light energy absorption. Singlet oxygen and other reactive oxygen species that cause cytotoxic damage to the target cells are produced when energy is transferred from this triplet state to molecular oxygen. The primary photocytotoxic route of photosensitizers like 5-ALA and MAL is the production of singlet oxygen, which depends on the simultaneous existence of molecular oxygen. This reaction mechanism is mostly Type II.3,11
There are two different types of photochemical reactions that make up the mechanism of action of photodynamic treatment: Type I and Type II, which have fundamentally different paths of reactive oxygen species formation and oxygen dependence.12,13 In type I reactions, the excited triplet state of the photosensitizer transfers electrons or hydrogen atoms straight to molecular oxygen or biological substrate molecules like lipids, proteins, or nucleic acids. Superoxide anion radical (O2•−), hydroxyl radical (•OH), and hydrogen peroxide (H2O2) are among the radical species produced by this electron transfer mechanism.
Because these radicals do not need high molecular oxygen concentrations to develop, they can harm target cells even under relative hypoxia. The extremely reactive hydroxyl radical, which can cause delayed oxidation events in cells, is derived from the superoxide anion radical by dismutation into hydrogen peroxide. Because of their decreased reliance on oxygen levels, type I photosensitizers have drawn more attention. This makes them especially useful for treating the hypoxic tumor microenvironments found in solid tumors. According to recent studies, the primary photochemical mechanism behind Type I PDT is intermolecular electron transfer, or Interet (Figure 1). Despite new approaches including cyclometalation with thiophenyl-based ligands, conjugation with fluorophores, and biotinylation of conventional photosensitizers, the creation of Type I photosensitizers is still difficult due to a lack of mechanistic knowledge.12–17
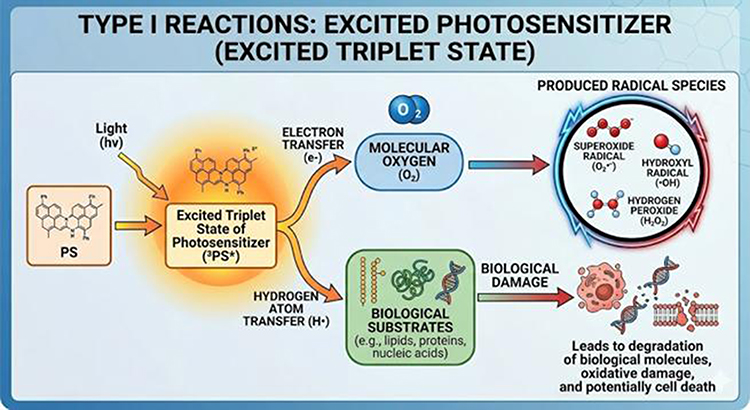 |
Figure 1 Mechanism of Type I Photodynamic Reactions. |
Singlet oxygen (1O2), a highly reactive and powerful oxidant, is produced in Type II reactions when the excited triplet state photosensitizer immediately transfers energy to ground-state molecular oxygen (3O2). The primary photocytotoxic species thought to be in charge of the early photodynamic reactions in Type II PDT is singlet oxygen. This very reactive species oxidizes proteins, lipids, and DNA, causing necrosis or apoptosis, which results in cell death. Because singlet oxygen in biological systems has a very short lifespan (usually microseconds) and a diffusion distance of only 10–300 nm, cellular damage mostly happens in the immediate area of the photosensitizer location. The majority of conventional photosensitizers used in dermatology employ type II PDT, which is the most prevalent functioning mechanism for clinically authorized photosensitizers (Figure 2).
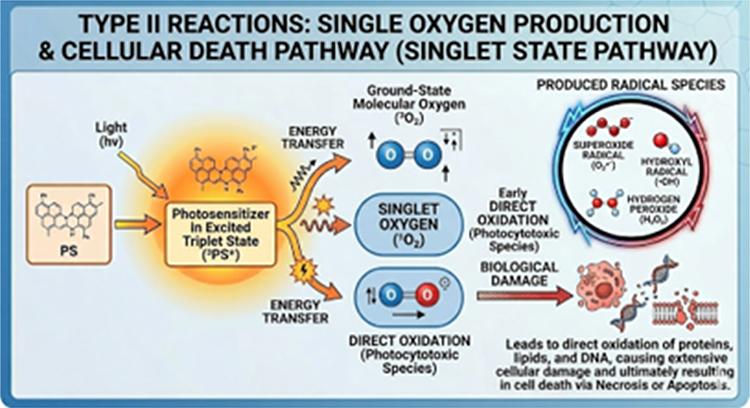 |
Figure 2 Mechanism of Type II Photodynamic Reactions. |
However, this mechanism’s effectiveness in hypoxic tumor settings may be limited because of its strong reliance on oxygen supply. The traditional view of oxygen reliance has been called into question by recent research, which suggests that effective singlet oxygen synthesis may take place even in hypoxic environments if specific kinetic characteristics are satisfied.14,18–20
In order to optimize therapeutic efficacy over a range of oxygen concentrations, dual Type I/Type II mechanisms are becoming more and more important in modern photosensitizer design. Under hypoxic circumstances, photosensitizers that can concurrently produce singlet oxygen and superoxide anion radicals exhibit increased cytotoxicity and better performance.
