Back to Journals » Research Reports in Clinical Cardiology » Volume 5
Current concepts in the management of cardiogenic shock
Authors Trohman R
Received 7 October 2013
Accepted for publication 6 December 2013
Published 5 July 2014 Volume 2014:5 Pages 145—154
DOI https://doi.org/10.2147/RRCC.S39094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Video abstract presented by Richard G Trohman.
Views: 1618
Richard G Trohman
Cardiology, Electrophysiology, Arrhythmia and Pacemaker Service, Department of Medicine, Rush University Medical Center, Chicago, IL, USA
Abstract: Cardiogenic shock most commonly results from myocardial infarction and is associated with mortality rates ranging from 40% to 50%. Early revascularization improves mortality. Mechanical complications of myocardial infarction require surgical intervention. Medical, device and mechanical therapies may improve hemodynamics, but are not associated with improvement in short term survival. Massive pulmonary embolism may also result in cardiogenic shock. Prevention of fatal RV failure requires treatment that will result in rapid restoration of flow through the occluded pulmonary arteries. This review summarizes these and other clinical entities that may result in cardiogenic shock with an emphasis placed on a guideline-based approach to their management.
Keywords: myocardial infarction, revascularization, mechanical complications, surgery, pulmonary embolism
Introduction
Cardiogenic shock (CS) is characterized by tissue hypoperfusion resulting from cardiac dysfunction. The hemodynamic criteria for CS include a systolic blood pressure <90 mmHg, a cardiac index <2.2 L/min/m2, a pulmonary capillary wedge pressure >18 mmHg or a right ventricular (RV) end diastolic pressure >10–15 mmHg. Although myocardial infarction (MI) with left ventricular (LV) failure remains the most common etiology, any acute cause of severe LV or RV dysfunction may lead to cardiogenic shock.1–3
Advanced age, anterior MI, hypertension, diabetes mellitus, multivessel coronary disease, prior MI, systolic BP <120 mmHg, heart rate >90 bpm, heart failure present on admission, ST-elevation MI (STEMI), and left bundle branch block on the electrocardiogram are all predictors of CS complicating acute MI.4
Acute myopericarditis, Takotsubo cardiomyopathy, and hypertrophic cardiomyopathy may present with ST elevation, troponin elevation, and shock, in the absence of hemodynamically significant coronary artery disease. Acute valvular regurgitation, caused by endocarditis or chordal rupture, may also lead to CS. These and other mechanical complications, including ventricular septal rupture, contained free-wall rupture, and papillary muscle rupture, should be suspected when CS complicates a nonanterior MI. Aortic dissection may result in severe valvular regurgitation or MI (usually involving the right coronary artery), resulting in CS. CS may also result from a massive pulmonary embolism or cardiac tamponade.3
