Back to Journals » Patient Preference and Adherence » Volume 16
COVID-19 Vaccination Acceptance and Its Associated Factors Among the Iraqi Population: A Cross Sectional Study
Authors Al-Qerem W ![]() , Hammad A
, Hammad A ![]() , Alsajri AH
, Alsajri AH ![]() , Al-Hishma SW
, Al-Hishma SW ![]() , Ling J
, Ling J ![]() , Mosleh R
, Mosleh R ![]()
Received 6 December 2021
Accepted for publication 20 January 2022
Published 5 February 2022 Volume 2022:16 Pages 307—319
DOI https://doi.org/10.2147/PPA.S350917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Walid Al-Qerem,1 Alaa Hammad,1 Alaa Hussein Alsajri,2,3 Shadan Waleed Al-Hishma,2 Jonathan Ling,4 Rami Mosleh5
1Department of Pharmacy, Al-Zaytoonah University of Jordan, Amman, Jordan; 2Specialized Bone Marrow Transplant Center, Baghdad, Iraq; 3University of Sains Malaysia, School of Pharmaceutical sciences, Penang, Malaysia; 4Department of Pharmacy, Faculty of Science and Wellbeing University of Sunderland, Sunderland, UK; 5Department of Pharmacy, Faculty of Medicine & Health Sciences, An-Najah National University, Nablus, Palestine
Correspondence: Rami Mosleh
Department of Pharmacy, Faculty of Medicine & Health Sciences,An-Najah National University, PO Box 7, Nablus, Palestine
, Tel +970 592859300
, Email [email protected]
Purpose: The Coronavirus Disease 2019 (COVID-19) pandemic poses a serious threat to countless lives. Development of an efficient vaccination can help end the pandemic. Vaccine hesitancy/refusal is a huge issue that could stymie attempts to combat the disease. The goal of this study is to examine COVID-19 vaccine hesitancy in Iraq where at the end of July 2021, only 7.4% of the population was vaccinated.
Participants and Methods: This is a cross-sectional web-based study. A survey was used to assess knowledge, attitudes and practice (KAP) toward COVID-19. Willingness to be vaccinated against COVID-19 was assessed, with a logistic regression used to identify variables associated with vaccine acceptance. Motives for vaccination refusal/hesitation were reported.
Results: A total of 1542 participants (females = 56.7%) completed the questionnaire. Participants displayed high knowledge and good protective practices toward COVID-19 (median score = 15 out of 19 and 20 out of 25 respectively). 88.6% were willing to be vaccinated. Variables associated with vaccine acceptance included have not been infected with COVID-19 (OR=0.53, p=0.01), low- and moderate-income (ORs=0.42 and 0.63, p< 0.01 respectively), low education level (OR=0.33, p-value< 0.01) and perceived degree of vaccination importance (OR=1.30, P-value< 0.01). The most mentioned reasons for vaccine refusal were concerns about vaccine safety and side effects (90.35%) and the need for more information about the vaccine (81.2%).
Conclusion: Participants showed high acceptance toward COVID-19 vaccination, nevertheless more efforts should be applied to overcome barriers mentioned by the participants.
Keywords: vaccine hesitancy, vaccine refusal, Iraq, pandemic, COVID-19
Introduction
Coronavirus disease 2019 (COVID-19), is an infectious disease that threatens the lives of millions worldwide. COVID-19 emerged in China in 2019 and rapidly spread across the globe.1 According to the WHO, COVID-19 has caused nearly five million deaths and over 251 million confirmed positive cases. In Iraq there have been about 23 thousand deaths and 2 million confirmed positive cases.2
COVID-19 spreads between individuals by respiratory droplets and/or physical contact. The symptoms of most cases extended from being asymptomatic to mild illness with fewer than 20% experiencing severe or life-threatening complications. Medical comorbidities such as hypertension, diabetes mellitus, cardiovascular and immunodeficiency diseases increase the severity of the illness.3 Nevertheless, patients without such diseases can still develop severe COVID-19, which requires intensive inpatient medical attention.4 In addition to the substantial effect of the pandemic on the health of the individuals and societies globally, COVID-19 has other significant detrimental effects, including social and economic.5
The COVID-19 outbreak in Iraq has caused major alarm to the country’s fragile health infrastructure. Iraq reported its first case of COVID-19 on 21 February 2020.6 To try to control the rapid spread of the pandemic, Iraqi health authorities implemented a lockdown involving some public sectors.7 Yet, failure to control the situation had led to a total lockdown as well as enforcing strict preventative measures including social distancing, face masks, and banning social gatherings.8 Infection and mortality rates hit their peaks in July and August, peaking to 12185 reported cases on 27 July 2021.2
The rise in cases encouraged experts to adopt various treatment protocols, though with limited success. More convenient and efficient measures to halt or possibly end COVID-19 pandemic were therefore sought, particularly development of a vaccine.9 Vaccines have been the cornerstone in controlling and preventing several infectious epidemic diseases.9,10 Thus, huge efforts by global pharmaceutical companies were directed towards creating efficient and safe vaccines to address the COVID-19 pandemic.9
While some companies utilized old technologies in manufacturing the vaccine like live attenuated or dead virus forms, others embarked on developing advanced genetically engineered vaccines. Nonetheless, companies were under enormous pressure to speed up the production of vaccines which led to doubts in their public on their efficacy and safety. Despite of this, the urgency of the situation called for immediate initiation of vaccination protocols all over the world, including Iraq.9 Importantly, a previous study showed that the vast majority of side effects disappeared 1–3 days after immunization, which is encouraging from a safety standpoint.11 Moreover, a recent study has established a protocol for tracking COVID-19 vaccines’ side effects12 which confirms the safety of COVID-19 vaccine. Iraq received its first COVID-19 vaccines at the end of March 2021.13 The Ministry of Health sent vaccines to health institutions throughout the country to be used in protecting people from priority groups according to the national vaccine deployment plan and framework. By the end of July 2021 only 7.4% of the targeted Iraqis were vaccinated against COVID-19.2
Vaccine hesitancy is a long-standing problem that poses a severe threat to global health, as seen by the return of infectious diseases such as measles and pertussis.14 The rapid development of effective and safe COVID-19 vaccines was remarkable. Nonetheless, vaccination reluctance for COVID-19 could be a significant barrier to global efforts to contain the pandemic and limit its health and socioeconomic consequences. Previous work has indicated that the Middle East has one of the lowest COVID-19 vaccine acceptance rates14 Low vaccination rates have been attributed to conspiracy views, which has resulted in a negative attitude toward immunization.15 No information about the COVID-19 acceptance rate or the association factors for vaccination acceptance have yet been reported for Iraq. This study will be the first to quantify the vaccine acceptance in the general Iraqi population, evaluate variables associated with vaccination acceptance and shed light on the reasons of vaccine hesitancy.
