Back to Journals » International Journal of Women's Health » Volume 14
Cranberry Supplement, D-Mannose, and Other OTC Modalities for Prevention of Recurrent UTI in Women Post-Electrofulguration
Authors Kenee PRM ![]() , Christie AL, Zimmern PE
, Christie AL, Zimmern PE
Received 11 January 2022
Accepted for publication 23 April 2022
Published 3 May 2022 Volume 2022:14 Pages 643—653
DOI https://doi.org/10.2147/IJWH.S355469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Parker RM Kenee,1 Alana L Christie,2 Philippe E Zimmern1
1Department of Urology, UT Southwestern Medical Center, Dallas, TX, 75290-9110, USA; 2Simmons Comprehensive Cancer Center Biostatistics, UT Southwestern Medical Center, Dallas, TX, 75390-8852, USA
Correspondence: Philippe E Zimmern, Department of Urology, UT Southwestern Medical Center, 5323 Harry Hines Blvd, Dallas, TX, 75390-9110, USA, Tel +1 214 648 9397, Fax +1 214 648 8786, Email [email protected]
Purpose: To assess patient reliance on various over-the-counter (OTC) modalities used for prevention of recurrent urinary tract infection (RUTI) after electrofulguration (EF).
Patients and Methods: Following IRB approval, qualifying women were offered a short survey over the phone by a medical researcher to collect information about their use of various OTC modalities for prophylaxis of RUTI. Data was compared between two cohorts, ≥ 70 years old and < 70 years old, using chi-squared and Student’s t-tests.
Results: From a database of 324 patients, 163 accepted the interview. 17% (28/163) reported current use of cranberry supplements, 10% (16/163) D-mannose supplements, and 42% (69/163) another non-prescription modality for RUTI prophylaxis. The non-geriatric (< 70 years old) cohort spent, on average, $80 less annually on cranberry/D-mannose supplements (P=0.043) than the geriatric cohort and were more likely to use non-prescription modalities for the prevention of UTI (52% vs 30%; P=0.0061). Individuals using D-mannose were also much more likely to purchase their product online compared to those using cranberry supplements (85% vs 56%). Across all modalities, the perceived benefit difference in reducing UTI/year ranged from a median of 0 for Pyridium® (phenazopyridine hydrochloride) to four for probiotics, with D-mannose and cranberry at two/year, and those increasing daily fluid consumption at 2.5 fewer UTI/year.
Conclusion: Continued use of non-prescription modalities for RUTI prophylaxis were common among women with an EF history, but varied based on age groups. Across both age cohorts, annual expenditure and perceived benefit also varied among different OTC prophylactic modalities. Awareness of type and method of OTC modality implementation by patients with RUTI is essential to aligning use with current field recommendations.
Keywords: recurrent UTI, menopausal women, cranberry, D-mannose, UTI supplements
Introduction
An estimated 40% to 50% of women will experience at least one urinary tract infection (UTI) requiring antibiotic treatment in their lifetime, with an estimated annual cost to health care systems of nearly two billion dollars.1 According to a recent review of the literature, recurrent urinary tract infection (RUTI) is generally defined as a minimum of three symptomatic UTI within a 12-month period, or two symptomatic UTI within a six-month period.2 RUTI is becoming increasingly recognized as a commonly occurring condition placing significant burden both on women and the health-care infrastructure. In one study from Finland, 179 adult women treated for UTI at a clinic were followed for 12 months, with 44% suffering from recurrence.3 RUTI may become refractory to antibiotic treatment. In one study of 86 postmenopausal women suffering from RUTI, 17 out of 86 patients (20%) were resistant and/or allergic to trimethoprim/sulfamethoxazole, fluoroquinolones, and nitrofurantoin. A further 28% of patients in the study were sensitive to nitrofurantoin only.4 Furthermore, a recent study by Manseck et al reported a statistically significant higher rate of resistance to a variety of antibiotics when comparing 1115 patients, separated by ≥75 years old and <75 years old (ciprofloxacin, P=0.02; levofloxacin, P<0.001; trimethoprim/sulfamethoxazole, P=0.026; imipenem, P=0.002; fosfomycin, P=0.009).5 Consideration for the methods by which elderly women are treated for RUTI—both those moderated by health care professionals and those that are not—requires optimization. One study found 10.3% of hospitalizations are due to infections of the bladder, kidneys or urinary tract, with admission rates highest in women and individuals ≥80 years old.6 The need for effective alternate treatment modalities for patients suffering from antibiotic-refractory RUTI is apparent.
One such treatment modality is cystoscopy with electrofulguration (EF) of chronically infected areas (cystitis). Bladder biopsies of these areas of cystitis have confirmed the presence of residing bacteria in the bladder wall, likely causing the recurrence pattern and contributing to antibiotic resistance.7 In one study of 95 patients undergoing electrofulguration for the treatment of RUTI, 83 patients (88%) were clinically improved or cured in the five years following the procedure.8 Particularly among those improved, there is an interest to curtail new recurrences by using over-the-counter (OTC) medications and home remedies. Since little is known on how much OTC medications and home remedies are used by patients, we focused our research on cranberry and D-mannose supplements, two among the most popular such therapies considered by patients for the prevention and/or treatment of UTIs. Given the fact there is a subset of our patient population undergoing EF that continues to experience RUTI, we assessed patient reliance and perceived benefit of OTC and home remedies in one physician’s patient cohort of women with a history of antibiotic-refractory RUTI treated with EF.