CS is life-threatening, with mortality rates ranging from 40% to 50%. Nevertheless, prompt aggressive treatment can result in full recovery.3,5
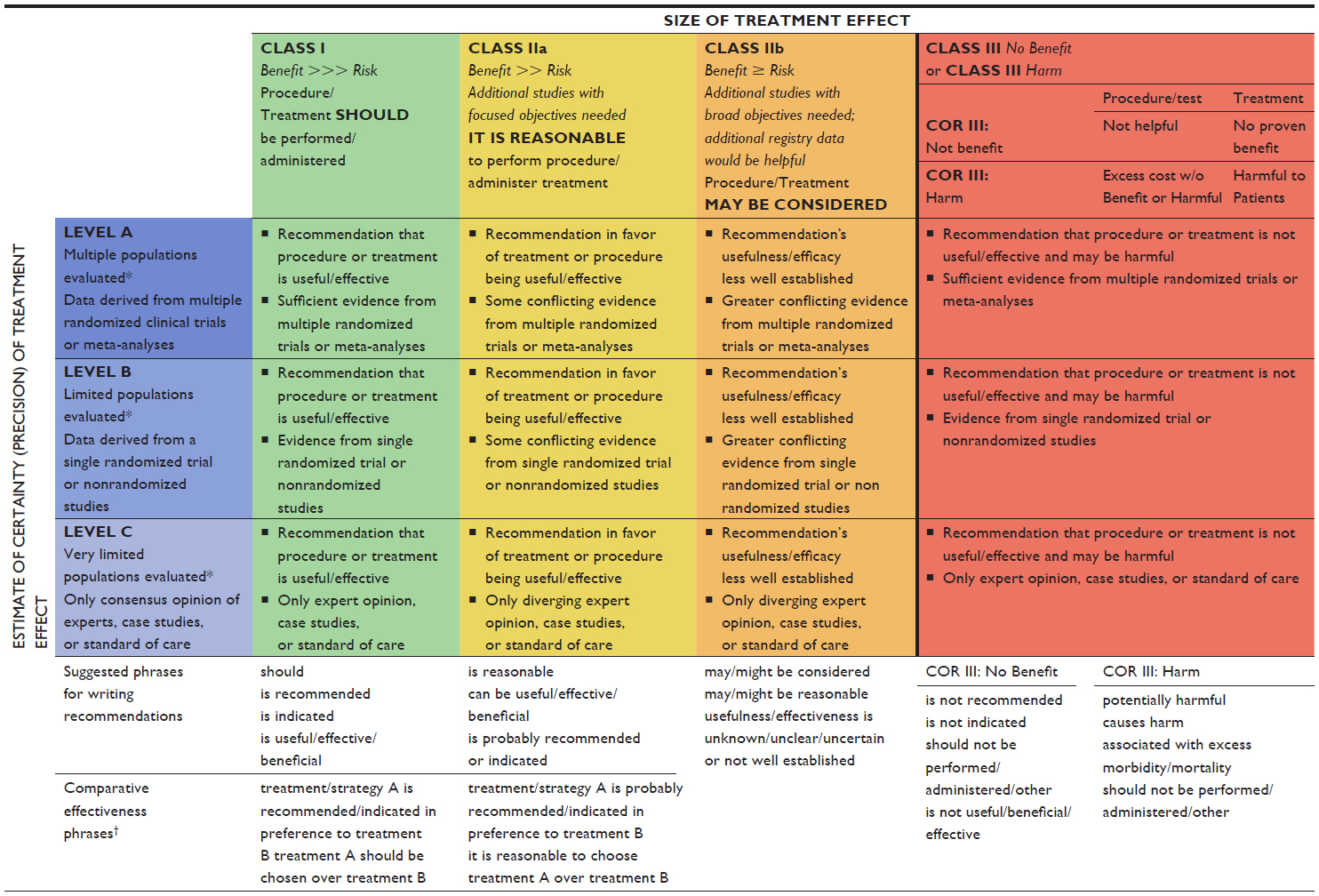
In this review, the various causes of CS are discussed, and the current treatment guidelines are elucidated – readers are encouraged to consult Table S1 for an explanation of indication classes and levels of evidence, upon which the guidelines are based.
Management of cardiogenic shock without mechanical complications of acute myocardial infarction
Pharmacotherapy for CS has primarily consisted of inotropic and vasopressor support. Unfortunately, use of these agents may increase myocardial oxygen consumption, result in arrhythmogenesis, or decrease splanchnic and renal blood flow.1
Medical therapy
Medical management of CS generally begins with a vasopressor. The administration of dobutamine or milrinone (inotropic agents that also produce vasodilation) does not reverse the hypotension associated with CS.
There is insufficient evidence to make a firm recommendation for the initial vasopressor of choice in patients with CS. Although dopamine is frequently chosen before norepinephrine, there is some evidence to suggest the latter is a better first option. In a large trial of patients with shock of various etiologies, there was a trend toward a higher death rate at 28 days with dopamine, and there were significantly more arrhythmias (predominantly atrial fibrillation).6,7
Hypothermia protects against neurological damage and death after resuscitation from cardiac arrest.8 The induction of mild to moderate hypothermia has also been suggested as adjunctive therapy when CS complicates resuscitated cardiac arrest. Therapeutic hypothermia has physiologic effects that could be beneficial to patients with post-MI shock. These include reduction in heart rate, vasoconstriction (requiring less exogenous pressor support), and possible increases in inotropy. Some authors have suggested that hypothermia could reduce oxygen consumption, whereas others believe the opposite to be true.9,10 The 2-year results from the Paris Sudden Death Expertise Centre Registry (presented at the 2013 European Society of Cardiology Congress) revealed that out-of-hospital cardiac arrest survival was just 7%. In this study, therapeutic hypothermia and early coronary reperfusion (see below) were significantly associated with survival (P<0.001), but these procedures were used in just 58% of patients admitted to hospital.11,12 Additional study is needed to clarify the role of therapeutic hypothermia in CS.
