Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Current Insights Into The Management Of Discoid Lupus Erythematosus
Authors Company-Quiroga J, Alique-García S, Romero-Maté A
Received 9 April 2019
Accepted for publication 18 September 2019
Published 3 October 2019 Volume 2019:12 Pages 721—732
DOI https://doi.org/10.2147/CCID.S184824
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jaime Company-Quiroga,* Sergio Alique-García,* Alberto Romero-Maté
Dermatology Department, Fuenlabrada Univesity Hospital, Madrid, Spain
*These authors contributed equally to this work
Correspondence: Jaime Company-Quiroga
Dermatology Department, Fuenlabrada Univesity Hospital, Camino del Molino 2, Fuenlabrada, Madrid 28942, Spain
Email [email protected]
Abstract: Discoid lupus erythematosus is the most disfiguring and common presentation of chronic cutaneous lupus erythematosus. Although most patients will respond to lifestyle measures and topical treatment, a non-negligible number of patients will require systemic and physical therapy, either alone or in combination. We performed a review of the available evidence on the discoid lupus erythematosus treatment. Lifestyle measures and topical treatment (corticosteroids and topical calcineurin inhibitors) remain the therapeutic strategies with the highest evidence level. Within systemic treatment approaches, antimalarial drugs are still the first-line therapy, while other systemic and physical therapies have highly variable evidence. Hence, we propose a therapeutic algorithm based on the strength of recommendations of the different treatment modalities, focusing on the refractory disease.
Keywords: discoid lupus erythematosus, cutaneous lupus erythematosus, disease management
Introduction
Discoid lupus erythematosus (DLE) is the most disfiguring form of cutaneous lupus erythematous (CLE). Recurrent outbreaks of inflammatory lesions usually affecting photo exposed areas (face, ears) and scalp, lead to a prominent scarring that might have a high impact on the quality of life of the patients. Therefore, early treatment is mandatory to minimize these undesirable consequences. Most patients with DLE will respond to strict photoprotection, smoking cessation and topical treatment (corticosteroids, calcineurin inhibitors). Antimalarial drugs are considered the first-line systemic treatment. Refractory DLE may benefit from other systemic therapies, although data on their effectiveness are limited to small open-label studies, retrospective reviews, case series, and case reports.
Methodology
We carry out a search in the PubMed, Web of Science and EMbase databases that include all articles published before January 2018, in the English and Spanish languages.
In each of the databases we use the appropriate vocabulary to perform the search. We also reviewed some papers included in the bibliography of the previous reviews. The keywords and search methods used for the Pubmed database were as follows:
Discoid lupus erythematosus
Intervention OR therapy OR treatment
#1 AND #2
After conducting the exhaustive search, 324 articles were suggestive of being reviewed. In a first screening we found 27 repeated articles and 54 works whose main objective was not focused on the treatment of DLE. The remaining 243 articles were thoroughly reviewed, of which 150 were suppressed for different reasons. Finally, 95 articles were included to carry out this review.
The strength of recommendation and the level of evidence were established for each therapy (Tables 1–3) according to the NICE (National Institute for Health and Clinical Excellence) guidelines.
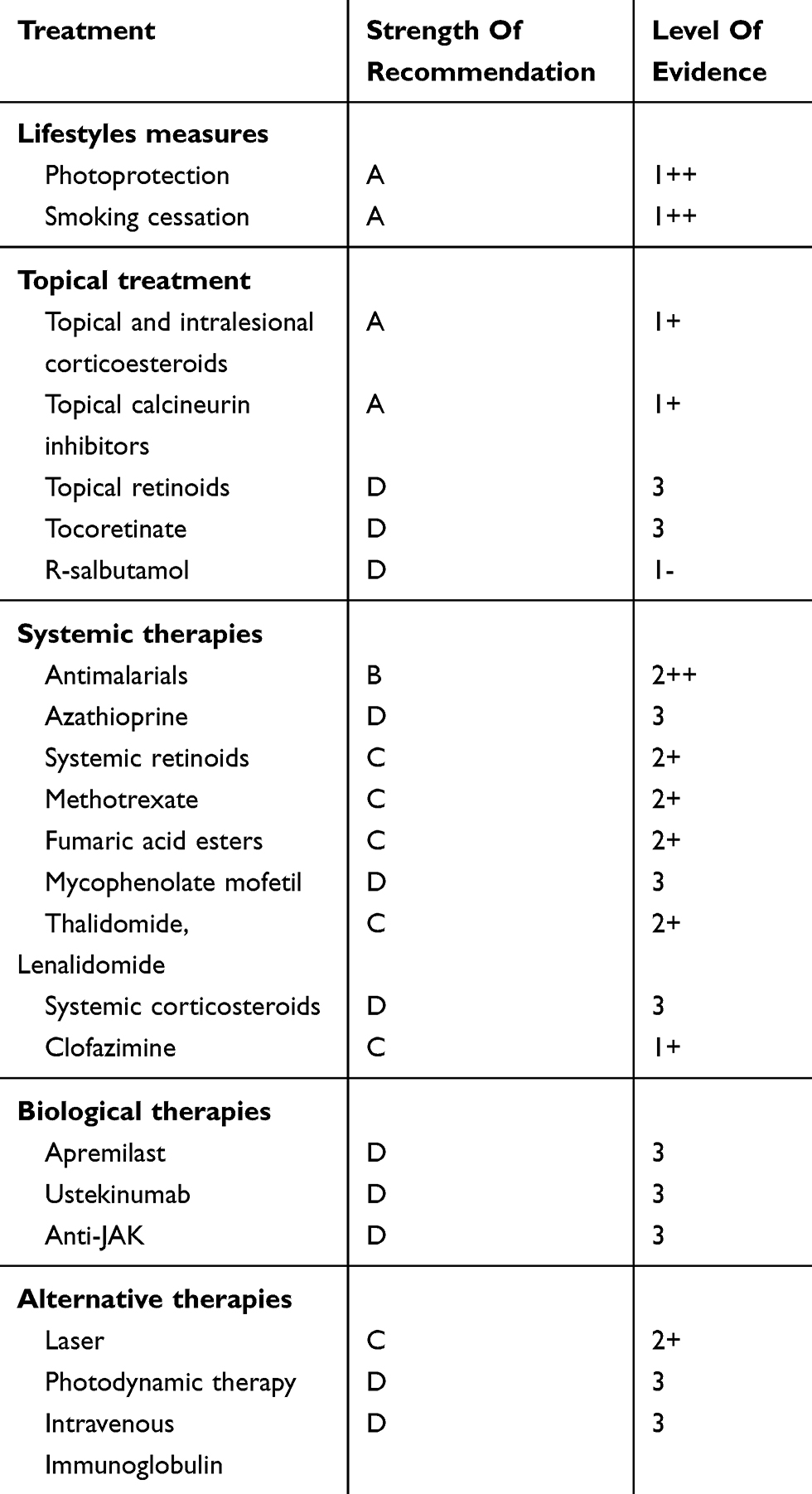 |
Table 1 Strength Of Recommendation And Level Of Evidence |
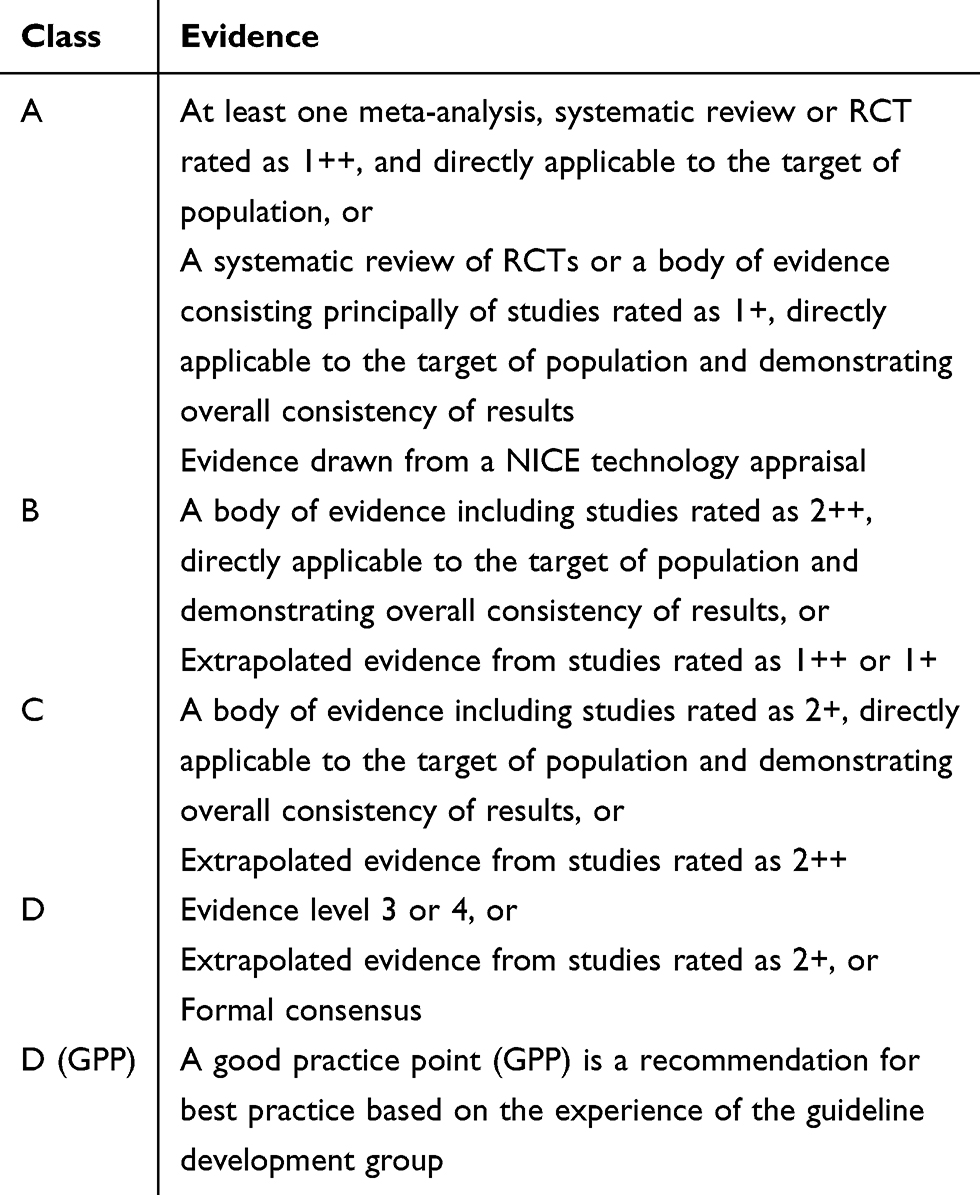 |
Table 2 Strength Of Recommendation (NICE, National Institute For Health And Clinical Excellence; RCT, Randomised Controlled Trial) |
 |
Table 3 Level Of Evidence (RCT, Randomized Controlled Trial; A. Studies With A Level Of Evidence “-” Should Not Be Used As A Basis For Making A Recommendation) |
Lifestyles Measures
Photoprotection (Strength Of Recommendation A, Level Of Evidence 1++)
Ultraviolet exposure is the most important precipitating factor of CLE flares. Daily photoprotection is essential to prevent the appearance of skin lesions, because UVA and UVB are known to cause CLE flares.1 Basic recommendations for patients include: avoid sunlight during peak day light hours, as well as artificial ultraviolet light used in tanning booths. It is essential to use sunscreen properly. Based on a randomized, controlled, double-blind clinical trial of 25 patients with CLE, it is recommended to apply a sufficient amount of 50 SPF sunscreen (at least 2mg/cm2 of body surface) 20–30 mins before exposure. Taking these factors into account, the authors of the trial published a total protection against UVA and UVB irradiation.2 Physical filters are recommended over chemical filters because they cover a broad radiation spectrum. In addition, the risk of vitamin D deficiency must be considered in patients who avoid sun exposure due to DLE. In these cases it is recommended to perform screening of 25-hydroxyvitamin D, and in cases of deficiency provide supplements of vitamin D3 or cholecalciferol (especially in countries with few sunlight hours).3
Recently, a survey on the habits of prophylactic measures in patients with CLE has been published.4 The results highlight that most of the physicians surveyed provided information about UV danger in CLE patients. They also provided prophylactic advice such as using topical photoprotector or wearing protective clothes. Interestingly, some notable differences were found, such as that physicians from Japan recommended sunscreens less frequently than in the USA or Europe.
