Back to Journals » Clinical Ophthalmology » Volume 14
Current Knowledge and Attitudes Concerning Cost-Effectiveness in Glaucoma Pharmacotherapy: A Glaucoma Specialists Focus Group Study
Authors Feldman RM ![]() , Cioffi GA, Liebmann JM, Weinreb RN
, Cioffi GA, Liebmann JM, Weinreb RN
Received 25 October 2019
Accepted for publication 9 January 2020
Published 6 March 2020 Volume 2020:14 Pages 729—739
DOI https://doi.org/10.2147/OPTH.S236030
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Robert M Feldman,1 George A Cioffi,2 Jeffrey M Liebmann,3 Robert N Weinreb4
1The University of Texas Medical School Houston, TX, USA; 2Department of Ophthalmology, NewYork Presbyterian Hospital Columbia University Irving Medical Center, NY, New York, USA; 3Columbia University Medical Center, New York, NY, USA; 4University of California San Diego, LaJolla, CA, USA
Correspondence: Robert M Feldman
Department of Ophthalmology and Visual Science, The University of Texas Medical School at Houston, 6400 Fannin St., Ste 1800, Houston, TX 77030, USA
Tel +1 713 559 5200
Fax +1 713 795 0733
Email [email protected]
Background: Rising healthcare costs motivate continued cost-reduction efforts. To help lower costs associated with open-angle glaucoma (OAG), a prevalent, progressive disease with substantial direct and indirect costs, clinicians need to understand the cost-effectiveness of intraocular pressure (IOP)-lowering pharmacotherapies. There is little published information on clinicians’ knowledge and attitudes about cost-effectiveness in glaucoma treatment.
Purpose: This pilot focus group study aimed to explore clinician attitudes and perspectives around the costs and cost drivers of glaucoma therapy; the implementation of cost-effectiveness decisions; the clinical utility of cost-effectiveness studies; and the cost-effectiveness of available treatments.
Methods: Six US glaucoma specialists participated in two separate teleconferencing sessions (three participants each), managed by an independent, skilled moderator (also a glaucoma specialist) using a discussion guide. Participants reviewed recent publications (n=25) on health economics outcomes research in glaucoma prior to the sessions.
Results: Participants demonstrated a clear understanding of the economic burden of glaucoma therapy and identified medications, diagnostics, office visits, and treatment changes as key cost drivers. They considered cost-effectiveness an appropriate component of treatment decision-making but identified the need for additional data to inform these decisions. Participants indicated that there were only a few recent studies on health economics outcomes in glaucoma which evaluate parameters important to patient care, such as quality of life and medication adherence, and that longitudinal data were scant. In addition to efficacy, participants felt patient adherence and side-effect profile should be included in economic evaluations of glaucoma pharmacotherapy. Recently approved medications were evaluated in this context.
Conclusion: Clinicians deem treatment decisions based on cost-effectiveness data as clinically appropriate. Newer IOP-lowering therapies with potentially greater efficacy and favorable side-effect and adherence profiles may help optimize cost-effectiveness. Future studies should include: clinicians’ perspectives; lack of commercial bias; analysis of long-term outcomes/costs; more comprehensive parameters; real-world (including quality-of-life) data; and a robust Markov model.
Keywords: open-angle glaucoma, ocular hypertension, cost-effectiveness, clinician knowledge and attitudes, focus group, prostaglandin analogs
Introduction
Glaucoma, the leading cause of irreversible blindness globally, is increasing in prevalence due to rapid increase in the aging population.1,2 An estimated 64.3 million people (aged 40 to 80 years) globally were affected by glaucoma in 2013, and that number is expected to reach 76 million by 2020.2 Open-angle glaucoma (OAG) accounts for more than 70% of all glaucoma cases.3 The number of Americans living with OAG—which is a chronic, progressive disease—was estimated to be 2.7 million in 2011 and projected to reach 7.3 million in 2050, growing at a rate of 28% per decade.4
Glaucoma decreases health-related quality of life; the extent of the reduction is directly associated with the severity or stage of the disease.5–7 Patients with glaucoma are faced with the difficult challenges of visual dysfunction in everyday life, such as reduced mobility and difficulty with reading. Among those with glaucoma, self-reported visual disability is associated with difficulty walking, falls, and depression. As the disease progresses, the psychological burden of vision loss increases.8 Besides the affected individual, blindness and visual impairment from glaucoma also impact the families, the healthcare system, and society in general, creating a substantial socioeconomic burden.7
The annual medical cost of glaucoma and disorders of the optic nerve in the US was estimated at $6.1 billion in 2014 and projected to be as high as $12 billion by 2032 and $17.3 billion by 2050.9 The true direct cost would be considerably higher if all patients with this heavily underdiagnosed disease were treated.7,10 A retrospective cohort analysis of Medicare claims found that glaucoma patients with any degree of vision loss had 46.7% higher total costs compared with those without vision loss, with mean total annual medical costs increasing from $8157 for no vision loss to $18,670 for blindness.11 A Markov model replicating health events over the remaining lifetime of a patient with newly diagnosed glaucoma on US Medicare claims data from 1999 to 2005 estimated that the average lifetime cost of care for people with primary OAG (POAG) was about $137 per patient per year, or $1688 greater than those without glaucoma.12 Using a large, nationally representative sample of Medicare beneficiaries, a recent study found that patients with glaucoma incurred an additional $2903 annual total health care costs and $2599 higher non-outpatient costs (total health care costs with the exclusion of outpatient payments) compared with those without.8
The cost of glaucoma care in the US, then, is high and expected to become higher as the prevalence of the disease increases. In order to lower those costs, stakeholders—including clinicians—need to better understand the cost-effectiveness of IOP-lowering therapies. Cost-effectiveness data provide information about the costs of different interventions or treatment strategies relative to their performance, which can be helpful in identifying potential ways to reduce the economic burden of treatment. Over the past decade, research has begun to address cost-effectiveness in the treatment of OAG and ocular hypertension (OHT).13–16
While awareness of costs is of increasing importance, little is known about whether and how clinicians treating glaucoma patients use cost-effectiveness in clinical decision-making. We convened a small focus group of glaucoma specialists to learn more about their knowledge and attitudes regarding cost-effectiveness in the treatment of patients with OAG or OHT. The focus group method’s main advantage is its qualitative nature, which is complementary to that of quantitative research and allows in-depth exploration of thoughts, attitudes, and opinions via open-ended questions. It is commonly used to gain original insights and perspectives, uncover opinion trends, deepen understanding, and develop new hypotheses or ideas for further research. The aim of this pilot focus group study was to: 1) explore clinician perspectives regarding the costs and cost drivers of glaucoma therapy; 2) explore clinician attitudes and experience regarding the implementation of cost-effective decisions when treating patients with OAG or ocular hypertension (OHT) and the clinical utility of cost-effectiveness studies; and 3) explore clinician views about the cost-effectiveness of available treatment strategies and modalities for OAG and OHT and identify potential opportunities to improve glaucoma pharmacotherapy and reduce costs.