The oxygen restriction that has hitherto limited PDT efficacy in solid tumors can be overcome with this combinatorial approach. Most photosensitizers utilized in clinical dermatological practice, especially the endogenous photosensitizer protoporphyrin IX produced from 5-aminolevulinic acid (5-ALA) or methyl aminolevulinate (MAL), mostly create singlet oxygen through the Type II mechanism. Nonetheless, research and development of chemicals that support the Type I mechanism is ongoing, especially for use in hypoxic environments where traditional Type II PDT may be less successful.3,5,14,15,17,21,22
Clinical Protocol of Photodynamic Therapy in Dermatology
Lesion preparation, photosensitizer administration and incubation, light illumination, and post-treatment care are all crucial steps in the multi-stage process of photodynamic therapy in dermatology. To maximize treatment efficacy while reducing side effects, each step must be properly carried out. The clinical indication, the photosensitizer used, and the treatment protocol chosen (conventional PDT, daylight PDT, or modified low-pain protocols) all affect the particular parameters of each step, including the choice of photosensitizer formulation, incubation time, light source, fluence, and irradiance.3,6,23 Preparing the target lesion to maximize photosensitizer penetration into the diseased tissue is the first and most important stage in the PDT process. A major physical obstacle to the topical absorption of ALA and MAL is the stratum corneum and any overlaying hyperkeratosis, crusts, or scales; their removal has been demonstrated to significantly increase the intracellular accumulation of protoporphyrin IX (PpIX). To eliminate hyperkeratoses, increase photosensitizer absorption, and boost therapy effectiveness, European PDT guidelines advise skin preparation prior to topical photosensitizer application.24,25 Scales, crusts, and the superficial hyperkeratotic layer are removed from the lesion surface using a curette or sharp spoon as part of the normal preparation procedure, being careful to prevent excessive bleeding. The treatment region should be cleaned with a cotton pad soaked in ethanol or isopropanol before curettage. Curettage significantly increases PpIX fluorescence for MAL from 1 to 21 hours after application (P < 0.0041), supporting its use as a routine pretreatment technique, according to a randomized clinical trial by Bay et al24 Additionally, Nissen et al endorsed curettage as the conventional pretreatment in PDT by demonstrating that it is superior to short-term chemical pretreatment in boosting PpIX fluorescence from 1 to 5 hours.26
Alternative pretreatment techniques have been investigated since curettage can be uncomfortable and may result in bleeding and leaking. It has been demonstrated that chemical keratolytic pretreatment using topical agents like 10% salicylic acid, 40% urea cream, or 30% urea cream applied for 1–7 days prior to PDT can achieve lesion response rates comparable to curettage, albeit with more noticeable local reactions and possibly increased pain during illumination. According to a randomized clinical experiment by Caccavale et al, a mean lesion reduction of 54.7% was obtained with daylight PDT without curettage, although this was not substantially different from the 58.7% reduction obtained with normal curettage (P > 0.05) after 7 days of 30% urea cream administration.27 Additionally, more sophisticated physical pretreatment methods have been studied. Pretreatment with ablative fractional laser (AFXL) produces vertical ablation channels in the skin that greatly improve PpIX accumulation and photosensitizer penetration. In a randomized clinical experiment, Bay et al showed that a single pass was adequate to enhance photosensitizer absorption and that AFXL pretreatment produced the greatest and most homogenous PpIX fluorescence, far surpassing curettage, microdermabrasion, and microneedling. Other options that perforate or thin the stratum corneum are microneedling and microdermabrasion, which have demonstrated intermediate PpIX-enhancing potential similar to curettage.24,25
The topical photosensitizer is administered to the treatment region once the lesion has been prepared. The particular product and the treatment procedure being employed determine the photosensitizer composition and incubation settings. There are several formulas for ALA-based preparations. When combined with blue light illumination, ALA 20% topical solution (Levulan Kerastick) was the first photosensitizer authorized by the FDA in the United States in 1999 for the treatment of nonhyperkeratotic actinic keratoses on the face and scalp. According to the original FDA procedure, blue light irradiation at 10 J/cm2 was followed by an incubation period of 14 to 18 hours.3 More recently, mild-to-moderate actinic keratoses on the face and scalp have been approved for lesion-directed and field-directed therapy with ALA 10% gel in a nanoemulsion formulation (Ameluz) in conjunction with red light PDT utilizing the BF-RhodoLED or RhodoLED XL lamp. The Ameluz technique entails applying a layer of gel that is about 1 mm thick to the lesion or lesions and about 5 mm of surrounding skin, occlusion for three hours, and then red light illumination.28 The conventional European approach for MAL (methyl aminolevulinate) is applying a 1 mm thick coating of MAL cream (Metvix/Metvixia, 160 mg/g) to the prepared lesion and surrounding 5–10 mm of normal skin. This is followed by three hours of occlusion with an adhesive, light-opaque dressing. The occlusive dressing has two functions: it keeps the environment moist, which promotes photosensitizer absorption, and it stops ambient light from prematurely photoactivating PpIX.3,6 One important factor that directly affects the quantity of PpIX accumulated in target cells and, in turn, the therapeutic effectiveness is the incubation duration. To improve full removal of actinic keratoses, the AAD Work Group conditionally suggests longer treatment durations (1–4 hours) over shorter application times. Protocols usually need a 3-hour application period prior to 10 minutes of red light activation for the 10% ALA gel (Ameluz). In order to cut down on clinic time and patient discomfort, shorter incubation protocols have been studied. Some studies have shown that treatments with incubation times as short as 30 minutes to 1 hour can be effective, especially when combined with improved pretreatment methods or daylight activation.29 Following the incubation time, the treatment region is exposed to light of the proper wavelength to activate the deposited PpIX after the occlusive dressing and any remaining photosensitizer cream are removed. The choice of light source, wavelength, irradiance (power density in mW/cm2), and fluence (total light dosage in J/cm2) are important factors that affect the therapeutic result.3,30
Dermatological PDT uses a variety of light source types, each with unique spectrum properties and therapeutic uses. In clinical PDT treatment, light-emitting diodes (LEDs) are the most often utilized light sources. Through small semiconductor devices, they offer a limited spectrum of light irradiation, usually within a bandwidth of 20 to 50 nm. The usual light source for MAL-PDT and ALA gel-PDT in Europe is red LED lamps (peak emission at 630–635 nm), which provide a typical light dosage of 37 J/cm2 over around 8–10 minutes of illumination. The common light source for ALA solution-PDT in the US is a blue LED lamp (peak emission at 400–420 nm), which provides a typical light dosage of 10 J/cm2 for around 1,000 seconds (16 minutes 40 seconds). Because blue light stimulates PpIX more effectively than red light at the Soret band absorption peak, the effective photobleaching dosage for a light source at around 405 nm is 10 J/cm2, whereas it is 100 J/cm2 for a light source at 635 nm. In order to match absorption peaks throughout the porphyrin curve, lasers deliver precise amounts of light radiation at certain wavelengths. Tunable argon dye lasers (blue-green light, 450–530 nm), copper vapor laser-pumped dye lasers (510–578 nm), long-pulse pulsed dye lasers (585–595 nm), Nd:YAG KTP dye lasers (532 nm), gold vapor lasers (628 nm), and solid-state diode lasers (630 nm) are among the lasers used in PDT. Although lasers provide high irradiance and accurate wavelength selection, they are more costly and cover smaller areas than LED panels.3 Natural or artificial daylight offers a wide range of visible light that concurrently activates PpIX over several absorption peaks, such as the Q-bands (505, 540, 580, and 635 nm) and the Soret band (400–410 nm). Depending on the weather, the effective light dosage from daylight can range from 3 ± 0.4 J/cm2 on cloudy days to 44 ± 6 J/cm2 on bright, sunny days. Despite this fluctuation, it has been demonstrated that even comparatively low ambient light levels are enough for PpIX activation in daytime PDT regimens.31,32 For red light PDT, the typical fluence is 37 J/cm2 administered over 8–10 minutes at an irradiance of around 50–100 mW/cm2. The usual fluence for blue light PDT is 10 J/cm2 given over around 1,000 seconds.