Smoking Cessation (Strength Of Recommendation A, Level Of Evidence 1++)
Smoking is another cause of CLE worsening. Chasset et al conducted a study in patients with DLE and healthy controls.5 Their results showed a higher rate of smokers in individuals with DLE. Other studies have reported worse quality of life and greater severity of the disease (CLASI index) in smoking patients. There are also concerns about the decrease of antimalarials efficacy.
The former survey reported interesting results regarding smoking. Comparing with advice on sun exposure, smoking was a less discussed topic among physicians and CLE patients.4 The results showed that almost half of the participant physicians incentived patients to quit smoking. However, 13.3% recommended it rarely and 2% never mentioned it.
Topical Treatment
Topical And Intralesional Corticosteroids (Strength Of Recommendation A, Level Of Evidence 1+)
Topical corticosteroids are often the first step in the treatment of DLE, but they are commonly insufficient in isolation.6 They exert their effect on both B and T cells, and decrease immunoglobulins and TNF alpha production.7 In the review of the literature, we have found only one clinical trial that tests its efficacy in CLE. This is a 12-week crossover study with a total of 78 patients in whom healing or very good response was evidenced in 27% of the subjects randomized with fluocinonide 0.05% cream, with respect to 10% of the patients treated with hydrocortisone 1% cream at 6 weeks.6 These results highlight the convenience of using high-potency topical corticosteroids over medium- or low-potency topical corticosteroids in DLE patients. Most authors recommend the use of high-potency corticosteroids in acute flares, especially in cases of severe disease. It is important to know and warn patients of possible side effects if these drugs are used for long periods of time (skin atrophy, telangiectasia, striae, solar purpura and hypertrichosis). In patients with chronic DLE lesions not resolved with corticosteroids or topical calcineurin inhibitors, treatment with intralesional corticosteroids may be performed.8
Topical Calcineurin Inhibitors (Strength Of Recommendation A, Level Of Evidence 1+)
They are frequently used in thin skin areas such as the facial region, or in skin damaged by chronic treatment with topical corticosteroids. They decrease or block cytokine production by activated T lymphocytes. Currently there are two commercial preparations: pimecrolimus 1% cream and tacrolimus 0.03% or 0.1% ointment. Pothinamthong et al demonstrated good response with the combination of twice-daily tacrolimus 0.1% and once-daily clobetasol 0.05% in the treatment of DLE.9 Another randomized study in which 14 of 38 patients were diagnosed with DLE, proved better response in those treated with 0.1% tacrolimus ointment twice-daily for 3 months over patients treated with vehicle.10 Barikbin et al performed a comparative study (10 patients with DLE) between pimecrolimus 1% cream twice-daily and betamethasone 0.1% cream twice daily for 8 weeks. With both treatments they obtained similar responses improving the clinical severity.11 In a case series of 3 patients with scarring alopecia caused by DLE, the usefulness of the combination of a 0.3% tacrolimus lotion with oral antimalarial therapy was demonstrated. In these patients they achieved hair regrowth.12
Topical Retinoids (Strength Of Recommendation D, Level Of Evidence 3)
The mechanism of action of topical retinoids is based on the increase of collagen synthesis and epidermal turnover, as well as the inhibition of melanogenesis and inflammation.13 There are some clinical cases that have proven the efficacy of tretinoin and tazarotene in the treatment of DLE and hypertrophic lupus erythematosus. Edwards et al reported the complete resolution of facial lesions secondary to DLE in a woman, performing treatment with topical tazarotene 0.05% gel daily at night for several weeks.14
Tocoretinate (Strength Of Recommendation D, Level Of Evidence 3)
Tocoretinate or tretinoin tocopheryl is an alpha-tocopherol ester of all trans-retinoic acid (ATRA or tretinoin). With this combination we achieve the therapeutic effects of retinoids with less skin irritation. A two-case DLE report was published showing successfully treatment with topical tocoretinate. The first patient is a 43-year-old woman with erythematous-desquamative plaques with pigmentary changes and cutaneous atrophy located on the cheeks and ears. Topical tocoretinate twice daily was started. The authors describe improvement of pigmentation in 3 months and improvement of atrophy in 12 months. The second patient is a 37-year-old man with erythematous and erosive plaques on his temple. After 2 weeks of treatment with topical tocoretinate the lesions improved significantly. At 11 months, cutaneous atrophy was much less evident.15
R-Salbutamol (Strength Of Recommendation D, Level Of Evidence 1-)
R-Salbutamol is a beta2-adrenergic receptor agonist; this receptor is present in the outer membrane of several cell types. The binding of R-salbutamol to the receptors produces an inhibition of the inflammatory response that includes cytokines such as interleukin-2 and interferon-C.16 Jemec et al designed a randomized clinical trial to assess the efficacy of R-salbutamol in the treatment of DLE. They included 37 patients diagnosed with DLE: 19 were treated with R-salbutamol 0.5% cream twice-daily for 8 weeks, and the rest received placebo. In the R-salbutamol group authors demonstrated overall improvement both in the intensity of the lesions and in the symptoms.16 However, no subsequent studies have been published, so the treatment recommendation is controversial.