Methods
A focus group was formed to include six academic glaucoma specialists recognized as leading experts in the field of glaucoma treatment. Two separate teleconference sessions, each with three participants and led by the same moderator (also a glaucoma specialist) were conducted.
A discussion guide was created and distributed beforehand to the participants in order to facilitate and focus the discussion sessions. The discussion guide comprised a mixture of standardized/ranked and open-ended questions, which were grouped under the following general topics: the cost of care, cost considerations, current medical glaucoma therapies, and health economics and outcomes research (HEOR) (Figure 1). To help address the specific questions about HEOR in glaucoma, participants were asked to review the summaries of 25 recent publications on health economics of glaucoma therapies prior to the teleconferences (Table 1).
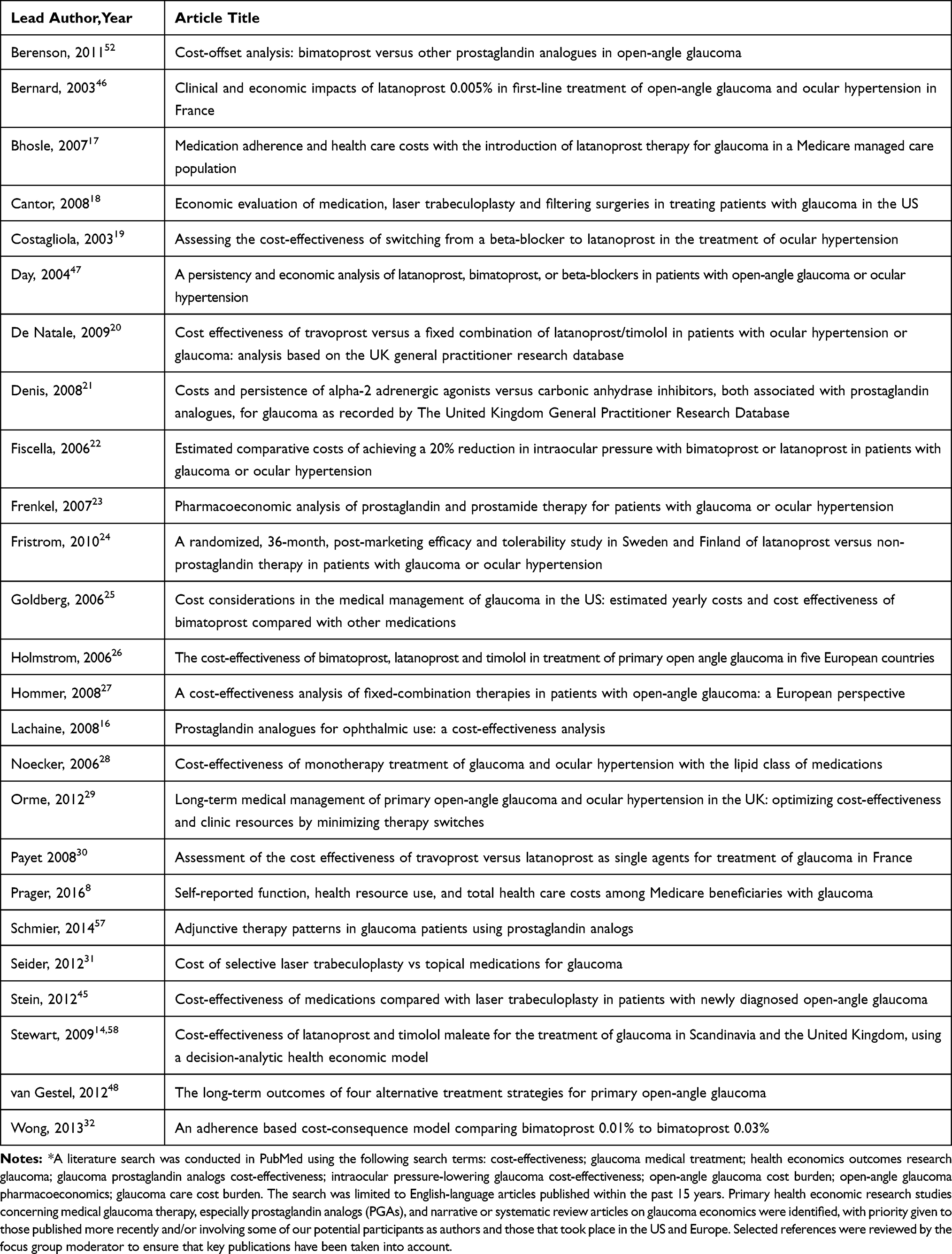 |
Table 1 Key HEOR Articles Identified Through Literature Search* |
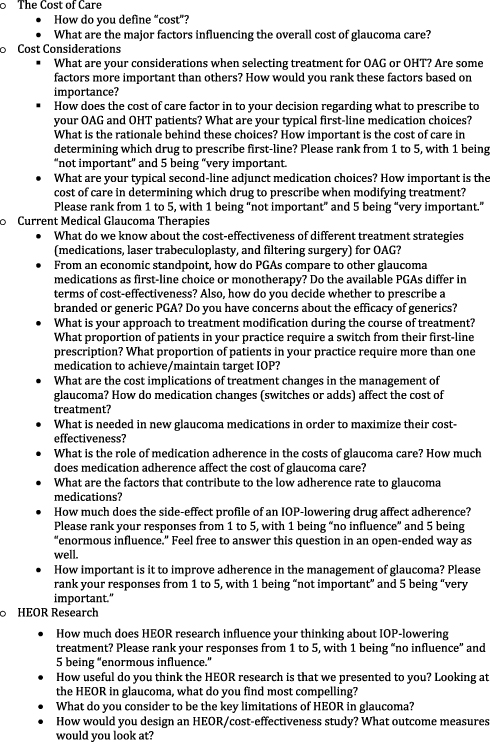 |
Figure 1 Topics discussed in focus groups of glaucoma specialists. |
Sessions spanned 2 h to allow the moderator ample time to solicit responses from participants to standardized/ranked questions, and to allow for additional discussion around open-ended questions. Following the conclusion of the discussion sessions, responses of the participants to open-ended questions were summarized descriptively based on the teleconference transcripts. Where possible, ranked responses were tallied.
