Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
Cost-effectiveness analysis of umeclidinium/vilanterol for the management of patients with moderate to very severe COPD using an economic model
Authors Wilson MR, Patel JG, Coleman A, McDade CL, Stanford RH ![]() , Earnshaw SR
, Earnshaw SR
Received 11 October 2016
Accepted for publication 30 January 2017
Published 24 March 2017 Volume 2017:12 Pages 997—1008
DOI https://doi.org/10.2147/COPD.S124420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Michele R Wilson,1 Jeetvan G Patel,2,3 Amber Coleman,2 Cheryl L McDade,1 Richard H Stanford,2 Stephanie R Earnshaw1
1RTI Health Solutions, Research Triangle Park, NC, USA; 2GSK, Research Triangle Park, NC, USA; 3Amgen Inc., Thousand Oaks, CA, USA
Background: Bronchodilators such as long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABAs) are central to the pharmacological management of COPD. Dual bronchodilation with umeclidinium/vilanterol (UMEC/VI; 62.5/25 µg) is a novel LAMA/LABA combination approved for maintenance treatment for patients with COPD.
Objective: The objective of this study was to assess the cost-effectiveness of maintenance treatment with UMEC/VI compared with tiotropium (TIO) 18 µg, open dual LAMA + LABA treatment, or no long-acting bronchodilator treatment in patients with moderate to very severe COPD.
Methods: A Markov model was developed to estimate the costs and outcomes associated with UMEC/VI treatment in patients with moderate to very severe COPD (GSK study number: HO-13-13411). Clinical efficacy, costs, utilities, and mortality obtained from the published literature were used as the model inputs. Costs are presented in US dollars based on 2015 prices. The model outputs are total costs, drug costs, other medical costs, number of COPD exacerbations, and quality-adjusted life-years (QALYs). Costs and outcomes were discounted at a 3% annual rate. Incremental cost-effectiveness ratios were calculated. One-way and probabilistic sensitivity analyses were conducted to assess the effects of changing parameters on the uncertainty of the results.
Results: UMEC/VI treatment for moderate to very severe COPD was associated with lower lifetime medical costs ($82,344) compared with TIO ($88,822), open dual LAMA + LABA treatment ($114,442), and no long-acting bronchodilator ($86,751). Fewer exacerbations were predicted to occur with UMEC/VI treatment compared with no long-acting bronchodilator treatment. UMEC/VI provided an 0.11 and 0.25 increase in QALYs compared with TIO and no long-acting bronchodilator treatment, and as such, dominated these cost-effectiveness analyses. Sensitivity analyses confirmed that the results were robust.
Conclusion: The results from this model suggest that UMEC/VI treatment would be dominant compared with TIO and no long-acting bronchodilator treatment, and less costly than open dual LAMA + LABA treatment in patients with moderate to very severe COPD.
Keywords: umeclidinium, vilanterol, cost-effectiveness, tiotropium, COPD
Introduction
COPD is a highly prevalent,1,2 debilitating, chronic condition that has a significant impact on quality of life3 and costs borne by health care systems.4 In 2010, $32.1 billion direct medical costs were estimated to be attributable to COPD and its sequelae in the USA and a further $3.9 billion to absenteeism costs.5 Maintenance bronchodilator therapy is the foundation of stable COPD treatment, and combining bronchodilators is supported as a useful treatment option for patients with a higher symptom burden.2
The combination of the long-acting muscarinic antagonist (LAMA) umeclidinium (UMEC) with the long-acting β2-agonist (LABA) vilanterol (VI) is an approved maintenance treatment for COPD in the USA, the EU, and several other countries.6–8 Treatment with UMEC/VI increases lung function compared with tiotropium (TIO) monotherapy or placebo and has a clinically acceptable safety profile;9–11 however, its cost-effectiveness remains unknown. A potential barrier to the use of dual bronchodilator therapy could be the cost and complexity of adding an additional inhaler to patients’ treatments.
To address this, we examined the cost-effectiveness of UMEC/VI versus TIO, no long-acting bronchodilator treatment, and open dual (LAMA + LABA) bronchodilator treatment in patients with moderate to very severe COPD in the USA.
Methods
Analytic framework
A Markov model was developed with 1-year cycle times in which patients progressed through three COPD severity levels as defined by the 2013 COPD clinical guidelines.12 Severity of COPD was classified according to the predicted postbronchodilator forced expiratory volume in 1 second (FEV1) of patients, as shown in Figure 1.12
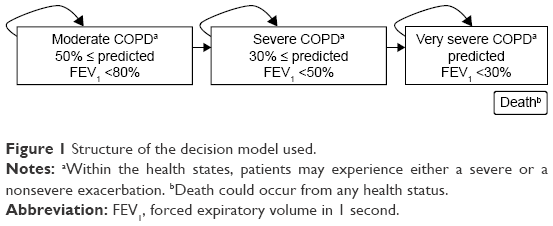 | Figure 1 Structure of the decision model used. |
Data from an initial mix of patients in different disease severity health states were entered into the Markov model (GSK study number: HO-13-13411). This mix was obtained from a prevalence study1 and from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) observational study (NCT00292552).13 Upon entering into the model, patients were prescribed a maintenance COPD treatment plus usual care. Each year in the model, patients remained in their current disease severity health state or moved to the next more severe health state. Within a year, patients could also experience an exacerbation or remain event free (ie, with no exacerbation). Death could occur from any health state according to the natural progression of the disease.14
The perspective of the analysis was that of a third-party payer in the USA where only direct medical costs were considered. A 20-year time horizon was assessed. Costs and outcomes were discounted at 3% per annum, and costs were reported in 2015 US dollars.
Patient population
Consistent with the patient populations studied in UMEC/VI clinical trials,9–11 patients included in this analysis were aged 40 years or older, had moderate to very severe COPD, and were eligible for maintenance treatment with LAMA/LABA combination therapy.6 Additional eligibility criteria included current smokers or ex-smokers with a smoking history of ≥10 pack-years, postalbuterol FEV1/forced vital capacity (FVC) ≤0.70, FEV1 ≤70% of predicted normal, and score of ≥2 using the Modified Medical Research Council Dyspnea Scale. Patients with a history of asthma or previous use of UMEC and/or VI were excluded.
