Back to Journals » Risk Management and Healthcare Policy » Volume 15
COVID-19-Related Perceived Threat Following a Second Dose Vaccination in Adults with Chronic Illness: A Mixed-Method Study
Authors Gebeyehu DA ![]() , Sisay E, Molla B
, Sisay E, Molla B ![]() , Terefe B
, Terefe B ![]()
Received 7 March 2022
Accepted for publication 10 May 2022
Published 19 May 2022 Volume 2022:15 Pages 1101—1111
DOI https://doi.org/10.2147/RMHP.S365389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Daniel Ayelegne Gebeyehu,1 Endalkachew Sisay,2 Bizuneh Molla,3 Bewuketu Terefe1
1Community Health Nursing Department, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia; 2Clinical Psychology Department, University of Gondar Comprehensive Specialized Hospital, University of Gondar, Gondar, Amhara, Ethiopia; 3Department of Psychiatry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia
Correspondence: Bewuketu Terefe, Postal address: 196, Tel +2519-18-09-95-04, Email [email protected]
Background: In patients with comorbidities such as chronic illness, the severity and mortality risk of the disease (COVID-19) are high. Even if they are fully vaccinated, they should follow all precautions for unvaccinated people because the vaccine may not provide them complete protection. As a result, understanding their response to a threat is essential because knowing their threat level can be a good predictor of behavioral changes and health-protective behaviors.
Methods: An institution-based cross-sectional mixed-method study design was used at the University of Gondar specialized hospital from May 1 to June 30, 2021. An interviewer-administered questionnaire was used for the quantitative, and tape recorders, field notes, and memos were properly taken during the in-depth interviews for the qualitative data. Multivariable logistic regression with consideration of adjusted odds ratio of 95% confidence interval and p-value of 0.05% was used for statistical significance.
Results: The study enrolled 239 people, with a 96% response rate, ranging from 24 to 67 years, with the majority (57.9%) male. Even after receiving the second dose of AstraZeneca, nearly half (46.5%) of participants with a chronic illness perceived a threat to COVID-19. The participant’s age ranges from 24 to 34 years [3.24 (AOR= 3.24 (95% CI: 1.08, 9.68))], patients who are student [2.38 (AOR= 2.38 (95% CI: 1.12, 5.06))], participants applying the recommended behavioral response [2.36 (AOR=2.36 (95% CI: 1.16, 4.81))] and duration of illness ranged from four to six-year [3.17 (AOR=3.17 (95% CI (1.05, 9.58))] were statistically associated with perceived threat.
Conclusion: Most people with chronic illnesses do not see the disease as a threat. Particular emphasis should be placed on creating awareness programs and disseminating information through media on prevention, and ongoing health education is strongly advisable.
Keywords: COVID-19, mixed approach study, patient with chronic illness, perceived threat, 2nd dose-vaccinated, vulnerable
Introduction
Coronavirus, which rightly belongs to the Coronaviridae group, is a widespread virus that parasitizes various animal species, including bats, camels, and cattle.1 The World Health Organization (WHO) named a new strain COVID19 that belongs to the same clade under the subgenus sarbecovirus of the subfamily Orthocoronavirinae.2 COVID19, previously called 2019nCoV,2,3 infects humans, animals, birds, and rodents, causing respiratory, digestive, hepatic, and central nervous system problems. MERS-CoV, SARS-CoV,4 and now this new virus dubbed (SARSCoV2). This virus infects humans by many mechanisms and spreads from human to human.5
Since the World Health Organization (WHO) declared a COVID-19 outbreak on December 31 in Wuhan, China,6 this disease has spread steadily worldwide. And now there are over six million infected people and a quarter million deaths.7 After the country’s vaccination rate was once the envy of the world and restrictions were lifted, the country was far ahead of many other countries. With the Delta variant surging, the movement of freedom is coming to an end. According to WHO, the Delta variant is now present in more than 111 countries, and we anticipate that it will soon be the dominant COVID-19 strain circulating globally; deaths are also on the rise as the virus continues to evolve, resulting in more transmissible variants.8
Countries paid particular attention to infected patients and frontline health workers, putting the problem first.9 Furthermore, people with chronic illnesses received valuable attention. They are advised to use behavioral precautions to prevent COVID-19 because the chronic disease can make them more likely to become severely ill from COVID-19.10
The COVID-19 pandemic has had both direct and indirect effects on people with chronic diseases; in addition to morbidity and mortality, high rates of community spread and various relief efforts, including stay-at-home recommendations, have disrupted lives and created social and economic hardships.11
Because human behavior has a significant impact on disease transmission and extinction (5), understanding how a population with a chronic condition responds to a threat is critical, as fear is a strong predictor of behavioral changes and health-securing behaviors.12,13 As conceptualized, protection motivation theory and the health belief model predict health-related behaviors about mechanisms of fear appeal, having perceived threat, perceived vulnerability/susceptibility, perceived efficacy/benefits, and barriers are all critical components for promoting protective behaviors.14,15 Negative emotions (eg, perceived threat) are also associated with good preventive behaviors, as reported by Rubin et al 2009; Seton and Raude 2010; and Goodwin et al 2011.16–18 Older people with different comorbid diseases or more vulnerable are more likely to be afraid of the covid-19 pandemic than the rest of the community; thus, effective infection prevention strategies and communications are needed.9,19 They emphasize, however, that the most desirable outcome is a careful balance of worry and just enough fear to change people’s behavior without the damaging effects of public panic.