Materials and Methods
This cross-sectional study used an online survey distributed as a Google Forms link. The questionnaire was distributed to different regions of Iraq using public social networking sites including Facebook, WhatsApp, Viber, Instagram and Telegram. The questionnaire was distributed between May-July 2021.
The inclusion criteria included all unvaccinated Iraqis aged 18 years old and above, residing in different regions of Iraq regardless of their job, gender, socio-economic status, or religion.
Ethical Approval
All the participants agreed to the informed consent form included in the questionnaire. Ethical approval was obtained from ethical committee of the Medical City Complex (IRB: 2021/04/01). The current study was conducted with accordance to the Declaration of Helsinki Ethical Principles.
Study Design and Data Collection
The questionnaire was based on Al-Qerem et al previously validated and used Arabic questionnaires in Jordan.14,16,17 The questionnaire was presented to a committee of experts and the integrity of the content of the questionnaire was confirmed to be ready for distribution. Furthermore, the questionnaire was presented to 20 people from the public to ensure that the questionnaire was straightforward and uncomplicated before it was distributed on social networking sites. As Arabic is the most spoken language in Iraq, the Arabic version of the questionnaire was used.
“Have you received COVID-19 vaccine yet?” is asked at the beginning of the questionnaire. If participants answered “Yes”, they were directed to submit the questionnaire. The questionnaire consists of five sections. The first section contains questions related to demographic information, including city, gender, age, smoking, economic, and marital status, pregnancy, education, and whether the participant has children or not. The second section includes questions about the health status of the participants and whether the participant had received the flu vaccine during the past year. The third section investigates experiences with COVID-19, including whether the participant was exposed to infection or if he/she knows someone who has been exposed to the virus. The fourth part contains questions about the knowledge of COVID-19, including viral transmission method, symptoms, and the use