Systemic Therapies
Antimalarial Drugs (Strength Of Recommendation B, Level Of Evidence 2++)
Antimalarial drugs were initially used for cutaneous lupus erythematosus (CLE) and later for systemic disease.17 The mechanism by which they are effective is still controversial. However, the last theories point to a reduction of the lysosomal pH and the chemotaxis/phagocytosis of immune cells, inducing an autoantigen presentation blockage. They also induce anti-inflammatory function, inhibiting cytokines (IL-1, IL-2, INF-γ, INF-α) and antagonizing the prostaglandin effects.18 Hydroxychloroquine (HCQ) is considered the first line oral treatment for DLE. Wahie et al designed a multicenter retrospective cohort study in 200 patients diagnosed with DLE who received long-term HCQ (more than 6 months).19 An adequate clinical response based on protocolized retrospective designation of response in medical case notes was achieved in 60% of patients within the first 6 months, which decreased to 45% after this date. 1 out of 5 responders lost their response after a median interval of 2 years, but they often regained disease control with a combination of HCQ and mepacrine. Non-responders within the first systemic frequently underwent oral corticosteroid therapy. Variable outcomes from different HCQ combinations with systemic therapies (immunosuppressive therapies, retinoids) or either phototherapy have been reported. Predictive variables of poor response to HCQ are disseminated disease and systemic involvement.20 One study evaluated the safety of chloroquine (CQ) and HCQ by describing the adverse reactions (including ocular toxicity) and the reasons for antimalarial suspension in patients with SLE and DLE. Among 504 patients who had received antimalarial therapy (1.4% HCQ, 88.5% HCQ, 10.1% both therapies but not concomitantly), less than 20% reported adverse reactions. Withdrawal of therapy was decided in less than 10% of patients in an average duration of 7 years of treatment (both temporary and definitive), whose main cause were ophthalmic effects, followed by skin rashes and gastrointestinal symptoms. While the latter are considered mild adverse reactions, treatment withdrawal is mandatory when retinal, neuromuscular and cardiological involvement are present.21–23 Skin reactions include hyperpigmentation, urticaria, pruritus, annular erythema, morbilliform rash, exfoliative dermatitis and xerosis.24,25 Ocular symptoms do not always correlate with retinal toxicity, which has a low incidence and is more frequent and severe in patients taking CQ.22 Antimalarial drugs bind to melanin of the macular pigment epithelium, but the mechanism of toxicity is still unclear. The daily dose (> 5 mg/kg and >2,3 mg/kg of HCQ y CQ for ideal weight, respectively), antimalarial treatment during more than 5 years, renal failure, concomitant use with tamoxifen and previous macular damage are major risk factors for developing retinal toxicity. The American Academy of Ophthalmology screening guidelines recommend a baseline evaluation for all patients before initiating antimalarial therapy or within the first year (fundus examination, visual fields and at least one objective test), and then annually after the 5th year of treatment. In high risk-patients (see above), the evaluation should be performed every 6 months.26 Several studies have shown the safety of antimalarials in pregnancy.27 The main strategy employed following failure of antimalarial monotherapy is switching to another antimalarial agent. A multicenter retrospective observational study in 64 patients with CLE who underwent antimalarial switching between HCQ and CQ both for inefficacy (48/62) and adverse effects (16/64), revealed that cutaneous improvement was detected in 50% of cases after 3 months, although the response used to be transient. The effectiveness of the switching was better (sustained response) when the first antimalarial agent withdrawal was for adverse effects.28
Azathioprine (Strength Of Recommendation D, Level Of Evidence 3)
Azathioprine (AZT) is a purine synthesis inhibitor with immunosuppressive effect. It has been effective for the treatment of DLE in some case reports.29–31 However, other case reports exhibited partial or no response.32 Therefore, the evidence of the use of AZT in DLE is limited. In addition, the possible side effects of treatment should be considered, including myelosuppression and the possibility of developing malignant tumors. The active substance thiopurine methyltransferase (TPMT) must be measured before starting treatment. If there are low levels of TMPT, AZT is contraindicated.33
Systemic Retinoids (Strength Of Recommendation C, Level Of Evidence 2+)
Retinoids act by modifying the function of the epidermal keratinocytes through their binding as ligands to the nuclear transcription factors. In a study the efficacy of isotretinoin was evaluated in 10 patients with CLE (9 with DLE). Patients received 80 mg daily of treatment for 16 weeks. Very good response was obtained in 80% (the other 2 patients lost the follow-up). No serious side effects were reported, except for xerosis.34 With respect to alitretinoin, Kuhn et al reported therapeutic success in 3 patients with CLE, so it could be a therapy to be considered in DLE, although specific studies are needed.35 It should be borne in mind that retinoids are teratogenic agents, so the use of contraceptive methods in women of childbearing age is mandatory. In addition, retinoids can alter the liver profile and raise cholesterol and triglycerides, so analytical tests are necessary during treatment.36,37
Methotrexate (Strength Of Recommendation C, Level Of Evidence 2+)
Methotrexate (MTX) is a folic acid antagonist that has been used since the 1960s for systemic lupus erythematosus. Proposed mechanisms for its therapeutic properties in connective tissue diseases include anti-inflammatory effects secondary to increased production of adenosine, inhibitory action on lymphocytes and neutrophils, and suppression of antibody production. Bottomley and Goodfield first described its use in 4 cases of refractory DLE in 1995, with great improvement in two of them.38 Since then, few studies have been reported about use of MTX in DLE. The most relevant is a retrospective study of 43 patients with refractory CLE, 12 of them with DLE, treated 7,5–25 mg/week methotrexate. A good response in DLE patients, especially in those with localized disease was observed.39 Even if the well-known side effects (gastrointestinal reactions, elevation of liver enzymes and pancytopenia) require monitoring blood tests, methotrexate is a well-tolerated and safety drug when used at standard doses.
Fumaric Acid Esters (Strength Of Recommendation C, Level Of Evidence 2+)
Fumaric acid esters (FAEs) inhibit the transcription factor NF-B activity, as well as the production of proinflammatory cytokines by T lymphocytes. FAEs have been used for years in the treatment of plaque psoriasis. There is published in the literature a clinical trial of 11 patients with recalcitrant DLE (a patient also with SCLE) to evaluate the effectiveness of FAEs.40 The results demonstrated that the mean activity of the disease according to RCLASI (Revised Cutaneous Lupus Erythematosus Disease Area and Severity Index) decreased significantly at 24 weeks of treatment. No serious side effects were reported.
