Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Current Perception Threshold Testing in Pharyngeal Paresthesia Patients with Depression or Anxiety
Authors Chang W, Xu W ![]() , Hu R, An Y
, Hu R, An Y
Received 3 February 2020
Accepted for publication 8 April 2020
Published 20 April 2020 Volume 2020:16 Pages 1023—1029
DOI https://doi.org/10.2147/NDT.S248236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Wei Chang, Wen Xu, Rong Hu, Yunsong An
Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, People’s Republic of China
Correspondence: Wen Xu Email [email protected]
Purpose: Satisfactory quantitative diagnostic approaches to pharyngeal paresthesia patients with depression or anxiety remain to be explored. This study investigated the plausibility of current perception threshold (CPT) testing in diagnosing pharyngeal paresthesia in patients with depression or anxiety.
Patients and Methods: A total of 41 patients with pharyngeal paresthesia with depression or anxiety were recruited as the study group. Additionally, 60 healthy volunteers constituted the control group. The CPT values associated with 5-, 250-, and 2000-Hz electrical stimulation frequencies were measured at the palatal lingual arch and posterior third of the lingual body (two sensory nerve distribution sites in the pharynx). The normal range of CPT values of the above three frequencies was analyzed. The differences in the CPT values for sensory nerves were compared.
Results: There were no significant differences in age and sex between the study and control groups. The CPT values of the pharynx at the two tested sites were not significantly correlated with age and gender. The CPT value of the study group was significantly lower than that of the control group in the palatal lingual arch and posterior third of the lingual body at an electrical stimulation of 5 Hz (p< 0.05). No significant differences in the CPT values at other frequencies were found between the two groups.
Conclusion: CPT testing is effective in determining pharyngeal paresthesia in patients with depression and anxiety. Paresthesia of the pharyngeal sensory nerve region is caused by damaged C fibers.
Keywords: pharyngeal paresthesia, sensory nerve fibers, current perception threshold testing, reference values, depression, anxiety
Corrigendum for this paper has been published
Introduction
Pharyngeal paresthesia is a syndrome that includes the sensation of a foreign body obstruction in the pharynx, phlegm attachment, itching, hypersensitivity and pain in the throat. The primary causes of pharyngeal paresthesia include local factors, psychiatric factors, and systematic factors. In addition to organic lesions, psychiatric factors are responsible for a significant proportion of pharyngeal sensory disorders. Patients experiencing pharyngeal paresthesia have a neuroallergic reaction and experience higher levels of psychological distress, such as anxiety and/or depression.1,2
Investigations into possible quantitative approaches to pharyngeal sensory nerve diagnosis are of critical importance. By estimating different sensations, such as tactile perception threshold measurement using von Frey hairs, the needle stimulation sensitivity test, and the vibration perception threshold measurement using the Rydel-Seiffer tuning fork,3 some perception thresholds can be measured. However, these tools can only provide a rough estimation range rather than specific values. Other quantitative approaches, such as the measurement of sensory nerve conduction velocity (NCV) and somatosensory evoked potential (SEP), ignore hypersensitivity and hypoesthesia and can test only 10% of crude myelinated nerve fibers.4 Furthermore, all the above-mentioned measurements are hand-controlled and single-blinded; during measurement, strong stimulation is required, which results in pain.5
Technological progress has provided potentially more accurate approaches to quantify and thus diagnose pharyngeal sensory nerve damage. The measurement of the current perception threshold (CPT) has attracted the attention of researchers in the field of sensory nerve measurement. CPT testing can quantitatively evaluate the function of sensory nerves and measure the minimum perceivable current when electrical stimulations of 2,000, 250, and 5 Hz are applied. The CPT values at each frequency indicate the threshold values of the Aβ fibers (sense of pressure), Aδ fibers (senses of temperature and pain), and C fibers (senses of pain and temperature).6 CPT testing can be performed on any skin/mucosa area of the body to determine the location and extent of sensory nerve dysfunction. It allows for the quantitative evaluation of damaged nerve fibers.7 CPT test results that are below the normal range are suspected to indicate hyperesthesia, while those above the normal range imply hypoesthesia.8 To date, CPT testing has been used for the evaluation of paresthesia in multiple medical fields.9–11 In addition, it has been used to explore the sensory nerve function of oral mucosa.12 However, no publications on the application of CPT in pharyngeal paresthesia have been released to the best of our knowledge.
