Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Effectiveness of Once-Weekly Insulin Icodec versus Daily Basal Insulins in Chinese Adults with T2DM: A Treatment-Background Stratified Analysis
Authors Xie Z ![]() , Deng W
, Deng W ![]() , Liang Z, Xie Y, Chen J
, Liang Z, Xie Y, Chen J ![]() , Cao W
, Cao W
Received 28 May 2025
Accepted for publication 13 October 2025
Published 27 October 2025 Volume 2025:17 Pages 771—787
DOI https://doi.org/10.2147/CEOR.S539841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xing Lin Feng
Zeyu Xie,1 Weishang Deng,2 Zhuoru Liang,1 Yilin Xie,1 Jisheng Chen,3 Weiling Cao1
1Department of Pharmacy, The Third Affiliated Hospital (The Affiliated Luohu Hospital) of Shenzhen University, Shenzhen, Guangdong Province, People’s Republic of China; 2School of Pharmacy, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China; 3Key Specialty of Clinical Pharmacy, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong Province, People’s Republic of China
Correspondence: Weiling Cao, Department of Pharmacy, The Third Affiliated Hospital (The Affiliated Luohu Hospital) of Shenzhen University, Shenzhen, Guangdong Province, 518001, People’s Republic of China, Email [email protected]
Objective: This study evaluated the long-term cost-effectiveness of once-weekly insulin icodec versus daily basal insulins in Chinese adults with type 2 diabetes mellitus (T2DM) across treatment backgrounds (insulin-naïve to basal-bolus users).
Methods: Using the UKPDS-OM2.1 model calibrated to ONWARDS trial data (1– 5), we simulated lifetime outcomes over a 40-year horizon. Cost-utility analyses incorporated direct healthcare costs, complication utilities. Uncertainties were addressed using one-way and probabilistic sensitivity analyses. Scenario analyses explored pricing thresholds and adherence assumptions.
Results: Insulin icodec demonstrated cost-effectiveness versus degludec in insulin-naïve populations (ICER=$24974.29, below China’s 3 times WTP threshold) but not versus glargine U100 (ICER=$45544.68) and once-daily basal insulin (ICER=$76877.59). For basal and basal-bolus insulin treated patients, insulin icodec does not offer long-term cost-effectiveness advantages over either insulin degludec and insulin glargine U100. One-way sensitivity analyses identified the simulation time horizon and discount rate as the most influential parameters, with probabilistic sensitivity analyses confirming the robustness of these findings. Scenario analyses demonstrated that insulin icodec’s would become cost-effective compared to basal insulins when patients were willing to pay an additional $150 annually.
Conclusion: Insulin icodec offers cost-saving potential versus degludec in insulin-naïve T2DM patients. For basal and basal-bolus-treated patients, the clinical use of icodec needs to be critically evaluated for cost burden, and it is recommended that it be used preferentially in patients who are sensitive to the frequency of injections.
Keywords: insulin icodec, insulin degludec, insulin glargine U100, cost-utility analysis, type 2 diabetes mellitus
Introduction
Diabetes is a chronic and complex condition that contributes significantly to morbidity and mortality.1 Despite China bearing the highest global diabetes burden (140.9 million cases in 2021),2 glycemic control remains suboptimal, with 44.3% insulin nonadherence rates linked to daily injection burdens.3–5
Insulin therapy remains a cornerstone of diabetes management, yet the requirement for daily injections contributes to clinical inertia (delayed initiation, inadequate titration, and missed doses) in type 2 diabetes mellitus (T2DM), ultimately compromising glycemic control.6 Whereas weekly insulin formulations theoretically address this issue and improved adherence and treatment satisfaction, notwithstanding the critical absence of China-specific cost-effectiveness evidence across treatment-experienced subgroups.7,8
A participant-level meta-analysis of the ONWARDS 1–5 trials demonstrated that icodec was associated with a similar rate of clinically significant hypoglycemia compared with basal daily insulins (including insulin glargine U100 and insulin degludec), while also resulting in fewer severe hypoglycemic events and a greater reduction in HbA1c.9 However, there is a scarcity of economic evaluations examining the long-term cost-effectiveness of icodec versus other basal insulin analogs, such as glargine U100 or degludec, within the Chinese healthcare context. Furthermore, no study to date has specifically assessed the cost-effectiveness of switching to icodec among T2DM patients with diverse insulin treatment backgrounds—a clinically relevant scenario given the potential of once-weekly dosing to improve treatment satisfaction and adherence. Therefore, this study evaluates the CE of once-weekly icodec versus daily basal insulins (glargine U100/degludec) in Chinese adults with T2DM from a healthcare system perspective, stratified by treatment background. Our findings aim to inform evidence-based decisions for clinicians and healthcare policymakers regarding insulin therapy optimization.
Method
UKPDS OM2.1 Model
The UKPDS-OM2.1 is a sophisticated and extensively validated computer simulation model that is based on patient data from the UK Prospective Diabetes Study (UKPDS). It is designed to predict the incidence of eight diabetes-related complications over a patient’s lifetime. This model is capable of estimating both lifetime healthcare costs and quality-adjusted survival, making it a valuable tool for assessing the long-term health and economic outcomes of T2DM.10
One of the strengths of the UKPDS-OM2.1 model is its adaptability and application across diverse populations worldwide, including White, Afro-Caribbean, and Asian-Indian demographic groups. This wide applicability enhances the reliability of its predictions across varied ethnic and racial backgrounds, which is critical given the differential impact of diabetes in different populations. Internal and external validations of the UKPDS OM 2.1 were calibrated against international trials.10,11 The model was operated at an annual cycle length. All the future costs and health outcomes were discounted at 5%.
In this specific study, risk factor data—including demographic characteristics, risk factor scores, prior events, specific costs, health utility, and other relevant parameters—were inputted from the participants at the conclusion of the study treatment phase into the UKPDS-OM2.1 model. The model then processed this data to output key outcomes such as life expectancy (LE), quality-adjusted life years (QALYs), treatment costs, complication costs, and total costs. These outputs allow for a comprehensive evaluation of the health and economic consequences for T2DM patients following the study period, providing crucial insights into the long-term viability and impact of the treatments under investigation.
Baseline Characteristics and Clinical Efficacy
This study constitutes a secondary analysis of data from the ONWARDS clinical trial program (comprising trials 1–5),12–16 which evaluated the efficacy and safety of once-weekly insulin icodec compared with daily basal insulins (insulin glargine U100 or insulin degludec) in adults with type 2 diabetes across a spectrum of previous treatment backgrounds—ranging from insulin-naïve to those receiving basal-bolus regimens. Specifically, ONWARDS 1, 3, and 5 enrolled insulin-naïve individuals, whereas ONWARDS 2 and 4 included patients who had previously been treated with basal insulin or basal-bolus insulin therapy.
Baseline data revealed comparable demographics: mean age 58–63 years, BMI 29–33 kg/m², HbA1c 8.1–9.0%, with high metformin use (65–93%). Notably, insulin-experienced cohorts (ONWARDS 2 and 4) had longer diabetes duration (16–18 years) and higher baseline insulin doses (25–29 U/day) versus naïve populations (10–12 years). Racial distribution was predominantly White (52–67%), followed by Asian (26–42%), with balanced sex representation (52–63% male). The baseline characteristics of the patients are presented in Table 1.