Mycophenolate Mofetil (Strength Of Recommendation D, Level Of Evidence 3)
Mycophenolate mofetil (MMF) is a reversible inhibitor of inosine monophosphate dehydrogenase, the rate-limiting enzyme of the biosynthesis of new guanosine triphosphate (GTP) used for B and T lymphocytes proliferation.41 MMF has shown effectiveness in the treatment of all subtypes of CLE in small case series. Goyal et al reported very good clinical response in 2 patients with DLE and systemic lupus erythematosus who presented palmoplantar lesions resistant to other treatments.42 In contrast, Pisoni et al administered MMF to 6 patients with therapy-resistant CLE. Five patients did not obtain response and only 1 achieved partial response. Therefore, the authors recommend limiting its use to severe CLE.43
Lenalinomide And Thalidomide (Strength Of Recommendation C, Level Of Evidence 2+)
Thalidomide has been used in refractory cutaneous lupus erythematosus due to its effect inhibiting the production of inflammatory cytokines and preventing keratinocyte apoptosis induced by UVB light. Frankel et al treated 5 patients with refractory CLE with low-dose thalidomide (50 mg/d). 80% of patients partially or completely resolved after an average of 5,5 weeks of therapy.44 These results are similar to previous retrospective studies using classical doses of 100mg/d.45,46 Low dose was not related with a lower incidence of neuropathy (80% patients), which resolved after drug withdrawal. Although thalidomide is an effective therapy, teratogenic activity and deep venous thrombosis limit its use. It should be noted that patients with DLE have higher recurrence rates after cessation of the drug with respect to other variants of CLE.47 Lenalidomide, a synthetic analogue of thalidomide with a similar mechanism of action, has proved to be a useful treatment in several studies, including a prospective phase II pivotal study.48–51 It is usually administered at doses of 5–10 mg/day, with a lower incidence of neuropathy than thalidomide, but similar recurrence rates of DLE lesions.51 The main adverse effect of lenalinomide are cytopenias, which rarely require treatment withdrawal, while blood test monitoring is mandatory.48
Systemic Corticosteroids (Strength Of Recommendation D, Level Of Evidence 3)
Systemic corticosteroids have a limited effect on chronic forms of lupus. They are usually used in the opening phase of treatment, when the lesions have a high inflammatory activity.52 They can also be used in combination with other immunosuppressants in the induction phase. The usual dose is 0.5 to 1 mg/kg/day orally, with a subsequent decrease after 2 to 4 weeks or 3 g/day in pulses intravenously, as described for SCLE.52 Its routine use is not recommended due to adverse effects.
Clofazimine (Strength Of Recommendation C, Level Of Evidence 1+)
Clofazimine inhibits mycobacterial growth by binding to DNA. Clofazimine also exerts antiinflammatory properties. Bezerra et al conducted a randomized clinical trial in which 17 patients with CLE (12 with DLE) were treated with chloroquine (250 mg daily) and 16 patients with CLE (14 with DLE) were treated with clofazimine (100 mg daily) added to sunscreen and oral prednisone. At 6 months, 82.4% of the patients in the clofazimine group experienced complete or almost complete resolution of the skin lesions, compared with 75% in the chloroquine group.53
Biological Therapies
Apremilast (Strength Of Recommendation D, Level Of Evidence 3)
Apremilast is a phosphodiesterase-4 (PDE4) inhibitor drug. Its main mechanism of action focuses on nulling Th1- and Th17-mediated immune activity. Currently there are numerous studies that support its effectiveness in psoriasis. Considering its mechanism of action could also be effective in other inflammatory diseases such as DLE. De Souza et al designed a study in which 8 patients were treated with apremilast (20 mg, every 12 hrs) for 85 days. A significant reduction in the disease activity was observed according to CLASI. The most common drug-related adverse events were nausea, headache and diarrhea. These events were classified as mild to moderate in severity and were transient in time, resolving after the initial 1 to 6 days of the study drug dosing.54
Ustekinumab (Strength Of Recommendation C, Level Of Evidence 3)
Ustekinumab is a monoclonal antibody that binds to the p40 subunit common to IL-12 and IL-23, inhibiting the Th1 and Th17 pathways of inflammation. IL-17 (produced by Th17 lymphocytes) is elevated in the skin of patients with DLE.55 The use of ustekinumab in DLE has anecdotal evidence in the literature, mainly clinical cases in patients with concomitant psoriasis.56–60 Our experience is based on a patient with facial refractory DLE previously treated with classic therapies and rituximab, who achieved good response with ustekinumab (45 mg/12 weeks), first associated with methotrexate and intralesional corticosteroids for 30 months and then in monotherapy.61 Combination might have been a therapeutic clue in disease control. Ustekinumab has a good safety profile and dermatologists have experience and expertise in treating psoriasis.
Anti-JAK (Strength Of Recommendation D, Level Of Evidence 3)
Kahn et al performed a literature review of the role of the JAK-STAT signalling pathway in the pathophysiology of DLE.62 JAK inhibitors (tofacitinib, ruxolitinib) could be useful in reducing the disease activity, that would correlate with a reduction of the epidermal hyperplasia and the inflammatory infiltrate. The main adverse reactions are infections, headaches and diarrhea. Further studies are needed to determine their efficacy in the clinical practice.
Alternative Therapies
Laser (Strength Of Recommendation C, Level Of Evidence 2+)
Contrary to the latest recommendations for the management of CLE developed by the European Dermatology Forum in collaboration with the European Academy of Dermatology and Venereology, laser devices have proven to be useful in active CLE lesions.63–65 Photosensitivity should not be a contraindication for laser application since it is related to UV lights. Of note, pulsed dye lasers, the most common used device, emit pulses of visible light (wavelength of 585–595 nm). Their effectiveness in DLE is based on the selective photothermolysis of the oxyhemoglobin, which induces thermal damage on the dermal microvasculature (a key point in the pathogenesis of CLE).66-68 This would lead to a modulation of inflammation and a subsequent reduction of the dermal infiltration. Several cases of successful treatment of DLE with PDL and IPL have been reported.64,67,69–72 A retrospective study of 16 patients with refractory DLE described the response to treatment with low-fluence PDL and IPL.73 A satisfactory clinical response was observed in all patients both in symptoms and appearance (desquamation, erythema and scar improvement). Laser PDL parameters used were 585nm, 5 mm spot, 0.45 ms, fluence 5.75–6.75 J/cm2 and 595 nm, 7 mm spot 0.45 ms–1.5 ms and 30/20 DCD (Dynamic Cooling Device) fluence 7.5–9 J/cm2. The average number of sessions was 5. IPL was preferred to PDL for telangiectasia treatment. Hyperpigmentation was the unique side effect, which occurred in one patient. No iatrogenic scars were appreciated. Therefore, the safety profile of the above-mentioned lasers is higher than less selective devices (CO2 and argon laser).74 Patients should be educated about photoprotection and informed of the possibility of recurrence. In conclusion, laser is a valuable and safety alternative to systemic therapy, and its early use may be useful in reducing scarring.75
Photodynamic Therapy (Strength Of Recommendation D, Level Of Evidence 3)
Photodynamic therapy (PDT) is a physical treatment widely used in dermatology, especially in non-melanoma skin cancer. The mechanism of action consists in the topical application of a photosensitizer, that accumulates in certain cells and once illuminated (in presence of oxygen), produces a selective cell destruction. In recent years it is being used in inflammatory pathologies with variable results. This therapy produces a local immunosuppression that results in a decrease in the number of Langerhans cells. This fact could explain its function in immuno-mediated skin pathologies.76 To date, two case reports have described DLE remission following PDT treatment. Fernández-Guarino et al treated a 45-yeard-old woman with eight weekly sessions of MAL-PDT showing clinical resolution. After 6 months, the patient remained free of lesions.77 Later, Debu et al reported a 72-year-old man with right cheek DLE lesions. They performed 5 sessions of MAL-PDT (every 2–3 weeks) with progressive improvement of the erythema, with respect to the left cheek (which authors used as control).76 In contrast to these reports, Romero-Maté et al reported PDT failure in two patients with recalcitrant DLE lesions. They performed three and two sessions (one per month) of 5-ALA-PDT (20% 5-aminolevulinic acid), respectively. Maybe the use of ALA instead of MAL played its part in the final result.78
Intravenous Immunoglobulin (Strength Of Recommendation D, Level Of Evidence 3)
Intravenous immunoglobulin (IGIV) is a combination of polyclonal immunoglobulins of plasmatic origin.79 They are commonly used in humoral immunodeficiencies, but also empirically as an immunosuppressant in various autoimmune processes, especially in the field of dermatology.80,81 Specifically, for the treatment of DLE Piette et al reported 5 patients treated with IVIG (dose of 1g/kg/day for 2 consecutive days of each month). In 3 individuals, a complete clinical response was obtained between 3 and 12 weeks after the last infusion of IVIG. However, they registered relapses between 2 and 10 months after the infusion (in one of them they disappeared when the treatment was restarted).82 Because there are just a few cases published in this pathology and the treatment schedule varies according to the different authors, it is not possible to recommend a routine use of IVIG in DLE.