According to the CDC, people who have a comorbid medical condition may not be fully protected from contracting the diseases even if they are fully vaccinated;20 they should continue to take all precautions recommended for unvaccinated people. Thus, to reduce morbidity and mortality, avoid a surge in demand on the healthcare system, and shortages of equipment such as ventilators needed to care for critically ill patients, people with chronic illnesses should be aware of the current pandemic, as the vaccine may not provide them with complete protection from contracting the disease, and further research is needed to determine how long COVID-19 vaccines can be used. Furthermore, even if vaccinated, individuals with chronic comorbidities should avoid contact and take appropriate precautions to prevent potential transmission.21
This study aims to shed light on the predictive value of perceived threat and its determinants in predicting fear of COVID-19, particularly the delta strain, following the second dose of its vaccine (AstraZeneca) among the second dose of its vaccine (AstraZeneca) vulnerable population. As such, it aims to provide guidance for effectively developing public health strategies in these populations and identify potential fear-arousal techniques for using behavioral interventions to reduce further declines in cases, hospitalizations, and deaths that will occur, particularly in the third wave.
Methods
The Study Design, Area, and Population
An institution-based cross-sectional quantitative and qualitative study design was conducted from May 1 – to June 30, 2021. The research was conducted at the University of Gondar Comprehensive Specialized Hospital /UOGCSH/, located northwest of Addis Ababa, Ethiopia’s capital.
The hospital is 750 kilometers from Addis Ababa. It provides services to approximately five million people in its northwest region.22 In several departments, the hospital offers inpatient and outpatient medical services. It has over 1000 patient beds and serves over 200,000 patients each year.23 According to reports from the COVID-19 vaccine room, approximately 900 people received their second dose vaccine (AstraZeneca) in the previous month.
All individuals who received their COVID-19 vaccine were considered a source population. In contrast, participants with a chronic illness who welcomed their second doses of the AstraZeneca vaccine and were available during the data collection period were considered study participants.
Inclusion and Exclusion Criteria
All individuals aged 18 and older,24 diagnosed with Hypertension (ICD-10-CM I10), Diabetic Mellitus (ICD-10-E08-E13), HIV/ADIS, and Chronic heart disease (ICD-10-CM I51.9), who received their second doses of COVID-19 vaccine, who could provide written informed consent to participate in the study and attending chronic disease clinic for the follow-up, were included; patients who were acutely ill were excluded because they could not respond to the questions correctly.
Sampling Technique and Procedure
For the quantitative analysis, a single population proportion formula is used, with the following statistical assumptions: the prevalence of perceived threat was set at 50% (because no similar study has been conducted in the country or on the continent among this segment of the population after receiving a second dose,25 95% confidence interval, 5% degree of precision, and 10% non-response rate resulted in a total sample size of 384; however, because our source population was less than 10,000, we used the correct formula, and the final sample size was 238. To enroll the participants, a simple random sampling technique was used.
The sample size for the qualitative analysis was determined by data saturation. As a result, approximately 15 people were chosen for the study. Purposive sampling was used to select participants, and maximum variation in age, literacy, and health condition was considered.
Data Collection Tools and Procedures
Questionnaires were translated (from English to Amharic). These questionnaires were adapted from previously published pandemic-related articles (19–21), and the tools were divided into four sections: (1) Socio-demographic variables, (2) Clinical variables, (3) psycho-social and other related variables, (4) behavioral precautions, and (5) perceived threat. To collect all of the data, face-to-face interviews were used.