Comparators
The following treatment regimens were compared: UMEC/VI (62.5/25 μg; delivering 55/22 μg administered once daily), TIO (18 μg; delivering 10 μg administered once daily), open dual LAMA + LABA therapy (TIO administered once daily and a LABA administered twice daily from separate inhalers), and no long-acting bronchodilator (where no such long-acting COPD maintenance treatment was administered).
TIO was chosen as the primary comparator for UMEC/VI, because it is one of the recommended first-line maintenance treatments for patients with moderate to very severe COPD2 and one of the most commonly used long-acting bronchodilators in the USA and Canada for the treatment of patients with COPD.15,16
Model inputs
Change in trough FEV1 efficacy
The model used 1) the improvement in lung function (ie, trough FEV1) in the first 24–26 weeks of treatment (Table 1),9–11,17 2) patient characteristics, 3) average predicted FEV1, and 4) annual rate of decline as observed among patients in the different disease severity health states to estimate the transition probabilities between the disease severity levels. Transitions between patients’ disease severity health states were based on the method described by Spencer et al,18 which used patients’ average time in each health state (Supplementary materials and Tables S1–S4).
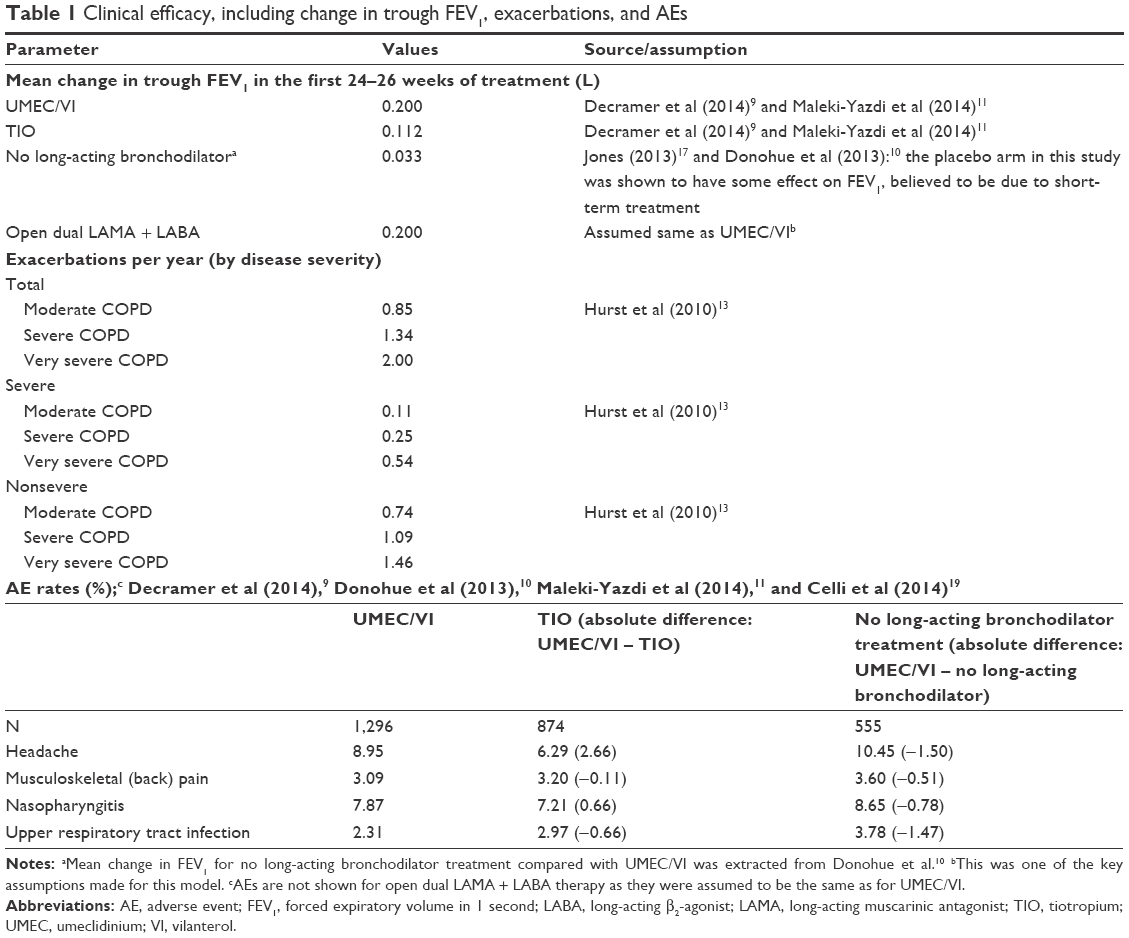 | Table 1 Clinical efficacy, including change in trough FEV1, exacerbations, and AEs |
Changes in trough FEV1 at 24–26 weeks for the different treatments were obtained from three studies for UMEC/VI (NCT01316900 [GSK study number DB2113360], NCT01316913 [DB2113374], and NCT01777334 [ZEP117115])9,11 and one study for no long-acting bronchodilator (NCT01313650 [DB2113373])10 (Table 1)9–11,17. Within these trials, the patient populations and methods used to measure relative changes in trough FEV1 were similar.9–11 It was therefore assumed that the relative changes in trough FEV1 observed for UMEC/VI compared with TIO reported in the head-to-head trials9,11 could be compared with the change in trough FEV1 observed in the placebo-controlled trial.10 It was also assumed that the change in trough FEV1 was the same for the UMEC/VI and open dual LAMA + LABA therapies (Table 1)9–11,17. As the change in trough FEV1 for each maintenance treatment was greater versus no long-acting treatment, patients in these groups remained in less severe health states longer than patients on no long-acting treatment.