of different means of protection. The fifth and final part of the questionnaire evaluated COVID-19 vaccine acceptance, and reasons for hesitancy/refusal for vaccination. This study adopted the Centers for Disease Control and Prevention (CDC) risk for severe COVID-19 infection and the study participants’ risk-degree were classified accordingly.3
Knowledge and practice scores were computed for each participant. The knowledge scores were based on knowledge of COVID-19 symptoms, transmission method and preventive measures. One point was given for each correct answer, with a maximum possible score of 19 (Table 3). Practice scores were the sum of the practices reported for the question “Which protective measures have you taken to protect yourself from COVID-19?” (Table 4). Responses were from “Never” (1 point) to “All the time” (5 points), with a maximum possible score of 25.
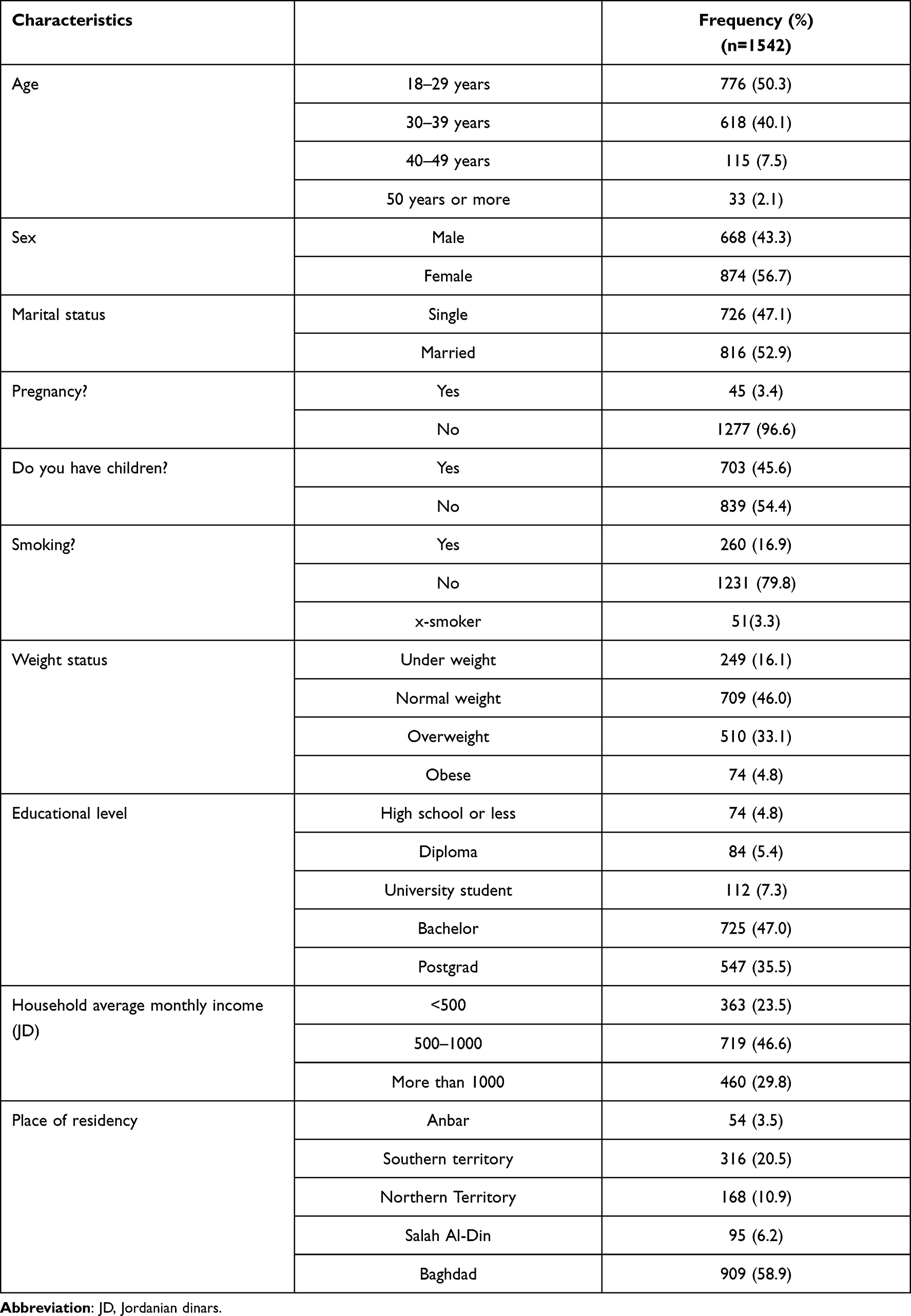 |
Table 1 Sample Characteristics and Demographics |
 |
Table 2 Health Status of Participants |
 |
Table 3 Participants’ Knowledge of COVID-19 |
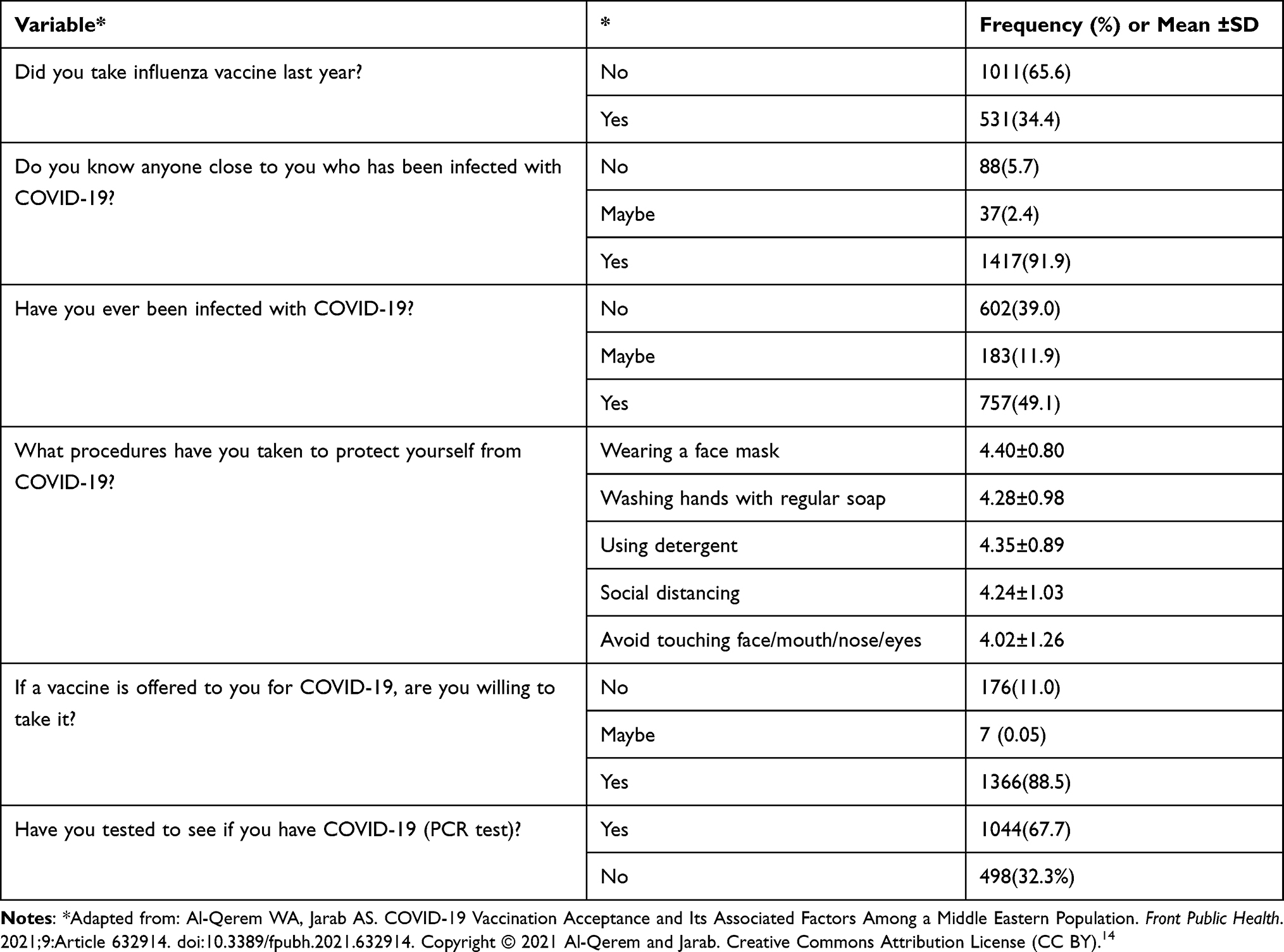 |
Table 4 Participants’ Attitudes and Practices Toward COVID-19 and Vaccination |
The medians for the knowledge and practice scores were calculated and participants were divided into two groups based on these. The first, high-level, group consisted of participants with scores above the median, while the second, low-level, group had scores below the median.
Sampling Type and Sample Size
Convenience sampling was used for this study. The required sample size was 1061, with significance at 95% and a 3% margin of error. The required sample size to conduct logistic regression was based on the rule of Events Per Variable criterion (EPV) ≥10, which depends on the number of participants in the smallest group and the number of independent variables included in the model. In the current study, three logistic regressions were conducted. Of these, the model with the largest number of independent variables and the smallest group was conducted to evaluate variables associated with vaccination intention, as 12 independent variables were included in the model and the smallest group (those who will not take the vaccine) was 176. Therefore, the required sample size to conduct logistic regression was met.