In terms of perceived threat, the questionnaire was adapted from a previously developed SARS risk perception questionnaire26 with some changes to address the COVID- 19. The following questions are included: Even if you have received a second dose of the COVID-19 vaccine; (1) Severity (“How serious (on a scale of 1 to 5) would the disease be for you if you got it?”; (2) Vulnerability (“How likely do you think it is that you will develop or contract COVID-19 in the next year compared to other people your age in the town; much less likely (1) too much more likely (5); (3) Comparative vulnerability (“How likely do you think it is that you will develop or contract COVID-19 in the next year compared to other people your age in the town; much less likely (1) too much more likely (5). As a result, those who scored higher than the mean (7.62) were deemed a threat to COVID-19.
The Multidimensional Scale of Perceived Social Support was used to assess social support (MSPSS). MSPSS is a self-report measure that includes 12-items rated on a seven-point Likert scale to determine an individual’s perceived level of social support from family, friends, and significant others. Participants with mean scale scores ranging from 1 to 2.9, 3 to 5, and 5.1 to 7 could be classified as having low, moderate, or high social support, according to the MSPSS.27
The WHO’s behavioral precautions were used to determine behavioral questions for those who received the vaccine, including the second dose;28 the questions are as follows: (1) Keep at least one meter away from others; (2) wear a mask, especially in crowded, closed, and poorly ventilated environments; (3) wash your hands frequently; and (4) When you are at home with others, make sure there’s plenty of ventilation, such as by opening a window. As a result, if a participant reported at least one “No” answer to the questions above, they were labeled as engaging in poor preventive practices.
To ensure the quality of the data, a pre-test was administered to 10% of the study participants at the Poly health center in Gondar before data collection. Cronbach’s alpha was used to perform the reliability test for perceived threat questionnaires, and the initial value was 0.74. In addition, data collectors received three hours of training in interviewing techniques using possible COVID-19 preventive mechanisms and checklist completion. Three nurses with bachelor’s degrees were assigned to collect data, and two psychiatry professionals with a master’s degrees were assigned to supervise. Finally, the questionnaires’ completeness was checked regularly.
Data Processing and Analysis
To conduct the quantitative analysis, data were coded and exported into a Statistical Package for Social Science (IBM-SPSS) Version 21.0 for further research using EPI info version 7. The study’s findings were presented using data summary measures such as texts, tables, and figures. Binary logistic regression analysis was used to identify the independent variables associated with the dependent variables. As a result, variables with a p-value of less than 0.2 in the bivariable research were entered into the multivariable regression model to control confounder effects and identify significant factors. Finally, variables with a p-value of 0.05 in the multivariate analysis were considered statistically significant; data interpretation was made using the adjusted odds ratio and p-value with a 95% confidence interval.
Field notes and memos were properly taken during in-depth interviews for qualitative data. The audio recordings of in-depth interviews were transcribed in the local language and translated to English. Thematic analysis was used to analyze the qualitative data by thematizing individuals’ ideas, feelings, and perceptions of the susceptibility and severity of the covid-19 pandemic.
After familiarizing ourselves with the data, we created codes, generated themes, reviewed themes, and defined and named pieces. Finally, in writing up steps, we wrote and explained the main takeaways of the given data.
Results
Demographic Variables
From 239 people invited, 228 responded to the questionnaires, yielding a 96% response rate. The ages of the participants ranged from 24 to 67 years; the majority (57.9%) were male; the large proportion (59.2%) was an Orthodox Christian (Table 1).