Exacerbations
Exacerbations in this model were events that caused patients to seek health care. Patients could experience different levels of exacerbations or no exacerbations. Severe exacerbations were classified as events requiring hospitalization, and nonsevere exacerbations as events requiring a change in treatment such as systemic corticosteroids and/or antibiotics and/or contact with a health care provider. Patients were considered event free if they experienced no exacerbations.
Exacerbation risk was based on patient COPD severity and was obtained from the ECLIPSE study (Table 1).13
As a result, the impact that a treatment has on exacerbation was considered implicitly in the model. A treatment’s direct impact on exacerbations was not modeled as the clinical studies reporting the treatment effects were not powered to do so.
Adverse events (AEs)
AEs not associated with discontinuation were accounted for within the model. Specifically, AEs that occurred in at least 3% of patients and those deemed to result in significant costs were identified. AE rates for each treatment option were estimated using pooled data from the comparative trials of UMEC/VI (Table 1),9–11,19 apart from the AE rates for open dual LAMA + LABA treatment that were assumed to be the same as UMEC/VI. It was also assumed that AEs occurred in year 1 of the model and subsequent AEs were accounted for in the discontinuation rates.
Discontinuations
Patients may discontinue treatment due to lack of efficacy and/or due to an occurrence of an intolerable AE. The clinical impact of discontinuations was captured in the clinical efficacy input and was assumed to be similar for open dual LAMA + LABA and UMEC/VI treatment. Patients who discontinued due to lack of efficacy were reverted to no treatment and were assumed to move to standard care (defined as no treatment with UMEC/VI) as seen in the trials. The cost of the respective treatments was reduced. However, additional drug costs were not captured. As a result, results may be considered to be conservative.
Mortality
Deaths (related to COPD and other causes) were considered in the model. Age-specific all-cause mortality was obtained from the US National Vital Statistics.20 COPD-specific death was incorporated by applying relative risks for moderate COPD (relative risk =1.4) and severe and very severe COPD (relative risk =2.6) from Shavelle et al.14 It was assumed that COPD-related mortality was only based on disease severity.
Drug costs
All costs included in the model were in US dollars and based on 2015 data. Estimations of monthly prescription costs were based on the recommended dosing of each treatment.6,21 No long-acting bronchodilator treatment was assumed to be the cost of the short-acting bronchodilators ipratropium/albuterol (Combivent®).22 Open dual LAMA + LABA treatment was assumed to include the cost of TIO and the estimated average cost of salmeterol and formoterol administered twice daily. All drug costs were obtained from Medi-Span 2.0 (Table 2).23 Patients were assumed to be fully compliant with UMEC/VI or TIO treatments.
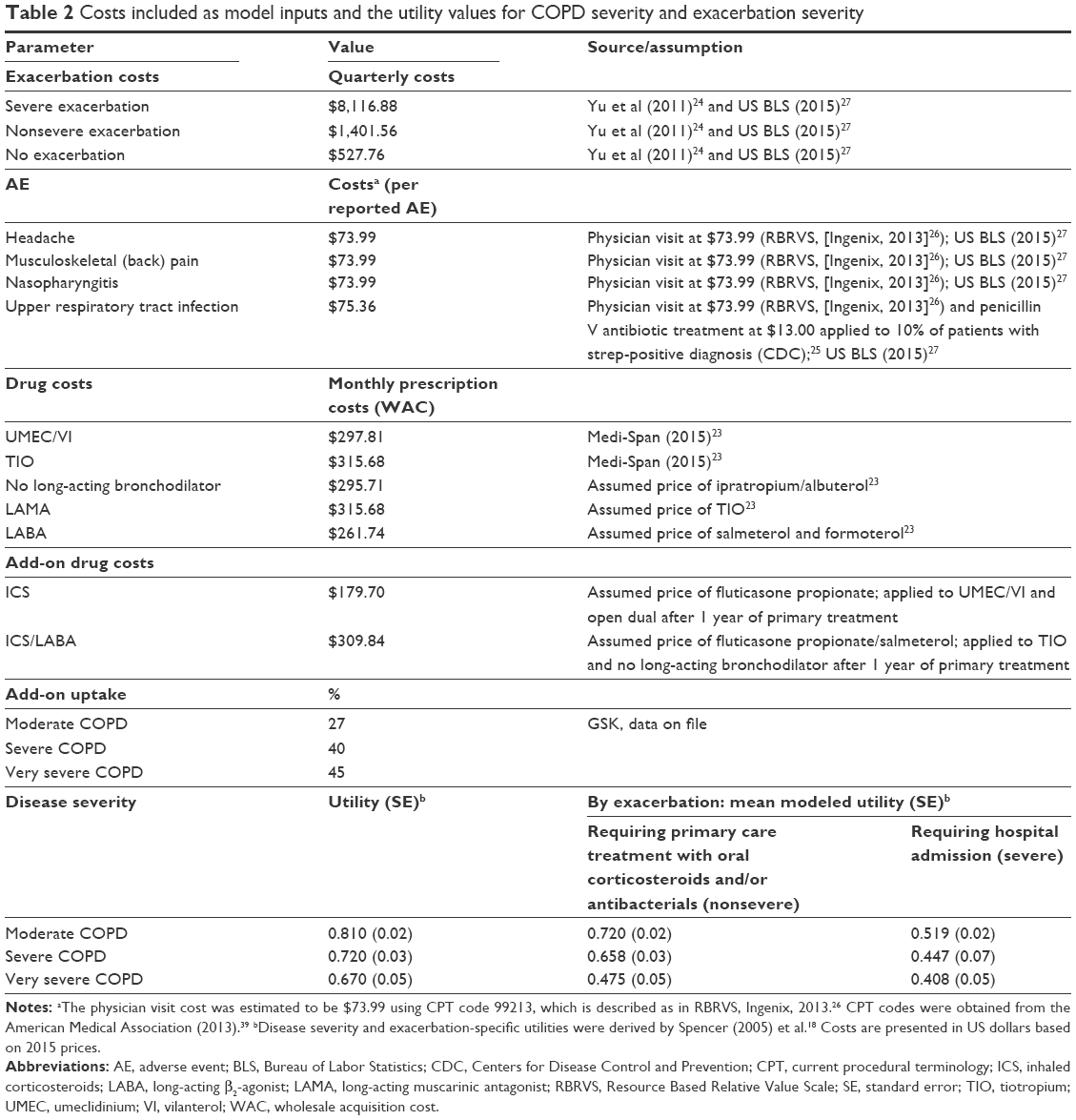 | Table 2 Costs included as model inputs and the utility values for COPD severity and exacerbation severity |
Add-on therapy
Add-on therapy was considered in the model to account for the additional costs incurred by patients who progress to triple therapy. The additional costs were for fluticasone propionate/salmeterol (Advair®) for patients in the TIO and no long-acting bronchodilation groups and also for fluticasone for UMEC/VI and open dual LAMA + LABA therapy groups. It should be noted that the percentage of patients who progressed to triple therapy was assumed to be related to disease severity and not to specific treatments, with the percentages used within this assumption obtained from a treatment pattern analysis (Table 2, GSK data on file).