Because the discussions were based on existing published literature and general clinical experiences and no research was performed on human or animal subjects, human cell lines, or human tissues, this study did not require ethics committee approval.
Results
Costs and Cost Drivers in Glaucoma Therapy
Participants noted that medical costs, including the financial burden of glaucoma therapy, are rising. They asserted the need to reduce that cost so that it is possible for clinicians to continue to provide their patients the best care. When asked to define “cost,” they noted that the economic implications of glaucoma extend well beyond the direct, short-term costs to the patient or health system. Some specifically stated that, apart from expenses for medical services including medications, office visits, diagnostic testing, and surgery, glaucoma also produces significant patient-based and societal costs in forms of productivity/income loss or expenses for assistance with daily living, ie, the long-term cost of vision loss.
Participants acknowledged that there are multiple cost drivers in glaucoma care. The drivers identified as having significant cost impact included medications, diagnostics, office visits, and treatment change (either switching medications or adding another agent, or advancement to laser or incisional surgery). Changes in treatment, the group noted, increase cost by adding office visits and patient time. Estimates of the contribution of medication cost to the overall cost of glaucoma care varied from 20% to 40% among the participants—and was perceived as a greater proportion of the cost relative to laser treatment and surgeries, especially among well-controlled patients.
Meanwhile, more than one participant noted that treatment costs are directly related to disease stage and the number of different treatments required. For OAG patients who are diagnosed and treated early, the greatest part of expenditure will most likely be on medication, these participants stated. However, they noted, for those patients who have more advanced disease when diagnosed, whose pressure is poorly controlled, and who require more interventions (multiple medications, even multiple surgeries), the overall cost will almost certainly be higher and likely be led by costs of surgical care and productivity losses.
Cost Considerations in Glaucoma Therapy
Participants acknowledged that patients’ access to prescription medications is a major concern and influenced primarily by price and health insurance status. They stated that out-of-pocket cost to patients is an important consideration in their practice; indeed, a significant reason why a generic prostaglandin analog (PGA) is the first-choice monotherapy for the majority of their glaucoma patients is insurance coverage. They further noted that efficacy, ocular and/or systemic side effects, dosing convenience, and patient adherence are the main factors that influence treatment choices, first or second line. Patient preferences also play a role, with many patients holding strong preferences among available treatment options. Patient perceptions or attitudes about generic substitutions, for example, can vary widely. The participants stated that many of their patients simply opt for the least costly alternative, while others place the highest value on clinical outcomes and are therefore willing to pay or tolerate more adverse effects for therapies with greater efficacy.
Participants added that, in reality, clinicians are often unaware of medications’ actual costs to patients. One noted that he prescribes mainly based on efficacy at least in part because it has become very difficult in the past few years to decipher the costs of medications charged at individual pharmacies.
Although the clinicians in this focus group generally do not view themselves as gatekeepers for the healthcare system, they were in agreement that cost is an important consideration in the management of glaucoma from the broader perspective of society. One of the participants specifically noted that, beyond a responsibility to patients, clinicians also have a responsibility to society. He pointed out that clinicians should keep in mind their obligation of being a good steward of societal dollars and healthcare resources when making treatment decisions.
Cost-Effectiveness of Current Medical Therapies
All participants agreed that PGAs, the most widely used first-line glaucoma medications, stand out as a cost-effective treatment among all available IOP-lowering medications. The drug class was described as efficacious (reaching a target IOP reduction of 30% most of the time), long-lasting in efficacy (which translates into less frequent visits and thus cost savings), safe (least number of systemic adverse events), time-tested (on the market more than 20 years), dosed conveniently at once daily, and reasonably priced in an era of generics. However, some participants cautioned that generics are not all created equal—their experiences indicate that the variability in efficacy and tolerability is significant between different generic brands.
Participants stated that first-line treatment with a PGA is efficacious in lowering IOP in the majority of patients with glaucoma and that only a small minority require an alternative therapy. However, they also noted that, from a longitudinal perspective, combination therapy is often necessary to achieve or maintain target IOP, and that medication switching due to reasons such as tachyphylaxis, side effects, and visual field progression is common despite treatment. One participant estimated that at least 80% of patients with moderate to advanced disease and possibly 20% of patients with early disease require adjunctive therapy. The general consensus among the clinicians was that newer agents with greater efficacy than current regimens are needed in order to better control the cost of glaucoma therapy. If most patients will require adjunctive therapy at some point—and if, as noted above, treatment changes increase the cost by adding office visits and patient time—then having better first- or second-line treatments should provide long-term cost savings.
The approach to adjunctive therapy varied among participants. The majority reported that they typically choose to add a second drug when PGA monotherapy is insufficient. Their add-on choices usually include a topical carbonic anhydrase inhibitor (CAI) or a beta-blocker. Some noted that they tend to switch medication when there is an inadequate initial response and may consider laser surgery earlier in some cases to avoid polypharmacy. While specific adjunctive intervention varies, the general consensus was that an optimal second-line therapy is still lacking. Two participants suggested that an alternative to adding a second drug is switching the initial PGA (typically generic latanoprost) to the NO-donating PGA latanoprostene bunod (LBN) 0.024%—the latter is as well tolerated and safe as latanoprost but has the potential to provide additional pressure-lowering.33 Latanoprostene bunod was approved by the FDA in late 2017 and represents the first new PGA in more than 5 years, as well as the first NO-donating PGA.34 One participant mentioned that he is considering the Rho kinase (ROCK) inhibitor netarsudil 0.02% as a second-line choice, another recently approved therapy, although it must be used in combination with another IOP-lowering medication, such as a PGA, in order to provide additional reductions in IOP over the standard of care; in addition, concerns about relatively high hyperemia rates exist with netarsudil.35
When asked what is needed in a new medication to make it cost-effective, participants responded that new drugs need to be significantly better than the current options in one or several ways: efficacy, tolerability, safety, duration of action, or any combination thereof. In addition, participants asserted that adherence is an important consideration in determining whether a glaucoma medication is cost-effective. As one of them pointed out, no therapy can be cost-effective if the patient is non-adherent. Thus, a new medication may initially cost more, but if patients take it as prescribed, the increase in adherence may justify the cost over the long run. Participants emphasized that glaucoma is a chronic disease associated with low medication adherence in general and noted that improvement in adherence is critical for better management of the disease. Indeed, when asked to rank the importance of adherence improvement in the management of glaucoma on a rank scale of 1 to 5 (with 1 being “not important” and 5 being “very important”), the responses were 4 or 5. One participant remarked that adherence is one of the greatest unmet needs in glaucoma pharmacotherapy. Furthermore, participants viewed adherence as a multifactorial issue and identified the following factors as the main barriers to adherence in glaucoma therapy: side effects, number of drops, costs, and patient understanding of the disease.