Tanew et al ‘s randomized controlled trial, however, showed that lowering the fluence rate and/or light dosage was linked to noticeably decreased PDT-induced discomfort without sacrificing the therapeutic effectiveness of traditional PDT for actinic keratoses in the head area. While the overall clearance rates at three and six months did not differ between the four treatment protocols tested (standard dose/standard rate, standard dose/halved rate, halved dose/standard rate, and halved dose/halved rate), the mean and maximum pain levels during illumination were significantly reduced at lower fluence rates.30 Below a threshold (about 60 mW/cm2 for irradiance and 50 J/cm2 for fluence), pain during illumination is positively correlated with fluence rate and dosage; when this threshold is exceeded, pain intensity saturates.This finding implies that lowering irradiance below this threshold might significantly reduce patient pain without necessarily sacrificing effectiveness, which has significant therapeutic implications.33
The most serious acute side impact and the main reason limiting patient compliance during PDT illumination is pain. Patients frequently describe their pain as searing, and it usually peaks in the first few minutes of therapy. Research utilizing the visual analog scale (VAS) has shown that about 20% of patients suffer pain that is assessed at 6 or higher on a 10-point scale, which is regarded as substantial and might result in lower compliance.3,33,34 With reactive oxygen species, transient receptor potential (TRP) channels, and inflammatory responses acting as important mediators, the mechanism of PDT-associated pain is believed to be secondary to the interaction between inflammation brought on by cell necrosis and stimulation of myelinated A-delta and unmyelinated C nerve fibers. Pain intensity is influenced by a number of factors, such as the type of photosensitizer (MAL-PDT is typically less painful than ALA-PDT), the location and type of lesion (areas with many nerve endings, like the hands and head, are more painful), the surface area treated (areas >130 mm2 are more painful), and the irradiance and fluence delivered.3,33 There are a number of evidence-based methods for managing discomfort during PDT. The most popular technique is cold air analgesia because freezing the skin activates A-delta fibers, which prevent the transmission of pain. However, excessive cooling should be utilized carefully as it may lower PpIX photobleaching and clinical clearance rates; to make up for this, treatment duration or incubation time may be extended. It has been demonstrated that employing cold water spray or cold water packs in conjunction with a 3-minute light interruption during therapy can lower pain intensity by 3.0–3.7 VAS points without reducing therapeutic efficacy. The best way to relieve pain is using nerve blocks. In contrast to intravenous analgesia (7.3 ± 1.1) and cold air analgesia alone (8.4 ± 2.0), scalp nerve blocks dramatically decreased maximal discomfort during PDT to a VAS of 2.1 ± 1.3 (P < 0.05). For PDT of the face, facial and supratrochlear/supraorbital nerve blocks have also proven to be more effective than cold air.
Injectable anesthetics should be used without vasoconstrictors to maintain sufficient oxygen flow, which is necessary for the photodynamic reaction, and are usually saved for situations where noninvasive techniques have failed due to the additional time and expense involved (Figure 3).
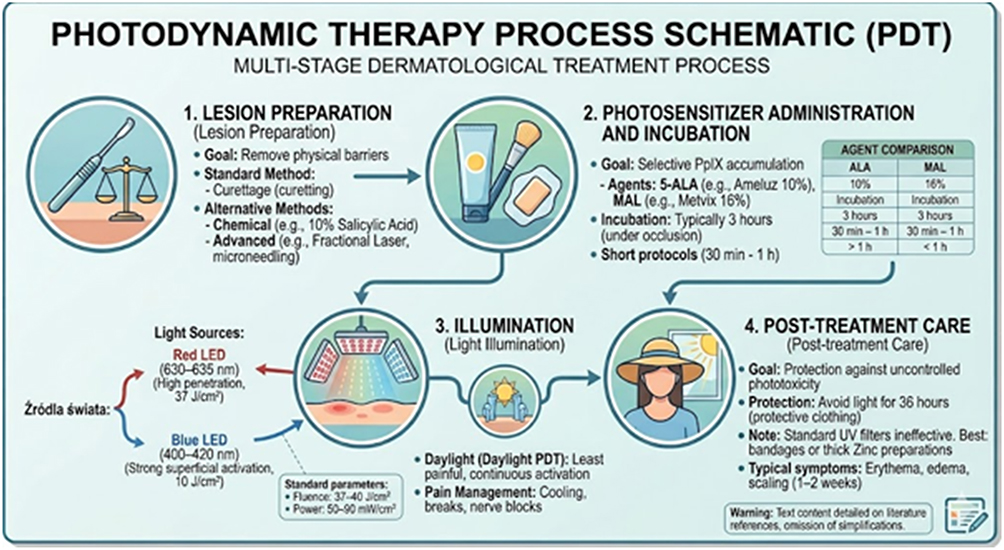 |
Figure 3 Procedural Workflow of Photodynamic Therapy (PDT) in Dermatology. |
By reducing the rate of reactive oxygen species formation, reduced irradiance protocols—such as daylight PDT and other modified low-pain protocols—represent the most efficient method of reducing pain.3,33,35 To maximize healing and reduce problems after lighting, proper post-treatment care is crucial. Since PpIX remains in the skin for 24 to 48 hours following treatment and exposure to ambient light might result in further phototoxic responses, patients are advised to stay indoors and avoid being outside from dawn to nightfall for 36 hours following the operation. If going outside is required, the best strategy to prevent more photoreactivity is to cover up with opaque clothes and a wide-brimmed hat. It should be noted that normal UV-blocking sunscreens, such as formulations containing micronized zinc oxide or titanium dioxide, are ineffective in blocking visible light wavelengths that activate PpIX and should not be used for post-PDT light protection unless they are applied in a thick, impenetrable film. It has been demonstrated that light-blocking plaster offers the best defense against post-PDT daylight exposure, lowering erythema by 44% as opposed to 19% for inorganic sunscreen and 27% for foundation (P = 0.002 for plaster). Patients may unintentionally be exposed to ambient light sources, such as fluorescent lights or sunlight from windows, if they feel tingling or stinging inside. They should be instructed to keep at least six feet away from any window.3,36 The phototoxic inflammatory response is the main cause of PDT’s immediate negative effects. The most frequent side effect, erythema, affects around 89% of patients, peaks 1–2 hours after irradiation, and typically goes away in 1–2 weeks. In most individuals, erythema is accompanied with edema, which usually goes away in a few days. Almost all patients report experiencing pain and burning during and just after illumination, with mean VAS values of 4.3 ± 2.5 right after treatment that rapidly go away as the light source is turned off. About 82% of patients have