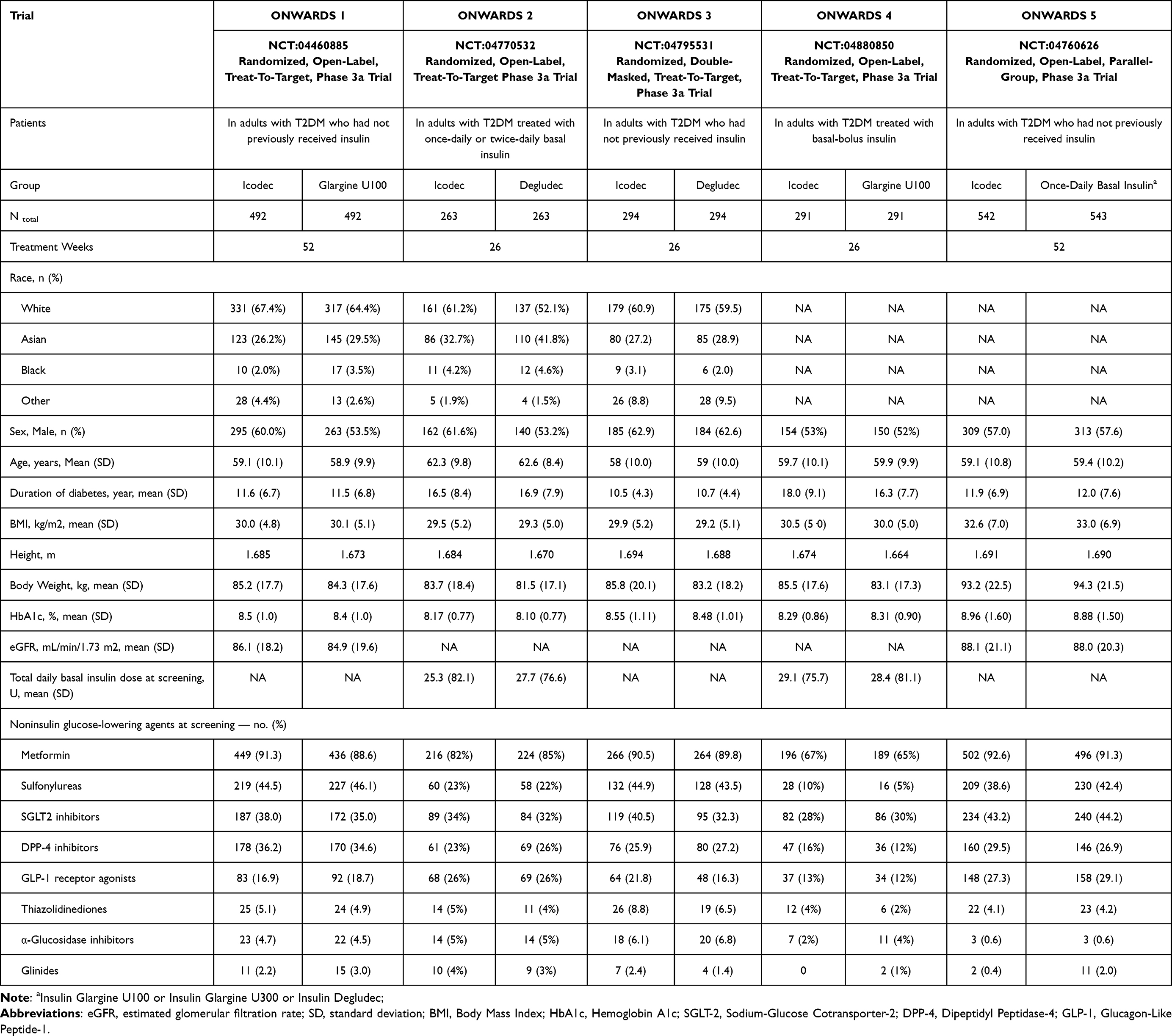 |
Table 1 Baseline Characteristics of Patients |
The clinical efficacy and safety outcomes for once-weekly insulin icodec versus daily basal insulins (glargine U100 or degludec) are presented in Table 2. Icodec demonstrated non-inferior/superior HbA1c reductions (-0.71% to -1.68%) across all trials versus comparators, albeit with consistently greater weight gain (+1.4 to +2.8 kg vs -0.3 to +2.3 kg). Weekly insulin dosage requirements were similar (185–305 U/week), while severe hypoglycemia rates remained low (0–4 events) without significant between-group differences.
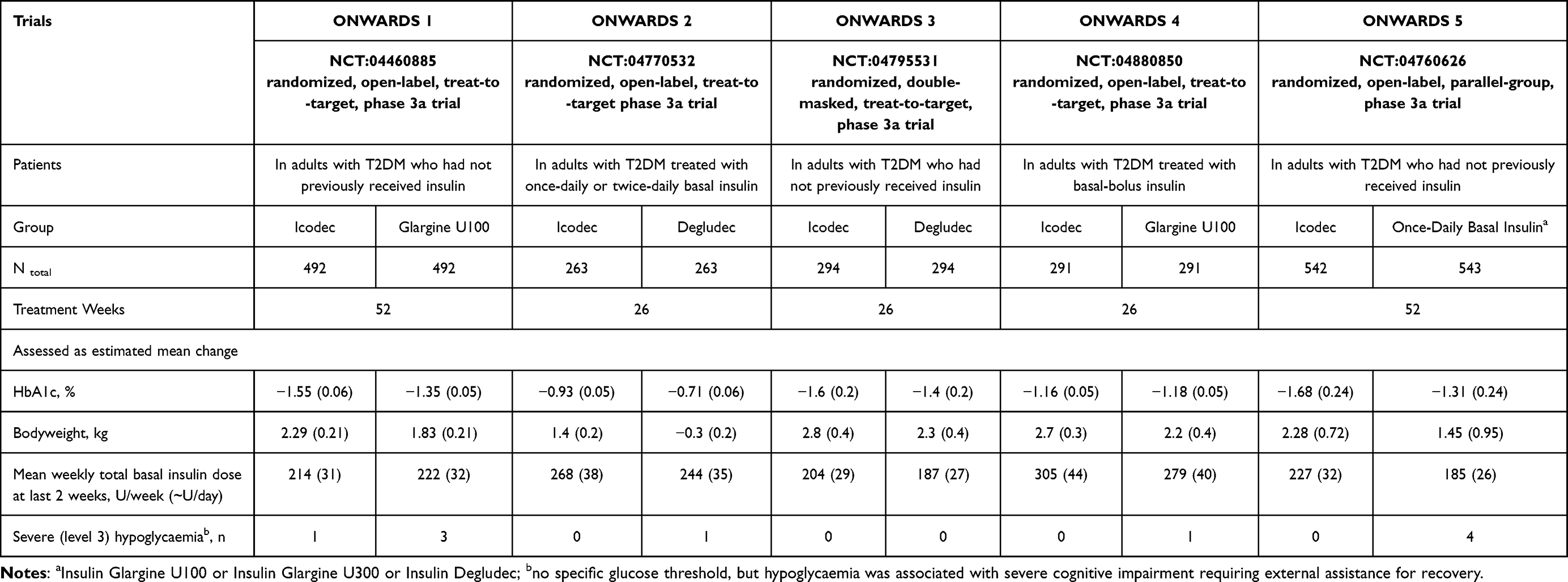 |
Table 2 Clinical Efficacy and Safety Outcomes |
In the five Phase 3 clinical trials of ONWARDS trial series (1–5), only the mean and standard deviation of baseline characteristics were reported. Therefore, to better reflect clinical practice, we used Stata 16.1 software to randomize patient-level data. The mean age of the patients ranged from 58 to 63 years, and we set the simulation time horizon to 40 years. Given that insulin therapy is typically a lifelong treatment, a treatment duration of 40 years was deemed sufficient to simulate the patients’ lifetime treatment. In accordance with World Health Organization (WHO) guidelines, a discount rate of 5% was pre-set.17 Our base-case analysis assumed 100% adherence to the treatment regimen, which represents an optimistic assumption rarely achieved in real-world clinical practice. This approach aligns with the intention of evaluating the intervention’s efficacy under ideal conditions, thereby providing an estimate of its maximum potential clinical benefit. The UKPDS-OM2.1 model was employed to extrapolate outcomes for each study participant, including all relevant long-term complications and associated lifetime costs, from the end of the treatment period until death. Additionally, the UKPDS OM2.1 model performed second-order Monte Carlo simulations with 1000 iterations to address parameter uncertainty.10
Costs and Utilities
The cost-utility analysis was based on the perspective of Chinese healthcare providers and only considered the direct healthcare costs of the different options, including the cost of acquiring the drugs, needles, the cost of diabetes management in the absence of complications, and the cost of diabetes-related complications. The insulin dosage was based on the treatment dose during the final two weeks of the RCTs, while insulin prices were derived from the 2024 Chinese medical insurance pricing, and needle costs were based on local market prices (Supplementary Table 1). All costs were expressed in 2024 US dollars (1 USD = 7.1217 CNY). The cost of managing diabetes without complications was obtained from a study by Li et al,18 which was a multicenter prospective cohort study implemented across 16 tertiary care hospitals in urban China. The costs of diabetes-related complications (eg, fatalities, nonfatalities, maintenance costs, etc.) were obtained from previously published literature on Pharmacoeconomics in China.19–23 In terms of utility, the initial utility value for diabetic patients without complications in this study was 0.876. This data was derived from the study by Pan et al,24 which utilized a 5-level, 5-dimensional EuroQol scale (EQ-5D-5L) to assess Chinese patients with T2DM. The utility decrement values for diabetes-related complications were obtained from previously published studies related to Chinese Pharmacoeconomics20,23,25 and the UKPDS 62 study26 and the specific cost and utility parameters are shown in Table 3.