Patients and Methods
This project was approved by the Institutional Review Board (IRB) at UT Southwestern Medical Center in Dallas, Texas. Participants were informed about the purpose of the survey and study, in accordance with the Declaration of Helsinki. Women with a history of prior EF for the treatment of antibiotic-refractory RUTI by one FPMRS urologist in a tertiary care center were included. Exclusion factors included non-English speaking patients and employees of the medical center where the procedure was performed due to restricted access to their electronic medical record. A medical researcher not involved with the care of these patients attempted to contact patients over a two-month period. Phone calls were made using the Doximity application to display the clinic’s caller ID. Up to three phone call attempts were made for each qualifying patient. When reached by phone, women were offered a short (3–5 min) survey, informed of the purpose of the study and, upon consenting, were asked a series of questions about their use of common OTC and home-remedy modalities for preventing RUTI grouped in “cranberry”, “D-mannose”, “others” (see Figure 1). “Others” and “nonantibiotic modifiers” as referenced in this study refers to any non-prescription modality for attempting to reduce the frequency or severity of UTI, and the items contained in this list was defined by the modalities cited by women during the surveys. Women’s responses included a diverse range of modalities, including: drinking cranberry juice, apple cider vinegar, or increased daily water; phenazopyridine hydrochloride; and consuming garlic and turmeric. The data was analyzed by comparing two cohorts, 70 years of age or older (geriatric) or less than 70 years (non-geriatric). Statistical methods: descriptive statistics were provided as medians and interquartile ranges (IQR) for continuous measures, and as frequencies and percentages for categorical measures. The chi-squared test was used to test for association between age group (<70 years vs ≥70 years) and categorical patient characteristics. Student’s t-tests were used to test for differences in the means of continuous measures between the age groups. All tests were performed at the 0.05 significance level without adjustment for multiple comparisons using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
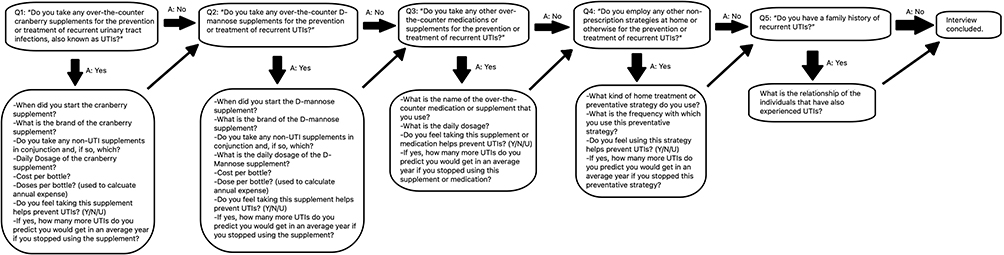 |
Figure 1 Depiction of the series of questions used to gather information from each participant about their use of nonantibiotic RUTI prophylactics. |
Results
From 324 patients in the database, 161 did not participate due to cognitive decline (7), deceased (6), non-English speaking (6), and no return call (142). The final study dataset comprises 163 patients. Demographic information, as well as general findings about patients’ use of cranberry supplements, D-mannose, or other OTC modalities, is presented in Table 1. The median age of participants was 72 years old (range: 25–94). A family history of RUTI was reported in 36% (58/163) of participants. Current use of cranberry supplements was reported by 17% (28/163) of patients, D-mannose supplements by 9% (14/163) of patients and use of other nonantibiotic modifiers was reported by 39% (64/163) of patients. 8% (13/163) of patients reported current use of multiple modalities (among Cranberry supplement, D-mannose supplement, or “Other” category), including 3% (5/163) that reported use of all three. For patients reporting current use of multiple modalities, information was collected for each as with other entries, and each usage was treated as a separate data point for statistical analyses. Among patients currently using cranberry or D-mannose supplements for the prevention of RUTI, the annual costs attributed to these supplements ranged from $72 to $418 with an average annual expenditure of $139.
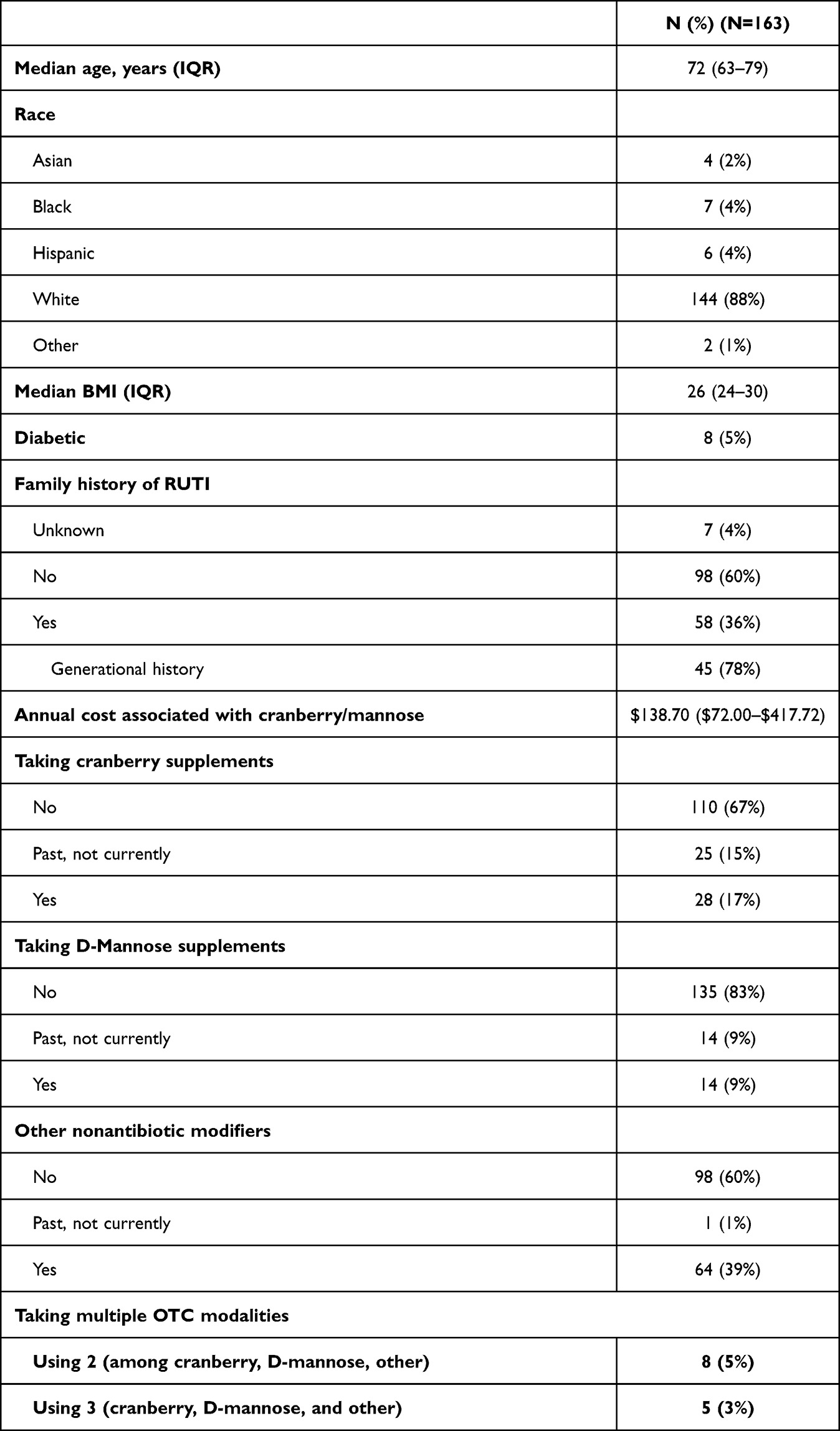 |
Table 1 Demographic and Patient Characteristics of Study Participants |
Patients responding affirmatively to the line of questioning about use of any OTC medications, supplements, or other nonantibiotic modifiers were asked further questions to provide more detailed information about the specific product they use, and their perceived benefit from said product. The results from these questions are listed in Table 2, categorized as “Cranberry”, “D-Mannose”, and “Other”.