Based on the aforementioned discussion, in this study, CPT testing of the distribution area of the pharyngeal sensory nerve was performed to identify the nerve fibers affecting pharyngeal sensation and to accurately locate the damage to different sensory nerve fibers in pharyngeal paresthesia.
Patients and Methods
Patients
Between December 2017 and December 2018, 41 patients with pharyngeal paresthesia were selected at Beijing Tongren Hospital. The diagnostic standard was mainly based on the patient’s complaints, including foreign body sensation, obstruction sensation, pain sensation, itching sensation and other discomfort in the pharynx. There were 17 males and 24 females (age range 22–74, mean 46.98±13.011 years). The inclusion criteria were as follows: recurrent history of pharyngeal paresthesia; no benign or malignant neoplasms, acute inflammation or anatomical abnormalities as detected by otorhinolaryngology; and the disease duration was at least two months. The exclusion criteria were as follows: 1) vertebral/cervical abnormalities, such as spondylosis, according to radiological examination; 2) nasopharyngitis, nasopharyngeal tumor, pharyngolaryngeal tumors, neck tumors and other organic diseases based on nasopharyngeal endoscopy, cervical B-ultrasound, laryngoscopy and/or cervical MRI; 3) those with emaciation, hoarseness or other warning signs; 4) those with serious cardiovascular, lung, kidney, liver or digestive tract diseases and connective tissue disease history; 5) a history of use of medication for the treatment of pharyngeal paresthesia, antipsychotics, or drugs for pharyngitis; and 6) those who refused to sign the informed consent form or cooperate with the investigators.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Beijing Tongren Hospital affiliated with Capital Medical University (approval no.TRECKY2018-061). Written informed consent was obtained from each participant.
Control Group
The control group consisted of 60 healthy individuals, recruited mainly from the general public. There were 37 males and 23 females (age range 23–72 years, median 38 years). The selection criteria were as follows: healthy; no complaints of pharyngeal sensory abnormalities, chronic pharyngitis, pharyngeal susceptibility or other pharyngeal sensory abnormalities; no organic lesions of the ear, nose, and throat; no reflux-related diseases; and no special organic and psychological diseases. No peripheral neuropathy was found.
Data Collection
Before CPT testing, all subjects were asked about their medical history and underwent a physical examination. The information collected included details regarding gender, age, and occupation. Symptom assessment included a foreign body sensation in the throat, sore throat, dry throat, itchy throat, and heartburn due to acid regurgitation. The physical signs of the 41 patients with pharyngeal paresthesia included follicular hyperplasia (36/41, 87.8%), pharyngeal congestion (13/41, 31.7%), mucosal hypertrophy (23/41, 56.1%), and increased secretion (11/41, 26.9%).
All patients were assessed with the Hamilton Anxiety Scale (HAM-A) and Hamilton Depression Scale (HAM-D). The HAM-A is one of the earliest developed scales to measure the severity of anxiety symptoms,13 and it is still widely used in clinical and scientific research. The scale is composed of 14 items, and each item is scored using a 5-level scoring method consisting of 0–4 points as follows: (0) no; (1) mild; (2) moderate; (3) severe; and (4) extreme. The total score reflects the severity of anxiety symptoms. The higher the score, the more serious the anxiety symptoms are. The maximum score is 56, and the classification of anxiety level is as follows: no anxiety≤ 7; mild anxiety = 8–14; moderate anxiety = 15–23; and severe anxiety≥ 24. HAM-D is the most widely used depression assessment scale in clinical practice.14 The scale consists of 17 items, most of which are graded with a 5-level scoring method of 0–4 points as follows: (0) none; (1) mild; (2) moderate; (3) severe; and (4) extremely severe. A small number of items are graded with a 3-level scoring method with 0–2 points as follows: (0) none; (1) mild–moderate; and (2) severe. The total score reflects the severity of depressive symptoms. The higher the score, the more serious the depressive symptoms are. The maximum score is 52. The assessment of depression is classified as follows: no depression≤7; mild depression = 8–17; moderate depression = 18–24; and severe depression ≥25.