The Utility of Cost-Effective Research
Participants were unanimous in their view that, overall, current cost-effectiveness research offers little clinical utility for the treatment of glaucoma or OHT. The group noted that published cost-effectiveness studies in the field of glaucoma have largely been geared towards insurers, payers, and pharmacy benefit managers, rather than doctors. They felt that few of the studies looked at parameters that are important to patient care and clinical practice, such as quality of life and medication adherence; and that longitudinal data are scant, with a dearth of evidence to determine what the most cost-effective treatment algorithm is over a patient’s lifetime.
Responses to the ranking question “How much does HEOR research influence your thinking about IOP-lowering treatment?” were 1 to 2 (on a rank scale of 1 to 5, with 1 being “no influence” and 5 being “enormous influence.") indicating that the influence of current cost-effectiveness data on clinical decision-making is indeed minimal. Participants stated that the available data may be used to guide insurers and payers but would need to be more persuasive and better designed in order to guide clinicians. Several participants commented that they find being good stewards of resources for the health care system as a whole an important goal but difficult to achieve given the current knowledge base about cost-effectiveness and payer-based variability in drug pricing.
According to participants, desirable elements of future economic studies in glaucoma pharmacotherapy include: a clinician’s perspective; an independent approach (ie, without commercial bias); analysis of long-term treatment outcomes and costs; a more comprehensive set of parameters, including stage of disease, treatment switch or addition, adherence, side effects associated with various therapies; real-world data related to clinical practice, including quality-of-life data; and a robust Markov model that allows assessment of all the costs.
Participants asserted that cost-effectiveness should be considered in the context of the patient’s age and expected lifespan, and, if possible, it would be important to determine the incremental cost of every additional mm Hg of IOP reduction.
Discussion
The cost-effectiveness of care is becoming an increasingly important aspect of glaucoma therapy because of the growing patient population and associated cost increases. Some prior research has investigated the economic outcomes of various glaucoma treatments, but few if any past studies have sought to identify clinicians’ views regarding cost-effectiveness and their attitudes and experience using cost-effective data in the treatment of glaucoma.
Participants in the present study displayed a consistent understanding of the economic impact of glaucoma and the need to reduce treatment costs. Their perception that medication use contributes substantially to costs is consistent with previous reports that prescription medication costs drive financial burden at all stages of glaucoma and are equal to or greater than all other charges.36–40 There is also evidence in support of participants’ impression that diagnostics are a significant cost driver. In a recent study among Medicare beneficiaries, diagnostic testing accounts for about one-third of glaucoma-related costs (excluding medication cost).41
There is abundant evidence from previous quantitative studies supporting participants’ assertion that disease severity has a direct impact on the costs of glaucoma. According to a US study, annual direct medical costs for patients with early glaucoma, advanced glaucoma, and end-stage glaucoma averaged $623, $1915, and $2511, respectively.36 European studies have reported similar findings. Resource utilization and direct medical costs increase as disease worsens, and medication costs ranged from 42% to 56% of direct costs at each disease stage.40 In a German cross-sectional study examining treatment costs of OHT and POAG, average total annual direct costs per patient were €226 for OHT, €423 for early POAG, €493 for moderate POAG, and €809 for advanced POAG.42 Among patients with early glaucoma, medication costs comprise most of the cost of care.39,42 For those with advanced disease, indirect costs such as costs for home health care and rehabilitation become predominant.43,44
The finding that many of the participants give considerable thought to cost—specifically fees charged to patients—in their prescribing decisions (in the context of ensuring efficacy) suggests that awareness of drug cost to patients is fairly high among prescribing clinicians. However, the results of the present study also suggest that some barriers exist to implementing cost-effectiveness decisions in the treatment of glaucoma. As the group noted, cost information for medications is often not readily accessible. This is not surprising, given that multiple middlemen (insurers, manufacturers, and pharmacy benefit managers) are involved in establishing drug prices. Without knowing what a drug’s actual price is at the pharmacy, it is difficult for clinicians to base decisions on costs.
Additionally, clinical decision-making that aims to reduce cost requires the guidance of research showing the relative cost-effectiveness of therapeutics and treatment strategies, but such evidence is largely lacking in the literature. Based on their own experience and a review of select economic studies in the field, this group of glaucoma specialists was of the opinion that there is a shortage of solid, useful data on cost-effectiveness of glaucoma therapies in the present literature. Major questions—such as how cost-effective a particular medication is compared to other treatment modalities such as laser trabeculoplasty or surgery and which medication is most cost-effective in lowering IOP—still lack a definite answer, although some evidence exists suggesting that first-line PGA monotherapy provides greater value than laser trabeculoplasty assuming optimal medication adherence and is the more cost-effective treatment compared to other types of available glaucoma medications.16,45–48 This highlights the need for unbiased, well-designed economic studies to establish the relative cost-effectiveness and impact on quality of life of the treatment regimens for OAG or OHT and to identify opportunities for further savings.
Since individual and societal economic burdens of glaucoma both increase with disease severity, early identification and effective treatment of patients may help reduce the overall costs.7 In support of this concept, a French study modeling the lifetime treatment cost in glaucoma showed that initial treatment with the most effective drug would reduce medical and social costs.49 Currently, PGAs are widely preferred as the first-line treatment for OAG or OHT. Highly effective in IOP-lowering and available in generic forms, PGAs are considered to be an overall cost-effective treatment option. Even so, as this group’s clinical experience indicates, many patients do not achieve adequate IOP-lowering with available agents and require further interventions, increasing the cost of the disease. While cost-effectiveness information on the two latest additions to the treatment options for glaucoma—LBN and netarsudil—is currently lacking, there is clearly a need for more cost-effective IOP-lowering medications (Table 2).