Additional medical costs
Medical costs (other than those detailed previously) were also included and were assumed to be specific to exacerbations. These medical costs included inpatient, emergency room, outpatient, and “other” medical costs. “Other” medical costs were those not previously covered, such as home visits and skilled nursing facility services. Total medical costs for a severe exacerbation, nonsevere exacerbation, and no exacerbation were estimated according to Yu et al.24 The costs included those of the index exacerbation visit and those of any subsequent treatments. The costs of an AE resulting from the COPD maintenance treatments (the cost per AE assumed one physician visit and antibiotics as applicable; Table 2)25–27 were also considered within the model.
Utility weights
The annual utility weights used within the model were derived from those previously published and were related to disease severity and exacerbation events (Table 2).18 Severe exacerbations and nonsevere exacerbations were assumed to have a duration of 28 days and 10.5 days, respectively. These utility values were used to estimate quality-adjusted life-years (QALYs) by multiplying the number of accrued life-years within a particular health state by the disease severity’s utility weight.
Model calculations
The following outputs were estimated by the model: total costs, drug costs, other medical costs, number of exacerbations (total, nonsevere, and severe), life-years, and QALYs.
The cost-effectiveness of UMEC/VI versus each comparator was determined by calculating the incremental total cost per life-year or QALY gained: (Ci – Cs)/(Ei – Es), where Ci is the cost accrued by the treatment of interest, Cs is the cost accrued by the status quo treatment, Ei is the effectiveness accrued by the treatment of interest (life-year or QALY), and Es is the effectiveness accrued by the status quo treatment (life-year or QALY); all over a lifetime horizon. Cost and health outcomes were discounted at a 3% rate per year.
The effect of changing parameters was examined in one-way sensitivity analyses to test the robustness of the model assumptions and specific parameters. The results of sensitivity analysis for each input were ranked from most sensitive to least sensitive and plotted on tornado diagrams, with the 15 most sensitive parameters presented.
Probabilistic sensitivity analyses (second-order Monte Carlo simulation), in which all parameters in the model were varied at the same time, were also performed. Analyses were run 10,000 times to capture stability in the results for each relevant scenario and presented using scatter plots.
Results
Base-case analysis
Treatment of patients with moderate to very severe COPD with UMEC/VI resulted in total remaining lifetime medical costs of $82,344 compared with $88,822 for TIO, $114,442 for open dual LAMA + LABA treatment, and $86,751 for no long-acting bronchodilator treatment (Table 3). Patients treated with UMEC/VI also experienced fewer exacerbations (due to initial improvements in lung function) compared with patients receiving no long-acting bronchodilator treatment.
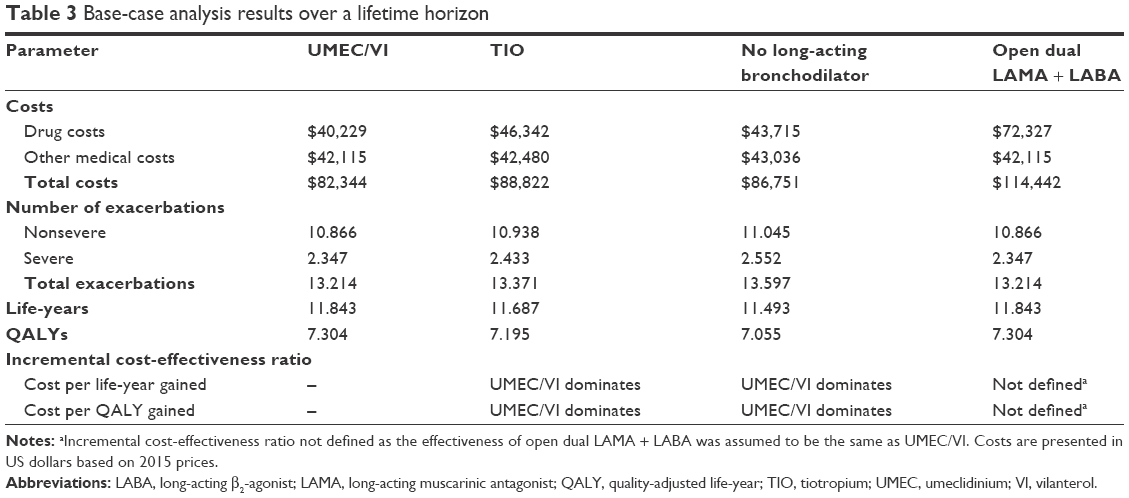 | Table 3 Base-case analysis results over a lifetime horizon |
Due to the assumptions used in the model, patients receiving UMEC/VI and open dual LAMA + LABA treatment experienced the same total life-years and QALYs. However, patients treated with UMEC/VI gained 0.16 life-years and 0.11 QALYs compared with TIO treatment and 0.35 life-years and 0.25 QALYs compared with no long-acting bronchodilator treatment. As UMEC/VI treatment was also less costly and was associated with fewer exacerbations compared with both TIO and no long-acting bronchodilator treatment, it was dominant to both (Table 3).