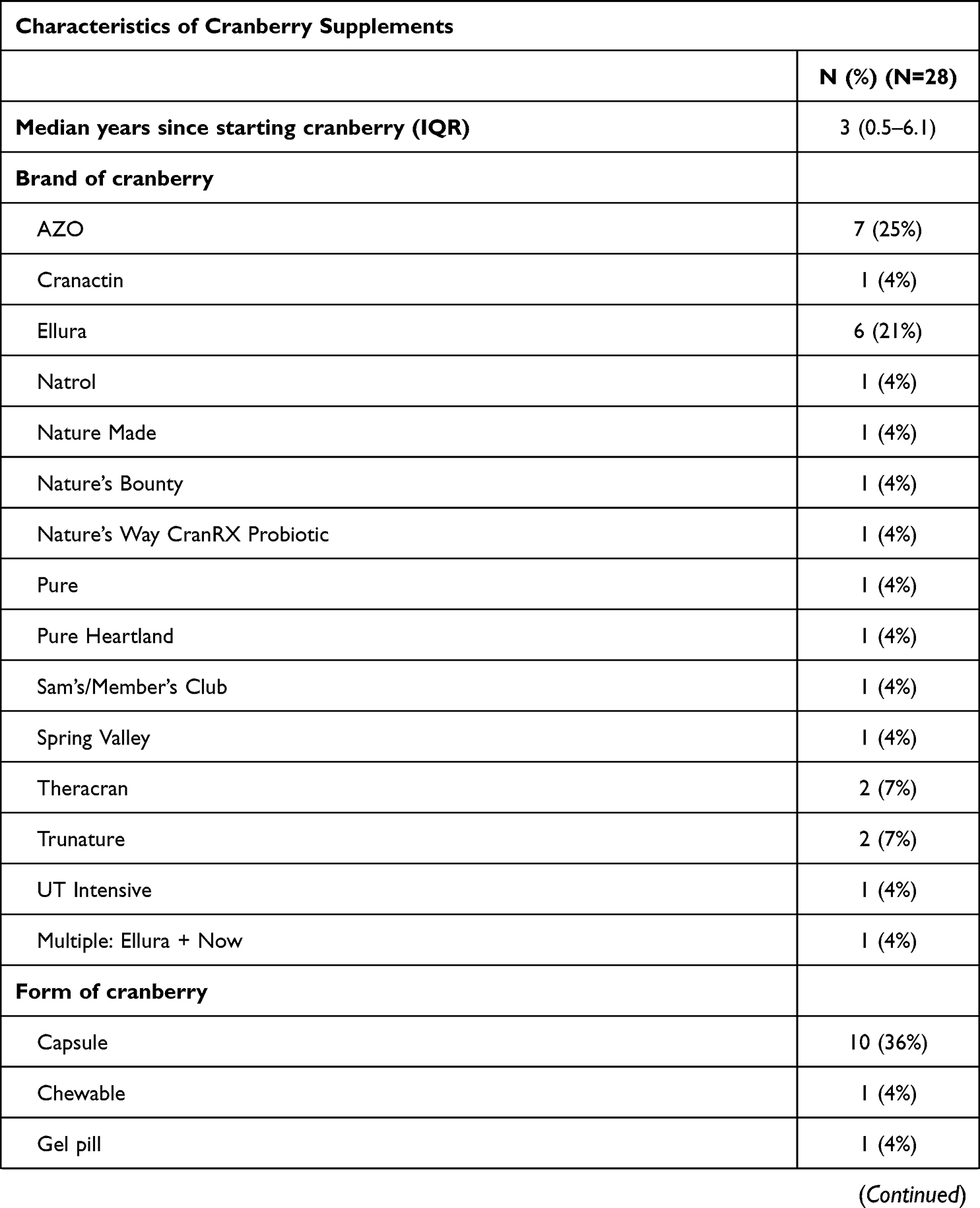 | 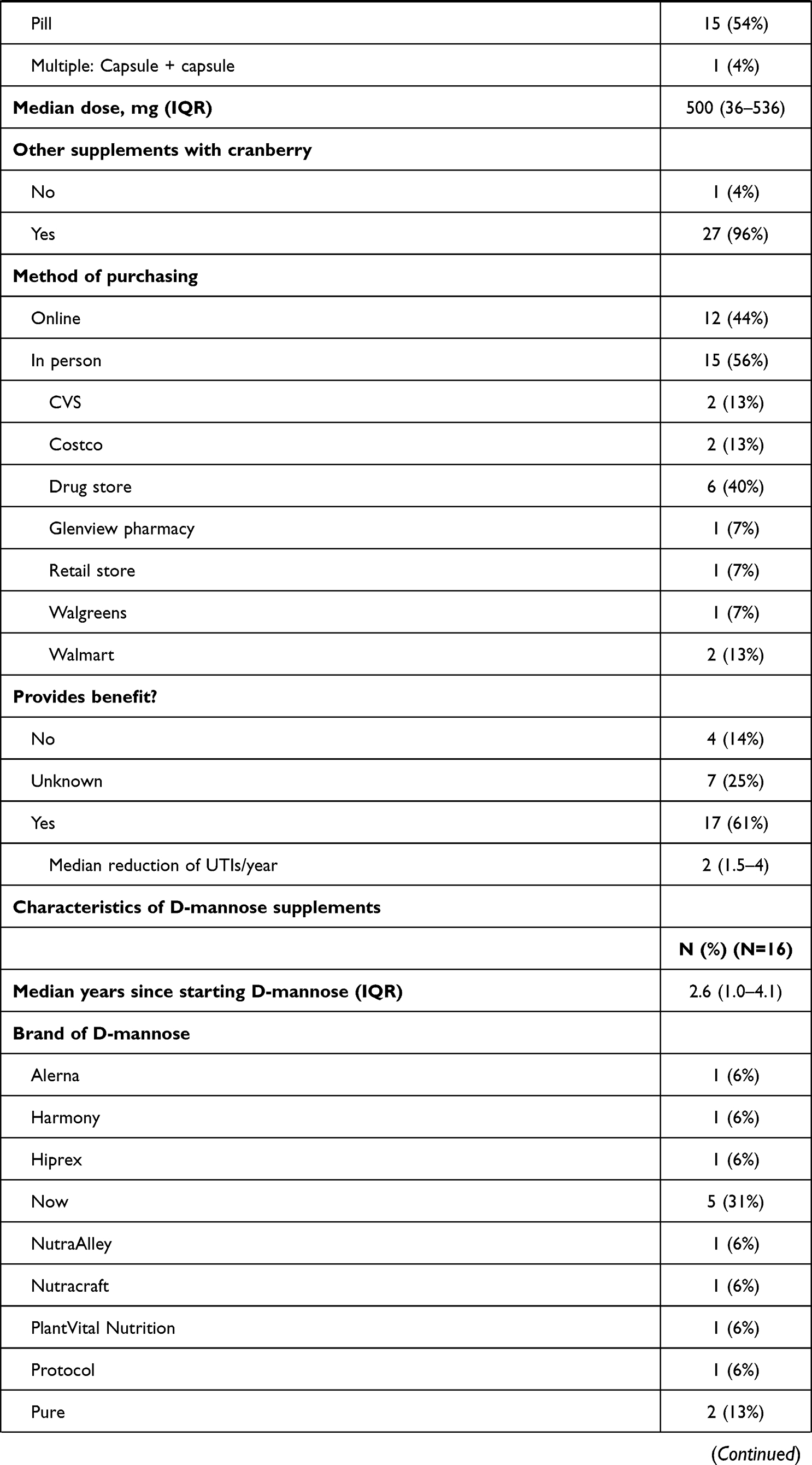 | 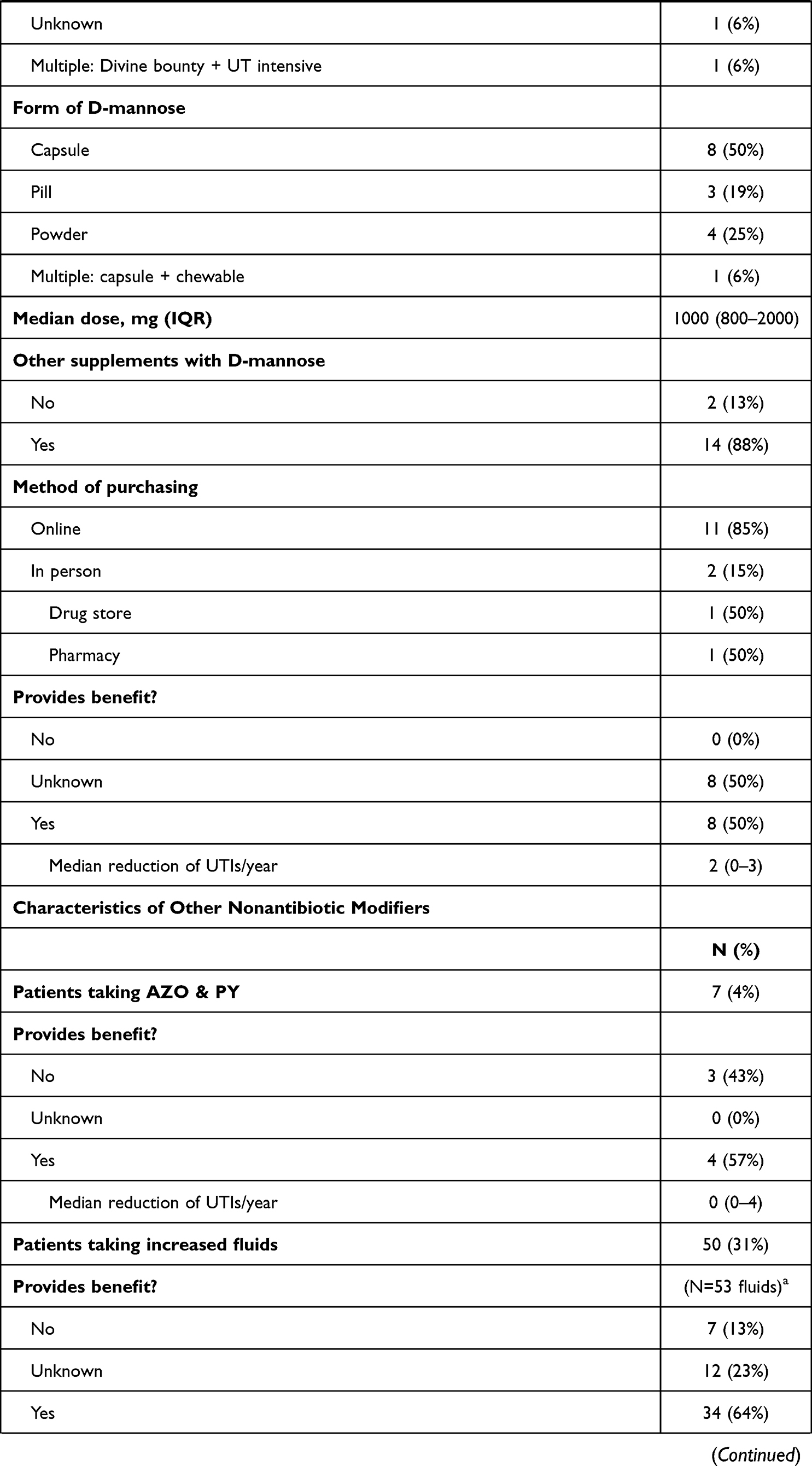 | 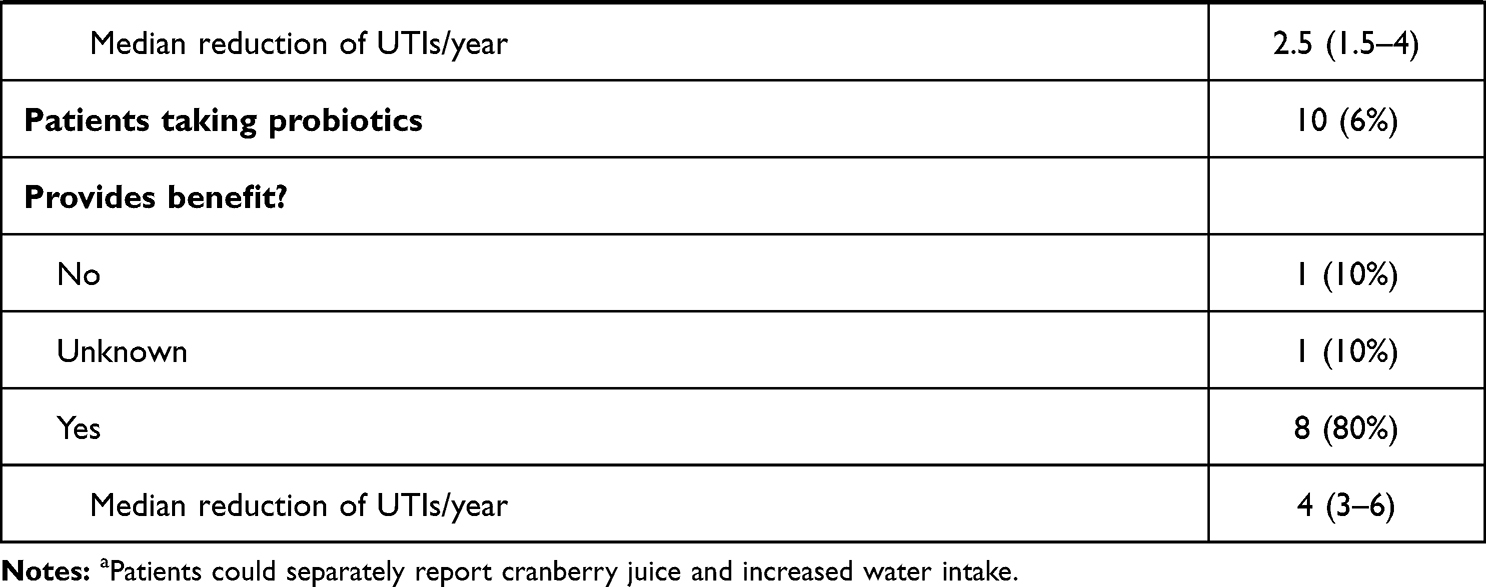 |
Table 2 Further Information About Cranberry/D-Mannose/Other Supplements Taken by Patients Reporting Current Use |
Detailed information about cranberry supplements used by patients is displayed in Table 2. The most popular brands of cranberry supplement used are AZO (25%) and Ellura (21%). In total, 15 different cranberry supplement products were reported. 96% of patients taking a cranberry supplement also reported using other OTC vitamins or supplements unrelated to RUTI prophylaxis. Of note, a majority (56%) of patients purchase their cranberry supplement in person rather than online. Sixty-one percent (17/28) of patients reported subjectively that taking cranberry supplements reduced the number of UTIs they experienced in a typical year, with a median reported number of two fewer UTI/year.