Mechanical- and device-based therapy
Mechanical options for drug refractory CS have included intra-aortic balloon pump (IABP) counterpulsation and percutaneous LV assist devices (LVADs), such as the TandemHeart® percutaneous LVAD system (Cardiac Assist, Inc, Pittsburgh, PA, USA), the Impella® LP2.5 and the (more powerful) Impella CP™ (Abiomed Europe GmbH, Aachen, Germany). The use of an IABP, in addition to assisting hemodynamic management, may be required to stabilize the patient enough to permit angiography and revascularization (a class IIa indication),6 as described below. The main limitation of IABP counterpulsation is the requirement of a residual level of LV function. In contrast, percutaneous LVADs provide active circulatory support. Percutaneous LVADs may rapidly reverse the hemodynamic compromise seen in patients with CS that is refractory to IABP and vasopressor support. Although percutaneous LVADs provide superior hemodynamic support compared with IABP counterpulsation, use of these devices has not translated into improved 30-day survival.15 The complications associated with percutaneous LVADs include arterial damage, limb ischemia, sepsis, coagulopathy/bleeding, and stroke. Patients treated with a percutaneous LVAD have a higher incidence of ischemic legs and device-related bleeding compared with those treated with IABP counterpulsation.1,6,13–16
Extracorporeal membrane oxygenation (ECMO) also offers temporary hemodynamic support for patients with CS refractory to high-dose inotropic and IABP therapy. There are two types of ECMO, venovenous (VV) and venoarterial (VA). Only VA ECMO provides hemodynamic support. One group of investigators reported that ECMO rescued 40% of patients with otherwise fatal CS.17 Survival rates of 20% to 43% have been reported among patients who received VA ECMO for cardiac arrest, severe CS, or failure to wean from cardiopulmonary bypass after cardiac surgery. The available evidence suggests that ECMO is more effective for pulmonary failure.18,19
Bleeding occurs in 30% to 40% of ECMO recipients.19 If it occurs, pulmonary or intracranial hemorrhage may be life threatening or fatal. Careful management of anticoagulation, prevention of renal failure, and prompt correction of thrombocytopenia may decrease the risk of intracranial hemorrhage in adults on ECMO. Although infrequent, systemic thromboembolism due to stasis and thrombus formation within the heart or extracorporeal circuit can also be catastrophic. A variety of complications can occur during cannulation, including vessel perforation, arterial dissection, distal ischemia, and incorrect cannula location. VA ECMO preferentially perfuses the lower extremities and the abdominal viscera. To avoid cerebral or cardiac hypoxia, upper extremity oxygen saturation must be carefully monitored.19,20
Percutaneous LVADs and ECMO may be used as “bridges” to long-term ventricular assist devices or to cardiac transplantation. In addition, they may be used in “bridge to bridge” therapy, where transfer to a long-term ventricular assist device ultimately leads to cardiac transplantation.21
The TandemHeart and the Impella percutaneous LVADs are about ten times as costly as an IABP catheter. The reliability of percutaneous LVADs remains to be confirmed. The cost of ECMO treatment is approximately £45,000 (more than US$70,000) per recipient. At the current time, it is premature to declare that an evidenced-based approach to CS demands the routine use of these devices.15,22,23
Eitel et al5 recently described the feasibility of temporary LV stimulation in patients with refractory CS, left bundle branch-type QRS morphologies, and asynchronous LV contraction. They reported that temporary LV pacing resulted in clinical improvement in about two-thirds of patients. The responders tended to have wider intrinsic QRS complexes than did the nonresponders. The reduction in mortality among the responders (30% vs 80% in the nonresponders) was impressive despite a failure to reach statistical significance.1 Further study of the clinical benefit of this intervention seems warranted.
Evolving clinical guidelines
The 2004 American College of Cardiology (ACC)/American Heart Association (AHA) practice guidelines emphasized the importance of IABP counterpulsation (class I, level of evidence: B) and early revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass grafting [CABG]), for patients under the age of 75 with STEMI and CS that developed within 36 hours and who can be revascularized within 18 hours of shock onset (class I, level of evidence: A) These recommendations were largely driven by the results of the Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial, in which early revascularization did not improve 30-day mortality but resulted in significant mortality reduction at 6 and 12 months post MI.3,24,25
The Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO-I) database identified predictors of 30-day survival for patients with CS complicating STEMI who received initial fibrinolysis. These included: 1) increasing age (odds ratio 1.49 for every 10-year increase); 2) prior MI; 3) altered sensorium and cold, clammy skin; and 4) oliguria. A variety of hemodynamic parameters correlate with mortality in CS. The cardiac power index (mean arterial pressure × cardiac output/[451 × body surface area in m2]) is the strongest predictor.6,26,27