Other Possible Treatments
Other drugs (that have not demonstrated specifically efficacy in the treatment of DLE) have been used successfully in other forms of CLE or in SLE. All of them could be future therapies to be explored in DLE. Also, there are some drugs that have a good response in DLE, but they could produce flares of SLE, so treatment with them is not recommended.
Dapsone
Dapsone is an antibiotic from the sulphonamide group. Its mechanism of action is based on the inhibition of dihydropteroate synthase, a critical enzyme in bacterial development. Its anti-inflammatory properties prompted its wide use in dermatology. There are case reports postulating its effectiveness in several types of cutaneous lupus, including DLE, with a clinical resolution percentage of 55% in 55 patients.83 This drug can produce hematological alterations (such as methemoglobinemia and agranulocytosis), therefore, during treatment, blood count and hepatic activity must be monitored. Due to the possible hemolysis dapsone should not be administered in patients with glucose-6-phoshate dehydrogenase deficiency.
Acitretin
Acitretin is a second-generation retinoid (derived from etretinate) commonly used for psoriasis. Ruzicka et al designed a randomized clinical trial in 20 patients for the treatment of CLE. The authors report excellent results in 15 patients, especially in SCLE (in this subtype 5/6 individuals presented complete resolution after 2–4 weeks of treatment).84
Phenytoin
Phenytoin or diphenylhydantoin is a commonly used anticonvulsant drug that works by blocking voltage-sensitive sodium channels. Rodriguez-Castellanos et al carried out a clinical trial in which 93 patients with DLE were included. The results were very satisfactory, with a 90% clinical resolution (relapse of 15.7% at 6–12 months).85 However, the risk of development of systemic lupus erythematosus due to phenytoin is described, so its use is not recommended in DLE.
Sulfasalazine
Sulfasalazine (SSZ) is a drug of the sulfonamide group with anti-inflammatory effects. It is composed of a combination of sulfapyridine and a compound similar to aspirin (5-aminosalicylic acid). Case reports have investigated the efficacy of sulfasalazine in treating DLE.86 There are some clinical cases published for the treatment of DLE. However, it can also produce drug-induced lupus.
Rituximab
Rituximab is a chimeric monoclonal antibody (murine and human). It is a glycosylated immunoglobulin with activity against the CD20 antigen, located in the surface of lymphocytes. Several clinical cases have investigated its use in SCLE and in SLE patients with cutaneous lesions.87 However, there are no reported cases in DLE. Also, due to the cost of treatment, lack of further studies and possible side effects, its use is only recommended for selected cases.
Anti-IL-6 Antibodies
Interleukin 6 (IL-6) is a glycoprotein secreted by macrophages, T cells, endothelial cells and fibroblasts. Located on chromosome 7, its release is induced by IL-1 and increases in response to TNFα. Therefore, it is essentially a proinflammatory cytokine. Tocilizumab is the first monoclonal antibody with anti-IL-6 activity. An open-label phase 1 demostrated good results in SLE.88 In recent years, another anti-IL-6 monoclonal antibody (with high affinity and specificity) called sirukumab has been developed. Based in SLE results with tocilizumab, a clinical trial was designed to evaluate the pharmacokinetics and safety of sirukumab in 31 patients with CLE (39% DLE) and in 15 patients with SLE. The treatment was well tolerated in both CLE and SLE patients, so this drug could be an alternative to DLE disease.89
Anti-TNF-Alpha Inhibitors
Although experimental analyses have insinuated the theoretical efficacy of anti-TNFα drugs in severe CLE, current research suggests that these treatments may be responsible for flares of the disease. Levine et al reported a patient with persistent DLE exacerbated by adalimumab. In addition, in their review of the literature they found 128 cases in which these drugs could produce drug-induced lupus.90
Current/Upcoming Clinical Trials
There are currently several clinical trials aimed at treating different forms of CLE. These new molecules are mainly directed to the proinflammatory cytokine pathways. Specifically, monoclonal antibodies against IFNα are being investigated for DLE. In this pathway, the AMG 81191 and PD-036032492 molecules have shown changes in biomarkers and signaling pathways, although patients with DLE have not presented clinical improvement.
In addition, a clinical trial with etarnercept was recently been completed in 25 patients; results have not yet been published.
Lastly, from our point of view it would be interesting to investigate the new biological drugs (anti-IL-17 or anti-IL-23 antibodies) employed in other inflammatory cutaneous pathologies such psoriasis.
Conclusion
In conclusion, classic recommendations on photo protection, smoking cessation and topical therapy remain the most evidence-based approaches for the majority of DLE patients. Refractory DLE may benefit from systemic therapy, thereby we propose a therapeutic algorithm based on the strength of recommendations of the multiple treatment options (Table 4). Even if antimalarial drugs are still considered the first-line systemic therapy in non-responder to lifestyle measures and topical treatment, a combination of both systemic and physical therapies might eventually reach better results than antimalarial monotherapy (e.g. HCQ and laser in refractory individual lesions). Further studies are needed to assess the benefits of treatment combination, which we hypothesize would be the better option in refractory DLE.