Detailed information about D-mannose supplements used by patients is displayed in Table 2. The most popular brand reported for D-mannose supplementation was Now (31%). Consistent with the findings for cranberry supplements, 88% of patients taking D-mannose also reported use of other OTC vitamins or supplements unrelated to RUTI prophylaxis. In stark contrast to findings for cranberry supplements, 85% (11/16) of patients taking a D-mannose supplement reported obtaining their D-mannose via online purchase. Fifty percent (8/16) of patients reported a subjective benefit to their UTIs from taking D-mannose, with a median reported number of two fewer UTI/year.
Detailed information about non-cranberry, non-D-mannose OTC modalities used by patients for RUTI prophylaxis is displayed in Table 2. A diverse range of modalities were reported by a total of 69 patients, with the most popular being increased daily water intake (72%; 50/69), probiotics (14%; 10/69), and phenazopyridine hydrochloride (10%; 7/69). Among the three most popular modalities, 69% (46/67) reported a subjective benefit to their UTIs from using these modalities. Median reported number of fewer UTI/year was separated by modality, with probiotic having the highest reported benefit, at four fewer UTI/year.
Information across all survey questions were aggregated and compared based on two cohorts, separated by age: ≥70 years old (geriatric), and <70 years old (non-geriatric). These findings are displayed in Table 3. Patients <70 years old using cranberry or D-mannose supplements spent on average 40% less ($80; $121 vs $201) annually (P=0.043). Patients in the cohort <70 years old were also much more likely to use other non-cranberry, non-D-mannose RUTI prophylactics, with 52% (36/69) reporting current use compared with 30% (28/94) in the ≥70 years old cohort (P=0.0062).