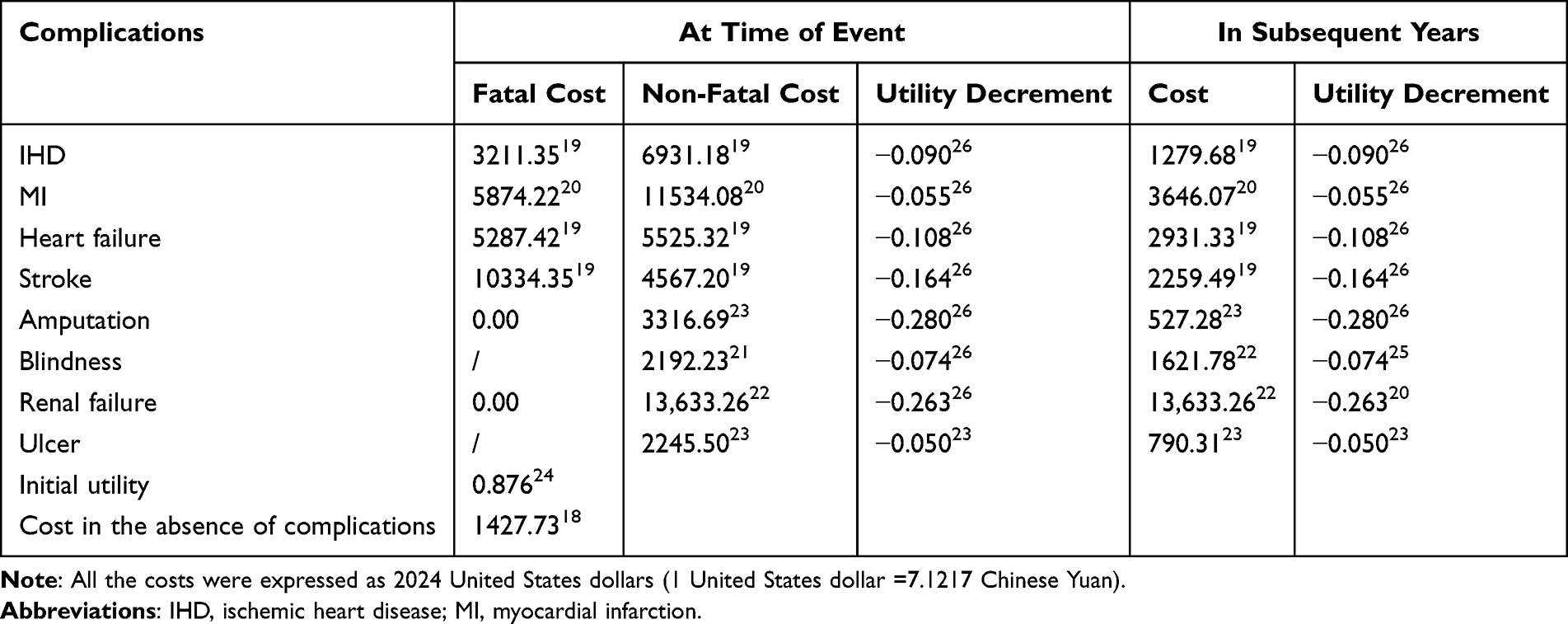 |
Table 3 Key Model Inputs of Costs and Utilities |
Sensitivity Analysis
Over a 40-year simulation period, a cost-utility analysis was conducted using the Incremental Cost-Effectiveness Ratio (ICER) as the primary evaluation metric. The cost-utility analysis was performed in strict accordance with pharmacoeconomic guidelines27 and the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist28 (Supplementary CHEERS 2022 checklist). The ICER was evaluated against the willingness-to-pay (WTP) threshold, which was set at 1–3 times the Gross Domestic Product (GDP) per capita, as recommended by the WHO.29 We utilized current data to predict long-term outcomes, which inherently involves significant uncertainty. Therefore, one-way sensitivity analyses, scenario analyses, and probabilistic sensitivity analyses were conducted to assess the impact of uncertainty on key model parameters.
In the one-way sensitivity analyses, we evaluated the effects of variations in key model parameters, including costs, utilities, discount rates, initial utility values, treatment duration, and time horizon. The cost and utility values for complications and diabetes-related events were tested at the upper and lower bounds of their 95% confidence intervals. In cases where 95% confidence intervals were unavailable, cost variables were assessed within a range of -20% to +20%, and utility variables were assessed within a range of -10% to +10% for the one-way sensitivity analyses. Discount rates were set at 3% and 8%, treatment durations at 30 and 50 years, and time horizons at 30 and 50 years. The initial utility values evaluated ranged from 0.78 to 0.92. The specific parameters for the one-way sensitivity analysis are detailed in Table 4, and the results of this analysis are visually represented using tornado diagrams.