CPT Testing
Equipment and consumables. We used the Neurometer CPT/C Sensory Nerve Quantitative Detector (Neurotron, Inc., Baltimore, MD, USA). The electrode mainline was the electrode extension line (CBEX-4X), and we used self-adhesive stimulating electrodes (SDE-4).
Test location and mode selection. Test site selection was as follows: (A) palatal lingual arch and (B) posterior third of the lingual body (Figure 1). The CPT testing mode was set to automatic clinical CPT testing (p<0.005, resolution ±20t, tA) in automatic double-blind test mode.
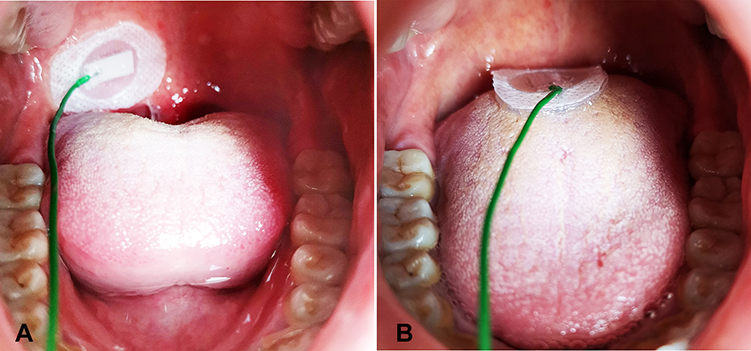 |
Figure 1 Measurement of the current perception threshold (CPT). (A) Point for measuring the CPT on the palatal lingual arch. (B) Point for measuring the CPT on the posterior third of the lingual body. |
The testing was performed as follows. Subjects were seated comfortably and tested in a quiet, light-friendly environment with a temperature of approximately 24±3 degrees Celsius. At the palatoglossal arch, oral secretions were removed as much as possible. The mucosal self-adherent electrode was placed at any palatoglossal arch. Three test frequencies (2000 Hz, 250 Hz, and 5 Hz) were tested, and the test results were recorded. After measurement, the electrodes were placed in the posterior third of the lingual body. The CPT values of three frequencies were measured using the same method. Each patient was tested for no more than 15 minutes.
Statistical Analysis
The categorical variables were recorded as frequencies and percentages. The distribution was evaluated with the one-sample Kolmogorov–Smirnov normality test. Normally distributed variables are presented as the mean (standard deviation) and non-normally distributed variables as the median (interquartile range). Differences between the groups were analyzed with independent samples t-tests for two groups. For non-normally distributed data, the Mann–Whitney U-test was used for comparisons between the two groups. In the correlation analysis, clinical factors influencing the CPT testing results were identified through logistic regression analysis. For multiple comparisons, one-factor analysis of variance (ANOVA) or non-parametric Kruskal–Wallis ANOVA followed by a Bonferroni test was performed. A p-value of 0.05 or less was considered statistically significant. Analyses were conducted using SPSS 20.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic Data
There were no significant differences in age or sex between the study and control groups (p>0.05; Table 1).
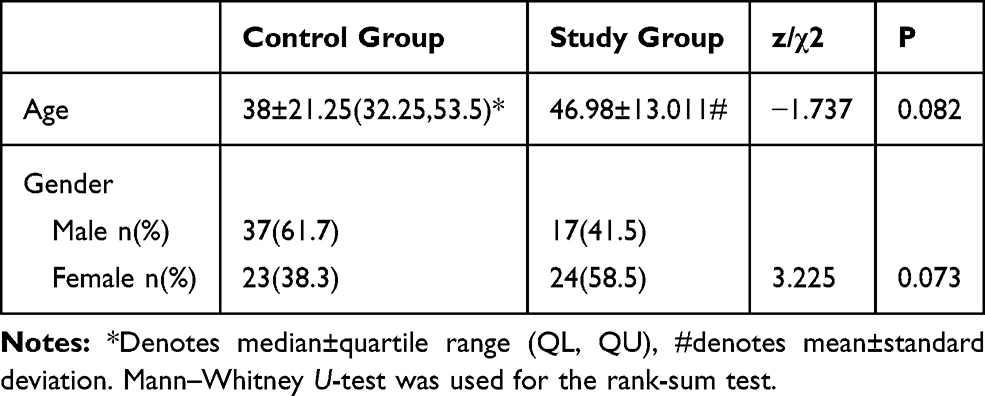 |
Table 1 Age and Gender Distribution of the Two Groups: Study Group and Control Group |
Factor Analysis
The results of the multiple linear regression analysis are summarized in Table 2. There was no correlation between CPT value and gender. No correlation between CPT value and age was observed either.