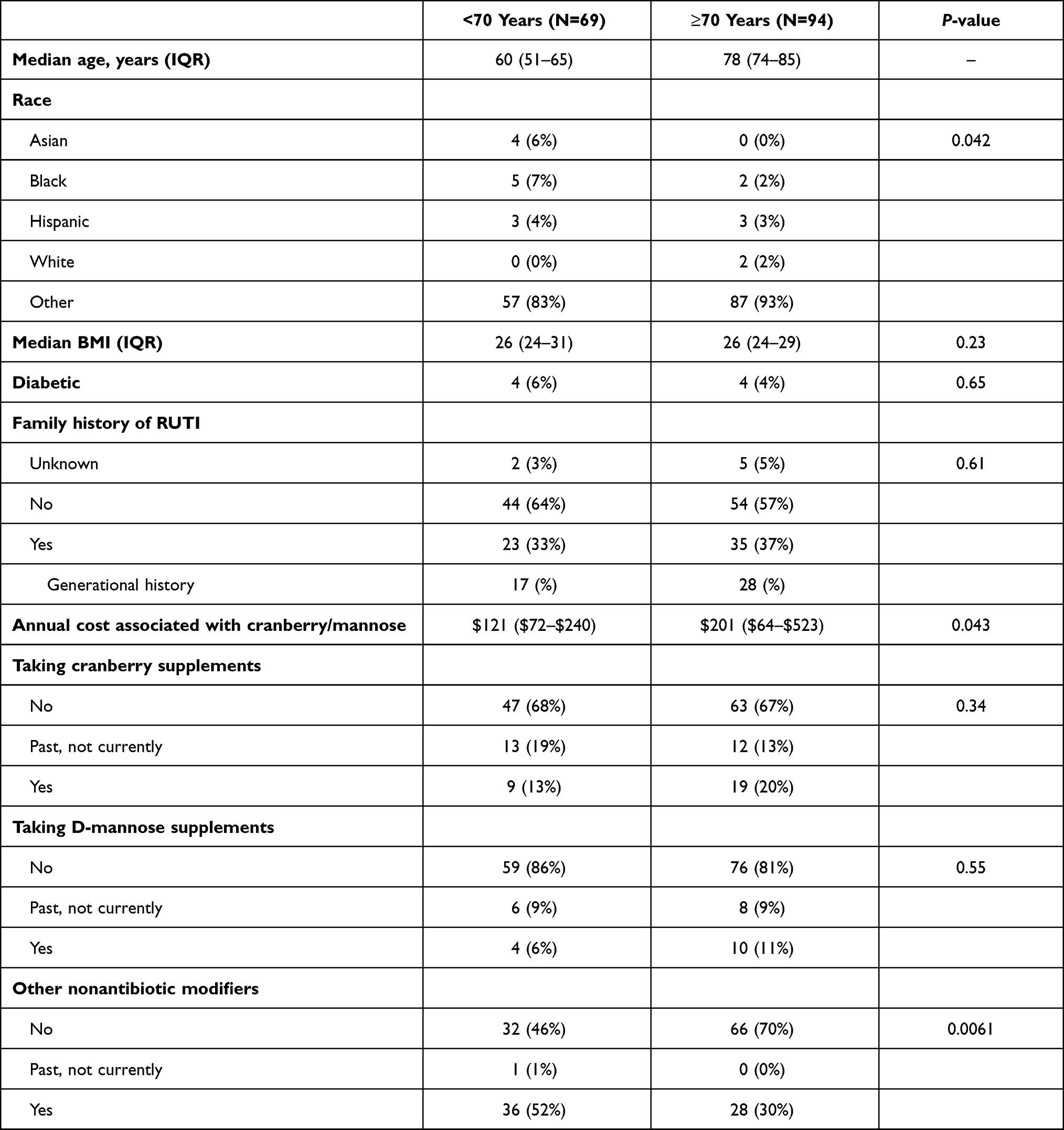 |
Table 3 Patient Characteristics and General Findings Regarding Patients’ Supplement Usage, Analyzed Across Age Cohort (≥70 and <70 Years Old) |
Discussion
Among the women surveyed with a history of electrofulguration for the control of antibiotic-refractory RUTI, nonantibiotic modifiers for the prevention of UTI recurrence not including cranberry supplement or D-mannose were most popular, with 42% (69/163) reporting use of at least one treatment modality. This included a range of modalities; the most cited nonantibiotic UTI preventative approach was daily increased fluid intake (33%; 53/163). Increasing fluid intake (of which 50/53, 94% were water), has been researched historically to determine efficacy for preventing UTIs. Hooten et al, in a randomized controlled trial, found a statistically significant reduction in the number of UTIs experienced within a one-year time span among individuals increasing their water intake by 1.5 L daily over the 12 months they were observed, when compared to a control group that maintained their normal hydration habits in a cohort of female premenopausal adults with a history of RUTI.9 Several studies, including Hooten et al, have assessed the efficacy of increasing water intake for the prevention of RUTI.9–11 No studies, however, have assessed the prevalence with which this strategy or any other nonantibiotic modality is implemented in any subpopulation of patients experiencing RUTI. The cited motivation to implement one modality or another has not been evaluated, though increasing fluid intake, and water specifically, may be the most common modality reported in this study among women with a history of EF for antibiotic-refractory RUTI not because it is more efficacious than cranberry or D-mannose, but because of ease of access and limited cost. This speculation is supported by findings in other related studies: Stothers, in an RCT including 150 female participants, estimated the average annual cost of cranberry supplement and juice at $624 and $1400, respectively.12 Furthermore, while either option may be a prohibitively high price for many women that would otherwise consider some form of cranberry supplementation for reducing RUTI, the study additionally found that women were more likely to use cranberry supplements than cranberry juice.12 Our study was consistent with this finding: Women were more likely to use the more affordable cranberry supplement than the juice (28 vs 3; 17% vs 2%). In addition, when comparing the geriatric and non-geriatric cohorts participating in our survey, women under the age of 70 were more likely to use additional non-cranberry, non-D-Mannose modalities, and spent less money on their cranberry or D-mannose supplement RUTI prophylactics. Possible explanations include the greater likelihood for financial stability that comes with increasing age, and secondarily a willingness to spend more on OTC prophylactic medications in the geriatric cohort.13
Women that have turned to cranberry supplements or D-mannose supplements have used them for, on average, a similar length of time prior to the time of survey (3 years for cranberry supplements vs 2.6 years for D-mannose supplements). Women purchased their nonantibiotic RUTI prophylactics online or in person, though the online method of purchase was much more common among those using D-mannose (85% of D-mannose users and 44% of cranberry supplement-users). The cause for the discrepancy in method of purchase and attainment between cranberry and D-mannose supplements is unclear, but may have impacted our finding that survey participants reported a subjective reduction of two UTI/year for either cranberry or D-mannose supplements. A recent study by Howell et al found that, based on the prior determination that proanthocyanidins (PACs) are primarily responsible for the Escherichia coli fimbriae anti-adhesion activity, products with a higher soluble PAC concentration would be expected to have more efficacy in preventing UPEC infection.14–16 Furthermore, Howell et al determined that products available exclusively online, such as Ellura, are often cranberry juice-derived and have a much higher soluble PAC content than whole cranberry fruit-derived products such as AZO that are also available for in-person purchase. That the cohort of patients in our study were far more likely to acquire cranberry products in-person may have contributed to our finding that cranberry products did not subjectively out perform D-mannose products.14
In animal models, the presumed mechanism for cranberry to prevent infection by uropathogenic E. coli (UPEC) is interference with P-fimbriae adhesion.17 As discussed above, when the correct form is used, cranberry supplements are likely effective in reducing UTI.14,18–20 A 2021 meta-analysis by Xia et al including 23 trials with 3979 patients found a 32% relative risk reduction in women with RUTI when using cranberry-containing products (RR=0.68; 95% CI: 0.56~0.81).20