Statistical Analysis
Categorical variables were presented as frequencies and percentages, and continuous variables as means and standard deviations (SD). Stepwise (forward conditional) binary logistic regressions were conducted to explore variables associated with knowledge and protective practices. The following variables were included in the Knowledge model: age, sex, social status, monthly income, have children, education, ever had COVID-19, perceived seriousness of COVID-19, risk category, and area of residency. Furthermore, the practice model included the variables included in the knowledge model as well as participants’ knowledge score. Cronbach’s alpha was used to evaluate the internal consistency of the items used to compute the knowledge and practice scores. The minimum acceptable alpha for the practice score was 0.7, while for knowledge it was above 0.5 as lower alphas are expected for binary data.18 The computed Cronbach’s alphas were 0.80 and 0.59 for the practice and knowledge scores, respectively.
As only 7 participants answered “Maybe” to the question “If a vaccine is offered to you for COVID-19, are you willing to take it?” they were excluded from the analysis and stepwise (forward conditional) binary regression was conducted to evaluate variables associated with vaccine acceptance (Yes vs No), the model included all the variables listed in the practice model in addition to the participants’ practice level.
Results
Sample characteristics are presented in Table 1. A total of 1765 participants completed the questionnaire. Of these, 1542 had not been vaccinated against COVID-19 and were therefore included in the analysis. Almost half of the participants (50.3%) were aged between 18–29 years, and 40.1% were aged between 30–39 years. Overall, 56.7% of the participants were female and 82.9% of all participants were married, and 54.4% did not have children. Those with undergraduate degrees constituted 47% of the sample, with 4.8% having a high school education or less.
The health status of participants is outlined in Table 2. Most of the participants (88.4%) reported no chronic diseases. Approximately 49% of participants had a low risk of COVID-19 complications, with 37% having medium risk.
Knowledge about COVID-19 and vaccinations is shown in Table 3. Fever was the most well-known COVID-19 symptom (96.1%), followed by loss of smell and taste (92.0%). The least known symptom was chills (23.9%). Almost all the participants (98.2%) agreed that COVID-19 can be contracted by inhaling respiratory droplets from infected people. The most well-known protective measure against COVID-19 was social distancing (96.8%), followed by mask wearing (93.5%) using detergents (90.3%) and the least was washing hands with regular soap (86.9%).
Regarding attitudes and practices toward COVID-19 (see Table 4), 67.7% of participants reported having had a PCR test, with 49% of these tests being positive. Most participants (88.6%) were willing to take the vaccine once offered to them.
Participants were classified according to their scores in knowledge and practice into high-knowledge/practice groups and low-knowledge/ practice groups. Those who scored above the median (knowledge median=15 out of maximum possible score of 19; practice median=20 out of maximum possible score of 25) were placed into the high-level groups while those with scores below the median allocated to the low-level group. As shown in Table 5, females had significantly higher odds of being in the higher knowledge group when compared to male participants (OR=1.34, p < 0.01). Participant who had high school or less and university student had significantly lower odds of having a high knowledge level when compared to people with postgraduate qualifications (ORs=0.38 and 0.55, respectively, both p < 0.01). Those who answered “No” to have you ever been infected with COVID-19 had significantly higher odds of being in the high-knowledge group when compared with those who were infected (OR=1.82, p < 0.01). Low- and moderate-income groups had significantly less knowledge when compared with the high-income group (ORs=036 and 0.66, p-value < 0.01).
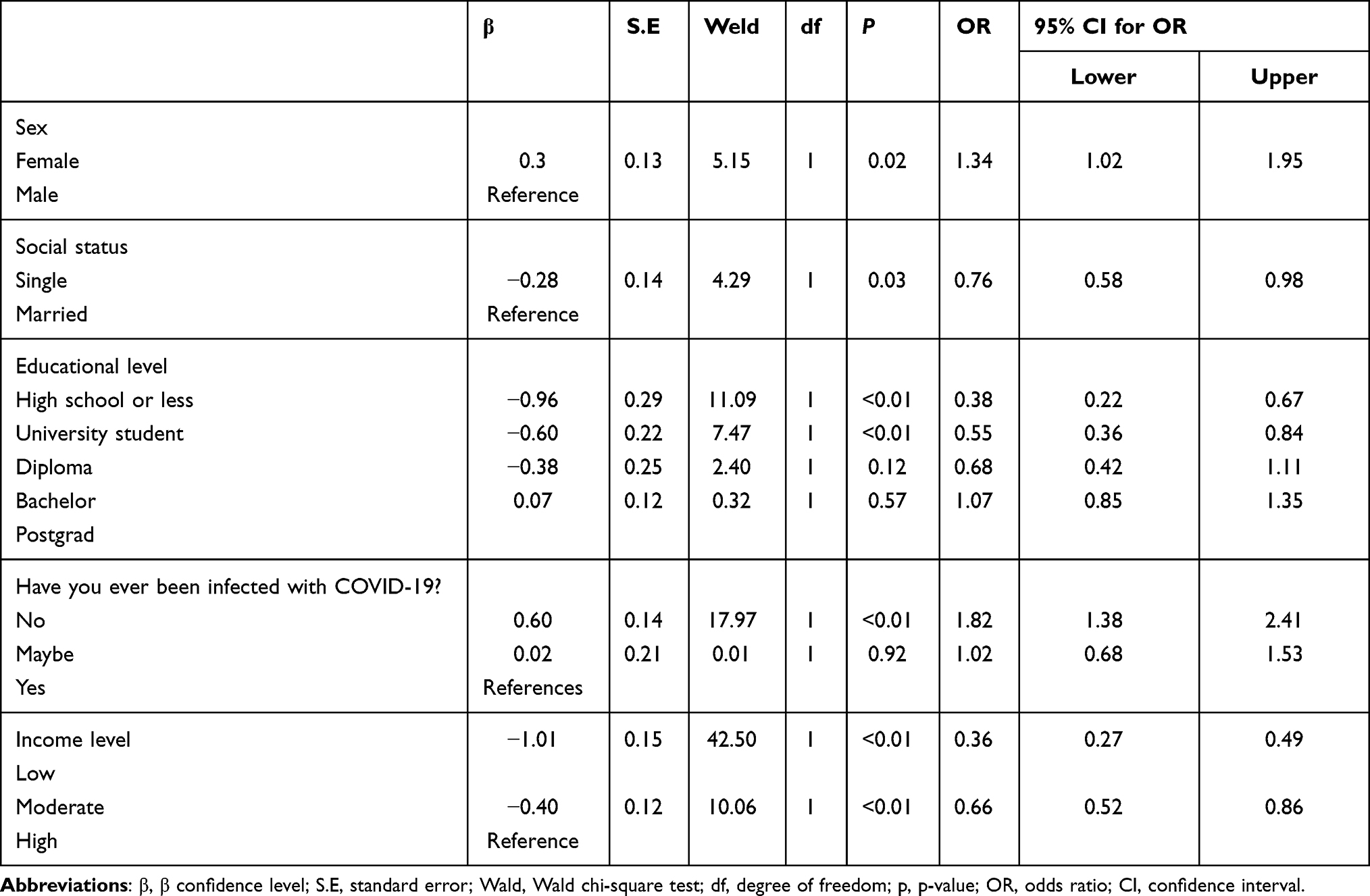 |
Table 5 Binary Logistical Regression Analysis of Variables Associated with Knowledge Score |
Binary logistical regressions between practice groups and sample characteristics indicated that females had significantly better practices when compared to males (OR=1.35, p = 0.04). Participants who had low knowledge had lower practice scores (OR=0.36, p < 0.01) and perceived degree of seriousness of COVID-19 was significantly associated with practice scores (OR=1.11, p = 0.02).