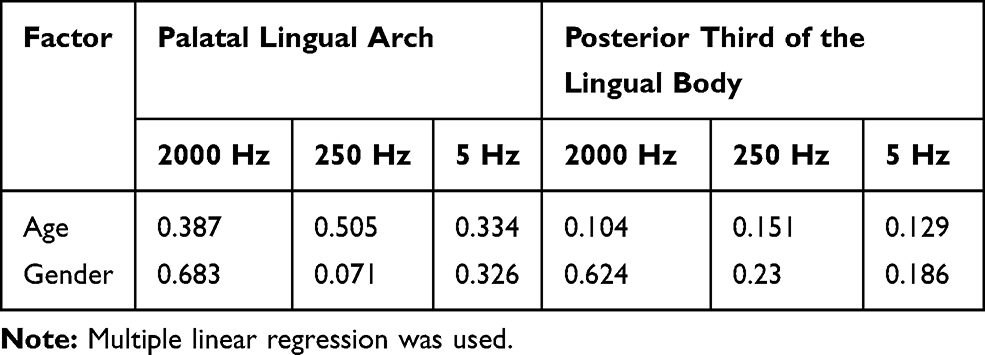 |
Table 2 Multiple Linear Regression Analysis of Influencing Factors |
Reference Values for CPT Testing
Based on the influencing factor analysis, the reference values for CPT testing at three frequencies at different sites were established (Table 3).
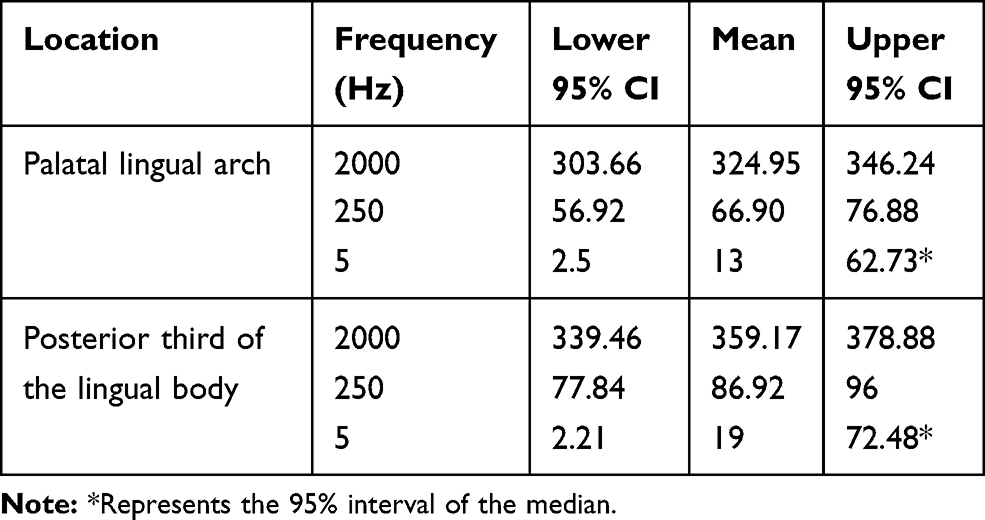 |
Table 3 Reference Values for CPT Testing in the Pharynx (n=60) |
Comparison of Testing Sites
In the 60 control group cases and 41 study group cases, the CPT values of the three different frequencies for current stimulation and two different stimulation sites were compared. A significant difference was identified between the two groups at the palatoglossal arch and posterior third of the lingual body at 5 Hz (p<0.05). The CPT value of the study group was significantly lower than that of the control group. There were no significant differences in the other frequencies and locations between the two groups (Table 4).