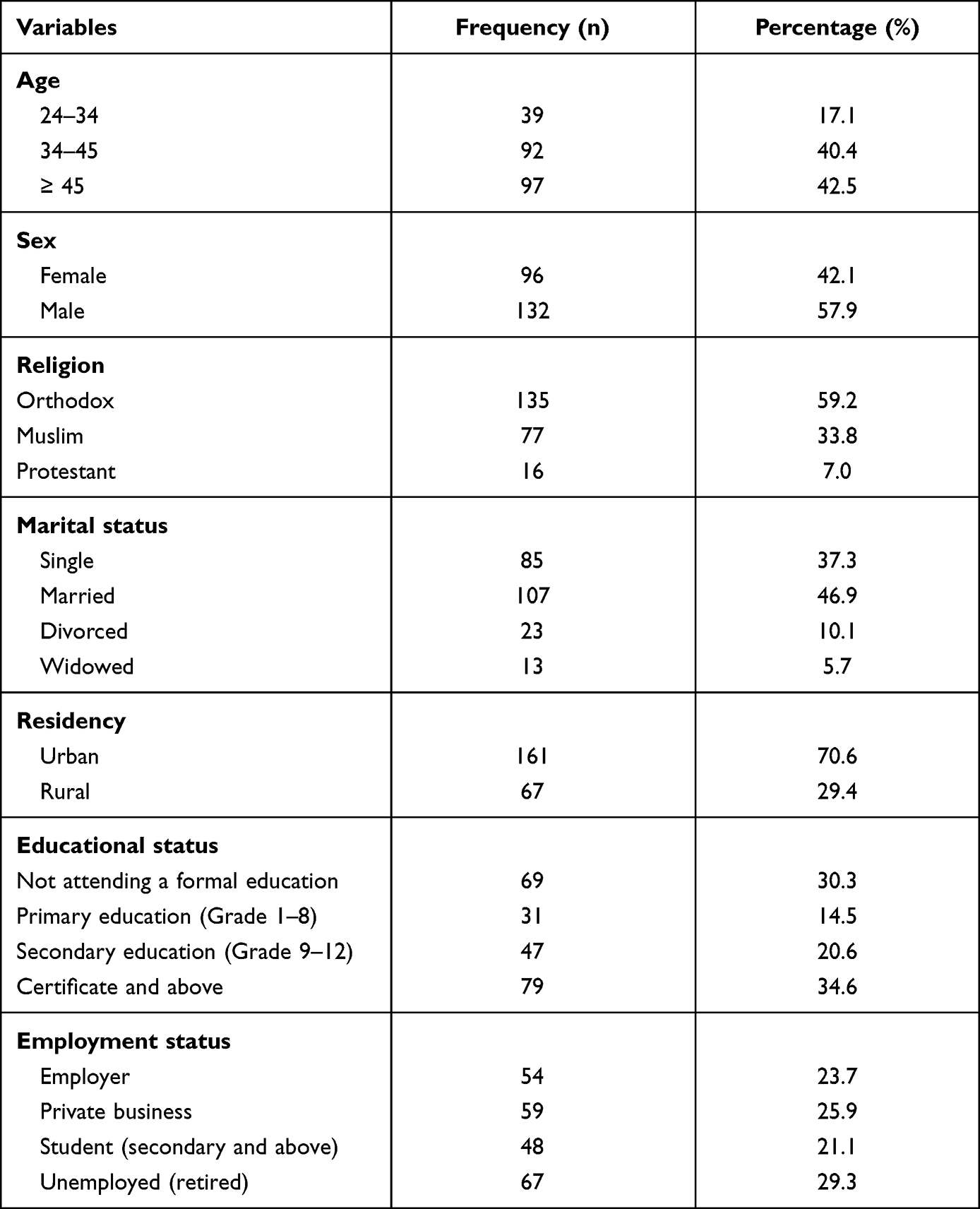 |
Table 1 Demographic Characteristics of the Participants with a Chronic Illness at University of Gondar Specialized and Comprehensive Referral Hospitals, 2021 |
Participants Clinical Variables
As shown in Figure 1, less than half of the participants (43.9%) were diagnosed with Hypertension.
 |
Figure 1 Diagnosis of Chronic illness among patients visited University of Gondar specialized and comprehensive referral hospital, 2021. |
The total duration of illness ranged from one to ten years, with an average of 3.7 (SD 2.58) years. More than half of the 129 (56.6%) had been sick for 1 to 3 years (Figure 2).
 |
Figure 2 Duration chronic illness among patients saw University of Gondar specialized and comprehensive referral hospital, 2021. |
Participants Psycho-Social and Another Related Variable
The status of patients with good social support, a large proportion (60.5%) of the study participants had good social support, and more than one-third of the respondents received health education about the vaccine (AstraZeneca), its effect, and behavioral precautions that should be taken after receiving the second-dose of it.
The Behavioral Response Among People with Chronic Illness to the COVID-19 Pandemic
After receiving a second dose of the COVID-19 vaccine, only 96 (42.1%) of the participants had practiced the required behavioral response recommended by WHO to protect themselves from the COVID-19 pandemic.
We assessed qualitatively why participants had a typical behavioral response to COVID-19 after receiving two doses of its vaccine; we discovered that people are having difficulty adapting to the new COVID-19 preventive measurements for a variety of reasons, one of which was started by one of the participants as follows:
We Ethiopians, for example, walk together, share a common dish, celebrate together, and attend wedding and funeral ceremonies with large crowds. As a result, because I am a member of society, abandoning societal norms and values in the face of the corona pandemic is difficult for me. I even hug and kiss my relatives and friends from other cities or the countryside when they visit.