The result of the binary regression analysis (see Table 6), indicated that participants who reported never having been infected with COVID-19 had lower odds of accepting the vaccine compared to those who reported a confirmed COVID-19 infection (OR=0.53, p = 0.01). Low- and moderate-income groups had significantly lower odds of accepting the vaccine when compared with the high-income group (ORs=0.42 and 0.63, respectively, both p < 0.01). Similarly, those reporting high school or lower education were less willing to be vaccinated compared to participants with a postgraduate education (OR=0.33, p < 0.01). Finally, perceived degree of seriousness of COVID-19 was associated with readiness to take the vaccine (OR=1.30, P-value<0.01).
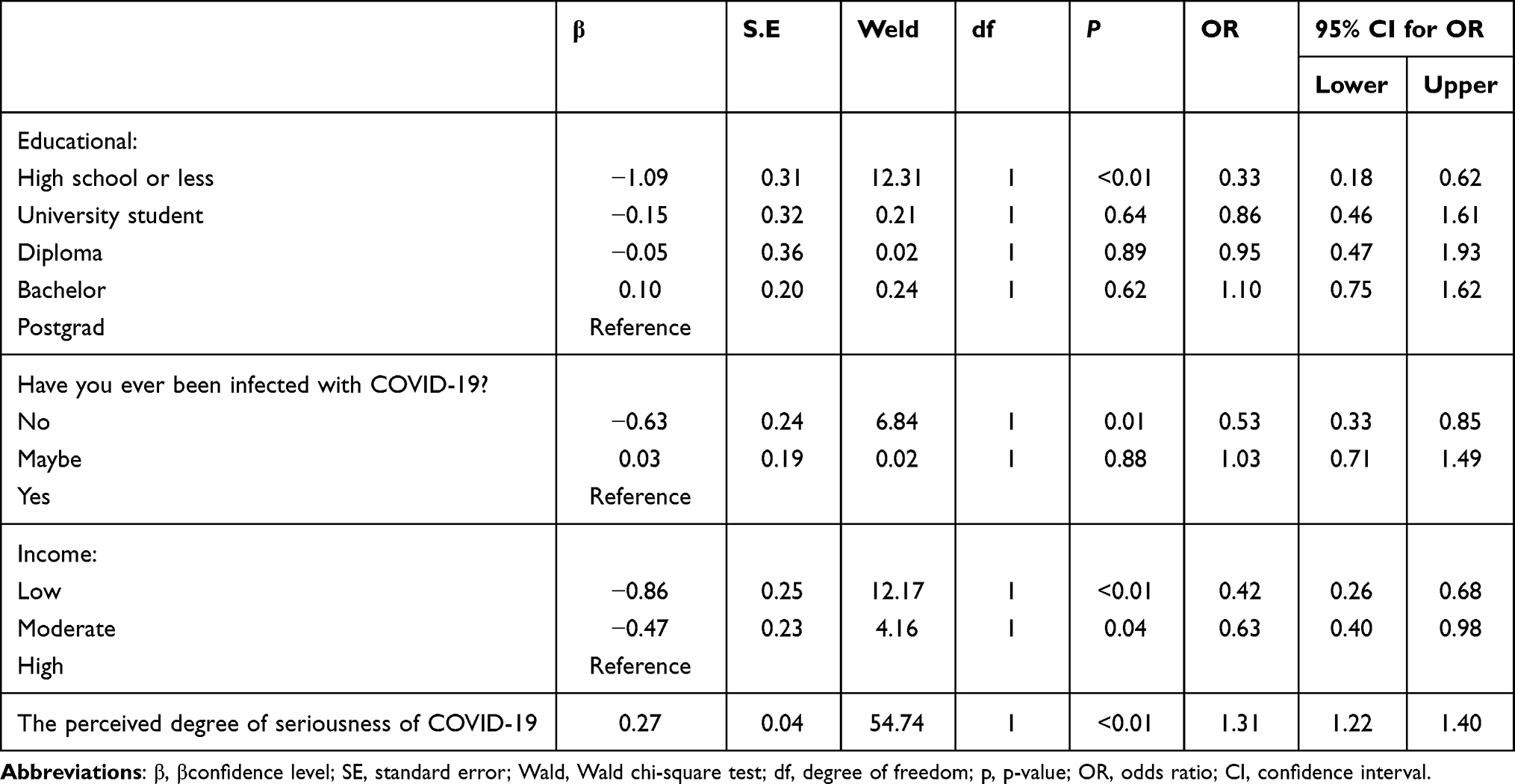 |
Table 6 Binary Logistical Regression Analysis of Variables Associated Vaccine Intention |
Participants gave reasons for vaccine refusal or hesitation (see Table 7). The most mentioned concerns were vaccine safety and side effects (90.35%), the (lack of) rigor in testing the vaccine (83.5%) and the need for more information about the vaccine (81.2%).
 |
Table 7 Reasons Participants Gave for Responding “No” or “Not Sure” Regarding Vaccination Intention for COVID-19 |
Discussion
Vaccinations have a major role in reducing the burden of infectious diseases. Vaccines for COVID-19 from several companies have recently been accepted by the FDA. However, access to these is still limited. Once the vaccine is widely available, establishing the population’s desire to be vaccinated as well as obstacles to vaccination could help increase vaccination rates.