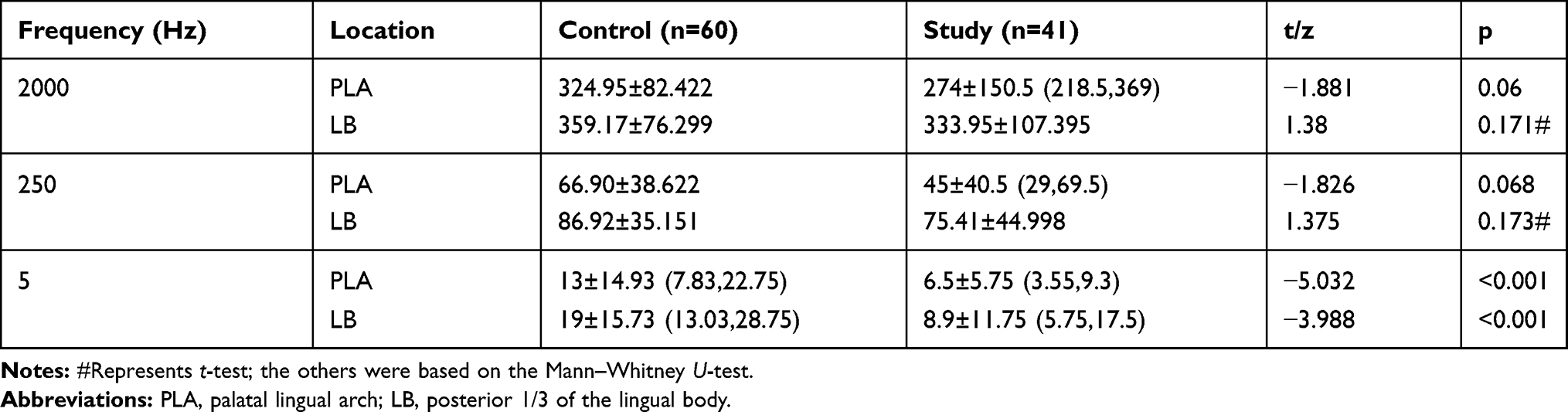 |
Table 4 Comparisons of the CPT Values Between the Control and Study Groups |
Comparisons of the CPT Values Between Different Groups of Patients with Anxiety or Depression
The 41 pharyngeal paresthesia patients with anxiety or depression were subgrouped according to the severity of anxiety or depression. There were 16, 17, and 8 mild, moderate and severe cases, respectively. There were significant differences in the CPT values between the control group and the study subgroups at the palatoglossal arch and posterior third of the lingual body at 5 Hz (corrected p<0.05; Table 5). Although no significant difference in the CPT values was observed between the mild subgroup and the moderate subgroup at the palatoglossal arch and among the three study subgroups at the posterior third of the lingual body, a noticeably decreasing trend in the CPT values at 5 Hz from the severe subgroup to the mild subgroup was observed at both sites.
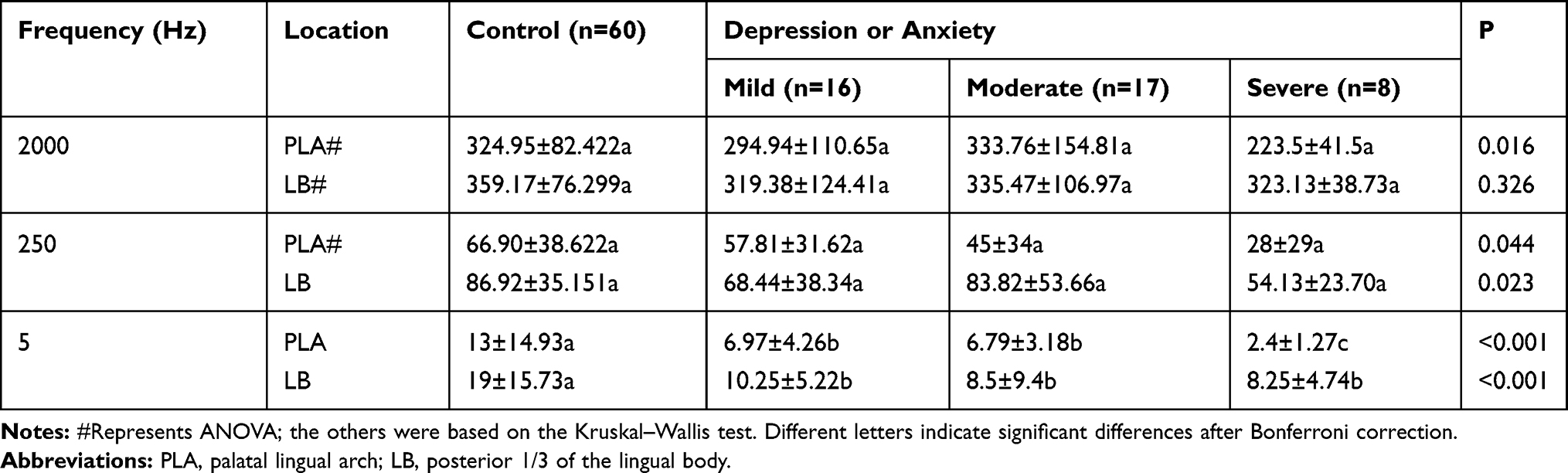 |
Table 5 Comparisons of the CPT Values Between Different Groups of Patients with Anxiety or Depression |
Discussion
The pathogenesis of pharyngeal paresthesia is very complicated. It exists in a wide range of psychiatric disorders, with depression and somatization disorders having a prominent position as associated factors.15 In this study, HAM-A and HAM-D were used to preliminarily explore the correlation between pharyngeal paresthesia and psychological symptoms. Then, CPT was adopted to quantitatively detect the function of the pharyngeal sensory nerve and to locate the most relevant sensory nerve fibers.
The sensory nerves of the pharynx are mainly glossopharyngeal nerves and vagus nerves. The sensory fibers of glossopharyngeal nerves are distributed throughout the mucous membrane of the root of the tongue, tonsil and pharynx. The soft palatal mucosa and tonsil are innervated by the lesser palatal nerves and glossopharyngeal nerves.16 The palatal