The 2007 ACC/AHA STEMI Focused Update recommended an immediate invasive strategy in patients who have received fibrinolysis and have CS. Coronary angiography with intent to perform revascularization (after fibrinolysis) was recommended as a class I indication (level of evidence: B) for CS (and severe heart failure) patients less than age 75 who were suitable revascularization candidates and was also suggested to be reasonable for suitable patients over the age of 75 (class IIa indication, level of evidence: B).28
Two trials, the Combined Abciximab REteplase Stent Study in Acute Myocardial Infarction (CARESS in AMI) and the Trial of Routine ANgioplasty and Stenting after Fibrinolysis to Enhance Reperfusion in Acute Myocardial Infarction (TRANSFER-AMI), demonstrated that after fibrinolytic therapy, prompt transfer to a PCI-capable hospital resulted in better outcomes than waiting to assess the results of fibrinolysis in a non-PCI-capable facility.29,30 Therefore, the 2009 ACC/AHA STEMI Focused Update recommended that each community develop prehospital identification and transfer protocols (class I indication, level of evidence: C) for high-risk patients, such as those who arrive in CS.31
The 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction states unequivocally (class I, level of evidence: B) that emergent revascularization should be performed after STEMI, in patients with CS that develops (irrespective of the time delay) after initial presentation. Advanced age alone was not deemed a contraindication to emergency revascularization; however, individualized clinical judgment, based on comorbidities, functional status, and patient directives, was considered crucial in the elderly.32 Despite the 2004 practice guidelines, the current evidence does not support the routine use of an IABP in most patients with acute myocardial infarction complicated by CS in whom primary PCI has been attempted or performed or in whom fibrinolytic therapy has been administered.6,32
RV infarction, most often due to a proximal occlusion of the right coronary artery, complicates about one-third of inferior STEMIs and is associated with a higher mortality risk. A clinical triad of hypotension, elevated jugular venous pressure, and clear lung fields characterizes RV infarction. The presence of a 1 mm ST elevation in lead V1 and in right precordial lead V4R is the most sensitive electrocardiogram (ECG) marker of RV injury. Treatment includes maintaining the RV preload, reducing the RV afterload, providing inotropic support when needed, and immediate reperfusion. Restoration of atrioventricular synchrony or cardioversion from atrial fibrillation may also be required.32
CS may also occur in the setting of non-STEMI (NSTEMI). In the SHOCK trial, ~20% of all CS was associated with NSTEMI. The GUSTO and Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin (PURSUIT) studies found that up to 5% of the NSTEMI patients had CS, and their mortality exceeded 60%. The 2007 Focused Update of the ACC/AHA/The Society for Cardiac Angiography and Interventions (SCAI) 2005 Guideline Update for Percutaneous Coronary Intervention recommended an early invasive strategy (ie, diagnostic angiography with intent to perform revascularization) for unstable angina/NSTEMI patients (without serious comorbidities or contraindications to such procedures) who have refractory angina or hemodynamic or electrical instability.33–36
Management of cardiogenic shock from mechanical complications of acute myocardial infarction
Most mechanical complications of MI occur in the first 24 hours, and the remainder present within the first week32 Diagnosis can usually be established via transthoracic echocardiography. The following discussion focuses briefly on the management of these complications.
Acute severe mitral regurgitation after STEMI is most often due to posterior papillary muscle rupture. Mitral valve replacement, rather than repair, is usually required. Emergency mitral valve replacement is associated with a 20% mortality rate. Survival and ventricular function are improved with surgery compared with medical therapy. Postoperative 5-year survival rates average 60% to 70%.32
Ventricular septal rupture occurs most often within the first 24 hours, in patients treated with fibrinolytic therapy. An emergency surgical repair is necessary. Surgical mortality rates are high, especially among patients with CS, ranging from 20% to 87%.32 The mortality risk is higher in patients with inferior-basal defects compared with those with anterior-apical defects. Temporizing medical treatment, stabilization, and an IABP (when necessary) should be attempted for acute mitral regurgitation and ventricular septal rupture.32 Percutaneous transcatheter closure has been reported. Employment of devices with a diameter greater than the ventricular septal defect has been associated with relatively good outcomes.3,32,37