One-way sensitivity analyses
One-way sensitivity analyses showed that UMEC/VI treatment remained the dominant treatment compared with TIO and no long-acting bronchodilator treatment within the range of uncertainty applied to all variables in the model. UMEC/VI also had lower total costs compared with open dual LAMA + LABA within the range of uncertainty for all variables, mainly due to a lower acquisition cost.
Probabilistic sensitivity analyses
The probabilistic sensitivity analyses demonstrated that UMEC/VI was dominant 81.5% of the time, was not dominant but was cost-effective (incremental cost per QALY <$50,000) 13.8% of the time, and was cost-effective 95.3% of the time compared with TIO (Figure 2A). Compared with no bronchodilator treatment, UMEC/VI was dominant 71.1% of the time, was not dominant but was cost-effective 27.8% of the time, and was cost-effective 98.9% of the time (Figure 2B). The safety and efficacy of open dual LAMA + LABA was assumed to be the same as UMEC/VI making a probabilistic sensitivity analysis for this particular comparison unnecessary.
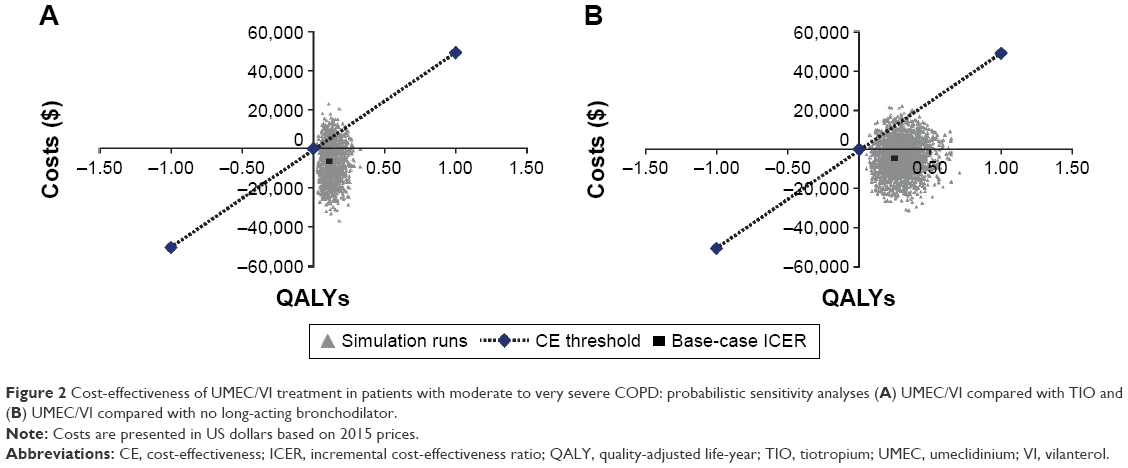 | Figure 2 Cost-effectiveness of UMEC/VI treatment in patients with moderate to very severe COPD: probabilistic sensitivity analyses (A) UMEC/VI compared with TIO and (B) UMEC/VI compared with no long-acting bronchodilator. |
Discussion
This analysis estimated the cost-effectiveness of UMEC/VI compared with other bronchodilator treatments for patients with moderate to very severe COPD and included a comparator of no long-acting bronchodilator treatment in which only short-acting rescue medication was permitted. In the base-case analysis, UMEC/VI was found to be dominant compared with TIO and no long-acting bronchodilator treatment. Furthermore, when UMEC/VI was compared with open dual LAMA + LABA treatment, both were assumed to have the same efficacy, but UMEC/VI was found to be less costly. Sensitivity analyses demonstrated that all cost-effectiveness findings were robust. Future analyses could investigate the cost-effectiveness of UMEC/VI compared with other closed dual bronchodilator treatments (eg, QVA149).
Since the approval of TIO as the first LAMA for the treatment of patients with COPD, several cost-effectiveness studies have been completed with different comparators.28–32 In this study, TIO cost more than no long-acting bronchodilation treatment but had an increased QALY of 0.14. An improvement in QALYs on TIO treatment has been reported in other studies comparing TIO with other treatments in COPD (0.051–0.15 QALYs),28–32 supporting the model assumptions used.
A strength of this analysis is that it incorporated progression to triple therapy (inhaled corticosteroids [ICS] + LAMA + LABA) for patients with COPD. This progression was based on disease severity and not specific treatments. A study in the UK found that patients with COPD often progress quickly to triple therapy33 and a second study in Japan found that more than half of patients who progress to triple therapy do so because of the need for additional symptom improvement.34 Progression to triple therapy incurs additional drug costs for COPD treatment, which this model accounted for in all treatment arms. Therefore, the reported cost-effectiveness for UMEC/VI includes this important aspect of COPD treatment.
A limitation of the study is that no formal statistical adjustments were made for the efficacy data of the treatments considered in this analysis, because of limited data on FEV1, comparative exacerbations, and treatment-related and exacerbation-related mortality. However, the sensitivity analysis that varied these parameters in the model showed that UMEC/VI remained cost-effective irrespective of variation in efficacy parameters.
Previous studies have shown that the major economic impact of maintenance treatment for COPD was in reducing exacerbations.29,31,32 While in this model, data were used from the ECLIPSE study13 that related FEV1 status to frequency of exacerbation events, other factors are also known to impact on exacerbation rate such as prior exacerbation history and heartburn.13 Furthermore, though disease severity has often been assessed using FEV1 performance in the past, recent clinical developments indicate that many other disease characteristics should be considered when assessing COPD severity. These factors were not directly accounted for in the model, and the analysis may need adjusting in the future once further data are available.