lingual arch and posterior third of the lingual body are important regions of the distribution of the glossopharyngeal nerve sensory branches in the oropharyngeal region. Therefore, we selected these two sites to test the corresponding CPT values of the sensory nerve, which has a strong sensitivity and specificity to pharyngeal paresthesia.
In terms of gender effects, Seong et al reported gender differences in normal CPT values that only appeared in the 2000-Hz stimulus assessment, and males had a higher perception threshold.17 Females had higher myelinated nerve fiber densities than males,18 which partly explains the effects of gender on the CPT values under a stimulus of 2000 Hz. However, this study found that the CPT values of the pharyngeal sensory nerve are not related to gender at any frequency. This contradiction may be due to the different sizes of samples between our study and those in the literature.
In consideration of age effects, previous literature has indicated that the CPT value is closely related to age at 2000 Hz, and the sensitivity of vibration and pressure sensation decreases with age.19 In this study, there was no correlation between age factors and CPT values at two test sites. Presumably, this inconsistency may be caused by the different objectives of our study and the literature. Age affects the sensory pathways in every part of the body; thus, the density of nerve fibers and mechanoreceptors in skin and muscle decreases over time.18 More specifically, the decrease in nerve conduction velocity and the increase in sensory conduction amplitude are strongly correlated with the increase in age. These correlations are caused by a decrease in the number of nerve fibers, the shortening of the diameter of nerve fibers and the change in nerve fiber membranes.20 To make a more accurate correlation between the CPT reference values of the pharyngeal sensory nerve, age and gender in the normal population, further exploration is needed.