Participants’ Knowledge About COVID-19
As this study was conducted between May and July 2021 when COVID-19 information was available worldwide, participants showed moderate to high knowledge scores. This replicates other studies conducted in Iraq and showed high knowledge about COVID-19.19,20 Similarly, several surveys undertaken globally have found high levels of knowledge concerning COVID-19, including surveys conducted in the general community in Malaysia,21 China,22 Saudi Arabia,23 and Jordan.24
Most of the participants in our survey were either graduates or postgraduates, with high incomes. They exhibited a good understanding of the symptoms of COVID-19, route of infection, and precautionary measures. They also knew that there is currently no cure for COVID-19. Media coverage, and the influence of the epidemic on social life, which pushes people to comply with health guidance, could explain the good awareness among participants. This study showed that female participants as well as married participants have better knowledge related to COVID-19. This corroborates earlier work conducted in Jordan about misconceptions concerning COVID-19 which found that women and single participants have more misconceptions.15 Like previous studies, females were more likely to regard COVID-19 as a significant health issue, and endorsed policies and measures enacted to protect against it.25 Similarly, we discovered that people who have children had greater knowledge than those who did not. This outcome could be attributed to parents’ increased anxiety for their children, which may have led to following the media more closely for information related to COVID-19. Several studies have22 reported a strong relationship between knowledge and demographic variables including gender, age, and occupation, which is parallel to our findings. Awareness was higher among educated people, as found in earlier investigations.26 In a study conducted in Egypt and Nigeria, participants had good awareness of COVID-19. Knowledge scores were linked to age group 18–39, college/degree, undergraduate education and participants’ backgrounds.27 A study conducted in Pakistan found a link between good health and education, and acceptable attitudes and practices.28 In line with our findings, the majority of Malaysians had good knowledge, positive attitudes and good practices related to COVID-19. These were attributed to successful healthcare and government campaigns.21 In the Middle East, numerous gaps in public knowledge related to COVID-19 have been highlighted, which suggests that health education be used to improve education.29 A Chinese study22 made similar recommendations. Thus, campaigns in Iraq to improve knowledge of COVID-19 should be designed to target people with lower levels of education and income.
Practice and Attitude Towards COVID-19
We found most respondents had a good COVID-19 preventive and control methods, implying that some of the responders’ practices were very good. This result is parallel to a study conducted in Mosul19 as well as those from Malaysia21 and in Jordan.24 Similarly, a Japanese study found that participants, particularly females and older participants, had good practices.30 This result might be attributed to the drastic measures that the Iraqi government made to reduce the spread of the disease. Being male and having less knowledge were predictors of poor practice scores, while perceived seriousness of COVID-19 was an indicator of high practice scores. These findings mimic previously reported correlations between knowledge and protective practices against COVID-19 which may be affected by several factors including COVID-19 induced anxiety.31 These findings replicate other studies that found females a greater sense of responsibility than similarly-aged males.22
Most of our survey participants had a positive outlook and stated that if offered a COVID-19 vaccine they are willing to take it, as well as taking a PCR test to make sure they are not infected. Positive attitudes have also been documented in Malaysian and Chinese.22,32 The positive sentiments reported in our study may be linked to the Ministry of Health’s excellent awareness campaign for the Iraqi people, with information on preventive measures is disseminated through newspapers and media.
Vaccination Acceptance
The Iraqi populace showed high acceptability of COVID-19 vaccines, according to the present study. The majority of participants (88.5%) stated that they intended to get vaccinated when one was available. This mirrors findings from a global survey (71.5% vaccination intention), as well as studies in Ecuador (97%), the United States (57%), France (76%), Saudi Arabia (64.7%) and China (91.3%).33
The Iraqi population’s high approval of COVID-19 vaccination shows a good understanding of the role of vaccines in pandemic control. The pandemic has had a significant influence on Iraqi’s work, income, and daily lives. Since the outbreak of COVID-19, Iraq has taken substantial efforts and applied public health initiatives to address these challenges, and these actions have significantly halted the disease’s spread.34 The high rate of COVID-19 vaccinations among Iraqi adults may be explained by the positive attitude and extensive knowledge of COVID-19 and concerns related to the impact of the pandemic, as they perceive greater benefits than risks to vaccination. Moreover, this study showed that the predictors of responding “no” regarding intent to be vaccinated were low education and income, not being infected by COVID-19, and not believing COVID-19 to be a serious disease. Educational and income levels were also reported in a study conducted in Malaysia on COVID-19 vaccine acceptance.35 Furthermore, more efforts should be made to vaccinate vulnerable people such as people with dementia.36
Barriers
Despite the high acceptance rate, barriers still remain in shifting from intention to acceptance. Reservations about vaccine efficacy, safety and side effect have been identified as a major impediment to vaccination decisions, particularly for newly launched vaccinations that have not been thoroughly evaluated in the real world. Similarly, previous work found that 13% of Australians reported that they would wait to see if any negative side effects occurred before agreeing to be vaccinated, although their acceptance rate was 67%.37 The vaccine hesitancy found in this study could be due to: concern about the vaccine (mainly the safety and the efficacy); the need for additional information on the vaccine and the availability of information about the vaccine, and a lack of trust in authority. Moreover, reservations about new vaccines, new emerging infectious diseases, and apprehension about pharmaceuticals have all been reported as likely to influence vaccine acceptance.38 The hesitancy we found may decrease, when a nonemergency vaccine becomes accessible. Importantly, once the safety of newly introduced vaccinations is equivalent to that of existing vaccines, this factor loses prominence in vaccination decision-making in favor of other factors such as effectiveness.39 This therefore necessitates a greater emphasis on vaccine safety in new vaccines, and in other vaccine characteristics, such as price and convenience, in order to increase uptake.
