Back to Journals » International Journal of Women's Health » Volume 17
Cost-Effectiveness Analysis of Multiple Micronutrient Supplementation (MMS) Compared to Iron Folic Acid (IFA) in Pregnancy: A Systematic Review
Authors Alfiani F ![]() , Utami AM
, Utami AM ![]() , Zakiyah N
, Zakiyah N ![]() , Daud NAA
, Daud NAA ![]() , Suwantika AA
, Suwantika AA ![]() , Puspitasari IM
, Puspitasari IM ![]()
Received 16 August 2024
Accepted for publication 18 February 2025
Published 6 March 2025 Volume 2025:17 Pages 639—649
DOI https://doi.org/10.2147/IJWH.S489159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Fitri Alfiani,1,2 Auliasari Meita Utami,3 Neily Zakiyah,3,4 Nur Aizati Athirah Daud,5 Auliya A Suwantika,3,4,6 Irma M Puspitasari3,4
1Doctoral Program in Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Bandung, Indonesia; 2Faculty of Health Science, Universitas Muhammadiyah Cirebon, Cirebon, Indonesia; 3Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Bandung, Indonesia; 4Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Bandung, Indonesia; 5Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, Penang, Malaysia; 6Center for Health Technology Assessment, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Neily Zakiyah, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Bandung Sumedang KM 21, Jatinangor, 45363, Indonesia, Tel/Fax +62-22-7796200, Email [email protected]
Introduction: Multiple micronutrient deficiencies might increase the adverse outcome during pregnancy and after birth. Considering the WHO recommendations since 2016 and scientific evidence from previous studies that multiple-micronutrient supplementation (MMS) is more effective than iron folic acid (IFA) in improving pregnant women’s health, it is imperative to conduct an economic evaluation to assess the cost-effectiveness of MMS compared with IFA.
Methods: We conducted a systematic review from PubMed and Scopus to identify the cost-effectiveness analyses of MMS compared to IFA for pregnant women up to January 2024. Data extraction included specific study characteristics, input parameters, cost elements, cost-effectiveness results, and key drivers of uncertainty. This systematic review adhered to The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Results: After removing 111 duplicates and following the screening process on the title and abstract of 1201 records, resulting in 125 full-text articles assessed for eligibility, a total of 5 studies fulfilled the inclusion criteria and were included in the review. All included studies were from low- and middle-income countries and demonstrated that MMS compared to IFA for pregnant women is cost-effective and even very cost-effective in some countries. All included studies implemented cost-effectiveness analysis (CEA) and estimated its cost-effectiveness using incremental cost-effectiveness ratio (ICER) per disability-adjusted life years (DALY) averted. Results suggested that the transition from IFA to MMS was cost-effective. The range of ICER per DALY averted in this study is USD 3.62 to USD 1024, depending on the scenario. Overall, the main determinant influencing cost-effectiveness was the cost of MMS procurement.
Conclusion: Our findings highlight that transitioning from IFA to MMS in certain conditions has been proven cost-effective, emphasizing this intervention’s economic viability. MMS price and micronutrient deficiency-related disease burden are important determinants in assessing cost-effectiveness.
Registration: PROSPERO CRD42022319470.