In this study, the CPT values of the palatal lingual arch and posterior third of the lingual body at three different frequencies were compared between 60 normal people and 41 people suffering from pharyngeal paresthesia with depression or anxiety. We found significant differences in the CPT values at 5 Hz at two locations. The CPT values of the two loci in the study group were significantly lower than those in the control group. The principle of CPT detection is that three different frequencies of current stimulation and selectively stimulate different subsets of sensory nerve fibers. According to the literature, the 5-Hz test corresponds to the unmyelinated C fibers,21 which mainly transmit slow pain, temperature sensation, and multimodal sensory damage.22 In this study, patients with pharyngeal paresthesia and anxiety or depression often complained of chronic pharyngeal pain and burning sensations. The subjective feelings of the patients as well as the main findings at 5 Hz in this study suggest that these patients had a significant state of sensory hypersensitivity compared with the normal population and that this sensory hypersensitivity can be physiologically quantified as abnormal CPT values for the C nerve fibers. In addition, the 41 pharyngeal paresthesia patients with anxiety or depression were divided according to the severity of anxiety or depression for the subgroup analysis. Significant differences in the CPT values were observed between the control group and the subgroups at the sites of the palatoglossal arch and posterior 1/3 of the lingual body at 5 Hz, which indicates that the CPT value at these sites at 5 Hz is of diagnostic significance in distinguishing the normal population from pharyngeal paresthesia patients with anxiety or depression and that the measurement of CPT values in the sensory nerve fibers at 5 Hz can be an important quantitative detection method for pharyngeal paresthesia patients with anxiety or depression. However, our study did not show a significant difference between the mild subgroup and the moderate subgroup at the palatoglossal arch and among the subgroups at the posterior 1/3 of the lingual body. Presumably, these results were due to a rather small sample size involved in this study. There were only 16 cases of mild, 17 cases of moderate and 8 cases of severe disorders, and the data for subgroup analysis at 5 Hz were not normally distributed. Nevertheless, a noticeably decreasing trend in the CPT values at 5 Hz from the severe subgroup to the mild subgroup was observed at both sites. To verify the diagnostic value of CPT testing in distinguishing different severity levels of anxiety or depression in pharyngeal paresthesia patients, studies with a large sample size remain to be conducted in the future.
This study had the following limitations. First, it was conducted at a single center with a small sample size. To validate the outcomes obtained in this study and to further identify the diagnostic value of CPT for pharyngeal paresthesia in patients with anxiety or depression, future multi-center research with a larger sample size remains to be carried out. In addition, the results of this study may also suffer from subjectivity during the operation process. To obtain accurate outcomes, the close cooperation of highly experienced clinicians and subjects is required.
Conclusion
CPT has been used in the diagnosis and research of many types of sensory disorders, such as myelopathy, radiculopathy, peripheral nerve injury, and focal nerve injury.23 It can also be used to judge the severity of clinical conditions, monitor the progress of neuropathy, and monitor the recovery of neurological function after surgery or trauma.24,25 In this study, CPT was applied in the diagnosis of pharyngeal paresthesia, which has not been reported before to the best of our knowledge.
The current study led to the following conclusion. The CPT value of the pharyngeal nerve corresponding to 5 Hz in pharyngeal paresthesia in patients with anxiety or depression can be quantitatively detected, and this condition may be caused by damage to C fibers. The findings of this study can be used to quantify pharyngeal paresthesia in clinical settings.
Acknowledgments
This study was supported by a grant from the Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (grant no. XMLX201806).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wilson JA, Deary IJ, Maran AG. The persistence of symptoms in patients with globuspharyngis. Clin Otolaryngol Allied Sci. 1991;16:202–205. doi:10.1111/j.1365-2273.1991.tb01977.x
2. Deary IJ, Wilson JA, Harris MB, et al. Globus pharyngis: development of a symptom assessment scale. J Psychosom Res. 1995;39(2):203–213. doi:10.1016/0022-3999(94)00104-D
3. Maier C, Baron R, Tolle TR, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain. 2010;150:439–450. doi:10.1016/j.pain.2010.05.002
4. Chong MS, Hester J. Diabetic painful neuropathy: current and future treatment options. Drugs. 2007;67:569–585. doi:10.2165/00003495-200767040-00006
5. Dyck PJ, Dyck PJ, Larson TS, et al. Patterns of quantitative sensation testing of hypoesthesia and hyperalgesia are predictive of diabetic polyneuropathy: a study of three cohorts. Nerve growth factor study group. Diabetes Care. 2000;23(4):510–517. doi:10.2337/diacare.23.4.510
6. Katims JJ, Long DM, Ng LK. Transcutaneous nerve stimulation. Frequency and waveform specificity in humans. Appl Neurophysiol. 1986;49:86–91.
7. American Association of Electrodiagnostic M. Guidelines in electrodiagnostic medicine. Technology review: the neurometer Current Perception Threshold (CPT). Muscle Nerve Suppl. 1999;8:S247–S259.