The other participant expresses his thoughts and feelings in the following way:
When I don’t greet my friends or colleagues by holding their hands and hugging them tightly, I don’t feel good. I can’t leave someone without shaking his hand, even if he has the disease. Unless God wishes to punish the individual, the disease is less contagious. I came to this conclusion after my COVID—19 sickened neighbor fell out of his car while driving and was injured in his extremities; because I have experience with traditional treatments such as massage, I was the first to give him homemade treatment massaging his injured part with butter. Even though he was taking possible disease-treating medications, I was not susceptible to developing COVID-19 symptoms after treating him. As a result, I saw this pandemic as GOD’s punishment.
A Perceived Threat to COVID-19 in Adults with Chronic Illness
After receiving the second dose of the COVID-19 vaccine (AstraZeneca), slightly less than half [106 (46.5% (95% CI: 40.4%, 52.6%))] of patients with a chronic illness had a perceived threat regarding the COVID-19 pandemic.
The above quantitative result is also supported by the qualitative aspect of the current study, which found that this group of people percent lived minor threats from the pandemic. The first question assessed their attitude toward the vaccine and the danger. As a result, two participants have a higher level of trust in the vaccine than the others as they said,
Although I am not a medical professional, I enjoy asking questions, consulting with medical professionals, and reading a variety of materials. So, I learned a little bit about vaccines, and when I received them (first and second doses), I had complete faith in them as a preventative measure against the current pandemic. I’m confident that the vaccine will provide complete protection for me. Some claim that the vaccine does not work, but this is false. I would inform them that the vaccine is completely safe and effective and keep them from contracting the disease if I came across them. It would kill me if I contracted the disease, so I was quickly vaccinated. As a result, now that I’ve received two doses of its vaccine, I’m no longer at risk of contracting the disease.
Similarly, but a minor slight threat, the other interviewee, stated,
The coronavirus disease will not attack me, so I don’t feel afraid because I took the vaccine, which will protect me up to 80% from the disease; thus, to fill out the remaining 20%, I always keep my hygiene and use a face mask when I go to the bus station, taxi, etc.
In response to a question, the other participant stated,
Well, we live in cramped quarters like any other society. We make friends wherever we go, so even though I’m immunized, I’m still at risk of contracting the disease. This is a warning to be wary. However, I don’t always take the necessary precautions. It is difficult to be cautious all of the time, but it is possible with God’s help.
The rest of the participants’ perspectives on the COVID-19 pandemic, vaccines, and other preventive measures differed markedly from scientific facts. They also received the vaccine due to peer pressure because it is their duty and differentiated other reasons. For example, when asked, one participant stated,
I don’t believe in the vaccine because it doesn’t prevent me from developing the current pandemic. I assumed that the vaccine would provide no immunity; instead, I should have faith in God. Except for the harm caused by vaccination, I received no benefit.
The other participant provided a different response. He responded,
This is not because I believe in the vaccine’s results, but because I’ve heard that if I go abroad for work or other medical treatments, they won’t accept me if I don’t have the vaccine; because I don’t want to be bothered. But I’m not convinced by the vaccine. Instead, the best and most long-lasting solution is to use other preventive measures (face masks, sanitizer, and social distancing) and fasting and praying to the almighty God. Vaccination has only negative side effects such as headaches and fatigue. Furthermore, I am not concerned about the pandemic.
In conclusion, even if they have been diagnosed with a chronic illness, most participants have no fear of the disease. The participants were also strongly aversion to the vaccine and its side effects. Many people did not take the vaccine because they were afraid of the side effects. This indicates that action must be taken at the community level to overcome and create a threat for better prevention. Furthermore, participants’ most common side effects were headache, vomiting, fever, unconsciousness, and extremity tiredness.
Factors Associated with Perceived Threat After Receiving the Second Dose
Bi-variable and multivariate analyses were conducted to test the association between independent variables and the perceived threat to the COVID-19 pandemic. Variables that had a p-value of ≤0.2 in the bi-variable analysis, such as age, educational status, Occupation, Residency, Duration of Illness, health education from health professionals, and Behavioral response, were run in the multivariable analysis to test the adjusted odds ratio. Finally, in the multivariate analysis, the participant’s ages ranged from 24 to 34 years, students’ age, participants who had good behavioral practice, and duration of illness ranged from four to six-year were statistically associated with having a perceived threat of COVID-19 (Table 2).
 |
Table 2 Bi-Variable and Multivariable Factors Associated with Perceived Threat Among Patients with Chronic Illness Attending the University of Gondar Specialized and Comprehensive Referral Hospitals, 2021(n=228) |
After receiving the total dose, the odds of experiencing a perceived threat to COVID-19 were roughly three times higher among participants aged 24 to 34 years (AOR= 3.24 (95% CI: 1.08, 9.68)) than among participants aged 45 and above. The odds of experiencing a perceived threat to COVID-19 were 2.38 (AOR= 2.38 (95% CI: 1.12, 5.06) higher among students than those employed. Furthermore, the odds of experiencing a perceived threat from the COVID-19 pandemic were 2.36 (AOR= (95% CI: 1.16, 4.81)) times higher among participants who followed the practices. The likelihood of experiencing a perceived threat was 3.17 (95% CI: 1.05, 9.58) times higher among participants with four to six years of illness than those with six or more years of disease (Table 2).