Keywords: cost-effectiveness, economic evaluation, iron-folic acid, multiple micronutrient supplementation, pregnant woman
Introduction
Nutrition has a significant impact on the physical well-being, mental health, and general quality of life of pregnant women.1 Multiple micronutrient intakes should be adequate during pregnancy for maternal health and fetal development.2–4 Multiple micronutrient deficiencies might increase the risk of complications during pregnancy and after birth, especially anemia during pregnancy which is estimated at 40% globally.5,6 Multiple micronutrient deficiencies can also have adverse effects on pregnancy outcomes including fetal loss, preterm birth, small gestational age, increased risk of neural tube defects, preeclampsia, low birth weight (LBW), postpartum depression, and greater risk of death.7–9 These are associated with immune development and suboptimal neurodevelopmental outcomes in children.10,11 According to the World Health Organization’s (WHO) recommendations, providing MMS during prenatal care is a proactive measure to address the nutritional requirements of expectant mothers.3,12 Compared to the iron folic acid (IFA), a statistically significant reduction in preterm birth and LBW13 was observed, anemic women who received MMS during pregnancy had a greater reduction in the risk of LBW (19%), small gestational age (8%), and 6-month mortality (29%).2 Furthermore, infants born to mothers who received MMS had a significant reduction in neonatal mortality (15%), 6-month mortality (15%), and infant mortality (13%), compared with infants born to IFA-treated mothers.2 In addition, pregnant women’s adherence to MMS (95.4%) was significantly higher than IFA (92.2%).14 Considering the WHO recommendations since 2016 and scientific evidence from previous studies, MMS is more effective than IFA in helping improve pregnant women’s health.13,15–18 Transitioning from IFA to MMS tablets in different countries might take multiple years and require essential resources, involving human resources and funding.19 The costs related to transitioning from IFA to MMS would rise,12 so it is crucial to evaluate the cost-effectiveness of MMS compared with IFA. Therefore, the objective of this study was to systematically review all published studies on the cost-effectiveness analysis of MMS compared to IFA for pregnant women.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used for this systematic review20 and has been registered in the PROSPERO database (CRD42022319470).
Search Strategy
The systematic search was conducted in two databases (Scopus and PubMed) for all published studies comparing the cost-effectiveness of MMS to IFA for pregnant women. The following keywords were used for the search: (“multiple micronutrient supplementation” [Mesh] OR MMS) OR ((“Iron Folic Acid” [Mesh] OR IFA) AND (Pregnan*) AND (Costs and Cost Analysis OR Cost-Benefit Analysis OR Cost Effectiveness OR Economic Evaluation OR Economic Analysis OR Cost Evaluation). The screening process was conducted in two steps, ie, initial screening based on title and abstracts followed by full-text screening. The screening processes were performed by two of the authors (F.A. and A.M.I.).
Inclusion and Exclusion Criteria
The following inclusion criteria were used for the screening process: 1) full-text economic evaluation studies on the cost-effectiveness of MMS compared to IFA for pregnant women, and 2) published in English. Meanwhile, studies on animals, protocols, conference proceedings, review articles, and studies available in abstracts only were excluded.
Quality Assessment
The Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement was applied to assess the reporting quality of each included study. It consists of a checklist of 24 criteria, to assist appropriate reporting of economic evaluation studies. The criteria were grouped into 6 categories: title and abstract, introduction, methods, results, discussion, and others.21 Two independent reviewers (F.A. and A.M.I.) evaluated each study, and disagreements were resolved through discussion with the other reviewer. Specific attention was given to the completeness of reporting in key sections (eg, whether methods were clearly described or whether results addressed all relevant outcomes).
Results
Systematic Search
The initial search conducted up to June 2024 yielded 1312 records from PubMed and Scopus. After removing 111 duplicates, 1201 articles underwent title and abstract screening, resulting in the exclusion of 1076 records. Among 125 full-text screened, 42 articles were excluded due to non-economic evaluations, 72 articles were excluded due to non-MMS studies, and 6 articles were excluded since the research did not focus on pregnant women. As a result, 5 studies were finally included in the review (Figure 1).
 |
Figure 1 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection. Note: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. |
Characteristics of Included Studies
Our 5 included studies were from 6 different countries, all classified as low-income or lower-middle-income countries. Mali and Burkina Faso are two countries classified as low-income, while Bangladesh, India, Pakistan, and Tanzania are classified as lower-middle-income, according to the World Bank data.22,23 The initial two studies focused only on Bangladesh as the context for a health economic analysis.24,25 The third study focused on Bangladesh and Burkina Faso.12 The fourth study involved Pakistan, India, and Bangladesh.26 The fifth study involved India, Pakistan, Mali, and Tanzania.27 The oldest study that appeared from our search was from 2015, addressing the CEA of MMS intervention in Bangladesh, and the most recent one was from 2022, investigating the cost-effectiveness of MMS in India, Pakistan, Mali, and Tanzania. The most relevant aspects of these studies are presented in Table 1.