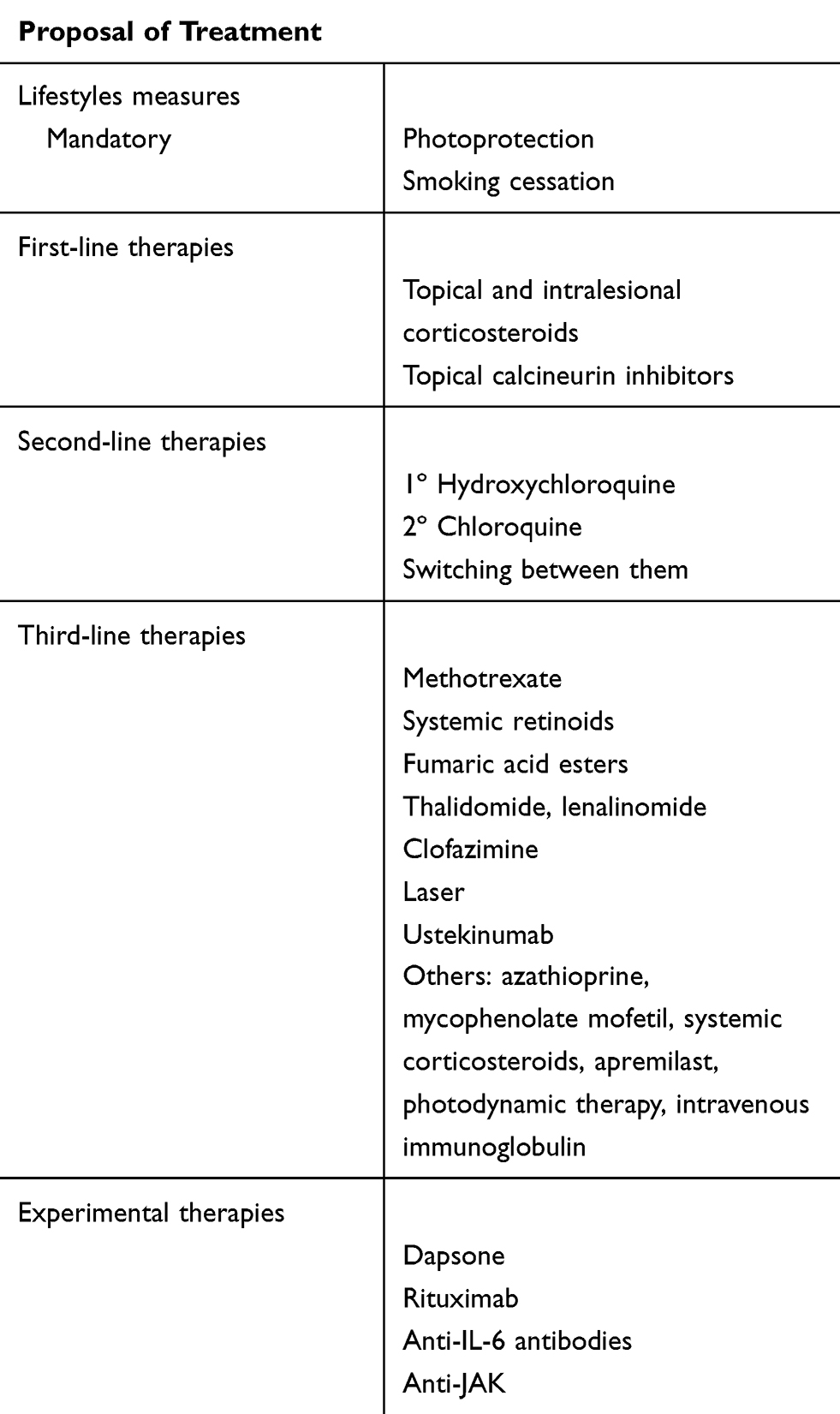 |
Table 4 Proposal Of Treatment Algorithm. Combination Between Medical (topical, Systemic Or Both) And Physical (laser, Photodynamic Therapy) Therapies In Refractory Lesions Should Be Considered |
Disclosure
Dr Alberto Romero-Maté reports personal fees from Celgene Corp., during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Lehmann P, Hölzle E, Kind P, Goerz G, Plewig G. Experimental reproduction of skin lesions in lupus erythematosus by UVA and UVB radiation. J Am Acad Dermatol. 1990;22(2 Pt 1):181–187. doi:10.1016/0190-9622(90)70020-I
2. Kuhn A, Gensch K, Haust M, et al. Photoprotective effects of a broad-spectrum sunscreen in ultraviolet-induced cutaneous lupus erythematosus: a randomized, vehicle-controlled, double-blind study. J Am Acad Dermatol. 2011;64(1):37–48. doi:10.1016/j.jaad.2010.06.028
3. Kuhn A, Ruland V, Bonsmann G. Cutaneous lupus erythematosus: update of therapeutic options part I. J Am Acad Dermatol. 2011;65(6):e179–e193. doi:10.1016/j.jaad.2010.06.018
4. Samotij D, Szczęch J, Werth VP, et al. Disease severity and prophylactic measures in patients with cutaneous lupus erythematosus: results of a worldwide questionnaire-based study. Postepy Dermatol Alergo. 2018;35(2):192–198. doi:10.5114/ada.2018.75242
5. Chasset F, Francès C, Barete S, Amoura Z, Arnaud L. Influence of smoking on the efficacy of antimalarials in cutaneous lupus: a meta-analysis of the literature. J Am Acad Dermatol. 2015;72(4):634–639. doi:10.1016/j.jaad.2014.12.025
6. Wolverton SE. Controversies in dermatologic drug therapy. Dermatol Ther. 2009;22(5):397. doi:10.1111/j.1529-8019.2009.01255.x
7. Jessop S, Whitelaw DA, Delamere FM. Drugs for discoid lupus erythematosus. Cochrane Database Syst Rev. 2009;4:CD002954.
8. Callen JP. Intralesional triamcinolone is effective for discoid lupus erythematosus of the palms and soles. J Rheumatol. 1985;12(3):630–633.
9. Pothinamthong P, Janjumratsang P. A comparative study in efficacy and safety of 0.1% tacrolimus and 0.05% clobetasol propionate ointment in discoid lupus erythematosus by modified cutaneous lupus erythematosus disease area and severity index. J Med Assoc Thai. 2012;95(7):933–940.
10. Kuhn A, Gensch K, Haust M, et al. Efficacy of tacrolimus 0.1% ointment in cutaneous lupus erythematosus: a multicenter, randomized, double-blind, vehicle-controlled trial. J Am Acad Dermatol. 2011;65(1):
11. Barikbin B, Givrad S, Yousefi M, Eskandari F. Pimecrolimus 1% cream versus betamethasone 17-valerate 0.1% cream in the treatment of facial discoid lupus erythematosus: a double-blind, randomized pilot study. Clin Exp Dermatol. 2009;34(7):776–780. doi:10.1111/j.1365-2230.2008.03138.x
12. Milam EC, Ramachandran S, Franks AG. Treatment of scarring alopecia in discoid variant of chronic cutaneous lupus erythematosus with tacrolimus lotion, 0.3. JAMA Dermatol. 2015;151(10):1113–1116. doi:10.1001/jamadermatol.2015.1349
13. Jones DA. The potential immunomodulatory effects of topical retinoids. Dermatol Online J. 2005;11(1):3.
14. Edwards KR, Burke WA. Treatment of localized discoid lupus erythematosus with tazarotene. J Am Acad Dermatol. 1999;41(6):1049–1050. doi:10.1016/s0190-9622(99)70278-1
15. Terao M, Matsui S, Katayama I. Two cases of refractory discoid lupus erythematosus successfully treated with topical tocoretinate. Dermatol Online J. 2011;17(4):15.
16. Jemec GBE, Ullman S, Goodfield M, et al. A randomized controlled trial of R-salbutamol for topical treatment of discoid lupus erythematosus. Br J Dermatol. 2009;161(6):1365–1370. doi:10.1111/j.1365-2133.2009.09330.x
17. Payne JF. A postgraduate lecture on lupus erythematosus. Clin J. 1894;4:223–229.
18. Wozniacka A, Carter A, McCauliffe DP. Antimalarials in cutaneous lupus erythematosus: mechanisms of therapeutic benefit. Lupus. 2002;11:71–81. doi:10.1191/0961203302lu147rr
19. Wahie S, Meggitt SJ. Long-term response to hydroxychloroquine in patients with discoid lupus erythematosus. Br J Dermatol. 2013;169(3):653–659. doi:10.1111/bjd.12378
20. Morand E, McCloud P, Littlejohn G. Continuation of long-term treatment with hydroxychloroquine in systemic lupus erythematosus and rheumatoid arthritis. Ann Rheum Dis. 1992;51:1318–1321. doi:10.1136/ard.51.12.1318
21. Stevens MA, Yeaney GA, Lacomis D. 42-year-old man with discoid lupus and progressive weakness. Brain Pathol. 2009;19:153–156. doi:10.1111/j.1750-3639.2008.00238.x
22. Kobak S, Deveci H. Retinopathy due to antimalarial drugs in patients with connective tissue diseases: are they so innocent? A single center retrospective study. Int J Rheum Dis. 2010;13:e11–e15. doi:10.1111/j.1756-185X.2010.01551.x
23. Tsang-A-Sjoe MW, Bultink IE, Voskuyl AE. Long-term evaluation of antimalarial in a Dutch SLE cohort: intolerance and other reasons for non-use. Clin Exp Rheumatol. 2014;32:95–100.