scaling and crusting, which usually goes away in one to two weeks. About 59% of patients have been documented to develop pustules. The inflammatory reaction may result in pigmentary alterations, such as hyperpigmentation and hypopigmentation; ALA has a higher prevalence than MAL and Fitzpatrick skin types IV–VI may be at increased risk; post-inflammatory pigmentation often goes away with time. Between 0.9% and 34% of individuals have been documented to have urticaria. Although it is uncommon, individuals who have had several treatments should be evaluated for contact allergy to photosensitizer prodrugs. Crucially, no indication of cumulative toxicity or photocarcinogenic risk has been found, and there are no notable longer-term concerns associated with topical PDT. During the healing phase, emollients and mild skin care should be used, and patients should be advised that the treated region may seem like a windburn, which will eventually go away.3,34,37 The clinical reason and the response to therapy determine how many PDT treatments are necessary. One to two treatment sessions are usually advised for actinic keratoses; the effectiveness of up to two ALA-PDT therapy sessions is supported by evidence of moderate to high confidence. Retreatment is recommended for lesions that have not entirely healed after three months of first treatment. The European protocol for Bowen’s disease and superficial basal cell carcinoma usually consists of two treatment sessions spaced one week apart, with red light exposure at 37 J/cm2 and a 3-hour MAL incubation. Aggressive repeated PDT following curettage has been studied for nodular basal cell carcinoma, with nonresponding lesions retreating at one week with a second treatment.6,29,38
Registered Indications for Photodynamic Therapy
With applications ranging from malignant and precancerous lesions, inflammatory and infectious dermatoses, and cosmetic purposes, photodynamic therapy (PDT) has established itself as a flexible, safe, and successful therapeutic method in dermatology. There are two main categories of clinical indications for PDT: authorized (registered) indications and emergent (off-label) indications. The data supporting each category varies.6,23,39
In Europe, photodynamic therapy is registered for the following dermatological indications:6
Actinic Keratosis
In dermatology, actinic keratoses (AKs) are the most well-established and commonly accepted reason for PDT. Since 1999, the FDA has only authorized PDT for the treatment of nonhyperkeratotic AKs on the face and scalp in the United States. After one to two treatment sessions employing a 14- to 18-hour incubation time followed by blue light irradiation at 10 J/cm2, the first FDA Phase II and III investigations of ALA-PDT showed clearance rates of 85% to 90%. In addition to red light PDT, ALA 10% gel (Ameluz) has recently received approval for the lesion-directed and field-directed treatment of mild-to-moderate AKs on the face and scalp.3,29 With a lesion-level complete response risk ratio (RR) of 1.87 (95% CI, 1.55–1.87) and a patient-level complete response RR of 3.07 (95% CI, 2.07–4.56), as well as better overall patient preference and cosmetic results, a thorough meta-analysis of 29 randomized controlled trials involving 3,850 participants and 24,747 lesions showed that PDT was found to be significantly more effective than other treatment modalities for AK. ALA-PDT demonstrated the best long-term participant complete clearance when compared to placebo (RR, 8.06; 95% CI, 2.07–31.37; GRADE, moderate), followed by imiquimod 5% (RR, 5.98), MAL-PDT (RR, 5.95), and cryosurgery (RR, 4.76), according to a systematic review and network meta-analysis that was published in JAMA Dermatology.40–42 According to the European Dermatology Forum (EDF) standards, PDT is a generally accepted treatment for AKs, and when normal treatment protocols are followed, recurrence rates are usually comparable to those of current treatments. PDT has the ability to prevent or slow the growth of new lesions and can be used as a field-directed or lesion-directed treatment. The data about the effectiveness of up to two ALA-PDT treatment sessions is of moderate to high certainty, according to the American Academy of Dermatology (AAD) Work Group, which conditionally supports ALA-red light PDT as a therapy for AKs. With mean pain levels of 1.7 ± 0.9 vs 5.2 ± 1.7 on an 11-point scale (P < 0.0001), the AAD also conditionally recommends ALA-daylight PDT as equally effective and less unpleasant than ALA-red light PDT.39
Squamous Cell Carcinoma in situ
Another known use for PDT is Bowen’s disease. In Bowen’s illness, complete response rates with MAL-PDT have been reported to be 68% at 24 months and 93% at 3 months. For Bowen’s illness, a retrospective comparison research revealed no statistically significant difference in full clinical response rates between ALA-PDT (89%) and MAL-PDT (78%). The European protocol usually consists of two treatment sessions spaced one week apart, each of which includes a 3-hour MAL incubation and red light illumination at 37 J/cm2. For cutaneous SCC in situ (Bowen disease), PDT (eg., ALA, porfimer sodium) is listed in the NCCN recommendations as a therapeutic option; nevertheless, cure rates are around 10% lower than for surgical therapy techniques.39,43,44
Superficial Basal Cell Carcinoma and Nodular Basal Cell Carcinoma
Superficial basal cell carcinoma (sBCC) and some thin nodular basal cell carcinomas (nBCC) can be treated with PDT. Initial clearance rates with sBCC are comparable to cryosurgery up to 60 months (75% vs. 74%) and vary from 85% to 93% at three months.