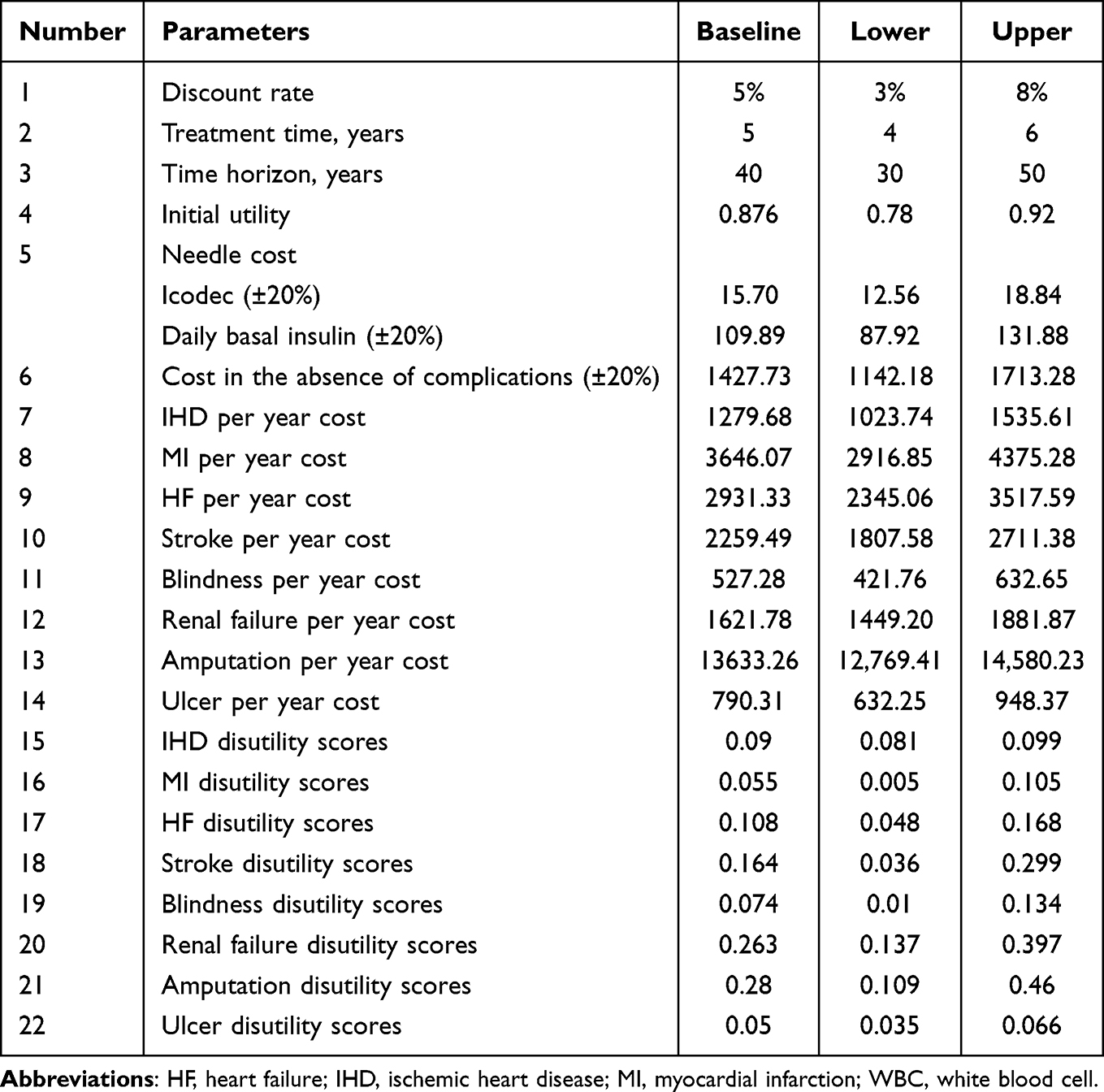 |
Table 4 Parameters for Sensitivity Analysis |
In the probabilistic sensitivity analysis, Monte Carlo simulations were performed with 1000 iterations to address second-order uncertainty, thereby enhancing the robustness of our findings. Gamma distributions were assigned to cost parameters, and beta distributions were applied to utility parameters, in order to capture sampling uncertainty. The results of this analysis are presented as scatter plots of the ICER and CE Acceptability Curves, providing a comprehensive overview of the potential range of outcomes and their probability of being cost-effective at various willingness-to-pay thresholds.
In the scenario analysis, since insulin icodec is administered once weekly compared to once-daily basal insulins (such as insulin glargine and insulin degludec), the reduction in injection frequency is critical for patient adherence. Therefore, we established three scenarios assuming that patients are willing to pay an additional annual cost of 50,100, and $150 for once-weekly insulin icodec therapy. Additionally, we considered the most influential parameters from the one-way sensitivity analysis and the potential impact of a 10% price reduction in basal insulins (insulin glargine and insulin degludec) in the future. Finally, based on the base-case analysis results, we employed a binary analysis approach to explore the required price reduction for Insulin Icodec to achieve cost-effectiveness (ICER < 3 times GDP per capita) across five patient populations with different disease states. This targeted approach helps identify the most feasible annual cost for Insulin Icodec to be a cost-effective option in the treatment of T2DM.
Results
The Results of Cost-Utility Analysis
After 40 years of simulation, Table 5 presents the outcomes of life expectancy, survival benefits, therapy costs, complication costs, total costs, ICER, and net monetary benefit (NMB) across five diverse treatment backgrounds (insulin-naïve to basal-bolus users). The results of the cost-utility analysis comparing insulin icodec versus daily basal insulin are presented in Table 6. In insulin-naïve adults with T2DM, insulin icodec versus insulin glargine U100 and once-daily basal insulin (ONWARDS 1 and 5) yielded ICERs of $ 45,544.69 and $ 76,877.59 per QALY gained, with negative NMB values (-183.54 and -1223.96, respectively). In contrast, insulin icodec versus insulin degludec (ONWARDS 3) demonstrated an ICER of $ 24,974.30 per QALY gained, which was below China’s 3 times GDP per capita threshold, along with appositive NMB values (774.50). These results indicate that insulin icodec is cost-effective compared to insulin degludec in insulin-naïve T2DM patients, but not when compared to insulin glargine U100 and once-daily basal insulin.
 |
Table 5 The Results of Cost-Utility Simulation |
 |
Table 6 The Results of Cost-Utility Analysis |
Among adults with T2DM receiving basal insulin therapy, insulin icodec versus insulin degludec (ONWARDS 2) showed an ICER of 80,186.91 per QALY and a negative NMB (-915.54). Meanwhile, among adults with T2DM receiving basal-bolus insulin therapy, insulin icodec versus insulin glargine U100 (ONWARDS 4) was associated with higher treatment costs ($30,888.00 vs $27,602.73) and fewer QALYs gained (10.8508 vs 10.8532). This suggests that insulin icodec does not offer long-term cost-effectiveness advantages over either insulin degludec or insulin glargine U100 in patients on basal and basal-bolus insulin regimens.
The Results of One-Way Sensitivity Analysis
The tornado diagram analysis systematically evaluated parameter uncertainties in the cost-effectiveness of insulin icodec versus other basal insulin (degludec or glargine U100) across four diverse treatment backgrounds (insulin-naïve to basal-bolus users) (Figure 1).