Studies conducted in the UK, France, and Australia found varying results on the effect of socio-demographic characteristics on pandemic vaccine acceptance.40–42 In our study, the main socio-demographic characteristics that influence vaccine hesitancy are working in a medical field, being infected before and knowing the seriousness of the disease. This replicates findings from previous work conducted in Jordan.14 Our findings can be used to develop targeted campaigns toward the effectiveness of the vaccination and immunization programs for people who are afraid of vaccines. Furthermore, information about vaccine safety should form part of a simultaneous health education campaign to reduce concerns about vaccine safety.43 To boost overall vaccine acceptance and public compliance in the event of future pandemics, various sectors, including health departments should undertake consistent education initiatives for non-pandemic infectious diseases such as influenza.43
Strengths and Limitations
This study had a large sample which reduces the impact of existing bias. Another noteworthy feature is that we measured KAP toward COVID-19 as well as vaccination intentions.
As this study is based on an online questionnaire, the results are prone to recall and selection bias. Previous work has shown, however, that online research is a cost-effective approach for generating a representative sample.44 When compared to face-to-face interviews, individuals who would otherwise be inaccessible can become participants, and a web-based approach also offers a safe and confidential space for respondents to respond.45 An additional limitation of the current study that it did not explore the impact of COVID-19 in many vulnerable subgroups including people with mental illness and. Previous studies have argued an urgent need to vaccinate such subgroups to improve their quality of life and wellbeing.35
Future Work
The government of Iraq, like many countries, has recently encouraged the vaccination of children 12 years and older. There is therefore a need to evaluate the of Iraqi parents’ intention to vaccinate their children, and to evaluate barriers behind any vaccination refusal/hesitancy.
Conclusion
In Iraq, the adult population showed a high acceptability of the COVID-19 vaccine. Vaccine hesitancy was higher among those with lower income education. Concerns regarding vaccination safety among the general population could frustrate future vaccine promotion efforts. Immunization strategies should be devised to reduce obstacles in vaccine and vaccination suitability to increase COVID-19 vaccine uptake. Furthermore, public health campaigns will be critical in reducing concerns regarding vaccine safety. These educational programs should target the high hesitancy group including low income and low education groups.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yu X, Sun X, Cui P, et al. Epidemiological and clinical characteristics of 333 confirmed cases with coronavirus disease 2019 in Shanghai, China. Transbound Emerg Dis. 2020;67(4):1697–1707. doi:10.1111/tbed.13604
2. WHO. Iraq: coronavirus Disease 2021 (COVID-19) - Weekly Situation Report (Week 29) (19 – 25 July 2021) [EN/AR] | reliefWeb mobile. Available from: https://m.reliefweb.int/report/3766143/iraq/iraq-coronavirus-disease-2021-covid-19-weekly-situation-report-week-29-19-25-july-2021?lang=es.
3. CDC. Certain Medical Conditions and Risk for Severe COVID-19 Illness. CDC. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
4. Tsatsakis A, Calina D, Falzone L, et al. SARS-CoV-2 pathophysiology and its clinical implications: an integrative overview of the pharmacotherapeutic management of COVID-19. Food Chem Toxicol. 2020;146:111769. doi:10.1016/j.fct.2020.111769
5. Karim SK, Taha PH, Amin NMM, Ahmed HS, Yousif MK, Hallumy AM. COVID-19-related anxiety disorder in Iraq during the pandemic: an online cross-sectional study. Middle East Curr Psychiatry. 2020;27(1):1–9. doi:10.1186/s43045-020-00067-4
6. Lami F, Rashak HA, Khaleel HA, et al. Iraq experience in handling the COVID-19 pandemic: implications of public health challenges and lessons learned for future epidemic preparedness planning. J Public Health (Bangkok). 2021;43(Supplement_3):iii19–iii28. doi:10.1093/pubmed/fdab369
7. Abed AH, Abdulwahid DA, Jassim HA. National health systems response to COVID-19 outbreak, Iraq an example. Med J Basrah Univ. 2021;39(1):1–6. doi:10.33762/mjbu.2021.130218.1071
8. Al-Jumaili MHA, Hamed AS. Coronavirus Disease-19: Outbreaks in Iraq. Dep Med Lab Tech Al-maarif Univ Coll Iraq; 2020.
9. Harrison EA, Wu JW. Vaccine confidence in the time of COVID-19. Eur J Epidemiol. 2020;35(4):325–330. doi:10.1007/s10654-020-00634-3
10. Al-Tammemi AB, Tarhini Z, Akour A. A swaying between successive pandemic waves and pandemic fatigue: where does Jordan stand? Ann Med Surg. 2021;65:102298. doi:10.1016/J.AMSU.2021.102298
11. Klugar M, Riad A, Mekhemar M, et al. Side Effects of mRNA-based and viral vector-based COVID-19 vaccines among German Healthcare Workers. Biol. 2021;10(8):752. doi:10.3390/BIOLOGY10080752
12. Riad A, Schünemann H, Attia S, et al. COVID-19 Vaccines Safety Tracking (CoVaST): protocol of a multi-center prospective cohort study for active surveillance of COVID-19 vaccines’ side effects. Int J Env Res Public Heal. 2021;18:15. doi:10.3390/ijerph18157859
13. UN Children’s Fund WHO. Iraq receives the first delivery of COVID-19 vaccines through the COVAX Facility; 2021. Available from: https://reliefweb.int/report/iraq/iraq-receives-first-delivery-covid-19-vaccines-through-covax-facility-enarku.
14. Al-Qerem WA, Jarab AS. COVID-19 vaccination acceptance and its associated factors among a middle eastern population. Front Public Heal. 2021;9:34.