Discussion
According to the current study, 46.5% of Patients with Chronic Illness were detected to have perceived threats after receiving the second dose of the COVID-19 vaccine; this implies that it is a significant public health concern and necessitates a well-designed and comprehensive strategy; because, according to the CDC, People with moderately to severely compromised immune systems may not build the same level of immunity;29 thus, the CDC advises this segment of the population that an additional dose of mRNA COVID-19 vaccine is required for better health.
The current study found that experiencing a perceived threat to COVID-19 after receiving a second dose of the COVID-19 vaccine was higher in inpatient age ranging from 24 to 34 years. Even though social theory states that individual behaviors reflect the social and environmental advantages and disadvantages of the times they lived, young people are eminently flexible and responsive to social conditions. Still, as their age increases, their flexibility gradually decreases.30,31 Moreover, Jon A. Krosnick Duane E Alwin believed that people experience more major life changes between the ages of 18 and 25 than at any other point in the life cycle and that they are more likely to exhibit higher levels of attitude change than older adults, spawning intervention strategies that are essential components of successful public health programs.32–34 However, in our study, most participants were 35 and older, indicating that this event may have resulted in the highest prevalence of having a poorly perceived threat. As a result, government policies aimed at combating COVID-19 should be reconsidered, with a greater emphasis placed on this population segment.
The study discovered that participants who were secondary and above level students were nearly three times higher than those who were employed to perceive a threat. Given that education is related to attitude-report precision,31 those who perceive a threat may exhibit better protective behavior because they are more in touch with current information.35,36 Furthermore, Rubin et al discovered that people with no educational qualifications were more likely to adopt avoidant behaviors than protective behaviors during the flu pandemic.34 In our study, half of the participants had no formal education. Thus, exercising the required behavioral response to prevent COVID-19 after being fully vaccinated may be less than expected, allowing them to acquire the virus more quickly than those with formal education. As a result, the government’s (Ethiopian Ministry of Health) current preventative measures recommendations may become ineffective. The government (Ethiopian Ministry of Health) should focus on this population and provide current information with these factors in mind.
The study found that participants who had a shorter duration of illness after being diagnosed with a chronic disease were more likely to experience a perceived threat than those who had a long-term sickness. This could be explained by the fact that they have had a chronic disease for a more extended period, impacting their health, economic, and social domains [30] and poor drug response associated with neurodegenerative aspects.37 As a result, they may struggle to implement the recommended behavioral responses to the pandemic.
Another intriguing finding from this study was that the WHO-recommended behavioral responses of those who received the second dose of the COVID-19 vaccine were significantly related to the presence of a threat. The individual’s belief in their ability to control the situation is likely to have a significant impact on the perceived threat level in a case at any given time;38 As a result, there must be a perceived threat and a response to act adaptively.39 Furthermore, according to the Fear-Arousing Communications stage model and the assumption of dual-process theories, when the risk is trivial, and individuals do not feel vulnerable, they are unlikely to invest much effort in thinking about the contents of the communication that aids in the early detection of the pandemic.39,40 Despite this, only slightly more than one-third of study participants perceived a threat from the COVID-19 pandemic, indicating that the responsible body should emphasize fear-inducing communications to ensure people feel vulnerable to the portrayed risk.41 As evidenced by the studies conducted in various settings, communication could effectively change individuals’ health-harming perceived threats, worry, and behaviors.39,41
This study has provided a timely wealth of information. It first looks at how vulnerable patients perceive COVID-19 risk and adjusts their behaviors based on their disease status, even if they have been vaccinated; it has implications for general patient care and public health. However, the study has a chance of being exposed to interviewer bias, which could affect its quality. The study could be more representative if it were conducted in multiple institutions with a large sample size, which would improve the quality of this paper. Because the pandemic is new and vaccine coverage is not fully addressed in the country, the study only focused on those who received the AstraZeneca vaccine; thus, there may be a difference in the level of experiencing a threat between the vaccines in patients with chronic illnesses.