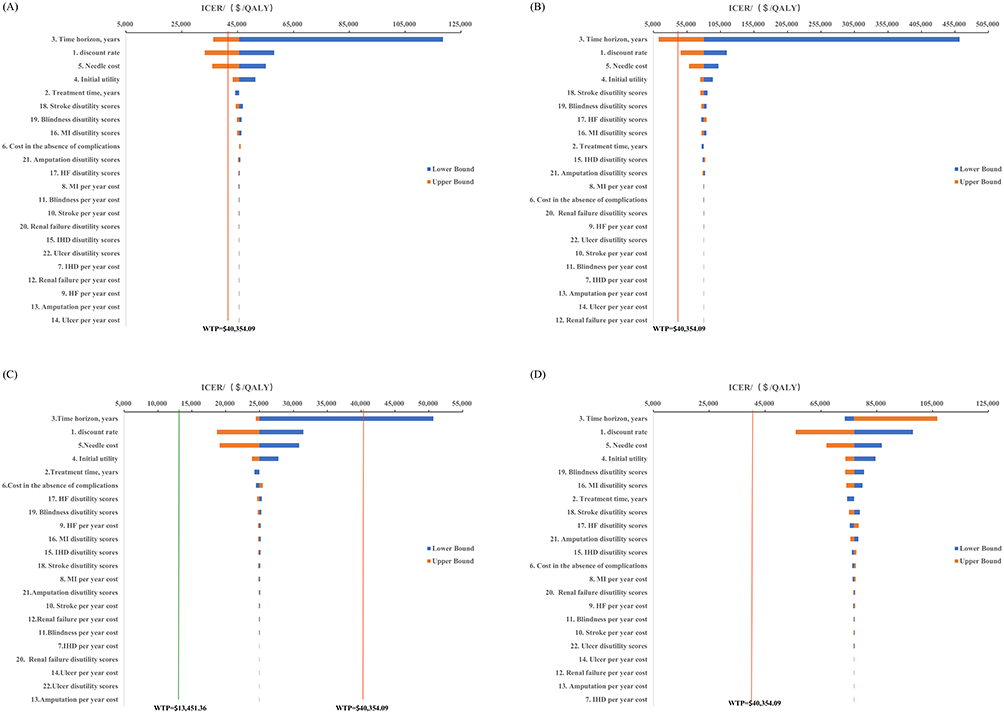 |
Figure 1 Tornado diagrams of the one-way sensitivity analysis. Note: QALY: Quality-Adjusted Life Year; ICER: Incremental Cost-Effectiveness Ratio; WTP: willingness-to-pay; WTP=$40,354.09=3 times GDP per capita in China; WTP=$13451.36=1 times GDP per capita in China. (A) Insulin Icodec vs Insulin Glargine U100 in insulin-naïve T2DM patients; (B) Insulin Icodec vs Insulin Degludec in basal insulin-treated T2DM patients; (C) Insulin Icodec vs Insulin Degludec in insulin-naïve T2DM patients; (D) Insulin Icodec vs daily basal insulin in insulin-naïve T2DM patients. |
Our univariate sensitivity analysis identified three key findings: Firstly, model time horizon and discount rate emerged as the most influential parameters, with their variations generating the widest ICER fluctuations, underscoring the critical importance of structural assumptions in the economic model. Secondarily, intervention-specific costs (eg, injection device expenses) and baseline utility values demonstrated substantial sensitivity, highlighting the pivotal role of initial health status and delivery system costs in cost-effectiveness evaluations. In contrast, complication-related parameters (including annual treatment costs and utilities) exhibited minimal impact on ICERs, confirming the model’s robustness to these clinical inputs.
Building upon our base-case findings, we conducted threshold analyses by systematically varying the annual treatment costs of insulin icodec across the four ONWARDS trial diverse treatment backgrounds populations (cohorts 1, 2, 4, and 5). The results demonstrated that to achieve cost-effectiveness at China’s willingness-to-pay threshold (ICER ≤$40,354/QALY) compared to either insulin glargine U100 or degludec, insulin icodec would require differential price reductions of 2.50%, 10.63%, 32.94%, and 15.79% for ONWARDS 1, 2, 4, and 5 cohorts, respectively. These findings reveal substantial heterogeneity in cost-effectiveness thresholds across clinical populations, with the most pronounced price reduction required in the ONWARDS 4 cohort (32.94%), suggesting distinct economic value propositions depending on treatment context and comparator regimens. This tiered sensitivity profile underscores the importance of context-specific pricing strategies for insulin icodec adoption.
Probabilistic Sensitivity Analysis
In the ONWARDS 4 trial population (adults with T2DM receiving basal-bolus insulin), insulin icodec was dominated by insulin glargine U100, demonstrating both higher costs and inferior clinical outcomes. Consequently, we present probabilistic sensitivity analysis results only for the remaining four trial populations (ONWARDS 1, 2, 3, and 5), with corresponding cost-effectiveness scatterplots and acceptability curves shown in Figures 2 and 3.
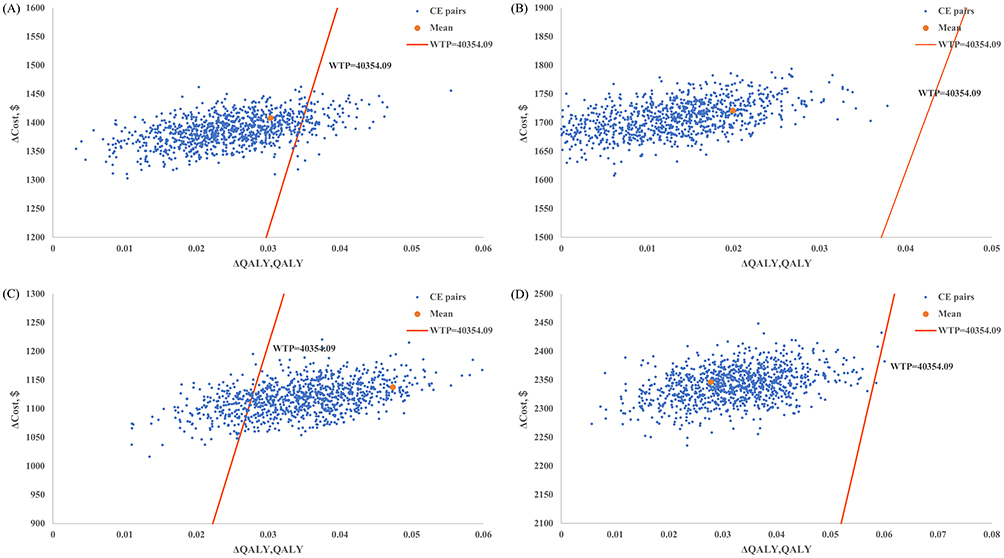 |
Figure 2 Cost-effectiveness scatter plots comparing once-weekly insulin icodec versus daily basal insulins. Abbreviations: QALY, Quality-Adjusted Life Year; WTP, willingness-to-pay. Notes: Δ: represents the difference between the two group; (A) Insulin Icodec vs Insulin Glargine U100 in insulin-naïve T2DM patients; (B) Insulin Icodec vs Insulin Degludec in basal insulin-treated T2DM patients; (C) Insulin Icodec vs Insulin Degludec in insulin-naïve T2DM patients; (D) Insulin Icodec vs daily basal insulin in insulin-naïve T2DM patients. |
 |
Figure 3 Cost-effectiveness acceptable curves comparing once-weekly insulin icodec versus daily basal insulins. Notes: (A) Icodee vs Glargine U100 CE Acceptability Curve in Insulin-naive T2DM Patients; (B) Icodec vs Degludec CE Acceptability Curve in Basal Insulin treated Patients; (C) Icodec vs Degludec CE Acceptability Curve in Insulin-naive T2DM Patients; (D) Icodee vs Basal Insulin CE Acceptability Curve in Insulin-naive T2DM Patients. |
The probabilistic sensitivity analysis involving 1000 Monte Carlo simulations revealed that the majority of cost-effectiveness pairs for insulin icodec versus comparator basal insulins across the four ONWARDS cohorts (1, 2, 3, and 5) were distributed in the northeast quadrant (Figure 2), indicating consistently higher total costs coupled with greater QALY gains. Among insulin-naïve adults with T2DM, the probability of insulin icodec being cost-effective was 9.3% versus insulin glargine U100 (Figures 2A and 3A), 80.1% versus insulin degludec (Figures 2C and 3C), and 0.2% versus once-daily basal insulin (Figures 2D and 3D). Notably, in adults with T2DM receiving basal-bolus insulin therapy, insulin icodec demonstrated a 0% probability of cost-effectiveness when compared with insulin degludec (Figures 2B and 3B).