24. Kalia S, Dutz JP. New concepts in antimalarial use and mode of action in dermatology. Dermatol Ther. 2007;20:160–174. doi:10.1111/dth.2007.20.issue-4
25. Costedoat-Chalumeau N, Dunogue´ B, Leroux G, et al. A critical review of the effects of hydroxychloroquine and chloroquine on the eye. Clin Rev Allergy Immunol. 2015;49:317–326. doi:10.1007/s12016-015-8469-8
26. Marmor MF, Kellner U, Lai TY, Lyons JS, Mieler WF; American Academy of Ophthalmology. Revised recommendations on screening for chloroquine and hydroxychloroquine retinopathy. Ophthalmology. 2011;118:415–422. doi:10.1016/j.ophtha.2010.11.017
27. Clowse ME, Magder L, Witter F, Petri M. Hydroxychloroquine in lupus pregnancy. Arthritis Rheum. 2006;54:3640–3647. doi:10.1002/art.22159
28. Chasset F, Arnaud L, Jachiet M, et al. Changing antimalarial agents after inefficacy or intolerance in patients with cutaneous lupus erythematosus: a multicenter observational study. J Am Acad Dermatol. 2018;78(1):107–114.e1. doi:10.1016/j.jaad.2017.08.045
29. Ashinoff R, Werth VP, Franks AG. Resistant discoid lupus erythematosus of palms and soles: successful treatment with azathioprine. J Am Acad Dermatol. 1988;19(5 Pt 2):961–965. doi:10.1016/s0190-9622(88)70259-5
30. Tsokos GC, Caughman SW, Klippel JH. Successful treatment of generalized discoid skin lesions with azathioprine. Its use in a patient with systemic lupus erythematosus. Arch Dermatol. 1985;121(10):1323–1325.
31. Shehade S. Successful treatment of generalized discoid skin lesions with azathioprine. Arch Dermatol. 1986;122(4):376–377.
32. Callen JP, Spencer LV, Burruss JB, Holtman J. Azathioprine: an effective, corticosteroid-sparing therapy for patients with recalcitrant cutaneous lupus erythematosus or with recalcitrant cutaneous leukocytoclastic vasculitis. Arch Dermatol. 1991;127(4):515–522. doi:10.1001/archderm.127.4.515
33. Garza-Mayers AC, McClurkin M, Smith GP. Review of treatment for discoid lupus erythematosus. Dermatol Ther. 2016;29(4):274–283. doi:10.1111/dth.12358
34. Newton RC, Jorizzo JL, Solomon AR, et al. Mechanism-oriented assessment of isotretinoin in chronic or subacute cutaneous lupus erythematosus. Arch Dermatol. 1986;122(2):170–176.
35. Kuhn A, Patsinakidis N, Luger T. Alitretinoin for cutaneous lupus erythematosus. J Am Acad Dermatol. 2012;67(3):e123–126. doi:10.1016/j.jaad.2011.10.030
36. Winkelmann RR, Kim GK, Del Rosso JQ. Treatment of cutaneous lupus erythematosus: review and assessment of treatment benefits based on oxford centre for evidence-based medicine criteria. J Clin Aesthetic Dermatol. 2013;6(1):27–38.
37. Patel P, Werth V. Cutaneous lupus erythematosus: a review. Dermatol Clin. 2002;20(3):373–85. doi:10.1016/S0733-8635(02)00016-5
38. Bottomley WW, Goodfield MJ. Methotrexate for the treatment of discoid lupus erythematosus. Br J Dermatol. 1995;133(4):655–656. doi:10.1111/j.1365-2133.1995.tb02726.x
39. Wenzel J, Brahler S, Bauer R, Bieber T, Tuting T. Efficacy and safety of methotrexate in recalcitrant cutaneous lupus erythematosus: results of a retrospective study in 43 patients. Br J Dermatol. 2005;153(1):157–162. doi:10.1111/bjd.2005.153.issue-1
40. Kuhn A, Landmann A, Bonsmann G. Fumaric acid esters: a new therapeutic option for skin manifestations in lupus erythematosus? Br J Dermatol. 2017;176(2):301–302. doi:10.1111/bjd.14938
41. Okon LG, Werth VP. Cutaneous lupus erythematosus: diagnosis and treatment. Best Pract Res Clin Rheumatol. 2013;27(3):391–404. doi:10.1016/j.berh.2013.07.008
42. Goyal S, Nousari HC. Treatment of resistant discoid lupus erythematosus of the palms and soles with mycophenolate mofetil. J Am Acad Dermatol. 2001;45(1):142–144. doi:10.1067/mjd.2001.114297
43. Pisoni CN, Obermoser G, Cuadrado MJ, et al. Skin manifestations of systemic lupus erythematosus refractory to multiple treatment modalities: poor results with mycophenolate mofetil. Clin Exp Rheumatol. 2005;23(3):393–396.
44. Frankel HC, Sharon VR, Vleugels RA, Merola JF, Qureshi AA. Lower-dose thalidomide therapy effectively treats cutaneous lupus erythematosus but is limited by neuropathic toxicity. Int J Dermatol. 2013;52(11):1407–1409. doi:10.1111/j.1365-4632.2011.05200.x
45. Duong DJ, Spigel GT, Moxley RT
46. Cuadrado MJ, Karim Y, Sanna G, et al. Thalidomide for the treatment of resistant cutaneous lupus: efficacy and safety of different therapeutic regimens. Am J Med. 2005;118:246–250. doi:10.1016/j.amjmed.2004.04.032
47. Knop J, Bonsmann G, Happle R, et al. Thalidomide in the treatment of sixty cases of chronic discoid lupus erythematosus. Br J Dermatol. 1983;108(4):461–466. doi:10.1111/j.1365-2133.1983.tb04600.x
48. Kindle SA, Wetter DA, Davis MD, Pittelkow MR, Sciallis GF. Lenalidomide treatment of cutaneous lupus erythematosus: the Mayo Clinic experience. Int J Dermatol. 2016;55(8):e431–e439.
49. Shah A, Albrecht J, Bonilla-Martinez Z, et al. Lenalidomide for the treatment of resistant discoid lupus erythematosus. Arch Dermatol. 2009;145:303–306. doi:10.1001/archdermatol.2009.30
50. Braunstein I, Goodman NG, Rosenbach M, et al. Lenalidomide therapy in treatment-refractory cutaneous lupus erythematosus: histologic and circulating leukocyte profile and potential risk of a systemic lupus flare. J Am Acad Dermatol. 2012;66:571–582. doi:10.1016/j.jaad.2011.01.015
51. Cortes-Hernandez J, Avila G, Vilardell-Tarres M, et al. Efficacy and safety of lenalidomide for refractory cutaneous lupus erythematosus. Arthritis Res Ther. 2012;14:R265. doi:10.1186/ar4111
52. Kuhn A, Ochsendorf F, Bonsmann G. Treatment of cutaneous lupus erythematosus. Lupus. 2010;19(9):1125–1136. doi:10.1177/0961203310370345
53. Bezerra ELM, Vilar MJP, Da Trindade Neto PB, Sato EI. Double-blind, randomized, controlled clinical trial of clofazimine compared with chloroquine in patients with systemic lupus erythematosus. Arthritis Rheum. 2005;52(10):3073–3078. doi:10.1002/art.21358
54. De Souza A, Strober BE, Merola JF, Oliver S, Franks AG. Apremilast for discoid lupus erythematosus: results of a phase 2, open-label, single-arm, pilot study. J Drugs Dermatol. 2012;11(10):1224–1226.
55. Tanasescu C, Balanescu E, Balanescu P, et al. IL-17 in cutaneous lupus erythematosus. Eur J Intern Med. 2010;21(3):202–207. doi:10.1016/j.ejim.2010.03.004
56. Chyuan IT, Tsai TH, Chang TH, et al. Ustekinumab treatment in a patient with psoriasis and systemic lupus erythematosus. Lupus. 2015;24(6):650–651. doi:10.1177/0961203314561072
57. Winchester D, Duffin KC, Hansen C. Response to ustekinumab in a patient with both severe psoriasis and hypertrophic cutaneous lupus. Lupus. 2012;21(9):1007–1010. doi:10.1177/0961203312441982
58. Dahl C, Johansen C, Kragballe K, et al. Ustekinumab in the treatment of refractory chronic cutaneous lupus erythematosus: a case report. Acta Derm Venereol. 2013;93(3):368–369.
59. De Souza A, Ali-Shaw T, Strober BE, Franks AG. Successful treatment of subacute lupus erythematosus with ustekinumab. Arch Dermatol. 2011;147(8):896–898. doi:10.1001/archdermatol.2011.185
60. Varada S, Gottlieb AB, Merola JF, Saraiya AR, Tintle SJ. Treatment of coexistent psoriasis and lupus erythematosus. J Am Acad Dermatol. 2015;72(2):253–260. doi:10.1016/j.jaad.2014.10.038
61. Romero-Maté A, García-Donoso C, Hernández-Núñez A, Martínez-Morán C, Moreno-Torres A, Borbujo-Martínez J. Successful treatment of recalcitrant discoid lupus erythematosus with ustekinumab. Dermatol Online J. 2017;23(1).