15. Hammad AM, Hamed R, Al-Qerem W, Bandar A, Hall FS. Optimism bias, pessimism bias, magical beliefs, and conspiracy theory beliefs related to COVID-19 among the Jordanian Population. Am J Trop Med Hyg. 2021;1:1–11. doi:10.4269/ajtmh.20-1412
16. GL K, LL F. Description of the characteristics of pharmacist-based immunization services in North Carolina: results of a pharmacist survey. J Am Pharm Assoc. 2008;48(6):744–751. doi:10.1331/JAPHA.2008.07080
17. Al-Qerem W, Jarab AS, Qarqaz R, Al Hayek M. Attitudes of a sample of Jordanian young adults toward different available COVID-19 vaccines. Vacunas. 2021. doi:10.1016/j.vacun.2021.07.008
18. Cortina JM. What is coefficient alpha? An examination of theory and applications. J Appl Psychol. 1993;78(1):98–104. doi:10.1037/0021-9010.78.1.98
19. Saeed BQ, Al-Shahrabi R, Bolarinwa OA. Socio-demographic correlate of knowledge and practice toward COVID-19 among people living in Mosul-Iraq: a cross-sectional study. PLoS One. 2021;16(3):e0249310. doi:10.1371/journal.pone.0249310
20. Hussein NR, Naqid IA, Jacksi K, Abdi BA. Assessment of knowledge, attitudes, and practices toward COVID-19 virus among university students in Kurdistan region, Iraq: online cross-sectional study. J Fam Med Prim Care. 2020;9(9):4809. doi:10.4103/jfmpc.jfmpc_870_20
21. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. Tu W-J, ed. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
22. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
23. Al-Hanawi MK, Angawi K, Alshareef N, et al. Knowledge, attitude and practice toward COVID-19 among the public in the Kingdom of Saudi Arabia: a cross-sectional study. Front Public Heal. 2020;8:217. doi:10.3389/fpubh.2020.00217
24. Zaid AA, Barakat M, Al-Qudah RA, Albetawi S. Knowledge and awareness of community toward COVID-19 in Jordan: a cross-sectional study. Syst Rev Pharm. 2020;11(7):135–142.
25. Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci. 2020;117(44):27285–27291. doi:10.1073/pnas.2012520117
26. Huynh G, Nguyen TNH, Vo KN, Pham LA. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260. doi:10.4103/1995-7645.280396
27. Hager E, Odetokun IA, Bolarinwa O, Zainab A, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 Coronavirus Pandemic: a bi-national survey in Africa. PLoS One. 2020;15(7):e0236918. doi:10.1371/journal.pone.0236918
28. Tariq S, Tariq S, Baig M, Saeed M. Knowledge, awareness, and practices regarding the novel coronavirus among a sample of a Pakistani population: a cross-sectional study. Disaster Med Public Health Prep. 2020;1–6. doi:10.1017/dmp.2020.408
29. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
30. Muto K, Yamamoto I, Nagasu M, Tanaka M, Wada K. Japanese citizens’ behavioral changes and preparedness against COVID-19: an online survey during the early phase of the pandemic. PLoS One. 2020;15(6):e0234292. doi:10.1371/journal.pone.0234292
31. Riad A, Huang Y, Zheng L, Elavsky S. The associations of COVID-19 induced anxiety, related knowledge and protective behavior. Heal Psychol Res. 2021;9(1):24768. doi:10.52965/001c.24768
32. Geldsetzer P. Use of rapid online surveys to assess people’s perceptions during infectious disease outbreaks: a Cross-sectional Survey on COVID-19. J Med Internet Res. 2020;22(4):e18790. doi:10.2196/18790
33. Sallam M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccines. 2021;9(2):160. doi:10.3390/vaccines9020160
34. Jalil AT, Shanshool MT, Dilfy SH, Saleh MM, Suleiman AA. Hematological And serological parameters for detection of Covid-19. J Microbiol Biotechnol Food Sci. 2021;2021:e4229–e4229.
35. Marzo RR, Ahmad A, Abid K, et al. Factors influencing the acceptability of COVID-19 vaccination: a cross-sectional study from Malaysia. Vacunas. 2021. doi:10.1016/j.vacun.2021.07.007
36. Kennedy GJ. Advances in the epidemiology of Alzheimer’s disease: will empiricism improve the public’s health? Int J Geriatr Psychiatry. 2001;16(11):1028–1029. doi:10.1002/GPS.556
37. Eastwood K, Durrheim DN, Jones A, Butler M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med J Aust. 2010;192(1):33–36. doi:10.5694/j.1326-5377.2010.tb03399.x
38. Henrich N, Holmes B. The public’s acceptance of novel vaccines during a pandemic: a focus group study and its application to influenza H1N1. Emerg Health Threats J. 2009;2(1):7088. doi:10.3402/ehtj.v2i0.7088
39. Determann D, Korfage IJ, Lambooij MS, et al. Acceptance of vaccinations in pandemic outbreaks: a discrete choice experiment. PLoS One. 2014;9:7. doi:10.1371/journal.pone.0102505
40. Schwarzinger M, Flicoteaux R, Cortarenoda S, Obadia Y, Moatti J-P. Low acceptability of A/H1N1 pandemic vaccination in French adult population: did public health policy fuel public dissonance? PLoS One. 2010;5(4):e10199. doi:10.1371/journal.pone.0010199
41. Rubin GJ, Potts HWW, Michie S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK. Health Technol Assess (Rockv). 2010;14(34):183–266.
42. Seale H, Heywood AE, McLaws M-L, et al. Why do I need it? I am not at risk! Public perceptions towards the pandemic (H1N1) 2009 vaccine. BMC Infect Dis. 2010;10(1):1–9. doi:10.1186/1471-2334-10-99
43. Fenner Y, Garland SM, Moore EE, et al. Web-based recruiting for health research using a social networking site: an exploratory study. J Med Internet Res. 2012;14(1):e20. doi:10.2196/jmir.1978
44. Cantrell MA, Lupinacci P. Methodological issues in online data collection. J Adv Nurs. 2007;60(5):544–549. doi:10.1111/j.1365-2648.2007.04448.x
45. United Nations; Iraq. Iraq launches nationwide vaccination campaign to scale up immunity against COVID-19 [press release]; 2021. Available from: https://iraq.un.org/en/157219-iraq-launches-nationwide-vaccination-campaign-scale-immunity-against-covid-19.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.