The Results of Scenario Analysis
We assumed that T2DM patients (with or without receiving insulin at screening) were willing to pay an additional 50, 100, or $150 annually for once-weekly insulin icodec versus once-daily basal insulin. Accordingly, we conducted threshold analyses by progressively adjusting icodec’s annual treatment cost, with cost-utility outcomes presented in Table 7.
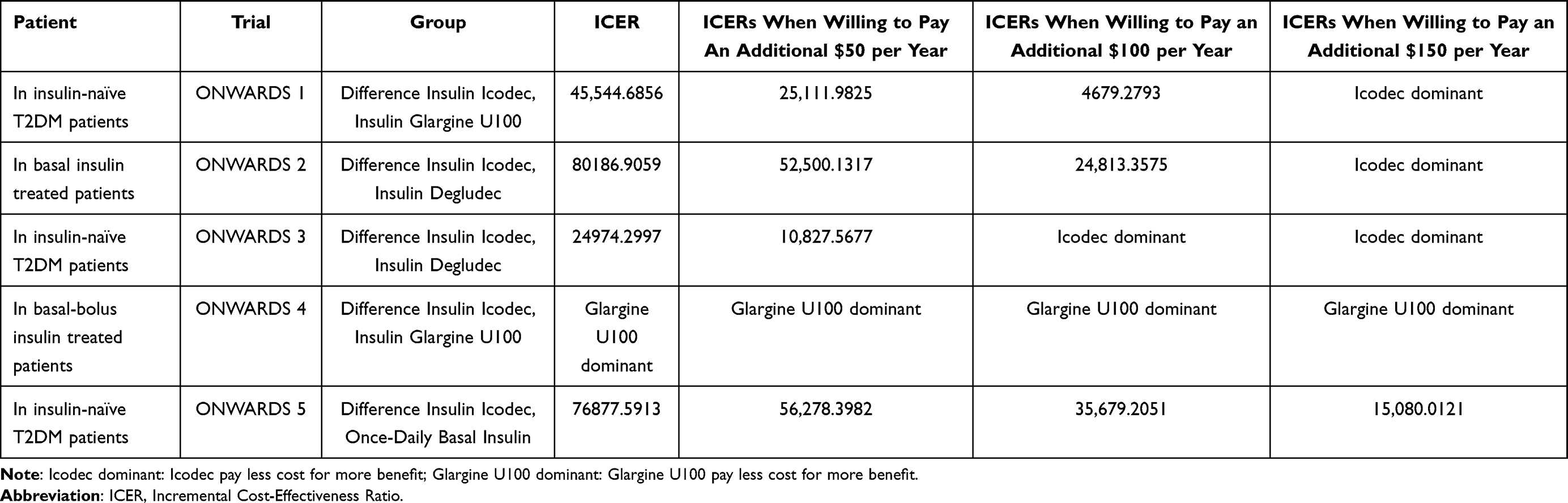 |
Table 7 The Results of Cost-Utility When Patients Willing to Pay an Additional 50, 100, or $150 Annually for Once-Weekly Insulin Icodec |
At $50/year WTP, among insulin-naïve adults with T2DM, insulin icodec demonstrated long-term cost-effectiveness advantages versus both insulin glargine U100 and insulin degludec. At 100 or $150/year WTP, in insulin-naïve patients, icodec remained cost-effective against all comparator basal insulins; For basal insulin treated T2DM adults, icodec showed cost-effectiveness versus insulin degludec but not glargine U100.
Under scenarios incorporating a 10% price reduction for glargine U100 and degludec and an extended 30-year time horizon (the most influential parameter), the long-term cost-utility analysis revealed that insulin icodec maintained its cost-effectiveness in insulin-naïve T2DM patients and icodec versus degludec retained cost-effectiveness in basal insulin treated patients regardless of price reductions or time horizon extensions at a $150/year WTP, with probabilistic sensitivity analysis results consistent with the base-case findings (Supplementary Figures 1 and 2).
Discussion
This study evaluated the long-term cost-effectiveness of once-weekly insulin icodec versus daily basal insulins (glargine U100/degludec) in Chinese adults with T2DM across diverse treatment backgrounds (insulin-naïve to basal-bolus users). The study results demonstrated that insulin icodec was cost-effective compared to degludec in insulin-naïve T2DM patients (ICER: $24,974/QALY; NMB: +775). However, it showed no advantage against glargine U100 or once-daily basal insulin (ICER exceeded the 3 times GDP threshold, and NMB was negative). Among patients on basal or basal-bolus regimens, icodec offered no long-term cost-effectiveness benefits. Sensitivity analysis confirmed that the simulation time horizon and discount rate had the greatest impact on outcomes. Scenario analysis revealed that patient’s WTP significantly influenced icodec’s cost-effectiveness—for instance, in most scenarios, icodec became advantageous when annual WTP reached $150 or higher.
In patients with T2DM receiving basal insulin therapy, approximately 50–73% fail to achieve glycemic targets.3 This treatment gap may be partially attributable to medication nonadherence, with Steenkamp et al4 reporting insulin nonadherence rates reaching 44.3% in T2DM populations - a clinically significant finding given its established association with both suboptimal glycemic control (HbA1c >7%) and increased microvascular complication risks. Multiple systemic and patient-specific barriers contribute to these unsatisfactory outcomes, including: clinical inertia in insulin initiation/titration, needle anxiety associated with daily injections, missed doses, premature treatment discontinuation, and hypoglycemia-related concerns.30 The novel once-weekly insulin icodec presents a potential solution, demonstrating therapeutic advantages through: reduced injection frequency (weekly vs daily), simplified administration protocols, improved glycemic stability (as measured by time-in-range metrics), Mitigated risks of hypoglycemia and weight gain. These pharmacological properties collectively enhance treatment adherence rates in clinical trials.31 However, cost-effectiveness remains highly dependent on treatment background and comparator drug pricing. Hu S et al demonstrated that in patients previously on basal insulin, icodec versus degludec showed cost-effectiveness when icodec’s annual treatment cost fell between $597.66 and $736.34.32 Conversely, Dai et al found that in patients previously receiving basal-bolus therapy, icodec versus glargine U100 only demonstrated cost-effectiveness when icodec’s annual treatment cost ranged from $784.90 to $1145.96.33 These differential price sensitivity profiles across treatment-experienced populations align precisely with our pharmacoeconomic findings, suggesting that value-based pricing strategies for icodec should account for prior treatment regimens.
Contrasting with Torre et al,’s34 Italian data, our analysis revealed lower cost-effectiveness of icodec in basal-bolus users. This divergence likely stems from two methodological distinctions: Firstly, our inclusion of complication management costs absents in their model. Second, Enrico Tone et al’s cohort comprised Italian adults with both T1DM and T2DM receiving basal insulin therapy, whereas our study exclusively examined T2DM. Third, their analysis assumed equivalent therapeutic efficacy between treatments, without accounting for potential differences in HbA1c reduction or weight change. Furthermore, Dai N et al’s33 research suggested that in basal-bolus-experienced patients, icodec showed greater cost-effectiveness than glargine U100 after 40-year simulation (10.15 vs 10.07 QALYs). This finding diverges from our results, potentially due to differences in baseline characteristic modeling - specifically, whether patient-level data were randomized based on mean and standard deviation parameters.