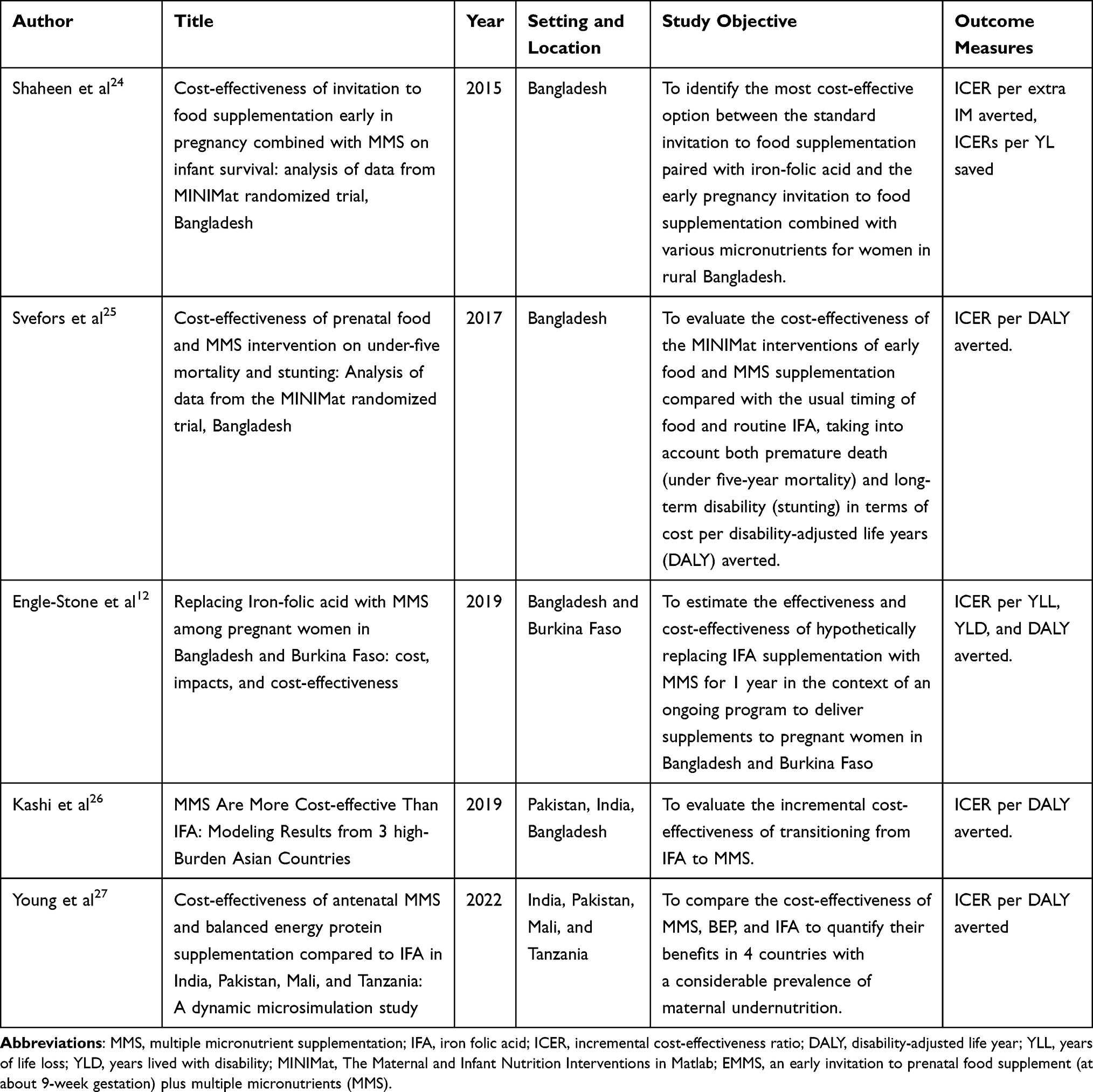 |
Table 1 Summary of 5 Selected Articles on Cost-Effectiveness Analysis of MMS Compared to IFA |
Study Design and Data Collection
All included studies provided information on MMS’s potential costs and consequences compared to IFA. Four of the five included studies in the review used the Bangladesh setting to analyze cost-effectiveness. Two studies in Bangladesh by Shaheen et al and Svefors et al24,25 estimated cost-effectiveness by comparing six scenarios, including MMS with food supplementation starting at either 9 weeks (EMMS) or 20 weeks (UMMS) of pregnancy, and IFA with either 60 mg (EFe60F, UFe60F) or 30 mg (EFe30F, UFe30F) of iron, combined with food supplementation starting at 9 or 20 weeks of pregnancy, considering cost per disability-adjusted life years (DALY) averted.24,25
A cost-effectiveness study of MMS compared to IFA in Bangladesh and Burkina Faso by Engle-Stone et al was conducted by comparing two scenarios. The first scenario estimates cost-effectiveness based on 100% coverage and adherence, assuming all pregnant women received and used MMS. The second scenario was on current IFA coverage in Bangladesh (60.7% urban area, 47.4% rural area) and Burkina Faso (16.0% urban area, 8.4% rural area). The population-based model was used in urban areas and rural areas to estimate the cost and clinical outcome in each scenario and consider the cost per DALY averted in Bangladesh and Burkina Faso.12