Complete response rates with nBCC vary from 75% to 82% at three months to 77% at sixty months. Nevertheless, PDT is not advised for invasive squamous cell carcinoma, and recurrence rates after PDT are greater than those after surgery for nodular BCC. Depending on the photosensitizer employed, BCC recurrence rates were 17.8% (95% CI, 9.1%–31.8%) or 16.9% (95% CI, 7.4%–34.4%) in a meta-analysis of 16 RCTs. According to the EDF recommendations, PDT often produces better cosmetic results than current conventional treatments, which is a major benefit, especially for lesions in aesthetically sensitive regions like the face.39,43,45,46
Field Cancerization
PDT is being utilized more often for field cancerization in photodamaged skin because a topical photosensitizer may be administered over vast regions. Although there is still no direct proof of preventing invasive SCC, PDT employing a nanoemulsion of ALA in a daylight or standard PDT protocol has been authorized for use in field cancerization and has the ability to postpone the formation of new AKs and BCCs.39 PDT is being researched and utilized for a variety of non-neoplastic skin disorders in addition to the recognized oncological applications. High-quality evidence supports a strong recommendation for the use of topical PDT in photorejuvenation, acne, refractory warts, cutaneous leishmaniasis, and onychomycosis, according to the EDF guidelines (Part 2, 2019). However, these indications currently lack regulatory approvals, and protocols still need to be optimized.6
Photodynamic therapy is used beyond the registered indications in, among others (Table 1).
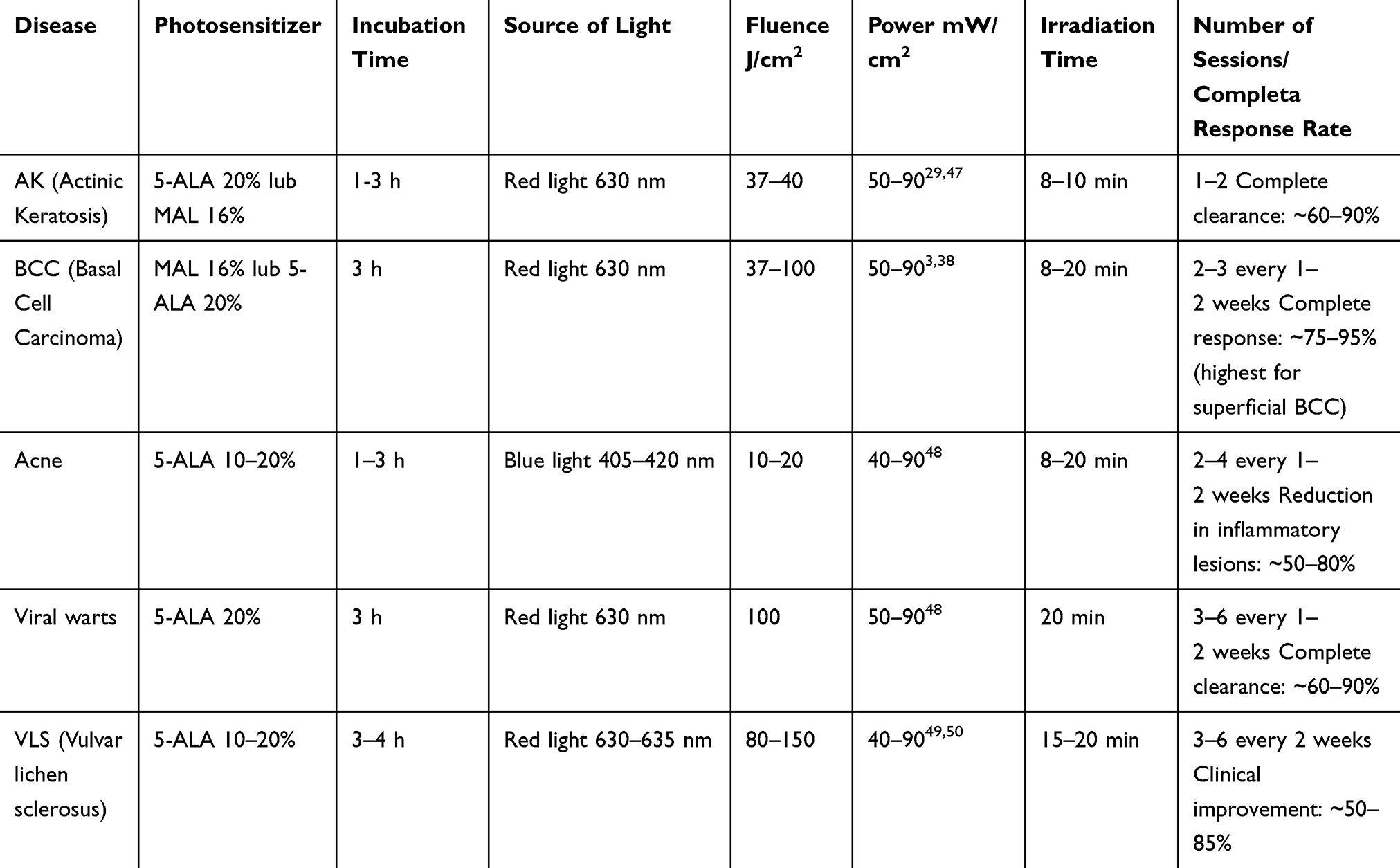 |
Table 1 Sample Photodynamic Therapy Parameters for Selected Diseases |
Lichen Sclerosus
PDT has been studied as a potential therapy for vulvar lichen sclerosus (LS). The complete response rate in the ALA-PDT group (14/20, 70%) was twice that of the clobetasol propionate group (7/20, 35%) (P < 0.05), according to a randomized comparative study. At a one-month follow-up, only one patient in the PDT group relapsed, compared to all seven responders in the clobetasol group. PDT is a useful therapeutic approach for the treatment of vulvar LS, according to a comprehensive evaluation of 20 research.49,51
Photorejuvenation
Roughness, sallowness, patchy hyperpigmentation, and fine wrinkles have all been observed to improve with PDT’s increasing usage in cosmetic dermatology for photorejuvenation. The process entails the selective elimination of photodamaged cells and the photodynamic promotion of collagen rebuilding. The use of ALA- and MAL-PDT for the treatment of certain aging and photoaging-related cosmetic alterations is firmly supported by evidence from the literature.6,52,53
Acne Vulgaris
PDT has become a viable treatment for acne vulgaris, especially for individuals who are not good candidates for isotretinoin and have not responded to topical therapy and oral antibacterials. Red light was the most commonly employed light source, and both ALA and MAL showed comparable effectiveness, according to a comprehensive evaluation of 69 clinical trials, 4 case reports, and 2 retrospective investigations. Both inflammatory and non-inflammatory lesions responded to therapy; in the majority of investigations, inflammatory lesions showed higher clearance. Mild adverse effects included erythema and edema following the procedure, as well as discomfort upon light. Acne is caused by the selective build-up of PpIX in the pilosebaceous unit, which reduces the colonization of Propionibacterium acnes and destroys sebaceous glands.5,54
Refractory Warts, Plane and Genital Warts
Although there is growing evidence to support the use of PDT for refractory viral warts, its general acceptance has been hampered by the severe discomfort it can cause during treatment. Despite its shown effectiveness, PDT is usually saved for warts that have not responded to traditional treatments such topical medications and cryotherapy.6,52
Cutaneous Leishmaniasis
Evidence from both controlled and uncontrolled research supports the use of PDT as an alternative to traditional therapy for cutaneous leishmaniasis, especially in situations when normal treatments are ineffective. The process entails the development of a local immune response and the direct photodynamic killing of Leishmania parasites within macrophages. Other conditions Condylomata acuminata, onychomycosis, atypical mycobacteriosis, psoriasis, and chronic wounds are among the other conditions for which PDT has been studied; however, the level of evidence for the majority of these conditions is still lower, and controlled randomized studies with extended follow-ups are required to establish clinical usefulness.23,52