The Diabetes Prevention and Treatment Guidelines recommend that once-weekly insulin icodec demonstrates comparable efficacy to daily basal insulin analogs (glargine U100, glargine U300, and degludec) in HbA1c reduction, with similar hypoglycemia risk and weight effects, while significantly improving treatment satisfaction and adherence.35,36 For insulin-naïve patients, icodec may be prioritized - particularly when compared to degludec. However, in patients receiving basal or basal-bolus regimens, careful cost-benefit evaluation is warranted, with consideration limited to injection frequency-sensitive populations. In clinical practice, physicians should balance icodec’s convenience against its economic impact, incorporating both patient willingness-to-pay and diverse treatment background into therapeutic decision-making. From a policy perspective, China’s healthcare insurance system could implement differentiated reimbursement strategies based on patients’ treatment backgrounds to alleviate financial burdens while optimizing cost-effective care.
The current limited use of insulin icodec in China can be attributed to several factors, including the natural delay between regulatory approval and widespread adoption within a large healthcare system, its absence from the National Reimbursement Drug List (NRDL), which results in high out-of-pocket costs and poses a barrier to local budget allocation, limited clinical familiarity among providers, and infrastructural challenges such as cold chain requirements and training needs in rural areas. In conclusion, while icodec’s weekly profile is particularly promising for simplifying therapy in hard-to-reach populations, its successful implementation will depend on overcoming infrastructural barriers, ensuring affordable access through NRDL inclusion, and investing in healthcare professional training. Our cost-effectiveness findings provide a strong economic argument for policymakers to support its adoption across diverse treatment backgrounds in T2DM, offering evidence-based guidance for insulin therapy selection, contingent upon these implementation challenges being addressed.
This study utilized the validated UKPDS-OM2.1 model (demonstrated in multiple populations) and ONWARDS trial data to evaluate the long-term cost-effectiveness of once-weekly insulin versus daily basal insulins (glargine U100 and degludec), enhancing the reliability of outcome extrapolation. Comprehensive sensitivity analyses (including one-way, probabilistic, and scenario analyses) confirmed the robustness of our findings. However, several limitations should be acknowledged: First, the model relied on clinical trial data (eg, HbA1c changes, weight fluctuations), potentially underestimating real-world variability in adherence patterns and complication rates. Second, China-specific cost parameters (particularly complication-related expenses) may limit the generalizability of conclusions to other healthcare systems. For example, a study aiming to project the potential cost savings from implementing a multidisciplinary team (MDT) approach for reducing macrovascular and microvascular complications in patients with T2DM successfully demonstrated that the MDT model is effective in improving glycemic control. This intervention is projected to significantly reduce the incidence of diabetes-related complications, thereby resulting in substantial cost savings.37 Third, the model could not incorporate certain complication data as these were not reported in the original RCTs, which may affect outcome validity. Fourth, once-weekly insulin icodec may enhance treatment adherence and satisfaction as a convenient therapeutic option, real-world evidence on its actual adherence rates remains limited. Our base-case analysis assumed 100% adherence to the treatment regimen, which is an optimistic assumption rarely achieved in real-world clinical practice. Non-adherence can diminish treatment effectiveness, potentially alter the clinical outcomes and reduce the cost-effectiveness of the intervention. While this assumption aligns with the intention to evaluate the intervention’s efficacy under ideal conditions, it may overestimate its real-world value. Although our trial-based adherence assumptions may overestimate real-world outcomes, the scenario analyses with variable WTP thresholds ($50-$150) provide robust sensitivity testing. Finally, projecting long-term outcomes from short-term therapeutic effects may introduce estimation bias. Future research should: incorporate Chinese real-world evidence with long-term follow-up of icodec’s actual adherence rates and complication profiles to validate model assumptions; and expand the analytical framework to include indirect costs (eg, productivity losses) and societal preferences (eg, patient utilities for injection frequency).
Conclusion
This study demonstrates that once-weekly insulin icodec is a cost-effective alternative to insulin degludec in insulin-naïve Chinese patients with type 2 diabetes, but not against insulin glargine U100 or the class of once-daily basal insulins. No cost-effectiveness advantage was observed in patients previously treated with basal or basal-bolus insulin. For healthcare payers, these findings suggest that icodec could be prioritised for reimbursement specifically in insulin-naïve patients, while its use in insulin-experienced populations may require stricter criteria or value-based pricing strategies that account for actual injection frequency and adherence benefits. To further support decision-making, future research should include real-world studies in the Chinese context to evaluate long-term adherence, persistence, and associated complication rates under routine clinical practice.
Ethics Approval
This study utilizes previously anonymized data/desensitized biological samples and falls under the exemption from ethical review as stipulated in Article 32 of the “Ethical Review Measures for Life Sciences and Medical Research Involving Humans” in China. The research involves no harm to human subjects, does not involve sensitive personal information, and uses only rigorously desensitized data without any identifiable markers. Furthermore, it has no commercial interests or purposes.