Another limitation is that COPD-related mortality was assumed to be disease severity specific and only indirectly accounted for treatment and exacerbation status, which is not necessarily the case and may have impacted the outcomes.35,36 Soler-Cataluna et al35 demonstrated that mortality is correlated with increasing severe exacerbations. However, as the impact of UMEC/VI on exacerbations has not yet been fully determined,9 this could not be fully included in the current model. Inclusion of treatment-specific impact on exacerbations and the associated mortality risk for exacerbations could affect the results, but it is unclear in which direction the effect would be without observing the exacerbation data for UMEC/VI. However, the data used within the model were the most accurately available at the time the analysis was undertaken and mortality was included. Finally, the assumption that patients would be fully compliant with the prescribed treatment regimens is unlikely to be true. While adherence with a once-daily TIO regimen is known to be high,37 it has not yet been directly evaluated with once-daily UMEC/VI. Adherence is likely to be similar as both treatments are once-daily inhalers, so it is unlikely to have an impact on the cost-effectiveness of UMEC/VI over TIO. Adherence to these once-daily LAMA treatments is likely to be much higher compared with adherence to any open dual regimen, as found in the recent real-world study comparing once-daily TIO with twice-daily budesonide/formoterol.38
Conclusion
The results from this model suggest that UMEC/VI treatment would be dominant compared with TIO and no long-acting bronchodilator treatment and be less costly than open dual LAMA + LABA treatment in patients with moderate to very severe COPD. Compared with TIO and no long-acting bronchodilator treatment, UMEC/VI was associated with fewer exacerbations as well as gains in life-years and QALYs.
Acknowledgments
GSK funded this study (study number HO-13-13411). Editorial assistance was provided by Gillian Groeger, PhD, Fishawack Indicia Ltd (UK), which was funded by GSK.
Author contributions
MRW, JGP, AC, CLM, RHS, and SRE contributed to the concept and design of this study and undertook data analysis and interpretation. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
MRW, CLM, and SRE are employees of RTI Health Solutions, an independent contract research organization that has received funding from GSK for this and other studies and from other pharmaceutical companies that market drugs for the treatment of patients with COPD and other medical conditions. AC and RHS are employees of GSK and holders of GSK stock. JGP was an employee of GSK and holder of GSK stock at the time of the study. JGP is now employed by Amgen. The authors report no other conflicts of interest in this work.
References
Buist AS, McBurnie MA, Vollmer WM, et al; BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. | ||
GOLD [homepage on the Internet]. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2015. Available from: http://www.goldcopd.com/. Accessed March 2015. | ||
Nagai K, Makita H, Suzuki M, et al; Hokkaido COPD Cohort Study Investigators. Differential changes in quality of life components over 5 years in chronic obstructive pulmonary disease patients. Int J Chron Obstruct Pulmon Dis. 2015;10:745–757. | ||
Dalal AA, Liu F, Riedel AA. Cost trends among commercially insured and Medicare Advantage-insured patients with chronic obstructive pulmonary disease: 2006 through 2009. Int J Chron Obstruct Pulmon Dis. 2011;6:533–542. | ||
Ford ES, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state-specific medical and absenteeism costs of COPD among adults aged >/= 18 years in the United States for 2010 and projections through 2020. Chest. 2015;147(1):31–45. | ||
GSK. ANORO™ ELLIPTA® [prescribing information]. 2014. Available from: https://www.gsksource.com/gskprm/htdocs/documents/ANORO-ELLIPTA-PI-MG.PDF. Accessed June 2015. | ||
GSK [webpage on the Internet]. ANORO™ ELLIPTA® summary of product characteristics; 2014. Available from: http://www.medicines.org.uk/emc/medicine/28949#INDICATIONS. Accessed June 2015. | ||
Blair HA, Deeks ED. Umeclidinium/vilanterol: a review of its use as maintenance therapy in adults with chronic obstructive pulmonary disease. Drugs. 2015;75(1):61–74. | ||
Decramer M, Anzueto A, Kerwin E, et al. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: results from two multicentre, blinded, randomised controlled trials. Lancet Respir Med. 2014;2(6):472–486. | ||
Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respir Med. 2013;107(10):1538–1546. | ||
Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. | ||
GOLD. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. 2013. Available from: http://www.atsjournals.org/doi/abs/10.1164/rccm.201204-0596PP. Accessed February 2017. | ||
Hurst JR, Vestbo J, Anzueto A, et al; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. | ||
Shavelle RM, Paculdo DR, Kush SJ, Mannino DM, Strauss DJ. Life expectancy and years of life lost in chronic obstructive pulmonary disease: findings from the NHANES III Follow-up Study. Int J Chron Obstruct Pulmon Dis. 2009;4:137–148. | ||
Diette GB, Dalal AA, D’Souza AO, Lunacsek OE, Nagar SP. Treatment patterns of chronic obstructive pulmonary disease in employed adults in the United States. Int J Chron Obstruct Pulmon Dis. 2015;10:415–422. | ||
Green ME, Natajaran N, O’Donnell DE, et al. Chronic obstructive pulmonary disease in primary care: an epidemiologic cohort study from the Canadian Primary Care Sentinel Surveillance Network. CMAJ Open. 2015;3(1):E15–E22. | ||