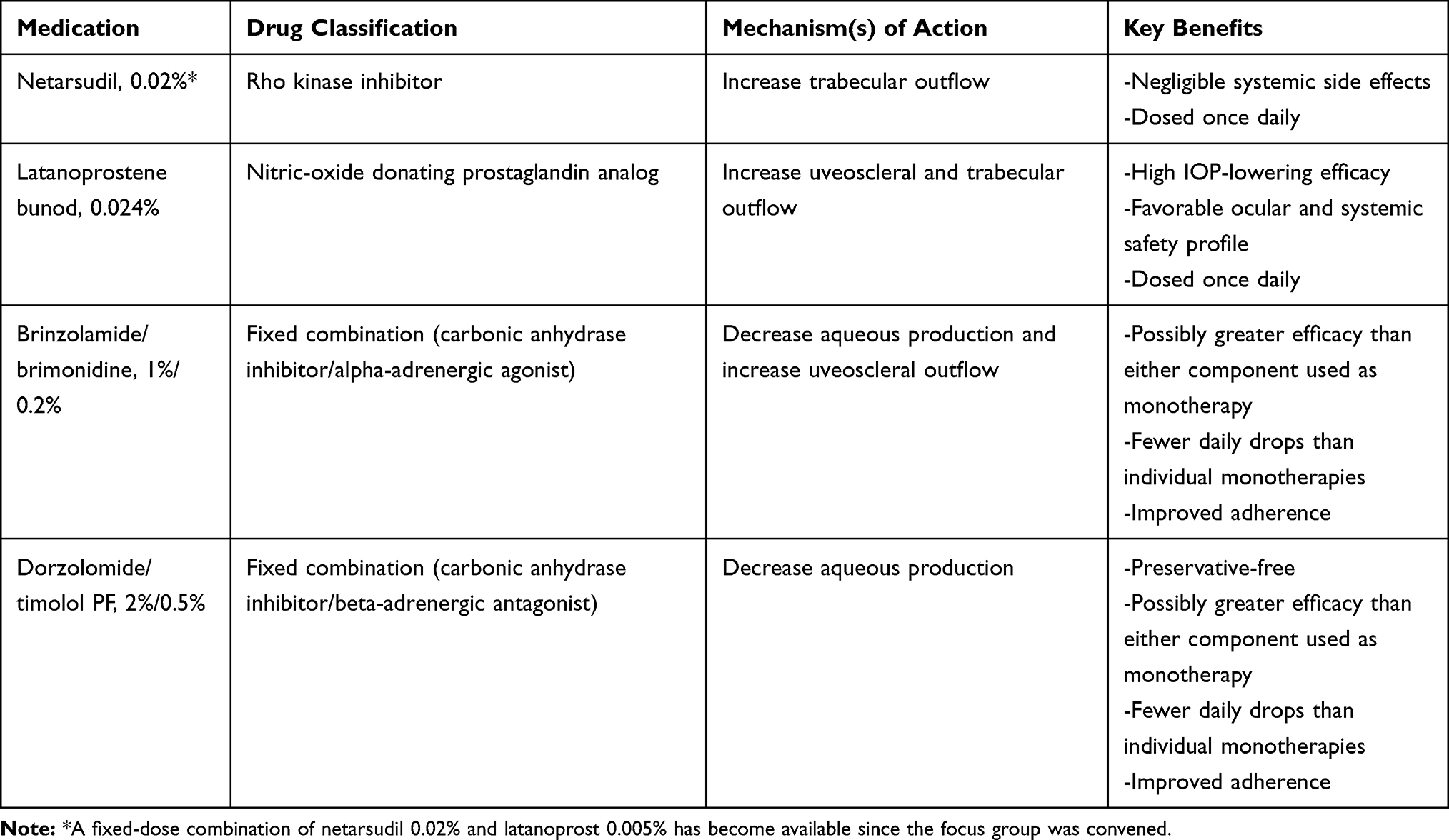 |
Table 2 Glaucoma Medications Approved in the US Since 2013 |
In reality, prices for new medications are relatively high, but price alone does not determine whether or not a treatment is cost-effective. Any economic assessment of a new treatment must also take into account the other determinant of its cost-effectiveness: the clinical benefits it provides, which may translate to savings in other categories of care. As pointed out by participants of this study, a new medication can be cost-effective as long as it provides enough “added value” for which patients and the society are willing to pay.
One medication that participants discussed in this context was LBN 0.024%, the NO-donating PGA approved in late 2017 for lowering IOP in patients with OAG or OHT. LBN acts through its two metabolites—latanoprost acid and an NO-releasing moiety (butanediol mononitrate)—and lowers IOP by enhancing aqueous outflow through both the uveoscleral and trabecular meshwork pathways.50 The new drug appears to have all the important therapeutic advantages of a first-line therapy: high IOP-lowering efficacy, once-daily dosing, negligible systemic side effects, and low rate of ocular hyperemia. In a pooled analysis of the pivotal clinical trials, it was more effective at lowering IOP than timolol 0.5% and safe and well tolerated.51 Furthermore, LBN has been associated with an IOP reduction of 1 to 1.5 mm Hg greater than that of latanoprost 0.005% (Xalatan).33
An incremental improvement in efficacy, such as that reported with LBN, could be fairly significant from the cost-effectiveness standpoint. As mentioned, more effective lowering of IOP and the resulting decrease in the risk of glaucoma progression itself could generate cost savings from reduced health care resource utilization. In a study using a cost-offset model to analyze the clinical and economic outcomes of PGAs, an extra 1 mm Hg of IOP reduction accounted for fewer cases of progression and increased cost savings on office visits, visual field tests, additional glaucoma medications, and surgeries over a 7-year period.52 Further, when a monotherapy combines greater efficacy with a once-daily regimen and a tolerable side effect profile, treatment persistence may improve, with less likelihood of medication addition or switch and potentially better adherence. Poor adherence to topical therapy is a well-established challenge in the management of glaucoma patients.53,54 According to the Glaucoma Adherence and Persistency Study, only 10% of patients are continuously persistent with IOP-lowering medications throughout a year, and, among the slightly more than half of patients who restart after a gap in refilling the prescription, nearly 80% will have at least another gap.53 One possible barrier to adherence is the use of adjunctive agents, which is required within a year for adequate IOP control in about one-third of patients starting glaucoma therapy and has been shown to contribute to higher management costs.55–57,59 Side effects of medications may also adversely impact adherence to therapy.56,60
Netarsudil 0.02%, another new topical therapy that is most recently available for reducing IOP in patients with glaucoma or OHT, is a Rho kinase (ROCK) inhibitor. Like LBN, netarsudil enhances trabecular outflow facility.35 The drug is thought to also decrease aqueous production and episcleral venous pressure. Clinical trial data suggest that netarsudil is not as effective as the PGAs, and that more than half of patients experience conjunctival hyperemia.35,61 As the most common side effect of topical ocular prostaglandins, hyperemia in glaucoma patients has been shown to be a major reason for medication changes and result in increased overall treatment costs.59,62 Given that it is conveniently dosed once-daily and no associated systemic safety issues have been identified, however, netarsudil could be potentially a more cost-effective adjunctive option relative to the available alternatives.