A study by Kashi et al evaluated the cost-effectiveness of MMS compared to IFA using Monte Carlo Simulation (Lancet Scenario28 that only considered studies that compared MMS with IFA and Cochrane Scenario29 that compared MMS with IFA or iron alone) by calculating cost per DALY averted.26 A study in India, Pakistan, Mali, and Tanzania by Young et al was conducted to compare the cost-effectiveness of MMS, Balanced Energy Protein (BEP), and IFA to quantify their benefits.27 More information about the study design and data collection of selected studies is presented in Table 2.
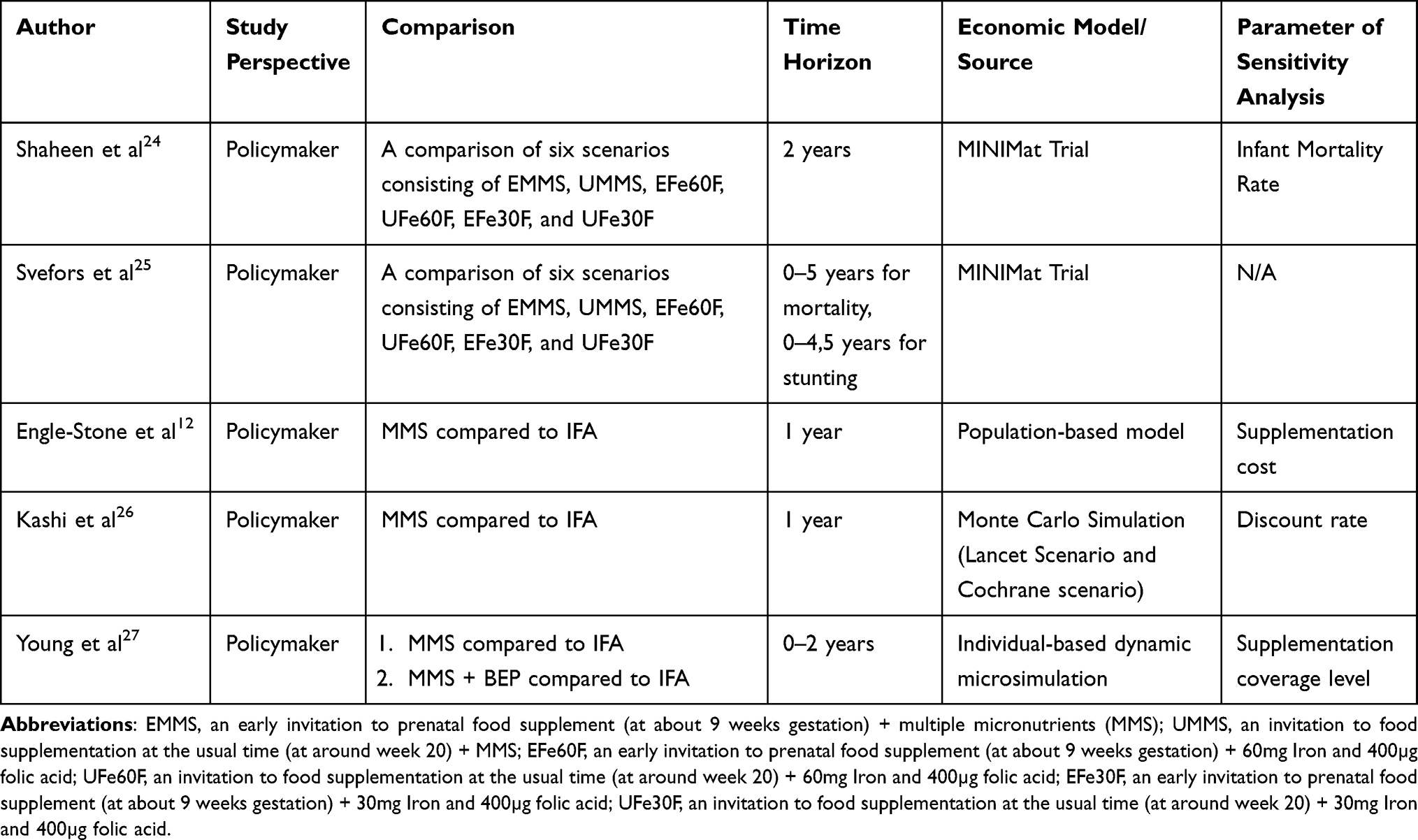 |
Table 2 Methodological Characteristics of 5 Selected Articles |
Time Horizon and Economic Modeling
The time horizons used are one year, two, and five years (see Table 2). This time horizon is chosen as a framework to evaluate the use of MMS from pregnancy until birth. Furthermore, postnatal analysis was conducted at 1-year and 5-year intervals to assess the health of both the mother and the infant. Shaheen et al and Svefors et al24,25 used the Maternal and Infant Nutrition Interventions in Matlab (MINIMat) Trial model, a database that belongs to Bangladesh, in their publication. The economic model employed in Engle-Stone et al12 suggests assumptions regarding the costs associated with transitioning from IFAS to MMS. Meanwhile, The Lancet scenario and the Cochrane scenario are the models employed in the publications of Kashi et al and Young et al.26,27 Only the publications by Svefors et al did not apply sensitivity analysis in the study.25
Cost Estimation
The inclusion of cost is essential in economic evaluation studies, particularly in low- and middle-income countries (LMICs) where resources are limited. All included studies estimated the supplementation cost. The costs associated with the shift from IFA to MMS would increase. The first two studies conducted in Bangladesh by Shaheen et al and Svefors et al, along with a study in Pakistan, India, and Bangladesh by Kashi et al, assess the costs associated with supplementation, including both micronutrients and food supplements, as well as the transition costs encompassing staff, training, administration, capital, community volunteer time, patient cost, program cost, and ongoing activities.24–26 Additionally, two studies by Engle-Stone et al (Bangladesh and Burkina Faso) and Young et al (India, Pakistan, Mali, and Tanzania) focus only on the costs related to supplementation.12,27 Further details are presented in Table 3.