LV free-wall rupture is typified by recurrent chest pain and ST-T wave changes. A rapid progression to hemodynamic collapse, electromechanical dissociation, and death is characteristic. Emergency surgery should be considered for pseudoaneurysm formation with contained rupture and tamponade. Most of the case series describing patients reaching the operating room have been small, with mortality rates approaching 60%.32
Other causes of cardiogenic shock
Cardiac tamponade is typified by the accumulation of fluid under pressure in the pericardial space. As the effusion increases, movement of the parietal pericardium decreases. Tamponade occurs when increased intrapericardial pressure compresses all the cardiac chambers to the point of compromising systemic venous return to the right atrium. The increased intrapericardial pressure reduces the myocardial transmural pressure, the cardiac chambers become smaller, and have reduced diastolic compliance, resulting in a decline in cardiac output and blood pressure. Despite tamponade, much of the inspiratory decrease in thoracic pressure is transmitted through the pericardium to the right heart, resulting in an increase in systemic venous return with inspiration and RV distention. However, once the intrapericardial pressure is high enough, the RV free wall is prevented from expanding. Expansion is limited to the interventricular septum, and the RV bulges into the LV. This bulging results in decreased LV compliance and reduced LV filling during inspiration. Pericardiocentesis is life saving in cardiac tamponade (class I indication, level of evidence B). Surgical pericardiectomy (often referred to as a “window”) is an alternate approach to fluid evacuation.38,39
The two most common causes of acute aortic regurgitation (AR) in a native aortic valve are endocarditis and aortic dissection.43 Acute thoracic aortic dissection involving the ascending aorta should be evaluated for emergent surgical repair because of the high risk of associated life-threatening complications, such as rupture or AR (class I, level of evidence: B).42 The acute onset of severe AR is usually a medical emergency, due to the inability of the LV to adapt quickly to the rapid increase in end-diastolic volume caused by regurgitant blood. If not surgically corrected, acute severe AR commonly results in CS. The treatment for acute severe AR is emergency aortic valve repair or replacement. If there is any delay in surgery, temporary stabilization may be attempted using intravenous vasodilators, such as nitroprusside, and possibly inotropic agents, such as dopamine or dobutamine, to decrease LV end-diastolic pressure and enhance forward flow. IABP counterpulsation is contraindicated40,43 because balloon inflation in diastole will worsen the severity of AR. Similarly, LVADs are not helpful because retrograde filling of the LV occurs across the incompetent valve, without improvement in forward cardiac output or LV diastolic pressure.40–43
Acute massive pulmonary embolism (PE) has been defined as the obstruction of blood flow to a lobe or multiple segments of the lung, or unstable hemodynamics (failure to maintain blood pressure without supportive measures). Acute massive PE is characterized by sustained hypotension (systolic blood pressure <90 mmHg for at least 15 minutes) or hypotension requiring inotropic support (excluding causes such as arrhythmia, hypovolemia, sepsis, or LV dysfunction, or persistent profound bradycardia [heart rate <40 bpm with signs or symptoms of shock]). Prevention of fatal RV failure in high-risk patients, characterized by shock or hypotension, requires treatment that will result in rapid restoration of flow through the occluded pulmonary arteries.44 Therapeutic anticoagulation, with subcutaneous low-molecular-weight heparin; intravenous or subcutaneous unfractionated heparin with monitoring; unmonitored weight-based subcutaneous unfractionated heparin; or subcutaneous fondaparinux, should be given to patients with objectively confirmed PE and no contraindications to anticoagulation (class I; level of evidence A).45 Thrombolysis may be contemplated to treat massive pulmonary emboli (class IIa; level of evidence B).45 Patients treated with fibrinolytic agents have faster restoration of lung perfusion. The data suggest that heparin plus fibrinolysis yields a significant favorable change in RV systolic pressure and pulmonary arterial pressure between the time of diagnosis and follow up compared with heparin alone. A meta-analysis of randomized controlled trials suggested that the combination of fibrinolysis followed by heparin and/or warfarin for massive PE results in a significant reduction in recurrent PE or death when compared with heparin alone.46 Thrombus fragmentation achieved by manual rotation of a pigtail catheter or with peripheral balloon angioplasty catheters may result in macroembolization, causing hemodynamic deterioration if fragments from a large nonobstructive thrombus embolize.47 Emergent surgical or catheter-based embolectomy with cardiopulmonary bypass may be an effective strategy for managing patients with massive PE or submassive PE with RV dysfunction, when thrombolysis is contraindicated (class IIa; level of evidence C).45