Acknowledgments
The UKPDS Outcomes Model software (version 2.1) was provided by The Chancellor, Masters & Scholars of the University of Oxford.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2024 ‘Real-World Evidence and Health Technology Assessment for Clinical Use of Medicines’ Special Project (No. 2024-0808-03); Sanming Project of Medicine in Shenzhen (No. SZSM201801060).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu X, Zhang L, Chen W. Trends in economic burden of type 2 diabetes in China: based on longitudinal claim data. Front Public Health. 2023;11:1062903. doi:10.3389/fpubh.2023.1062903
2. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Dalal MR, Grabner M, Bonine N, et al. Are patients on basal insulin attaining glycemic targets? Characteristics and goal achievement of patients with type 2 diabetes mellitus treated with basal insulin and physician-perceived barriers to achieving glycemic targets. Diabet Res Clin Pract. 2016;121:17–26. doi:10.1016/j.diabres.2016.08.004
4. Yavuz DG, Ozcan S, Deyneli O. Adherence to insulin treatment in insulin-naïve type 2 diabetic patients initiated on different insulin regimens. Patient Prefer Adherence. 2015;9:1225–1231. doi:10.2147/PPA.S87935
5. Liu J, Liu M, Chai Z, et al. Projected rapid growth in diabetes disease burden and economic burden in China: a spatio-temporal study from 2020 to 2030. Lancet Reg Health West Pac. 2023;33:100700. doi:10.1016/j.lanwpc.2023.100700
6. Peyrot M, Rubin RR, Kruger DF, et al. Correlates of insulin injection omission. Diabetes Care. 2010;33(2):240–245. doi:10.2337/dc09-1348
7. Peyrot M, Barnett AH, Meneghini LF, et al. Insulin adherence behaviours and barriers in the multinational global attitudes of patients and physicians in insulin therapy study. Diabet Med. 2012;29(5):682–689. doi:10.1111/j.1464-5491.2012.03605.x
8. Polonsky WH, Fisher L, Hessler D, et al. Patient perspectives on once-weekly medications for diabetes. Diabetes Obes Metab. 2011;13(2):144–149. doi:10.1111/j.1463-1326.2010.01327.x
9. Bajaj HS, Ásbjörnsdóttir B, Bari TJ, et al. Once-weekly insulin icodec compared with daily basal insulin analogues in type 2 diabetes: participant-level meta-analysis of the ONWARDS 1–5 trials. Diabetes Obes Metab. 2024;26(9):3810–3820. doi:10.1111/dom.15726
10. Hayes AJ, Leal J, Gray AM, et al. UKPDS outcomes model 2: a new version of a model to simulate lifetime health outcomes of patients with type 2 diabetes mellitus using data from the 30year United Kingdom prospective diabetes study: UKPDS 82. Diabetologia. 2013;56(9):1925–1933. doi:10.1007/s00125-013-2940-y
11. Leal J, Reed SD, Patel R, et al. Benchmarking the cost-effectiveness of interventions delaying diabetes: a simulation study based on NAVIGATOR data. Diabetes Care. 2020;43(10):2485–2492. doi:10.2337/dc20-0717
12. Rosenstock J, Bain SC, Gowda A, et al. Weekly icodec versus daily glargine U100 in type 2 diabetes without previous insulin. N Engl J Med. 2023;389(4):297–308. doi:10.1056/NEJMoa2303208
13. Philis‐Tsimikas A, Asong M, Franek E, et al. Switching to once-weekly insulin icodec versus once-daily insulin degludec in individuals with basal insulin-treated type 2 diabetes (ONWARDS 2): a phase 3a, randomised, open label, multicentre, treat-to-target trial. Lancet Diabetes Endocrinol. 2023;11(6):414–425. doi:10.1016/S2213-8587(23)00093-1
14. Lingvay I, Asong M, Desouza C, et al. Once-weekly insulin icodec vs once-daily insulin degludec in adults with insulin-naive type 2 diabetes: the ONWARDS 3 randomized clinical trial. JAMA. 2023;330(3):228–237. doi:10.1001/jama.2023.11313
15. Mathieu C, Ásbjörnsdóttir B, Bajaj HS, et al. Switching to once-weekly insulin icodec versus once-daily insulin glargine U100 in individuals with basal-bolus insulin-treated type 2 diabetes (ONWARDS 4): a phase 3a, randomised, open-label, multicentre, treat-to-target, non-inferiority trial. Lancet. 2023;401(10392):1929–1940. doi:10.1016/S0140-6736(23)00520-2
16. Bajaj HS, Aberle J, Davies M, et al. Once-weekly insulin icodec with dosing guide app versus once-daily basal insulin analogues in insulin-naive type 2 diabetes (ONWARDS 5): a randomized trial. Ann Intern Med. 2023;176(11):1476–1485. doi:10.7326/M23-1288
17. World Health Organization. The World Health Report 2002. Midwifery. 2022;19:72–73.
18. Li X, Xu Z, Ji L, et al. Direct medical costs for patients with type 2 diabetes in 16 tertiary hospitals in urban China: a multicenter prospective cohort study. J Diabetes Investig. 2019;10(2):539–551. doi:10.1111/jdi.12905
19. Su W, Li C, Zhang L, et al. Meta-analysis and cost-effectiveness analysis of insulin glargine 100 u/Ml versus insulin degludec for the treatment of type 2 diabetes in China. Diabetes Ther. 2019;10(5):1969–1984. doi:10.1007/s13300-019-00683-2
20. Deng J, Gu S, Shao H, et al. Cost-effectiveness analysis of exenatide twice daily (Bid) vs insulin glargine once daily (QD) as add-on therapy in Chinese patients with Type 2 diabetes mellitus inadequately controlled by oral therapies. J Med Econ. 2015;18(11):974–989. doi:10.3111/13696998.2015.1067622
21. Cai X, Shi L, Yang W, et al. Cost-effectiveness analysis of dapagliflozin treatment versus metformin treatment in Chinese population with type 2 diabetes. J Med Econ. 2019;22(4):336–343. doi:10.1080/13696998.2019.1570220
22. Hou X, Wan X, Wu B. Cost-effectiveness of canagliflozin versus dapagliflozin added to metformin in patients with type 2 diabetes in China. Front Pharmacol. 2019;10:480. doi:10.3389/fphar.2019.00480
23. Wu B, Wan X, Ma J. Cost-effectiveness of prevention and management of diabetic foot ulcer and amputation in a health resource-limited setting. J Diabetes. 2018;10(4):320–327. doi:10.1111/1753-0407.12612
24. Pan CW, Sun HP, Zhou HJ, et al. Valuing health-related quality of life in type 2 diabetes patients in China. Med Decis Making. 2016;36(2):234–241. doi:10.1177/0272989X15606903
25. Currie CJ, McEwan P, Peters JR, et al. The routine collation of health outcomes data from hospital treated subjects in the health outcomes data repository (HODaR): descriptive analysis from the first 20,000 subjects. Value Health. 2005;8(5):581–590. doi:10.1111/j.1524-4733.2005.00046.x
26. Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Med Decis Making. 2002;22(4):340–349. doi:10.1177/027298902400448902
27. China Pharmaceutical Association Pharmacoeconomics Professional Committee. China guidelines for pharmacoeconomic evaluations. 2020: T/CPHARMA 003-2020[S]. 2020.
28. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Value Health. 2022;25(1):3–9. doi:10.1016/j.jval.2021.11.1351
29. Bertram MY, Lauer JA, De Joncheere K, et al. Cost-effectiveness thresholds: pros and cons. Bull World Health Organ. 2016;94(12):925–930. doi:10.2471/BLT.15.164418
30. Bajaj HS, Goldenberg RM. Insulin Icodec weekly: a basal insulin analogue for type 2 diabetes. Touch REV Endocrinol. 2023;19(1):4–6.
31. Ribeiro ESR, de Miranda GM, Guisso MES, et al. Once-weekly insulin icodec vs. once-daily insulin glargine U100 for type 2 diabetes: a systematic review and meta-analysis of Phase 2 randomized controlled trials. Arch Endocrinol Metab. 2023;67(5):e000614. doi:10.20945/2359-3997000000614
32. Hu S, Gu S, Wang S, et al. Cost-utility analysis and drug pricing of once-weekly insulin icodec versus once-daily insulin degludec for type 2 diabetes patients treated with basal insulin in China. Diabetes Obes Metab. 2024;26(12):5995–6006. doi:10.1111/dom.15973
33. Dai N, Su X, Wang Y. Cost-utility analysis of once-weekly insulin icodec and once-daily insulin glargine in patients with type 2 diabetes receiving basal-bolus insulin therapy in China. Diabetes Obes Metab. 2025;27(1):377–386. doi:10.1111/dom.16031
34. Torre E, Di Matteo S, Bruno GM, et al. Economic evaluation of once-weekly insulin icodec from Italian NHS perspective. Clinicoecon Outcomes Res. 2024;16:799–811. doi:10.2147/CEOR.S475461
35. Chinese Diabetes Society. Guideline for the prevention and treatment of diabetes mellitus in China (2024 edition). Chin J Diabetes Mellitus. 2025;2025:16–139.
36. American Diabetes Association Professional Practice Committee. 9. pharmacologic approaches to glycemic treatment: standards of care in diabetes—2025. Diabetes Care. 2025;48(Supplement_1):S181–S206. doi:10.2337/dc25-S009
37. Alshowair A, Altamimi S, Alruhaimi FA, et al. Cost-savings associated with multi-disciplinary team approach for reducing macrovascular and microvascular complications in patients with type 2 diabetes: a predictive model. Clinicoecon Outcomes Res. 2024;16:211–223. doi:10.2147/CEOR.S451739
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.