Limitations of the present study include the small sample size (a single focus group of only six participants) and the lack of participant diversity with regard to demographics and/or professional backgrounds. In particular, the study included no input from comprehensive ophthalmologists or optometrists, who also manage glaucoma patients in everyday practice. All the participants were glaucoma specialists, whose patients are more likely to have advanced disease and thus require special treatment considerations. Although the group discussions yielded meaningful data, the results may not be generalizable. The majority of this group of glaucoma specialists said that they discuss medication costs with their patients, for example, but research indicates that cost-related conversations between ophthalmologists and glaucoma patients are uncommon. In a recent study that analyzed 275 video-recorded glaucoma office visits at six different medical centers located in various geographic areas, only 87 visits involved a discussion of medication cost.63
In summary, the present study provides new data on glaucoma specialists’ knowledge and attitudes about cost-effectiveness and cost-effectiveness research in glaucoma therapy. The results suggest that these clinicians support the incorporation of cost-effectiveness into treatment decisions for glaucoma patients and are willing to provide care proved to be cost-effective. A more robust evidence base is needed to derive clear practical guidelines for decisions based on cost-effectiveness. Newer IOP-lowering medications with the potential to provide clinically meaningful benefit, such as LBN 0.024% and netarsudil 0.02%, or a fixed-dose combination of netarsudil and latanoprost approved for marketing after this focus group convened, may be helpful in applying cost-effectiveness to the treatment of OAG or OHT.
Acknowledgments
This pilot focus study was conducted by all listed authors, with editorial assistance from Ethis Inc. Funding was provided by Bausch Health US, LLC.
Disclosure
Dr Robert N Weinreb reports grants and personal fees from Bausch Health US, LLC, personal fees from Aerie Pharmaceuticals, personal fees from Allergan, personal fees from Eyenovia, and personal fees from Novartis, outside the submitted work. Dr Robert M Feldman reports personal fees from Bausch Health US, LLC, personal fees from Alcon, and personal fees from Aerie, outside the submitted work. Dr. Jeffrey M Liebmann reports personal fees from Bausch Health US, LLC, personal fees from Aerie Pharmaceuticals, personal fees from Allergan, and personal fees from Novartis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, Vision Loss Expert Group of the Global Burden of Disease Study, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. doi:10.1136/bjo.2005.081224
4. Vajaranant TS, Wu S, Torres M, Varma R. The changing face of primary open-angle glaucoma in the United States: demographic and geographic changes from 2011 to 2050. Am J Ophthalmol. 2012;154(2):303–314. doi:10.1016/j.ajo.2012.02.024
5. Freeman EE, Munoz B, West SK, et al. Glaucoma and quality of life: the Salisbury eye evaluation. Ophthalmology. 2008;115:233–238. doi:10.1016/j.ophtha.2007.04.050
6. McKean-Cowdin R, Wang Y, Wu J, Los Angeles Latino Eye Study Group, et al. Impact of visual field loss on health-related quality of life in glaucoma: the Los Angeles Latino Eye Study. Ophthalmology. 2008;115:941–948. doi:10.1016/j.ophtha.2007.08.037
7. Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011;152(4):515–522. doi:10.1016/j.ajo.2011.06.004
8. Prager AJ, Liebmann JM, Cioffi GA, Blumberg DM. Self-reported function, health resource use, and total health care costs among medicare beneficiaries with glaucoma. JAMA Ophthalmol. 2016;134(4):357–365. doi:10.1001/jamaophthalmol.2015.5479
9. Wittenborn JS, Rein DB The future of vision: forecasting the prevalence and costs of vision problems. NORC at the University of Chicago. Prepared for Prevent Blindness America, June 11, 2014. Available from: https://www.preventblindness.org/sites/default/files/national/documents/Future_of_Vision_final_0.pdf.
10. Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004;111(8):1439–1448. doi:10.1016/j.ophtha.2004.01.025
11. Bramley T, Peeples P, Walt JG, et al. Impact of vision loss on costs and outcomes in medicare beneficiaries with glaucoma. Arch Ophthalmol. 2008;126:849–856. doi:10.1001/archopht.126.6.849
12. Kymes SM, Plotzke MR, Li JZ, Nichol MB, Wu J, Fain J. The increased cost of medical services for people diagnosed with primary open angle glaucoma – a decision analytic approach. Am J Ophthalmol. 2010;150(1):74–81. doi:10.1016/j.ajo.2010.01.037
13. Rein DB, Wittenborn JS, Lee PP, et al. The cost-effectiveness of routine office-based identification and subsequent medical treatment of primary open-angle glaucoma in the United States. Ophthalmology. 2009;116(5):823–832. doi:10.1016/j.ophtha.2008.12.056
14. Stewart WC, Stewart JA, Nasser QJ, Mychaskiw MA. Cost-effectiveness of treating ocular hypertension. Ophthalmology. 2008;115(1):94–98. doi:10.1016/j.ophtha.2007.01.040
15. Kymes SM, Kass MA, Anderson DR, et al. Management of ocular hypertension: a cost-effectiveness approach from the ocular hypertension treatment study. Am J Ophthalmol. 2006;141(6):997–1008. doi:10.1016/j.ajo.2006.01.019
16. Lachaine J, Hodge WG, Steffensen I, et al. Prostaglandin analogues for ophthalmic use: a cost-effectiveness analysis. Can J Ophthalmol. 2008;43(1):33–41. doi:10.3129/i07-182
17. Bhosle MJ, Reardon G, Camacho FT, Anderson RT, Balkrishnan R. Medication adherence and health care costs with the introduction of latanoprost therapy for glaucoma in a medicare managed care population. Am J Geriatr Pharmacother. 2007;5:100–111. doi:10.1016/j.amjopharm.2007.05.004
18. Cantor LB, Katz LJ, Cheng JW, Chen E, Tong KB, Peabody JW. Economic evaluation of medication, laser trabeculoplasty and filtering surgeries in treating patients with glaucoma in the US. Curr Med Res Opin. 2008;24:2905–2918. doi:10.1185/03007990802379996
19. Costagliola C, Parmeggiani F, Sebastiani A. Assessing the cost-effectiveness of switching from a beta-blocker to latanoprost in the treatment of ocular hypertension. Expert Opin Pharmacother. 2003;Oct:1775–1788. doi:10.1517/14656566.4.10.1775
20. De Natale R, Lafuma A, Berdeaux G. Cost effectiveness of travoprost versus a fixed combination of latanoprost/timolol in patients with ocular hypertension or glaucoma: analysis based on the UK general practitioner research database. Clin Drug Investig. 2009;29:111–120. doi:10.2165/0044011-200929020-00005
21. Denis P, Lafuma A, Berdeaux G. Costs and persistence of alpha-2 adrenergic agonists versus carbonic anhydrase inhibitors, both associated with prostaglandin analogues, for glaucoma as recorded by The United Kingdom general practitioner research database. Clin Ophthalmol. 2008;2:321–329. doi:10.2147/opth.s2832
22. Fiscella R, Walt J. Estimated comparative costs of achieving a 20% reduction in intraocular pressure with bimatoprost or latanoprost in patients with glaucoma or ocular hypertension. Drugs Aging. 2006;23:39–47. doi:10.2165/00002512-200623010-00004
23. Frenkel RE, Frenkel M, Toler A. Pharmacoeconomic analysis of prostaglandin and prostamide therapy for patients with glaucoma or ocular hypertension. BMC Ophthalmol. 2007;27(7):16. doi:10.1186/1471-2415-7-16
24. Fristrom B, Uusitalo H. A randomized, 36-month, post-marketing efficacy and tolerability study in Sweden and Finland of latanoprost versus non-prostaglandin therapy in patients with glaucoma or ocular hypertension. Acta Ophthalmol. 2010;88:37–43. doi:10.1111/j.1755-3768.2009.01663.x
25. Goldberg LD, Walt J. Cost considerations in the medical management of glaucoma in the US: estimated yearly costs and cost effectiveness of bimatoprost compared with other medications. Pharmacoeconomics. 2006;24:251–264. doi:10.2165/00019053-200624030-00005
26. Holmstrom S, Buchholz P, Walt J, Wickstrøm J, Aagren M. The cost-effectiveness of bimatoprost, latanoprost and timolol in treatment of primary open angle glaucoma in five European countries. Curr Med Res Opin. 2006;22:897–905. doi:10.1185/030079906X104687
27. Hommer A, Wickstrøm J, Friis MM, et al. A cost-effectiveness analysis of fixed-combination therapies in patients with open-angle glaucoma: a European perspective. Curr Med Res Opin. 2008;24:1057–1063. doi:10.1185/030079908X280626
28. Noecker RJ, Walt JG. Cost-effectiveness of monotherapy treatment of glaucoma and ocular hypertension with the lipid class of medications. Am J Ophthalmol. 2006;141:S15–S21. doi:10.1016/j.ajo.2005.06.030
29. Orme M, Collins S, Loftus J. Long-term medical management of primary open-angle glaucoma and ocular hypertension in the UK: optimizing cost-effectiveness and clinic resources by minimizing therapy switches. J Glaucoma. 2012;21:433–449. doi:10.1097/IJG.0b013e31821dac2a
30. Payet S, Denis P, Berdeaux G, Launois R. Assessment of the cost effectiveness of travoprost versus latanoprost as single agents for treatment of glaucoma in France. Clin Drug Investig. 2008;28:183–198. doi:10.2165/00044011-200828030-00005
31. Seider MI, Keenan JD, Han Y. Cost of selective laser trabeculoplasty vs topical medications for glaucoma. Arch Ophthalmol. 2012;130:529–530. doi:10.1001/archophthalmol.2012.355
32. Wong WB, Patel VD, Kowalski JW, Schwartz G. An adherence based cost-consequence model comparing bimatoprost 0.01% to bimatoprost 0.03%. Curr Med Res Opin. 2013;29:1191–1200. doi:10.1185/03007995.2013.815159
33. Weinreb RN, Ong T, Scassellati SB, Vittitow JL, Singh K, Kaufman PL, VOYAGER study group. A randomised, controlled comparison of latanoprostene bunod and latanoprost 0.005% in the treatment of ocular hypertension and open angle glaucoma: the VOYAGER study. Br J Ophthalmol. 2015;99(6):738–745. doi:10.1136/bjophthalmol-2014-305908