In animal models, the presumed mechanism for D-mannose to prevent infection by UPEC is interference with type 1 pilus adhesin (FimH) binding. However, while one meta-analysis of D-mannose as an RUTI treatment modality found an overall reduction in relative risk when comparing D-mannose to placebo, other research has highlighted the difficulty in applying the proposed mechanism of D-mannose to an effective therapeutic.21 A study by Spaulding et al found that specifically engineered biphenyl mannoside FimH inhibitors demonstrated FimH affinity 100,000 times higher than natural D-mannose sugar.22 Previously, there was concern that therapeutic levels of nonspecific D-mannose could create severe side effects in patients due to interference with immune response, glycosylation of proteins elsewhere in the body, and development of toxic end products when compounded with the body’s natural production of mannose.22 Though development is ongoing, it is believed that more targeted FimH antagonists may overcome these obstacles.23
Perhaps most interestingly, there were several key differences in the use of OTC medications and at-home remedies when comparing the geriatric (≥70) and non-geriatric (<70) patient cohorts. Patients in the non-geriatric cohort spent, on average, $80 (40%) less on cranberry or D-mannose products per year (P=0.043). Patients in the non-geriatric cohort were also more likely to use non-cranberry, non-D-mannose modalities than those from the geriatric cohort (52% vs 30%, P=0.0061). One possible explanation is younger patients’ greater likelihood to be active on internet social networking platforms that disseminate information about nonantibiotic options and strategies for RUTI prophylaxis. An aggregate study of Americans’ internet use from 2000–2004 found that 22% of Americans aged 65 and older report using the internet, compared to 75% of Americans 30–49 years old and 77% of Americans 18–29 years old.24 In addition, another study assessing the prevalence of use of the internet for patient self-education about pelvic-floor conditions found that nearly 42% of women used social networking websites to collect information about their condition, and that this medium was more commonly used in younger age cohorts.25
To our knowledge, no studies have investigated the prevalence of use for these modalities in real life practice. Jepson et al performed a comprehensive meta-analysis of the effectiveness of cranberry for RUTI prophylaxis in the literature, but all studies analyzed actively assigned participants to arms of the study, rather than observational methods of those using cranberry among a larger patient base.26 Our research provides a snapshot of prevalence of use of these OTC RUTI prophylactic modalities in one cohort of RUTI-prone patients—post-EF women—and paves the way to more research on these UTI-prone patients. Given the rise of antibiotic-resistant pathogens in causing RUTI, it is important for older women who select OTC methods for UTI prevention to rely on evidence-based medicine.
Strengths of the study included conducting the survey over the phone, allowing open-ended questions and confirmation that information received was correct and relevant to the question asked; also, we had access to a relatively large sampling of women that had previously undergone EF for treatment of RUTI, and were concerned about a future possible UTI recurrence. Historical studies have shown that conducting surveys via telephone yields higher response rates. One study by Rhee et al found a response rate of 41.4% for 360 individuals contacted via telephone, and a response rate of 19.7% for 360 individuals contacted via mail.27 Limitations of this study included relying on the effectiveness of the patient as a reporter of the supplements and home-remedies they utilize for preventing RUTI. There were also some inconsistencies in the way in which participants reported their answer responses, and these had to be normalized for statistical analysis (ie, estimate of annual cost vs exact value).
Conclusion
Cranberry supplements, D-mannose, and other OTC medications and home remedies are used as RUTI prophylaxis among women that have undergone EF for antibiotic-refractory UTI. Our data confirms a difference in the modalities implemented by women of different age groups: Women under the age of 70 were more likely to use non-cranberry, non-D-mannose modalities than their geriatric counterparts, and spent an average of $80 less annually on cranberry and/or D-mannose supplements. Our study suggests that women ≥70 years old may be purchasing products (low soluble PAC-containing cranberry supplement or D-mannose) with variable reported efficacy. This is especially concerning for a cohort of patients in which rate of RUTI and antibiotic-resistance is highest. This study represents just the first step in monitoring the application of OTC modalities for RUTI prevention in susceptible patient populations. A better understanding of the way otherwise unmonitored OTC modalities are used will help health care providers tailor recommendations and ensure that the way patients use these products is aligned with current study findings. More research would be needed to determine the prevalence of use for these nonantibiotic UTI prophylactics in the general population suffering from RUTI.