Conclusions
In dermatology, photodynamic therapy (PDT) is a novel therapeutic approach that uses the interaction of three key elements—a photosensitizer, light with the right wavelength, and molecular oxygen—to selectively destroy pathological tissue while protecting nearby healthy structures. Protoporphyrin IX (PpIX), an active photosensitizer, is produced by the topical administration of prodrugs, mainly 5-aminolevulinic acid (ALA) or methyl aminolevulinate (MAL), which are preferentially absorbed by target cells and processed intracellularly. PpIX is stimulated from its ground state (S0) to higher singlet excited states (S1, S2) upon absorption of light energy. This is followed by intersystem crossover to the triplet excited state (T1). The photosensitizer can engage in two different kinds of photochemical reactions from this metastable triplet state: While Type II reactions transmit energy to molecular oxygen and produce extremely reactive singlet oxygen (1O2), Type I reactions directly transfer electrons or hydrogen atoms to biological substrates, creating free radicals such superoxide anion and hydroxyl radicals. Since Type II responses are more common for ALA and MAL in clinical dermatological practice, sufficient tissue oxygenation is crucial for treatment effectiveness.PDT’s cytotoxic effects are mediated by a variety of mechanisms, such as direct cellular damage caused by oxidation of lipids, proteins, and nucleic acids that results in necrosis or apoptosis; vascular damage that causes ischemia of the target tissue; and immunomodulatory effects that trigger both innate and adaptive immune responses against remaining pathological cells. This complex process adds to PDT’s good therapeutic index and underpins its clinical adaptability.3,6,23,39 Actinic keratoses, Bowen’s disease, and superficial basal cell carcinoma are the best-documented and regulatory-approved indications for PDT, which has proven to be a safe and effective treatment for malignant and precancerous skin lesions from a clinical standpoint. There is no indication of cumulative toxicity or photocarcinogenic risk with long-term usage, and the safety profile is quite good. The only side effects are temporary erythema, edema, discomfort, and crusting that usually go away in a few days to two weeks.34,42 In addition to oncological indications, PDT is being used more frequently for aesthetic purposes like photorejuvenation as well as inflammatory and infectious dermatoses like acne vulgaris, viral warts, cutaneous leishmaniasis, and lichen sclerosus. However, standardized procedures and regulatory approvals for these new uses are still pending.6,39 In summary, PDT’s distinct photophysical and photochemical characteristics, along with its favorable efficacy-to-safety ratio, excellent cosmetic results, repeatability without cumulative toxicity, and applicability to both large treatment fields and localized lesions, make it an indispensable and constantly developing tool in the current dermatological therapeutic arsenal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gheybi E, Hosseinzadeh P, Tayebi-Khorrami V, Rostami M, Soukhtanloo M. From reactive oxygen to cancer cell death: the science behind photodynamic therapy. Lasers Med Sci. 2025;40(1):448. doi:10.1007/s10103-025-04707-1
2. Kwiatkowski S, Knap B, Przystupski D, et al. Photodynamic therapy – mechanisms, photosensitizers and combinations. Biomed Pharmacother. 2018;106:1098–13. doi:10.1016/j.biopha.2018.07.049
3. Ozog DM, Rkein AM, Fabi SG, et al. Photodynamic therapy: a clinical consensus guide. Dermatol Surg. 2016;42(7):804–827. doi:10.1097/DSS.0000000000000800
4. Aebisher D, Czech S, Dynarowicz K, et al. Photodynamic therapy: past, current, and future. Int J Mol Sci. 2024;25(20):11325. doi:10.3390/ijms252011325
5. Fonda-Pascual P, Moreno-Arrones OM, Alegre-Sanchez A, et al. In situ production of ROS in the skin by photodynamic therapy as a powerful tool in clinical dermatology. Methods. 2016;109:190–202. doi:10.1016/j.ymeth.2016.07.008