34. Vyzulta® [package insert]. Bridgewater, NJ: Bausch + Lomb, a division of Bausch Health US, LLC; 2019.
35. Serle JB, Katz LJ, McLaurin E, ROCKET-1 and ROCKET-2 Study Groups, et al. Two Phase 3 clinical trials comparing the safety and efficacy of netarsudil to timolol in patients with elevated intraocular pressure: rho kinase elevated IOP treatment trial 1 and 2 (ROCKET-1 and ROCKET-2). Am J Ophthalmol. 2018;186:116–127. doi:10.1016/j.ajo.2017.11.019
36. Lee PP, Walt JG, Doyle JJ, et al. A multicenter, retrospective pilot study of resource use and costs associated with severity of disease in glaucoma. Arch Ophthalmol. 2006;124(1):12–19. doi:10.1001/archopht.124.1.12
37. Iskedjian M, Walker J, Vicente C, et al. Cost of glaucoma in Canada: analyses based on visual field and physician’s assessment. J Glaucoma. 2003;12:456–462. doi:10.1097/00061198-200312000-00002
38. Rylander NR, Vold SD. Cost analysis of glaucoma medications. Am J Ophthalmol. 2008;145:106–113. doi:10.1016/j.ajo.2007.08.041
39. Lindblom B, Nordmann JP, Sellem E, et al. A multicentre, retrospective study of resource utilization and costs associated with glaucoma management in France and Sweden. Acta Ophthalmol Scand. 2006;84:74–83. doi:10.1111/j.1600-0420.2005.00560.x
40. Traverso CE, Walt JG, Kelly SP, et al. Direct costs of glaucoma and severity of the disease: a multinational long term study of resource utilisation in Europe. Br J Ophthalmol. 2005;89(1):1245–1249. doi:10.1136/bjo.2005.067355
41. Quigley HA, Cassard SD, Gower EW, Ramulu PY, Jampel HD, Friedman DS. The cost of glaucoma care provided to Medicare beneficiaries from 2002 to 2009. Ophthalmology. 2013;120(11):2249–2257. doi:10.1016/j.ophtha.2013.04.027
42. Lorenz K, Wolfram C, Breitscheidel L, Shlaen M, Verboven Y, Pfeiffer N. Direct cost and predictive factors for treatment in patients with ocular hypertension or early, moderate and advanced primary open-angle glaucoma: the CoGIS study in Germany. Graefes Arch Clin Exp Ophthalmol. 2013;251(8):2019–2028. doi:10.1007/s00417-013-2354-z
43. Prum BE
44. Thygesen J, Aagren M, Arnavielle S, et al. Late-stage, primary open-angle glaucoma in Europe: social and health care maintenance costs and quality of life of patients from 4 countries. Curr Med Res Opin. 2008;24:1763–1770. doi:10.1185/03007990802111068
45. Stein JD, Kim DD, Peck WW, Giannetti SM, Hutton DW. Cost-effectiveness of medications compared with laser trabeculoplasty in patients with newly diagnosed open-angle glaucoma. Arch Ophthalmol. 2012;130:497–505. doi:10.1001/archophthalmol.2011.2727
46. Bernard LM, Althin R, Dhawan R, Grima DT, Lam A, Aballea S. Clinical and economic impacts of latanoprost 0.005% in first-line treatment of open-angle glaucoma and ocular hypertension in France. Eur J Ophthalmol. 2003;13(Suppl 4):S30–S43. doi:10.1177/112067210301304S04
47. Day DG, Schacknow PN, Sharpe ED, et al. A persistency and economic analysis of latanoprost, bimatoprost, or beta-blockers in patients with open-angle glaucoma or ocular hypertension. J Ocul Pharmacol Ther. 2004;20(5):383–392. doi:10.1089/jop.2004.20.383
48. van Gestel A, Webers CA, Severens JL, et al. The long-term outcomes of four alternative treatment strategies for primary open-angle glaucoma. Acta Ophthalmol. 2012;90(1):20–31. doi:10.1111/j.1755-3768.2011.02318.x
49. Nordmann J, Lafuma A, Berdeaux G. Modelling the lifetime economic consequences of glaucoma in France. JMed Econ. 2009;12(1):916. doi:10.3111/13696990902728729
50. Krauss AH, Impagnatiello F, Toris CB, et al. Ocular hypotensive activity of BOL-303259-X, a nitric oxide donating prostaglandin F2α agonist, in preclinical models. Exp Eye Res. 2011;93(3):250–255. doi:10.1016/j.exer.2011.03.001
51. Weinreb RN, Liebmann JM, Martin KR, Kaufman PL, Vittitow JL. Latanoprostene bunod 0.024% in subjects with open-angle glaucoma or ocular hypertension: pooled phase 3 study findings. J Glaucoma. 2018;27(1):7–15. doi:10.1097/IJG.0000000000000831
52. Berenson KL, Kymes S, Hollander DA, Fiscella R, Burk C, Patel VD. Cost-offset analysis: bimatoprost versus other prostaglandin analogues in open-angle glaucoma. Am J Manag Care. 2011;17(9):e365–e374.
53. Friedman DS, Quigley HQ, Gelb L, et al. Using pharmacy claims data to study adherence to glaucoma medications: methodology of the Glaucoma Adherence and Persistency Study (GAPS). Invest Ophthalmol Vis Sci. 2007;48(11):5052–5057. doi:10.1167/iovs.07-0290
54. Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the travatan dosing aid study. Ophthalmology. 2009;116:191–199. doi:10.1016/j.ophtha.2008.09.004
55. Robin AL, Covert D. Does adjunctive glaucoma therapy affect adherence to the initial primary therapy? Ophthalmology. 2005;112(5):863–868. doi:10.1016/j.ophtha.2004.12.026
56. Tsai JC. A comprehensive perspective on patient adherence to topical glaucoma therapy. Ophthalmology. 2009;116:S30–S36. doi:10.1016/j.ophtha.2009.06.024
57. Schmier JK, Hulme-Lowe CK, Covert DW. Adjunctive therapy patterns in glaucoma patients using prostaglandin analogs. Clin Ophthalmol. 2014;8:1097–1104. doi:10.2147/OPTH.S63760
58. Stewart WC, Stewart JA, Mychaskiw MA. Cost-effectiveness of latanoprost and timolol maleate for the treatment of glaucoma in Scandinavia and the United Kingdom, using a decision-analytic health economic model. Eye (Lond). 2009 Jan;23(1):132–140. doi:10.1038/sj.eye.6702964
59. Schmier JK, Covert DW, Robin AL. Estimated first-year costs of prostaglandin analogs with/without adjunctive therapy for glaucoma management: a United States perspective. Curr Med Res Opin. 2007;23(11):2867–2875. doi:10.1185/030079907X233287
60. Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the glaucoma adherence and persistency study. Ophthalmology. 2008;115:1320–1327. doi:10.1016/j.ophtha.2007.11.023
61. Bacharach J, Dubiner HB, Levy B, Kopczynski CC, Novack GD, AR-13324-CS202 Study Group. Double-masked, randomized, dose-response study of AR-13324 versus latanoprost in patients with elevated intraocular pressure. Ophthalmology. 2015;122(2):302–307. doi:10.1016/j.ophtha.2014.08.022
62. Schwartz GF, Tan J, Kotak S. Hyperemia-associated costs of medication changes in glaucoma patients treated initially with prostaglandin analogs. J Ocul Pharmacol Ther. 2009;25(6):555–561. doi:10.1089/jop.2009.0057
63. Slota C, Davis SA, Blalock SJ, et al. Patient-physician communication on medication cost during glaucoma visits. Optom Vis Sci. 2017;94(12):1095–1101. doi:10.1097/OPX.0000000000001139
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.