Jones C. ANORO™ ELLIPTA™ Umeclidinium/Vilanterol Inhalation Powder 62.5/25 mcg; 2013. Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Pulmonary-AllergyDrugsAdvisoryCommittee/UCM368638.pdf. Accessed June 2015. | ||
Spencer M, Briggs AH, Grossman RF, Rance L. Development of an economic model to assess the cost effectiveness of treatment interventions for chronic obstructive pulmonary disease. Pharmacoeconomics. 2005;23(6):619–637. | ||
Celli B, Crater G, Kilbride S, et al. Once-daily umeclidinium/vilanterol 125/25 mcg in COPD: a randomized, controlled study. Chest. 2014;145(5):981–991. | ||
Kochanek KD, Xu J, Murphy SL, Minino AM, Kung HC. Deaths: final data for 2009. Natl Vital Stat Rep. 2011;60(3):1–116. | ||
Boehringer Ingelheim. SPIRIVA® HandiHaler® [prescribing information]. 2014. Available from: http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing+Information/PIs/Spiriva/Spiriva.pdf. Accessed September 2015. | ||
Boehringer Ingelheim. Combivent® [prescribing information]. 2014. Available from: http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing+Information/PIs/Combivent+Respimat/CMVTRSPT.pdf. Accessed September 2015. | ||
Wolters Kluwer [webpage on the Internet]. Medi-Span® 2.0 Price Rx Electronic Version; 2015. Indianapolis, IN: Wolters Kluwer. Available from: https://pricerx.medispan.com/. Accessed February 8, 2016. | ||
Yu AP, Yang H, Wu EQ, Setyawan J, Mocarski M, Blum S. Incremental third-party costs associated with COPD exacerbations: a retrospective claims analysis. J Med Econ. 2011;14(3):315–323. | ||
Centers for Disease Control and Prevention [webpage on the Internet]. Adult Appropriate Antibiotic Use Summary: Physician Information Sheet. Available from: http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-approp-summary.html. Accessed September 2015. | ||
Ingenix. The Essential RBRVS (2013): A Comprehensive Listing of RBRVS Values for CPT and HCPCS Codes. New York, NY: St. Anthony Publishing; 2013. | ||
US Bureau of Labor Statistics. US Department of Labor [webpage on the Internet]. US city average, not seasonally adjusted medical care. Available from: http://data.bls.gov/PDQ/outside.jsp?survey=cu. Accessed October 2015. | ||
Hettle R, Wouters H, Ayres J, et al. Cost-utility analysis of tiotropium versus usual care in patients with COPD in the UK and Belgium. Respir Med. 2012;106(12):1722–1733. | ||
Hoogendoorn M, Kappelhoff BS, Overbeek JA, Wouters EF, Rutten-van Molken MP. Which long-acting bronchodilator is most cost-effective for the treatment of COPD? Neth J Med. 2012;70(8):357–364. | ||
Oostenbrink JB, Rutten-van Molken MP, Monz BU, FitzGerald JM. Probabilistic Markov model to assess the cost-effectiveness of bronchodilator therapy in COPD patients in different countries. Value Health. 2005;8(1):32–46. | ||
Rutten-van Molken MP, Oostenbrink JB, Miravitlles M, Monz BU. Modelling the 5-year cost effectiveness of tiotropium, salmeterol and ipratropium for the treatment of chronic obstructive pulmonary disease in Spain. Eur J Health Econ. 2007;8(2):123–135. | ||
Eklund O, Afzal F, Borgstrom F. Cost-effectiveness of tiotropium versus usual care and glycopyrronium in the treatment of chronic obstructive pulmonary disease in Sweden. Cost Eff Resour Alloc. 2015;13:13. | ||
Wurst KE, Punekar YS, Shukla A. Treatment evolution after COPD diagnosis in the UK primary care setting. PLoS One. 2014;9(9):e105296. | ||
Miyazaki M, Nakamura H, Takahashi S, et al; Keio COPD Comorbidity Research (K-CCR) Group. The reasons for triple therapy in stable COPD patients in Japanese clinical practice. Int J Chron Obstruct Pulmon Dis. 2015;10:1053–1059. | ||
Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. | ||
Hoogendoorn M, Feenstra TL, Asukai Y, et al. Cost-effectiveness models for chronic obstructive pulmonary disease: cross-model comparison of hypothetical treatment scenarios. Value Health. 2014;17(5):525–536. | ||
Huurne KK, Movig K, van der Valk P, van der Palen J, Brusse-Keizer M. Differences in adherence to common inhaled medications in COPD. COPD. 2015;12(6):643–648. | ||
Trudo F, Kern DM, Davis JR, et al. Comparative effectiveness of budesonide/formoterol combination and tiotropium bromide among COPD patients new to these controller treatments. Int J Chron Obstruct Pulmon Dis. 2015;10:2055–2066. | ||
American Medical Association (AMA). Current Procedural Terminology (CPT). Chicago, IL: AMA Press; 2013. |
Supplementary materials
Methods
Estimates of disease transitions were based on age, average height, percentage of the COPD population that was female, average percentage predicted forced expiratory volume in 1 second (FEV1) among patients in the health state at start of model, average predicted normal FEV1, and annual rate of decline as observed among patients in the different disease severity health states in the ECLIPSE study. Reference equations were also used to estimate predicted normal FEV1 in males and females (included subsequently).
To calculate disease progression transition probabilities, the method detailed in Spencer et al1 was followed (Tables S1–S4).
- T = (predFEV1 × (gamma − tau))/(delta − tau × beta) where predFEV1 is the predicted normal FEV1 patient population, gamma is the percentage that actual FEV1 at baseline is of predicted normal FEV1, delta is the annual decline in lung function in patients with COPD, T is the time (in years) from when patients start in a health state until patients change to a new health state, tau is the percentage of predicted FEV1 threshold at which patients enter a new health state, beta is the rate of decline for a normal patient without COPD.