6. Morton CA, Szeimies RM, Basset Séguin N, et al. European dermatology forum guidelines on topical photodynamic therapy 2019 part 2: emerging indications – field cancerization, photorejuvenation and inflammatory/infective dermatoses. J Eur Acad Dermatol Venereol. 2020;34(1):17–29. doi:10.1111/jdv.16044
7. Darlenski R, Fluhr JW. Photodynamic therapy in dermatology: past, present, and future. J Biomed Opt. 2012;18(6):061208. doi:10.1117/1.JBO.18.6.061208
8. Plaetzer K, Krammer B, Berlanda J, Berr F, Kiesslich T. Photophysics and photochemistry of photodynamic therapy: fundamental aspects. Lasers Med Sci. 2009;24(2):259–268. doi:10.1007/s10103-008-0539-1
9. Ochsner M. Photophysical and photobiological processes in the photodynamic therapy of tumours. J Photochem Photobiol B. 1997;39(1):1–18. doi:10.1016/S1011-1344(96)07428-3
10. Ohgari Y, Miyata Y, Miyagi T, et al. Roles of porphyrin and iron metabolisms in the δ-Aminolevulinic Acid (ALA)-induced accumulation of protoporphyrin and photodamage of tumor cells. Photochem Photobiol. 2011;87(5):1138–1145. doi:10.1111/j.1751-1097.2011.00950.x
11. Elmets CA, Lim HW, Stoff B, et al. Joint American academy of dermatology–national psoriasis foundation guidelines of care for the management and treatment of psoriasis with phototherapy. J Am Acad Dermatol. 2019;81(3):775–804. doi:10.1016/j.jaad.2019.04.042
12. Baptista MS, Cadet J, Di Mascio P, et al. Type I and type II photosensitized oxidation reactions: guidelines and mechanistic pathways. Photochem Photobiol. 2017;93(4):912–919. doi:10.1111/php.12716
13. Garcia-Diaz M, Huang YY, Hamblin MR. Use of fluorescent probes for ROS to tease apart type I and type II photochemical pathways in photodynamic therapy. Methods. 2016;109:158–166. doi:10.1016/j.ymeth.2016.06.025
14. An J, Tang S, Hong G, et al. An unexpected strategy to alleviate hypoxia limitation of photodynamic therapy by biotinylation of photosensitizers. Nat Commun. 2022;13(1):2225. doi:10.1038/s41467-022-29862-9
15. Jia M, Pan Y, Hu W. Intermolecular electron transfer: toward a general photochemical engine for type i photodynamic therapy. Small Methods. 2025;9(11):e01279. doi:10.1002/smtd.202501279
16. Vigueras G, Marchán V, Ruiz J. Insights into type I photoreactivity of cyclometalated iridium(
17. Li M, Xiong J, Zhang Y, et al. New guidelines and definitions for type I photodynamic therapy. Chem Soc Rev. 2025;54(15):7025–7057. doi:10.1039/D1CS01079D
18. Chang Z, Guo L, Cai J, Shu Y, Ding J, Sun Q. Oxygen concentration effect in photosensitized generation of1 O2 from normoxia to hypoxia. J Phys Chem Lett. 2024;15(44):11126–11130. doi:10.1021/acs.jpclett.4c02547
19. Cui S, Guo X, Wang S, et al. Singlet oxygen in photodynamic therapy. Pharmaceuticals. 2024;17(10):1274. doi:10.3390/ph17101274
20. Wan Y, Fu L, Li C, Lin J, Huang P. Conquering the hypoxia limitation for photodynamic therapy. Adv Mater. 2021;33(48):2103978. doi:10.1002/adma.202103978
21. Xu Z, Song Y, Sun J. Simultaneous production of singlet oxygen and superoxide anion by thiocarbonyl coumarin for photodynamic therapy. Spectrochim Acta A Mol Biomol Spectrosc. 2025;327:125327. doi:10.1016/j.saa.2024.125327
22. Liu S, Sun T, Chou W, Zhao H, Zhao Y. A design strategy of pure Type-I thiadiazolo[3,4-g]quinoxaline-based photosensitizers for photodynamic therapy. Eur J Med Chem. 2024;265:116059. doi:10.1016/j.ejmech.2023.116059
23. Balakirski G, Lehmann P, Szeimies R, Hofmann SC. Photodynamic therapy in dermatology: established and new indications. JDDG J Dtsch Dermatol Ges. 2024;22(12):1651–1662. doi:10.1111/ddg.15464
24. Bay C, Lerche CM, Ferrick B, Philipsen PA, Togsverd-Bo K, Haedersdal M. Comparison of physical pretreatment regimens to enhance protoporphyrin IX uptake in photodynamic therapy: a randomized clinical trial. JAMA Dermatol. 2017;153(4):270. doi:10.1001/jamadermatol.2016.5268
25. Liu D, Zhao S, Li J, Chen M, Wu L. The application of physical pretreatment in photodynamic therapy for skin diseases. Lasers Med Sci. 2021;36(7):1369–1377. doi:10.1007/s10103-020-03233-6
26. Nissen CV, Wiegell SR, Philipsen PA, Wulf HC. Short‐term chemical pretreatment cannot replace curettage in photodynamic therapy. Photodermatol Photoimmunol Photomed. 2016;32(3):146–152. doi:10.1111/phpp.12236
27. Caccavale S, Boccellino MP, Brancaccio G, Alfano R, Argenziano G. Keratolytics can replace curettage in daylight photodynamic therapy for actinic keratosis on the face/scalp: a randomized clinical trial. J Eur Acad Dermatol Venereol. 2024;38(3):594–601. doi:10.1111/jdv.19687