The 2008 European guidelines for the management of high-risk pulmonary emboli are somewhat different from the US guidelines described above. In the European guidelines, thrombolysis is considered first-line therapy (class I; level of evidence A) in patients with PE presenting with CS and/or persistent arterial hypotension. Surgical pulmonary embolectomy is recommended as a therapeutic alternative in patients with high-risk PE in whom thrombolysis is absolutely contraindicated or has failed (class I; level of evidence C). Catheter embolectomy or fragmentation of the proximal pulmonary arterial clots is considered an alternative to surgical treatment in high-risk patients when thrombolysis is absolutely contraindicated or has failed (class IIb; level of evidence C).48
Some experts have proposed that interventions that employ a dual pharmacological and mechanical approach to blood clot dispersion may offer the best opportunity for clot lysis. A meta-analysis of 594 patients in 35 studies suggested that hemodynamic stability, resolution of hypoxemia, and survival can be achieved in 86% of cases. Pooled success rates were higher when at least 80% of the participants received local thrombolytic therapy during their procedure. The authors suggested that catheter-directed therapy should be considered as a first-line treatment for patients with massive PE, at experienced centers.49,50
Case reports and small case series have suggested that VA ECMO may be a useful adjunct in the treatment of refractory massive PE. Mortality remains high and, given the significant cost of ECMO, more data are needed to ascertain the true value of this intervention.51–55
Takotsubo cardiomyopathy (also known as stress cardiomyopathy or broken-heart syndrome) is characterized by reversible LV apical ballooning, in the absence of obstructive coronary artery disease. The Japanese phrase “tako-tsubo” translates to “fishing pot for trapping octopus,” and the left ventricle of Takotsubo cardiomyopathy patients approximates that shape. Although the precise mechanism of this disorder remains unknown, enhanced sympathetic activity appears to play a pivotal role in its pathogenesis.56
Takotsubo cardiomyopathy classically presents in elderly or postmenopausal females in response to acute emotional stress or an acute medical illness. Resolution of the LV dysfunction prior to hospital discharge is typical. Nevertheless, the clinical spectrum is heterogeneous, with approximately one-third of the victims being male, ≤50 years old, lacking a stress trigger, or having an in-hospital death, clinical (nonfatal) recurrence, embolic stroke, or delayed normalization of LV function.56,57
Although transient inotropic support may be required, frank CS appears to be rare. In a series of 136 patients, one elderly female died from CS despite support with inotropic agents.56
Summary and conclusion
CS most commonly results from myocardial infarction and is associated with mortality rates ranging from 40% to 50%. The prognosis appears to correlate with age, clinical signs, and hemodynamic parameters. Early revascularization (percutaneous or surgical) improves mortality. Medical and mechanical support is commonly required to stabilize the patient for revascularization. Temporary LV pacing may be a useful adjunct in patients with left bundle branch-type QRS morphologies.
The mechanical complications of MI resulting in CS usually occur in the first 24 hours and require surgical intervention. Mortality rates range from 20% to nearly 90%, depending on the type of complication.
Acute thoracic aortic dissection involving the ascending aorta should be evaluated for emergent surgical repair. Without surgical correction, acute severe AR commonly results in life-threatening CS.
Pericardiocentesis is life saving in cardiac tamponade. The combination of heparin and fibrinolysis to treat massive pulmonary embolism results in a significant reduction in recurrent emboli or death compared with heparin alone. Emergent surgical or catheter-based embolectomy may be effective for patients with massive or submassive pulmonary emboli and RV dysfunction, when thrombolysis is contraindicated.
Takotsubo cardiomyopathy may mimic acute MI and require hemodynamic support. Complete recovery of myocardial function is the rule rather than the exception.
CS remains a difficult clinical entity, often associated with a grim prognosis. Its prompt recognition is pivotal because timely therapy may result in complete functional recovery. Closing the gaps in our knowledge base and expansion of our treatment armamentarium will be needed to improve long-term survival rates.
Disclosure
The author reports no conflict of interest in this work.
References
Trohman RG. Temporary left ventricular resynchronization therapy in cardiogenic shock: a new pacing paradigm to fight an old foe? Heart Rhythm. 2013;10(1):53–54. | |
Hollenberg SM, Kavinsky CJ, Parrillo JE. Cardiogenic shock. Ann Intern Med. 1999;131(1):47–59. | |