Conclusion
More than half of those suffering from chronic illnesses did not see the disease threat. Young age (18–24), secondary and higher-level students, people with good behavioral practices, and a four to six-year illness duration were all statistically significant predictors of a perceived threat. Particular emphasis should be placed on creating awareness programs and dissemination through mainstream media. Because these are the primary risk factors, data on COVID-19 prevention should be provided to older adults and those unemployed as soon as possible. Similarly, ongoing health education about the severity of the problem is highly recommended to ensure that people feel vulnerable to the portrayed risk. Patients with chronic illnesses are highly susceptible to developing the disease even if vaccinated.
Abbreviation
AOR, adjusted odds ratio; CD, chronic disease; CI, confidence interval; COR, crude odds ratio; OR, odds ratio; UOG, the University of Gondar; WHO, World Health Organization.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Research Ethical Committee of the University of Gondar. A permission letter to conduct the study in the Psychiatric clinic was also obtained from the UOGSCH Psychiatric clinic. In addition, written informed consent was obtained from each study participant by considering their health status; besides, only those who received the second dose of the COVID-19 vaccine were enrolled in the study. Ahead of the data collection, participants were briefed about the study’s objectives, benefits, possible risks, and voluntary participation. Initially, they were informed about their right to withdraw from the study at any time during the interview process. When they were informed about their right to remove, they agreed to leave the study whenever they felt uncomfortable Confidentiality was maintained by avoiding the name and other identifiers of the participants. During the interview, maximum COVID-19 protective measurements were secured to minimize the disease transmission from the patient to the data collector and vice versa. All the methods and ethical issues of the research were conducted following the declaration of Helsinki.
Acknowledgments
The authors express their gratitude to both the data collectors and the study participants.
Author Contributions
All authors contributed significantly to work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; participated in the drafting, revising, or critical review of the article; gave final approval of the version to be published; agreed on the journal to which the report was submitted; and agreed to be accountable for all aspects of the work.
Disclosure
All authors declare that there are no conflicts of interest.
References
1. Biscayart C, Angeleri P, Lloveras S, Chaves T, Schlagenhauf P, Rodríguez-Morales AJ. The next big threat to global health? 2019 novel coronavirus (2019-nCoV): what advice can we give to travellers?–Interim recommendations January 2020, from the Latin-American Society for Travel Medicine (SLAMVI). Travel Med Infect Dis. 2020;33:101567. doi:10.1016/j.tmaid.2020.101567
2. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–733. doi:10.1056/NEJMoa2001017
3. Chen Y, Liu Q, Guo D. Emerging coronaviruses: genome structure, replication, and pathogenesis. J Med Virol. 2020;92(4):418–423. doi:10.1002/jmv.25681
4. Sousou J. Middle East respiratory syndrome coronavirus: what do we know? J Nurse Pract. 2015;11(1):131–134. doi:10.1016/j.nurpra.2014.09.019
5. Wu G, Yang P, Xie Y, et al. Development of a clinical decision support system for severity risk prediction and triage of COVID-19 patients at hospital admission: an international multicentre study. Eur Clin Respir J. 2020;56(2):2001104.
6. World Health Organization. Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19: Interim Guidance, March 21 2020. World Health Organization; 2020.
7. World Health Organization WHO Coronavirus (Covid-19) Dashboard: Available from: https://covid19.who.int/.
8. United Nations Early stages’ of COVID third wave, amid Delta surge: WHO chief Available from: https://news.un.org/en/story/2021/07/1095882.
9. Cawcutt KA, Starlin R, Rupp ME. Fighting fear in healthcare workers during the COVID-19 pandemic. Infect Control Hosp Epid. 2020;41(10):1192–1193. doi:10.1017/ice.2020.315
10. Centers for Disease Control and Protection: Covid-19 People with Certain Medical Conditions Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
11. Nicola M, Alsafi Z, Sohrabi C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg Open. 2020;78:185–193. doi:10.1016/j.ijsu.2020.04.018
12. Tannenbaum MB, Hepler J, Zimmerman RS, et al. Appealing to fear: a meta-analysis of fear appeal effectiveness and theories. Psychol Bull. 2015;141(6):1178. doi:10.1037/a0039729
13. Cho H, Lee J-S, Lee S. Optimistic bias about H1N1 flu: testing the links between risk communication, optimistic bias, and self-protection behavior. Health Commun. 2013;28(2):146–158. doi:10.1080/10410236.2012.664805
14. Norman P, Boer H, Seydel ER, Mullan B. Protection motivation theory. Predict Chang Health Behav. 2015;16:70–106.
15. Champion VL, Skinner CS. The health belief model. Health Behav Health Educ. 2008;4:45–65.
16. Gare A. The palgrave encyclopedia of the possible. 2020.
17. Goodwin R, Gaines SO, Myers L, Neto F. Initial psychological responses to swine flu. Int J Behav Med. 2011;18(2):88–92. doi:10.1007/s12529-010-9083-z
18. Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: cross-sectional telephone survey. BMJ. 2009;339:b2651.