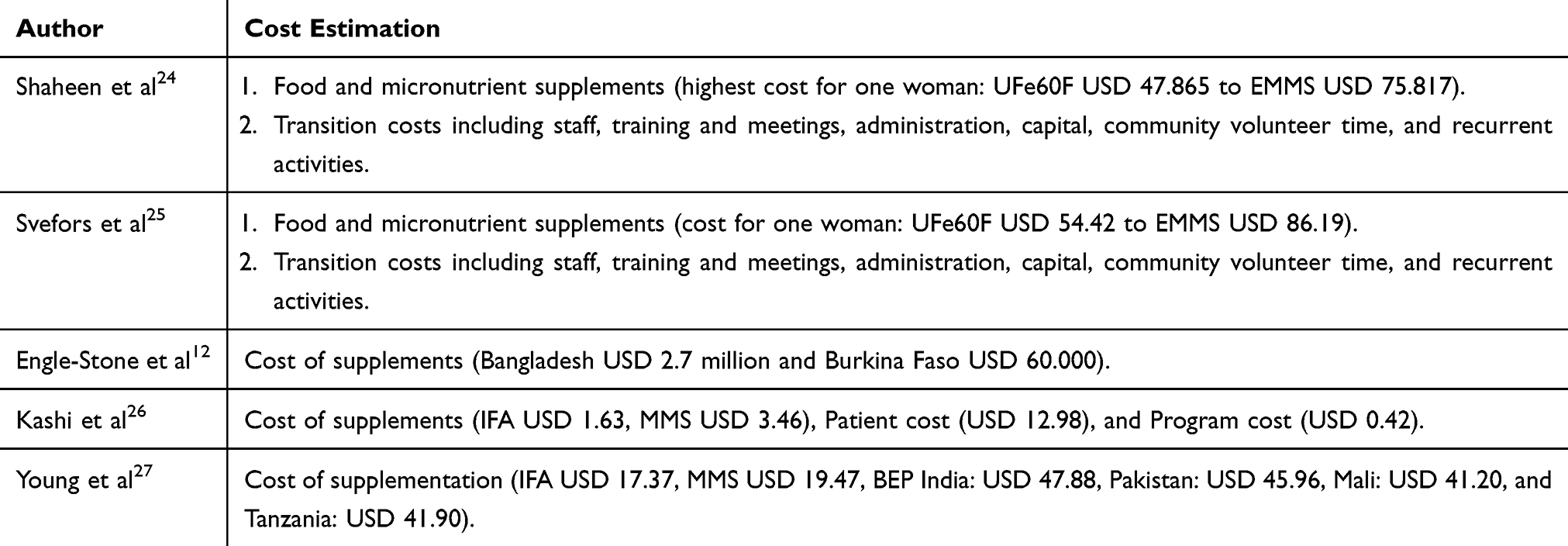 |
Table 3 Cost Components |
Primary Outcomes
According to five studies included in this review, the transition from IFA supplementation to MMS for pregnant women has been shown to be cost-effective. This assessment is based on the commonly used threshold of up to three times the GDP per capita, as recommended by the WHO, in the absence of country-specific cost-effectiveness thresholds for these countries.12,24–27,30 A study by Shaheen et al in Bangladesh conducted calculations utilizing delivery modes including for a non-governmental organization (NGO)-run community nutrition centers (CNCs), government-run CNCs, and a hypothetical highest-cost scenario. The analysis demonstrated cost-effective outcomes with ICER values for one additional IM averted by transitioning from UFe60F to EMMS were USD 907, USD 797, and USD 1024, respectively.24 Meanwhile, Svefor et al discovered that the implementation of EMMS supplementation was highly cost-effective than UFe60F with an ICER value per 5 years and lifetime DALY averted USD 187 and USD 24, respectively. The ICER value’s results are far below Bangladesh’s per capita income of USD 1190. Transitioning from UFe60F to EMMS is deemed reasonable in low-resource settings and is viable from both public health and economic points of view.25 Likewise, in a study by Engle-Stone et al in Bangladesh, changing from IFAS to MMS might prevent 15,000 newborn deaths and 30,000 preterm births, whereas, in Burkina Faso, it could avoid 5000 newborn deaths and 5000 preterm cases. In Bangladesh and Burkina Faso, the cost per DALY averted by changing from IFA to MMS ranged from USD 3.62 to USD 13.25 and USD 3.02 to USD 15.21, respectively, based on the employed scenario.12
Research done in Pakistan, India, and Bangladesh by Kashi et al found that transitioning from IFA to MMS resulted in ICER values of USD 41.54, USD 31.62, and USD 21.26 per DALY avoided.26 These findings support the conclusion that transitioning from IFA to MMS is cost-effective when evaluated against each country’s respective threshold of up to three times GDP per capita, as recommended by the WHO.26,30 According to a dynamic microsimulation study involving Tanzania, Pakistan, Mali, and India by Young et al providing MMS supplements to 90% of pregnant women who attend antenatal care (ANC) lowers morbidity and death among children under two. Combining MMS with targeted BEP results in a greater reduction of DALY than universal MMS when measured against baseline IFA. The ICER per DALY averted, based on current evidence for each country, is as follows: Tanzania: USD 245; Mali: USD 73; Pakistan: USD 54; India: USD 83.27 Detailed information is provided in Table 4.