Reynolds HR, Hochman JS. Cardiogenic shock: current concepts and improving outcomes. Circulation. 2008;117(5):686–697. | |
uptodate.com [homepage on the Internet]. Clinical manifestations and diagnosis of cardiogenic shock in acute myocardial infarction. UpToDate, Inc (Wolters Kluwer); 2103 [updated October 22, 2012; cited October 2, 2013]. Available from: http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-cardiogenic-shock-in-acute-myocardial-infarction?source=see_link. Accessed December 7, 2013. | |
Eitel C, Gaspar T, Bode K, et al. Temporary left ventricular stimulation in patients with refractory cardiogenic shock and asynchronous left ventricular contraction: a safety and feasibility study. Heart Rhythm. 2013;10(1):46–52. | |
uptodate.com [homepage on the Internet]. Prognosis and treatment of cardiogenic shock complicating acute myocardial infarction. UpToDate, Inc (Wolters Kluwer); 2103 [updated September 9, 2013; cited October 2, 2013]. Available from: http://www.uptodate.com/contents/prognosis-and-treatment-of-cardiogenic-shock-complicating-acute-myocardial-infarction?source=see_link Accessed December 7, 2013. | |
De Backer D, Biston P, Devriendt J, et al; SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362(9):779–789. | |
Schmidt-Schweda S, Ohler A, Post H, Pieske B. Moderate hypothermia for severe cardiogenic shock (COOL Shock Study I and II). Resuscitation. 2013;84(3):319–325. | |
Zobel C, Adler C, Kranz A, et al. Mild therapeutic hypothermia in cardiogenic shock syndrome. Crit Care Med. 2012;40(6):1715–1723. | |
Stegman BM, Newby LK, Hochman JS, Ohman EM. Post-myocardial infarction cardiogenic shock is a systemic illness in need of systemic treatment: is therapeutic hypothermia one possibility? J Am Coll Cardiol. 2012;59(7):644–647. | |
Taylor J. Highlights from European Society of Cardiology Congress 2013. Eur Heart J. 2013;34(39):3009–3013. | |
Bougouin W, Lamhaut L, Marijon E, et al; Paris sudden Death Expertise Center. Incidence, characteristics and outcome of sudden cardiac death in France [abstract]. Eur Heart J. 2013;34(Suppl 1):328. | |
Kar B, Adkins LE, Civitello AB, et al. Clinical experience with the TandemHeart percutaneous ventricular assist device. Tex Heart Inst J. 2006;33(2):111–115. | |
Seyfarth M, Sibbing D, Bauer I, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol. 2008;52(19):1584–1588. | |
Cheng JM, den Uil CA, Hoeks SE, et al. Percutaneous left ventricular assist devices vs intra-aortic balloon pump counterpulsation for treatment of cardiogenic shock: a meta-analysis of controlled trials. Eur Heart J. 2009;30(17):2102–2108. | |
Kar B, Gregoric ID, Basra SS, Idelchik GM, Loyalka P. The percutaneous ventricular assist device in severe refractory cardiogenic shock. J Am Coll Cardiol. 2011;57(6):688–696. | |
Combes A, Leprince P, Luyt CE, et al. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36(5):1404–1411. | |
Hsu PS, Chen JL, Hong GJ, et al. Extracorporeal membrane oxygenation for refractory cardiogenic shock after cardiac surgery: predictors of early mortality and outcome from 51 adult patients. Eur J Cardiothorac Surg. 2010;37(2):328–333. | |
uptodate.com [homepage on the Internet]. Extracorporeal membrane oxygenation (ECMO) in adults. UpToDate, Inc (Wolters Kluwer); 2103 [updated October 2, 2013; cited October 26, 2013]. Available from: http://www.uptodate.com/contents/extracorporeal-membrane-oxygenation-ecmo-in-adults. Accessed December 7, 2013. | |
Kasirajan V, Smedira NG, McCarthy JF, Casselman F, Boparai N, McCarthy PM. Risk factors for intracranial hemorrhage in adults on extracorporeal membrane oxygenation. Eur J Cardiothorac Surg. 1999;15(4):508–514. | |
Hoefer D, Ruttmann E, Poelzl G, et al. Outcome evaluation of the bridge-to-bridge concept in patients with cardiogenic shock. Ann Thorac Surg. 2006;82(1):28–33. | |
Sedgwick C, Gati S, Sharma S. Extra corporeal membrane oxygenation (ECMO) devices in all heart attack centres in the UK? Br J Cardiol. 2012;19:102–103. | |
Desai NR, Bhatt DL. Evaluating percutaneous support for cardiogenic shock: data shock and sticker shock. Eur Heart J. 2009;30(17):2073–2075. | |
Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction; A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44(3):E1–E211. | |
Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341(9):625–634. | |
Fincke R, Hochman JS, Lowe AM, et al; SHOCK Investigators. Cardiac power is the strongest hemodynamic correlate of mortality in cardiogenic shock: a report from the SHOCK trial registry. J Am Coll Cardiol. 2004;44(2):340–348. | |
Hasdai D, Holmes DR, Califf RM, et al. Cardiogenic shock complicating acute myocardial infarction: predictors of death. GUSTO Investigators. Global Utilization of Streptokinase and Tissue-Plasminogen Activator for Occluded Coronary Arteries. Am Heart J. 1999;138(1 Pt 1):21–31. | |
Antman EM, Hand M, Armstrong PW, et al; Canadian Cardiovascular Society; American Academy of Family Physicians; American College of Cardiology; American Heart Association. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2008;51(2):210–247. | |
Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360(26):2705–2718. | |
Di Mario C, Dudek D, Piscione F, et al. Immediate angioplasty versus standard therapy with rescue angioplasty after thrombolysis in the Combined Abciximab REteplase Stent Study in Acute Myocardial Infarction (CARESS-in-AMI): an open, prospective, randomised, multicentre trial. Lancet. 2008;371(9612):559–568. | |
Kushner FG, Hand M, Smith SC, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54(23):2205–2241. | |
O’Gara PT, Kushner FG, Ascheim DD, et al; American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78–e140. | |
King SB, Smith SC, Hirshfeld JW, et al; 2005 Writing Committee Members. 2007 focused update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee. Circulation. 2008;117(2):261–295. | |
Hochman JS, Sleeper LA, White HD, et al; SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. One-year survival following early revascularization for cardiogenic shock. JAMA. 2001;285(2):190–192. | |
Holmes DR, Berger PB, Hochman JS, et al. Cardiogenic shock in patients with acute ischemic syndromes with and without ST-segment elevation. Circulation. 1999;100(20):2067–2073. | |
The PURSUIT Trial Investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med Med. 1998;339(7):436–443. | |
Holzer R, Balzer D, Amin Z, et al. Transcatheter closure of postinfarction ventricular septal defects using the new Amplatzer muscular VSD occluder: Results of a U.S. Registry. Catheter Cardiovasc Interv. 2004;61(2):196–201. | |
Maisch B, Seferović PM, Ristić AD, et al; Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004;25(7):587–610. | |
Khandaker MH, Espinosa RE, Nishimura RA, et al. Pericardial disease: diagnosis and management. Mayo Clin Proc. 2010;85(6):572–593. | |
uptodate.com [homepage on the Internet]. Acute aortic regurgitation in adults. UpToDate, Inc (Wolters Kluwer); 2103 [updated May 8, 2013; cited September 16, 2013]. Available from: http://www.uptodate.com/contents/acute-aortic-regurgitation-in-adults. Accessed December 7, 2013. | |
Hiratzka LF, Bakris GL, Beckman JA, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: Executive summary A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121:1544–1579. | |
Roberts WC, Ko JM, Moore TR, Jones WH. Causes of pure aortic regurgitation in patients having isolated aortic valve replacement at a single US tertiary hospital (1993 to 2005). Circulation. 2006;114(5):422–429. | |
Bonow RO, Carabello BA, Chatterjee K, et al; 2006 Writing Committee Members; American College of Cardiology/American Heart Association Task Force. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation. 2008;118(15):e523–e661. | |
Torbicki A. Thromboembolic venous disease. Available from: http://www.escardio.org/congresses/esc-2013/congress-reports/Pages/149-Torbicki.aspx#.UrjxVPud7To. Accessed December 2, 2013. | |
Jaff MR, McMurtry MS, Archer SL, et al; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–1830. | |
Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744–749. | |
Engelberger RP, Kucher N. Catheter-based reperfusion treatment of pulmonary embolism. Circulation. 2011;124(19):2139–2144. | |
Torbicki A, Perrier A, Konstantinides S, et al; ESC Committee for Practice Guidelines (CPG). Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008;29(18):2276–2315. | |
Gibbs S. Interventional management of acute pulmonary embolism. Available from: http://www.escardio.org/congresses/esc-2011/congress-reports/Pages/768-Gibbs.aspx#.UrjyPvud7To. Accessed December 2, 2013. | |
Kuo WT, Gould MK, Louie JD, Rosenberg JK, Sze DY, Hofmann LV. Catheter-directed therapy for the treatment of massive pulmonary embolism: systematic review and meta-analysis of modern techniques. J Vasc Interv Radiol. 2009;20(11):1431–1440. | |
Misawa Y. Extracorporeal membrane oxygenation support for acute pulmonary embolism. Circulation. 2004;109(20):e229. | |
Howes J, Khilkin M, DeRose J, et al. Veno-arterial extracorporeal membrane oxygenation as a salvage therapy in massive pulmonary embolism. Chest. 2011;140(4_MeetingAbstracts):64A. | |
Bauer C, Vichova Z, French P, et al. Extracorporeal membrane oxygenation with danaparoid sodium after massive pulmonary embolism. Anesth Analg. 2008;106(4):1101–1103. | |
Kawahito K, Murata S, Adachi H, Ino T, Fuse K. Resuscitation and circulatory support using extracorporeal membrane oxygenation for fulminant pulmonary embolism. Artif Organs. 2000;24(6):427–430. | |
Hsieh PC, Wang SS, Ko WJ, Han YY, Chu SH. Successful resuscitation of acute massive pulmonary embolism with extracorporeal membrane oxygenation and open embolectomy. Ann Thorac Surg. 2001;72(1):266–267. | |
Virani SS, Khan AN, Mendoza CE, Ferreira AC, de Marchena E. Takotsubo cardiomyopathy, or broken-heart syndrome. Tex Heart Inst J. 2007;34(1):76–79. | |
Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (tako-tsubo) cardiomyopathy. J Am Coll Cardiol. 2010;55(4):333–341. |
Supplementary material
 |
|
References
O’Gara PT, Kushner FG, Ascheim DD, et al; American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78–e140. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.