19. Kaplan AK, Sahin MK, Parildar H, Adadan Guvenc I. The willingness to accept the COVID‐19 vaccine and affecting factors among healthcare professionals: a cross‐sectional study in Turkey. Int J Clin Pract. 2021;75(7):e14226. doi:10.1111/ijcp.14226
20. Center for Disease Control and Protection : Covid-19: Stay Up to Date with Your COVID-19 Vaccines Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html.
21. Tran VT, Ravaud P. COVID-19–related perceptions, context and attitudes of adults with chronic conditions: results from a cross-sectional survey nested in the ComPaRe e-cohort. PLoS One. 2020;15(8):e0237296. doi:10.1371/journal.pone.0237296
22. Tefera B, Assefa M, Abebe B, Rauch D. Patterns of cancer in University of Gondar Hospital: North-West Ethiopia. J Oncol Med Pract. 2016;1:106.
23. Abdela OA, Bhagavathula AS, Getachew H, Kelifa Y. Risk factors for developing drug-related problems in patients with cardiovascular diseases attending Gondar University Hospital, Ethiopia. J Pharm Bioallied Sci. 2016;8(4):289.
24. Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health challenge. Lancet. 2007;369(9569):1302–1313. doi:10.1016/S0140-6736(07)60368-7
25. Naing L, Winn T, Rusli B. Practical issues in calculating the sample size for prevalence studies. Arch Orofac Sci. 2006;1:9–14.
26. Brug J, Aro AR, Oenema A, De Zwart O, Richardus JH, Bishop GD. SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg Infect Dis. 2004;10(8):1486. doi:10.3201/eid1008.040283
27. Bruwer B, Emsley R, Kidd M, Lochner C, Seedat S. Psychometric properties of the multidimensional scale of perceived social support in youth. Compr Psychiatry. 2008;49(2):195–201. doi:10.1016/j.comppsych.2007.09.002
28. World Health Organization COVID-19 advice for the public: Getting vaccinated Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice.
29. Centers for Disease Control and Prevention: COVID-19 Vaccines for People who are Moderately or Severely Immunocompromised Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html.
30. Niemi RG, Jennings MK. Generations and Politics: A Panel Study of Young Adults and Their Parents. Princeton: Princeton University Press; 1981.
31. Sears DO. Life-stage effects on attitude change, especially among the elderly. Aging. 1981;61:183–204.
32. Krosnick JA, Alwin DF. Aging and susceptibility to attitude change. J Pers Soc Psychol. 1989;57(3):416. doi:10.1037/0022-3514.57.3.416
33. Sears DO. College sophomores in the laboratory: influences of a narrow data base on social psychology’s view of human nature. J Pers Soc Psychol. 1986;51(3):515. doi:10.1037/0022-3514.51.3.515
34. Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: cross-sectional telephone survey. BMJ. 2009;339:b2651. doi:10.1136/bmj.b2651
35. Zhan S, Yang YY, Fu C. Public’s early response to the novel coronavirus–infected pneumonia. Emerg Microbes Infect. 2020;9(1):534. doi:10.1080/22221751.2020.1732232
36. Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol. 2010;15(4):797–824. doi:10.1348/135910710X485826
37. Altamura AC, Buoli M, Serati M. Duration of illness and duration of untreated illness in relation to drug response in psychiatric disorders. Neuropsychiatry. 2011;1(1):81–90. doi:10.2217/npy.10.2
38. Rapee RM. Perceived threat and perceived control as predictors of the degree of fear in physical and social situations. J Anxiety Disord. 1997;11(5):455–461. doi:10.1016/S0887-6185(97)00022-4
39. De Hoog N, Stroebe W, De Wit JB. The impact of vulnerability to and severity of a health risk on processing and acceptance of fear-arousing communications: a meta-analysis. Rev Gen Psychol. 2007;11(3):258–285. doi:10.1037/1089-2680.11.3.258
40. Eagly AH, Chaiken S. The psychology of Attitudes. Harcourt Brace Jovanovich College Publishers; 1993.
41. Vacondio M, Priolo G, Dickert S, Bonini N. Worry, perceived threat and media communication as predictors of self-protective behaviors during the COVID-19 outbreak in Europe. Front Psychol. 2021;12:231. doi:10.3389/fpsyg.2021.577992
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.