62. Kahn JS, Deverapalli SC, Rosmarin DM. JAK-TAT signaling pathway inhibition: a role for treatment of discoid lupuserythematosus and dermatomyositis. Int J Dermatol. 2018;57(8):1007–1014. doi:10.1111/ijd.14064
63. Kuhn A, Aberer E, Bata-Csörgo Z, et al. S2k guideline for treatment of cutaneous lupus erythematosus - guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermato-logy and Venereology (EADV). J Eur Acad Dermatol Venereol. 2017;31:389–404. doi:10.1111/jdv.14053
64. Henderson DL, Odom JC. Laser treatment of discoid lupus (case report). Lasers Surg Med. 1986;6:
65. Gupta G, Roberts DT. Pulsed dye laser treatment of subacute cutaneous lupus erythematosus. Clin Exp Dermatol. 1999;24:498–499. doi:10.1046/j.1365-2230.1999.00545.x
66. Nunez M, Boixeda P, Miralles ES, de Misa RF, Ledo A. Pulsed dye laser treatment of telangiectatic chronic erythema of cutaneous lupus erythematosus. ArchDermatol. 1996;132:354–355.
67. Raulin C, Schmidt C, Hellwig S. Cutaneous lupus erythematosus-treatment with pulsed dye laser. Br J Dermatol. 1999;141:1046–1050. doi:10.1046/j.1365-2133.1999.03203.x
68. Pindado-Ortega C, Alegre-Sánchez A, Pérez-García B, Boixeda P. Reply to: S2k guideline for treatment of cutaneous lupus erythematosus-guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV).J Eur Acad Dermatol Venereol. 2019;33(2):e70–e71. doi:10.1111/jdv.15209
69. Kuhn A, Becker-Wegerich PM, Ruzicka T, Lehmann P. Successful treatment of discoid lupus erythematosus with argon laser. Dermatology. 2000;201:175–177. doi:10.1159/000018467
70. Tremblay JF, Carey W. Atrophic facial scars secondary to discoid lupus erythematous: treatment using the Erbium: YAG laser. Dermatol Surg. 2001;27:675–677.
71. Baniandres O, Boixeda P, Belmar P, Perez A. Treatment of lupus erythematosus with pulsed dye laser. Lasers Surg Med. 2003;32:327–330. doi:10.1002/lsm.10169
72. Erceg A, Bovenschen HJ, van de Kerkhof PC, de Jong EM, Seyger MM. Efficacy and safety of pulsed dye laser treatment for cutaneous discoid lupus erythematosus. J Am Acad Dermatol. 2009;60:626–632. doi:10.1016/j.jaad.2008.11.904
73. Ekbäck MP, Troilius A. Laser therapy for refractory discoid lupus erythematosus when everything else has failed. J Cosmet Laser Ther. 2013;15(5):260–265.
74. Zachariae H, Bjerring P, Cramers M. Argon laser treatment of cutaneous vascular lesions in connective tissue diseases. Acta Derm Venereol. 1988;68:179–182.
75. Byun YS, Son JH, Cho YS, et al. Intense Pulsed Light and Q-Switched 1,064-nm Neodymium-Doped Yttrium Aluminum Garnet Laser Treatment for the Scarring Lesion of Discoid Lupus Erythematosus. Ann Dermatol. 2017;29(3):331–333. doi:10.5021/ad.2017.29.3.331
76. Debu A, Girard C, Bessis D. Discoid lupus erythematosus successfully treated by photodynamic therapy. Br J Dermatol. 2015;172(3):821–822. doi:10.1111/bjd.13407
77. Fernández-Guarino M, Pérez-García B, Harto A, Jaén P. Discoid lupus erythematosus: good response to treatment with photodynamic therapy. J Eur Acad Dermatol Venereol. 2008;22(9):1142–1143. doi:10.1111/j.1468-3083.2007.02560.x
78. Romero-Maté A, Castaño-Suárez E, García-Donoso C, Martínez-Morán C, Meseguer-Yebra C, Borbujo J. Unsuccessful treatment of recalcitrant cutaneous discoid lupus erythematosus with photodynamic therapy. Photodermatol Photoimmunol Photomed. 2010;26(3):156–158. doi:10.1111/j.1600-0781.2010.00506.x
79. Tenti S, Fabbroni M, Mancini V, Russo F, Galeazzi M, Fioravanti A. Intravenous Immunoglobulins as a new opportunity to treat discoid lupus erythematosus: a case report and review of the literature. Autoimmun Rev. 2018;17(8):791–795. doi:10.1016/j.autrev.2018.02.010
80. Gelfand EW. Intravenous immune globulin in autoimmune and inflammatory diseases. N Engl J Med. 2013;368(8):777.
81. Basyreva LY, Brodsky IB, Gusev AA, et al. The effect of Intravenous Immunoglobulin (IVIG) on\textit{ex vivo} activation of human leukocytes. Hum Antibodies. 2016;24(3–4):39–44. doi:10.3233/HAB-160293
82. Piette J, Frances C, Roy S, Papo T, Godeau P. High-dose Immuno-globulins in the Treatment of Refractory Cutaneous Lupus-erythematosus-open Trial in 5 Cases. In Philadelphia, PA: Lippincott-Raven; 1995:908.
83. Chang AY, Werth VP. Treatment of cutaneous lupus. Curr Rheumatol Rep. 2011;13(4):300. doi:10.1007/s11926-011-0180-z
84. Ruzicka T, Meurer M, Bieber T. Efficiency of acitretin in the treatment of cutaneous lupus erythematosus. Arch Dermatol. 1988;124(6):897–902.
85. Rodriguez-Castellanos MA, Rubio JB, Gomez JFB, Mendoza AG. Phenytoin in the treatment of discoid lupus erythematosus. Arch Dermatol. 1995;131(5):620–621. doi:10.1001/archderm.131.5.620b
86. Delaporte E, Catteau B, Sabbagh N, et al. Treatment of discoid lupus erythematosus with sulfasalazine: 11 cases. Ann Dermatol Venereol. 1997;124(2)151–156.
87. Kuhn A, Ruland V, Bonsmann G. Cutaneous lupus erythematosus: update of therapeutic options: part II. J Am Acad Dermatol. 2011;65(6):e195–e213. doi:10.1016/j.jaad.2010.06.017
88. Makol A, Gibson LE, Michet CJ. Successful use of interleukin 6 antagonist tocilizumab in a patient with refractory cutaneous lupus and urticarial vasculitis. JCR J Clin Rheumatol. 2012;18(2):92–95. doi:10.1097/RHU.0b013e31823ecd73
89. Szepietowski JC, Nilganuwong S, Wozniacka A, et al. Phase I, randomized, double‐blind, placebo‐controlled, multiple intravenous, dose‐ascending study of sirukumab in cutaneous or systemic lupus erythematosus. Arthritis Rheum. 2013;65(10):2661–2671. doi:10.1002/art.38091
90. Levine D, Switlyk SA, Gottlieb A. Cutaneous lupus erythematosus and anti-TNF-alpha therapy: a case report with review of the literature. J Drugs Dermatol. 2010;9(10):1283–1287.
91. Werth VP, Fiorentino D, Cohen S, Fivenson D, Hansen C, Zoog S. To evaluate the safety, tolerability, pharmacokinetics, pharmacodynamics, and clinical efficacy of AMG 811 (anti-IFN-gamma) in subjects with discoid lupus erythematosus. Arthritis Rheum. 2013;65(Suppl 10):1608.
92. Masek-Hammerman K, Peeva E, Ahmad A, et al. Monoclonal antibody against macrophage colony-stimulating factor suppresses circulating monocytes and tissue macrophage function but does not alter cell infiltration/activation in cutaneous lesions or clinical outcomes in patients with cutaneous lupus erythematosus. Clin Exp Immunol. 2016;183:258–270.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.