28. Biofrontera Bioscience GmbH. CHARAKTERYSTYKA PRODUKTU LECZNICZEGO Ameluz 78 Mg/g, Żel.
29. Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021;85(4):e209–e233. doi:10.1016/j.jaad.2021.02.082
30. Tanew A, Ristl R, Trattner H, Hacker V, Kroyer B, Radakovic S. Impact of light dose and fluence rate on the efficacy and tolerability of topical 5‐
31. Vignion‐Dewalle A, Baert G, Thecua E, et al. Comparison of 10 efficient protocols for photodynamic therapy of actinic keratosis: how relevant are effective light dose and local damage in predicting the complete response rate at 3 months? Lasers Surg Med. 2018;50(5):576–589. doi:10.1002/lsm.22827
32. Manley M, Collins P, Gray L, O’Gorman S, McCavana J. Quantifying the radiant exposure and effective dose in patients treated for actinic keratoses with topical photodynamic therapy using daylight and LED white light. Phys Med Biol. 2018;63(3):035013. doi:10.1088/1361-6560/aa9ea7
33. Wang B, Shi L, Zhang YF, et al. Gain with no pain? Pain management in dermatological photodynamic therapy. Br J Dermatol. 2017;177(3):656–665. doi:10.1111/bjd.15344
34. Ibbotson SH, Wong TH, Morton CA, et al. Adverse effects of topical photodynamic therapy: a consensus review and approach to management. Br J Dermatol. 2019;180(4):715–729. doi:10.1111/bjd.17131
35. Klein A, Karrer S, Horner C, et al. Comparing cold-air analgesia, systemically administered analgesia and scalp nerve blocks for pain management during photodynamic therapy for actinic keratosis of the scalp presenting as field cancerization: a randomized controlled trial. Br J Dermatol. 2015;173(1):192–200. doi:10.1111/bjd.13547
36. Petersen B, Wiegell SR, Wulf HC. Light protection of the skin after photodynamic therapy reduces inflammation: an unblinded randomized controlled study. Br J Dermatol. 2014;171(1):175–178. doi:10.1111/bjd.12882
37. Gholam P, Kroehl V, Enk AH. Dermatology life quality index and side effects after topical photodynamic therapy of actinic keratosis. Dermatology. 2013;226(3):253–259. doi:10.1159/000349992
38. Bichakjian C, Armstrong A, Baum C, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540–559. doi:10.1016/j.jaad.2017.10.006
39. Morton CA, Szeimies RM, Basset Seguin N, et al. European dermatology forum guidelines on topical photodynamic therapy 2019 part 1: treatment delivery and established indications – actinic keratoses, Bowen’s disease and basal cell carcinomas. J Eur Acad Dermatol Venereol. 2019;33(12):2225–2238. doi:10.1111/jdv.16017
40. Tian Y, Yao Y, Zhang J. Comparision of the efficacy of photodynamic therapy and imiquimod cream in patients with actinic keratosis: a systematic review and meta-analysis. Sci Rep. 2026;16(1):4370. doi:10.1038/s41598-025-34524-z
41. Steeb T, Wessely A, Petzold A, et al. Evaluation of long-term clearance rates of interventions for actinic keratosis: a systematic review and network meta-analysis. JAMA Dermatol. 2021;157(9):1066. doi:10.1001/jamadermatol.2021.2779
42. Hu C, Luo X, Jiang C, Lei S, Sun Y. Efficacy and safety of photodynamic therapy for the treatment of actinic keratoses: a meta-analysis update of randomized controlled trials. Dermatol Surg. 2023;49(6):544–551. doi:10.1097/DSS.0000000000003784
43. Lehmann P. Methyl aminolaevulinate?photodynamic therapy: a review of clinical trials in the treatment of actinic keratoses and nonmelanoma skin cancer. Br J Dermatol. 2007;156(5):793–801. doi:10.1111/j.1365-2133.2007.07833.x
44. Tarstedt M, Gillstedt M, Wennberg Larkö AM, Paoli J. Aminolevulinic acid and methyl aminolevulinate equally effective in topical photodynamic therapy for non‐melanoma skin cancers. J Eur Acad Dermatol Venereol. 2016;30(3):420–423. doi:10.1111/jdv.13558
45. Braathen LR, Szeimies RM, Basset-Seguin N, et al. Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: an international consensus. J Am Acad Dermatol. 2007;56(1):125–143. doi:10.1016/j.jaad.2006.06.006
46. Wehner MR. Keratinocyte carcinoma: a review. JAMA. 2026;335(1):70. doi:10.1001/jama.2025.18749
47. Wulf HC, Heerfordt IM. Counteracting side-effects of photodynamic therapy for actinic keratoses. Anticancer Res. 2022;42(10):5017–5020. doi:10.21873/anticanres.16009
48. Kim M, Jung H, Park H. Topical PDT in the treatment of benign skin diseases: principles and new applications. Int J Mol Sci. 2015;16(10):23259–23278. doi:10.3390/ijms161023259
49. Shi L, Miao F, Zhang LL, et al. Comparison of 5-aminolevulinic acid photodynamic therapy and clobetasol propionate in treatment of vulvar lichen sclerosus. Acta Derm Venereol. 2016;96(5):684–688. doi:10.2340/00015555-2341
50. Zhang F, Li D, Shi L, Gu Y, Xu Y, Wu C. Efficacy of 5-Aminolevulinic Acid (ALA)-Photodynamic Therapy (PDT) in refractory vulvar lichen sclerosus: preliminary results. Med Sci Monit Int Med J Exp Clin Res. 2021;27:e927406. doi:10.12659/MSM.927406
51. Gerkowicz A, Szczepanik-Kułak P, Krasowska D. Photodynamic therapy in the treatment of vulvar lichen sclerosus: a systematic review of the literature. J Clin Med. 2021;10(23):5491. doi:10.3390/jcm10235491
52. Monfrecola G, Megna M, Rovati C, et al. A critical reappraisal of off-label use of photodynamic therapy for the treatment of non-neoplastic skin conditions. Dermatology. 2021;237(2):262–276. doi:10.1159/000507926
53. Podgórska A, Kicman A, Wacewicz-Muczyńska M, Konończuk T, Niczyporuk M. Evaluating the effects of laser treatments on visible changes in the photoaging process of the skin using specialized measuring devices. J Clin Med. 2024;13:7439. doi:10.3390/jcm13237439
54. Boen M, Brownell J, Patel P, Tsoukas MM. The role of photodynamic therapy in acne: an evidence-based review. Am J Clin Dermatol. 2017;18(3):311–321. doi:10.1007/s40257-017-0255-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Plasma Treatment – Results of Skin Microbiome Analysis
Watanabe C
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1269-1279
Published Date: 26 May 2025