 | Table S1 Transition probabilities for UMEC/VI |
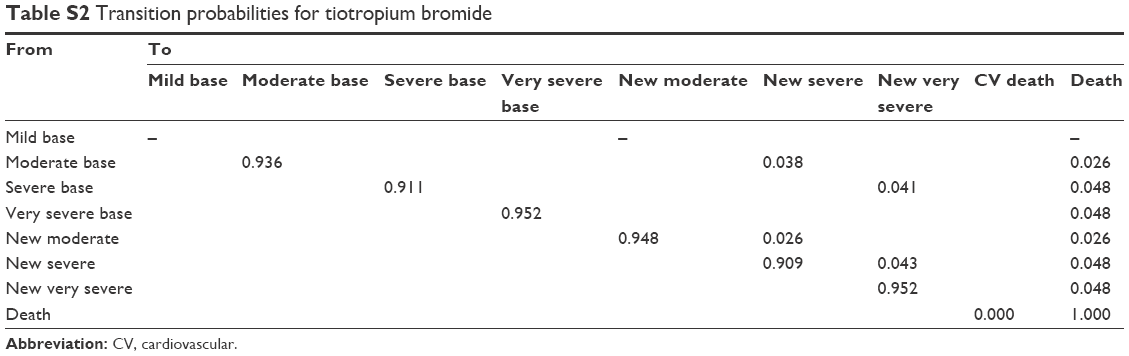 | Table S2 Transition probabilities for tiotropium bromide |
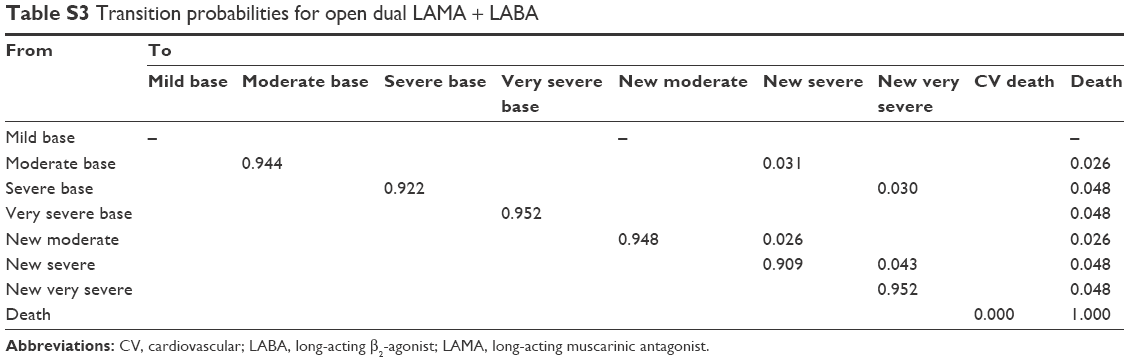 | Table S3 Transition probabilities for open dual LAMA + LABA |
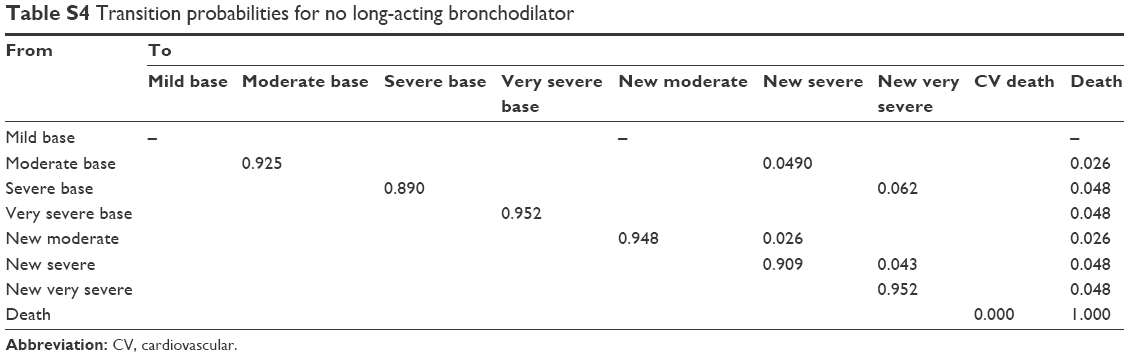 | Table S4 Transition probabilities for no long-acting bronchodilator |
The following National Health and Nutrition Examination Survey/Hankinson reference equation was also used:2
- Predicted FEV1% = predicted FEV1/predicted forced vital capacity (FVC)
Predicted FVC men, age to 19
= −0.2584 − 0.20415 × Age + 0.010133 × Age × Age + 0.00018642 × Height (in cm) × Height (in cm)
Predicted FVC men, age 20+
= −0.1933 + 0.00064 × Age − 0.000269 × Age × Age + 0.00018642 × Height (in cm) × Height (in cm)
Predicted FVC women
= −0.3560 + 0.01870 × Age − 0.000382 × Age × Age + 0.00014815 × Height (in cm) × Height (in cm)
Predicted FEV1 men, age to 19
= −0.7453 − 0.04106 × Age + 0.004477 × Age × Age + 0.00014098 × Height (in cm) × Height (in cm)
Predicted FEV1 men, age 20+
= 0.5536 − 0.01303 × Age − 0.000172 × Age × Age + 0.00014098 × Height (in cm) × Height (in cm)
Predicted FEV1 women
= 0.4333 − 0.00361 × Age − 0.000194 × Age × Age + 0.00011496 × Height (in cm) × Height (in cm)
Change in trough FEV1 (L) compared with no long-acting treatment for each maintenance treatment was used to increase FEV1 upon initiation of treatment and thus patients on maintenance treatment remained in less severe health states longer than patients on no long-acting treatment. The changes in trough FEV1 (at 24 hours) for umeclidinium/vilanterol (UMEC/VI) compared with tiotropium were obtained from the three clinical studies, and the estimate of change in trough FEV1 for no long-acting beta-2 agonist treatment was taken from GSK study DB113373, which compared UMEC/VI with a no-treatment arm where short-acting maintenance was allowed to treat short-term symptoms. Transition probabilities in years subsequent to year 1 were adjusted based on increased risk of death due to age.
The “moderate base” case represents transition probabilities of patients at the start of the model, in the context of their improvements in FEV1, which would be specific to their therapy regimen. The “moderate new” case, on the other hand, represents transition probabilities for patients newly transitioned into a given health state during the course of the model time horizon. Since these probabilities are not specific to a given drug, the values are the same for all drugs.
References
Spencer M, Briggs AH, Grossman RF, Rance L. Development of an economic model to assess the cost effectiveness of treatment interventions for chronic obstructive pulmonary disease. Pharmacoeconomics. 2005;23(6):619–637. | ||
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159(1):179–187. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.