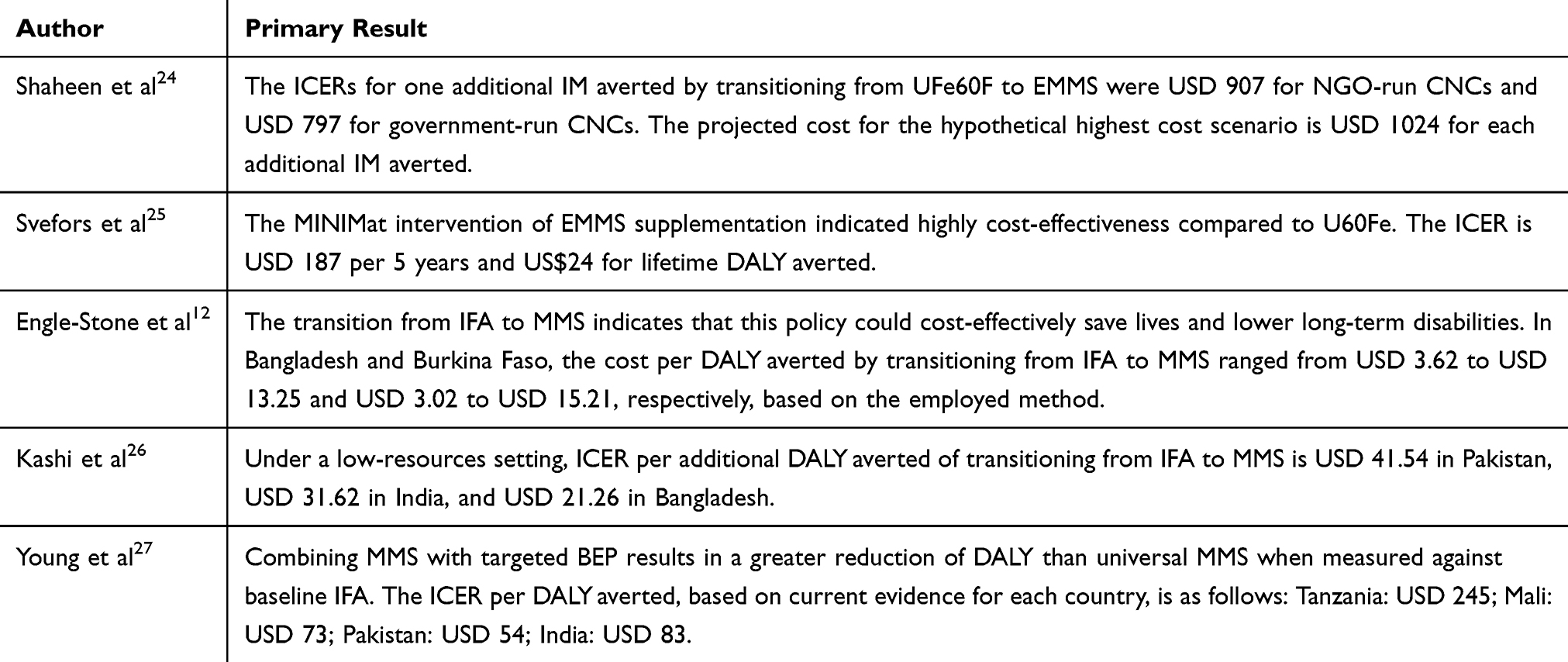 |
Table 4 Primary Outcomes |
Quality of Reporting
The section’s fulfillment of the reporting criterion based on the CHEERS checklist varied. Figure 2 illustrates the proportion of each CHEERS checklist item reported adequately or not at all by each study included in the review. All studies adequately reported the following sections: introduction, study perspective, setting, comparator, resources, and costs. The target population and time horizon were described in all studies. Most studies provide detailed information on how resources and costs were collected and estimated. Furthermore, all studies provided the study perspective when presenting included costs. Four studies presented policymaker’s perspectives and one study presented payer’s perspectives. All studies reported the incremental cost-effectiveness ratio of MMS compared to IFA. In addition, it has been found that only a few studies have reported the rationale for using such models, despite most studies have reported the choice of economic models. Only two studies mentioned potential conflicts of interest.
 |
Figure 2 The result of the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) assessment. |
Discussion
This systematic review demonstrated that transitioning IFA to MMS for improving pregnant women’s health would be a cost-effective intervention in Bangladesh, India, Pakistan, Mali, Tanzania, and Burkina Faso. The cost of MMS and the burden of micronutrient deficiency-related disease appeared as the most sensitive parameters influencing cost-effectiveness. Further, scientific evidence is needed to substantiate its potential benefits, as economic evaluation studies on MMS remain highly limited.31,32
From the included studies, a modeling approach was predominantly used to predict the economic impact of MMS by considering several alternative scenarios. Model-based evaluations offer an evidence-based method to estimate the cost-effectiveness of interventions, enabling policymakers to allocate limited resources efficiently, particularly in resource-constrained setting like LMICs. In these contexts, where empirical data may be scarce or incomplete, models can integrate information from multiple sources, including regional studies, databases, and global estimates.12,24–27,33