8. Katims JJ, Rouvelas P, Sadler BT, et al. Current perception threshold. Reproducibility and comparison with nerve conduction in evaluation of carpal tunnel syndrome. ASAIO Trans. 1989;35(3):280–284. doi:10.1097/00002216-198907000-00034
9. Ziccardi VB, Dragoo J, Eliav E, Benoliel R. Comparison of current perception threshold electrical testing to clinical sensory testing for lingual nerve injuries. J Oral Maxillofac Surg. 2012;70(2):289–294. doi:10.1016/j.joms.2011.08.019
10. Lv SL, Fang C, Hu J, et al. Assessment of peripheral neuropathy using measurement of the current perception threshold with the Neurometer(R) in patients with type 1 diabetes mellitus. Diabetes Res Clin Pract. 2015;109:130–134. doi:10.1016/j.diabres.2015.04.018
11. Knupfer SC, Liechti MD, Gregorini F, et al. Sensory function assessment of the human male lower urinary tract using current perception thresholds. NeurourolUrodyn. 2017;36:469–473.
12. Kimoto S, Ito N, Nakashima Y, et al. Maxillary sensory nerve responses induced by different types of dentures. J Prosthodont Res. 2013;57:42–45. doi:10.1016/j.jpor.2012.09.001
13. Matza LS, Morlock R, Sexton C, et al. Identifying HAM-A cutoffs for mild, moderate, and severe generalized anxiety disorder. Int J Methods Psychiatr Res. 2010;19:223–232. doi:10.1002/mpr.323
14. Boessen R, Groenwold RH, Knol MJ, et al. Comparing HAMD(17) and HAMD subscales on their ability to differentiate active treatment from placebo in randomized controlled trials. J Affect Disord. 2013;145:363–369. doi:10.1016/j.jad.2012.08.026
15. Gale CR, Wilson JA, Deary IJ. Globus sensation and psychopathology in men: the vietnam experience study. Psychosom Med. 2009;71:1026–1031. doi:10.1097/PSY.0b013e3181bc7739
16. Yoshida Y, Tanaka Y, Hirano M, Nakashima T. Sensory innervation of the pharynx and larynx. Am J Med. 2000;108(Suppl 4a):51S–61S. doi:10.1016/S0002-9343(99)00342-3
17. Kim SW, Shin JB, You S. Current perception threshold in different age, sex and body parts. J Korean EMG Electrodiagn Med. 2009;11:92–97.
18. Horowitz SH, Krarup C. Conduction studies of the normal sural nerve. Muscle Nerve. 1992;15:374–383. doi:10.1002/mus.880150318
19. Vega JA, Garcia-Suarez O, Montano JA, et al. The Meissner and Pacinian sensory corpuscles revisited new data from the last decade. Microsc Res Tech. 2009;72(4):299–309. doi:10.1002/jemt.20651
20. Tackmann W, Kaeser HE, Magun HG. Comparison of orthodromic and antidromic sensory nerve conduction velocity measurements in the carpal tunnel syndrome. J Neurol. 1981;224(4):257–266. doi:10.1007/BF00313289
21. Felix EP, Giuliano LM, Tierra-Criollo CJ, et al. Sensations and reaction times evoked by electrical sinusoidal stimulation. Clin Neurophysiol. 2009;39:283–290. doi:10.1016/j.neucli.2009.10.001
22. McGlone F, Reilly D. The cutaneous sensory system. Neurosci Biobehav R. 2010;34:148–159. doi:10.1016/j.neubiorev.2009.08.004
23. Nishimura A, Ogura T, Hase H, et al. Objective evaluation of sensory function in patients with carpal tunnel syndrome using the current perception threshold. J Orthop Sci. 2003;8(5):625–628. doi:10.1007/s00776-003-0684-0
24. Nawfar SA, Yacob NB. Effects of monochromatic infrared energy therapy on diabetic feet with peripheral sensory neuropathy: a randomised controlled trial. Singap Med J. 2011;52:669–672.
25. Imoto K, Takebayashi T, Kanaya K, Kawaguchi S, Katahira G, Yamashita T. Quantitative analysis of sensory functions after lumbar discectomy using current perception threshold testing. Eur Spine J. 2007;16:971–975. doi:10.1007/s00586-006-0285-7
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.