Ethical Considerations
Research involving human participants and/or animals—ethical approval: all procedures performed in studies involving human participants were in accordance with the ethical standards of institutional research committee (UT Southwestern IRB) and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med. 2002;113:5s–13s.
2. Malik RD, Wu YR, Zimmern PE. Definition of Recurrent Urinary Tract Infections in Women: which One to Adopt? Female Pelvic Med Reconstr Surg. 2018;24(6):424–429.
3. Ikäheimo R, Siitonen A, Heiskanen T, et al. Recurrence of urinary tract infection in a primary care setting: analysis of a 1-year follow-up of 179 women. Clin Infect Dis. 1996;22(1):91–99.
4. Malik RD, Wu YR, Christie AL, Alhalabi F, Zimmern PE. Impact of Allergy and Resistance on Antibiotic Selection for Recurrent Urinary Tract Infections in Older Women. Urology. 2018;113:26–33.
5. Manseck AS, Otto W, Schnabel M, Denzinger S, Burger M, Spachmann PJ. Geriatric Patients and Symptomatic Urinary Tract Infections: analysis of Bacterial Range and Resistance Rates at a 3rd Level of Care Hospital in Germany. Urol Int. 2022;106(3):298–303.
6. Matthews SJ, Lancaster JW. Urinary tract infections in the elderly population. Am J Geriatr Pharmacother. 2011;9(5):286–309.
7. De Nisco NJ, Neugent M, Mull J, et al. Direct Detection of Tissue-Resident Bacteria and Chronic Inflammation in the Bladder Wall of Postmenopausal Women with Recurrent Urinary Tract Infection. J Mol Biol. 2019;431(21):4368–4379.
8. Crivelli JJ, Alhalabi F, Zimmern PE. Electrofulguration in the advanced management of antibiotic-refractory recurrent urinary tract infections in women. Int J Urol. 2019;26(6):662–668.
9. Hooton TM, Vecchio M, Iroz A, et al. Effect of Increased Daily Water Intake in Premenopausal Women With Recurrent Urinary Tract Infections: a Randomized Clinical Trial. JAMA Intern Med. 2018;178(11):1509–1515.
10. Lotan Y, Daudon M, Bruyère F, et al. Impact of fluid intake in the prevention of urinary system diseases: a brief review. Curr Opin Nephrol Hypertens. 2013;22(Suppl 1):S1–10.
11. Beetz R. Mild dehydration: a risk factor of urinary tract infection? Eur J Clin Nutr. 2003;57(Suppl 2):S52–58.
12. Stothers L. A randomized trial to evaluate effectiveness and cost effectiveness of naturopathic cranberry products as prophylaxis against urinary tract infection in women. Can J Urol. 2002;9(3):1558–1562.
13. Land KC, Russell ST. Wealth Accumulation across the Adult Life Course: stability and Change in Sociodemographic Covariate Structures of Net Worth Data in the Survey of Income and Program Participation, 19841991. Soc Sci Res. 1996;25(4):423–462.
14. Howell AB, Dreyfus J-F, Chughtai B. Differences in Urinary Bacterial Anti-Adhesion Activity after Intake of Cranberry Dietary Supplements with Soluble versus Insoluble Proanthocyanidins. J Diet Suppl. 2021;3:1–18.
15. Beachey EH. Bacterial adherence: adhesin-receptor interactions mediating the attachment of bacteria to mucosal surface. J Infect Dis. 1981;143(3):325–345.
16. Howell AB, Vorsa N, Der Marderosian A, Foo LY. Inhibition of the adherence of P-fimbriated Escherichia coli to uroepithelial-cell surfaces by proanthocyanidin extracts from cranberries. N Engl J Med. 1998;339(15):1085–1086.
17. Sobota AE. Inhibition of bacterial adherence by cranberry juice: potential use for the treatment of urinary tract infections. J Urol. 1984;131(5):1013–1016.
18. Luís Â, Domingues F, Pereira L. Can Cranberries Contribute to Reduce the Incidence of Urinary Tract Infections? A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Clinical Trials. J Urol. 2017;198(3):614–621.
19. Wang CH, Fang CC, Chen NC, et al. Cranberry-containing products for prevention of urinary tract infections in susceptible populations: a systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172(13):988–996.
20. Xia JY, Yang C, Xu D. Consumption of cranberry as adjuvant therapy for urinary tract infections in susceptible populations: a systematic review and meta-analysis with trial sequential analysis. PLoS One. 2021;16(9):e0256992.
21. Lenger SM, Bradley MS, Thomas DA, Bertolet MH, Lowder JL, Sutcliffe S. D-mannose vs other agents for recurrent urinary tract infection prevention in adult women: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;223(2):
22. Spaulding CN, Klein RD, Ruer S, et al. Selective depletion of uropathogenic E. coli from the gut by a FimH antagonist. Nature. 2017;546(7659):528–532.
23. Mydock-McGrane LK, Hannan TJ, Janetka JW. Rational design strategies for FimH antagonists: new drugs on the horizon for urinary tract infection and Crohn’s disease. Expert Opin Drug Discov. 2017;12(7):711–731.
24. Fox S. Older Americans and the Internet: Just 22% Go Online, but Their Enthusiasm for Email and Search May Inspire Their Peers to Take the Leap. Pew Internet & American Life Project; 2004.
25. Mazloomdoost D, Kanter G, Chan RC, et al. Social networking and Internet use among pelvic floor patients: a multicenter survey. Am J Obstet Gynecol. 2016;215(5):
26. Jepson RG, Williams G, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2012;10(10):Cd001321.
27. Rhee KJ, Allen RA, Bird J. Telephone vs mail response to an emergency department patient satisfaction survey. Acad Emerg Med. 1998;5(11):1121–1123.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.