All included studies perform different economic models. Cost-effectiveness values were calculated in particular by comparing the use of MMS with IFA under various scenarios. The values were determined by cost/DALY averted. Two studies in Bangladesh applied six different scenarios to determine the cost-effectiveness of MMS compared to IFA. For DALY averted, one study used the infant mortality rate, while the other used years of life loss (YLL) (ie life expectancy at birth) and years lived with disability (YLD) (ie stunted children from 0 to 5 years). The other three studies assessed cost-effectiveness using a population-based model, Monte Carlo simulation, and individual-based dynamic microsimulation. All included studies have a perspective determination based on the perspective of policymakers as this type of approach is required in health technology assessment to develop public policies related to improving maternal health in several countries.34,35 In terms of sensitivity analysis, several studies considered ICER per DALY averted were sensitive to changes in supplementation cost, discount rate, supplementation coverage level, and infant mortality rate (burden disease).12,24–27
Although MMS has been recommended by the WHO6 and has the potential to reduce the burden on maternal and child health, it has not been included yet in existing maternal and child health programs in many countries. In addition, MMS is effective in reducing pregnancy risks including preterm birth, LBW, maternal and infant mortality rates due to micronutrient deficiency.2,5,7–9,36 To maximize the full benefits of this intervention, the level of adherence is critical.33 The level of adherence to MMS usage is better compared to IFA, 95.4%, and 92.2%, respectively.14 In some countries, such as LMICs, MMS might even be heavily covered by the government and have an impact on healthcare policies. Therefore, an economic evaluation study is required by the government as an essential aspect to consider in the decision-making process. It should be comprehensively assessed to enable policymakers to make decisions more appropriately while distributing budget and resources to maternal and child health programs.12,24–27,33 Systematically, transitioning from IFA to MMS tablets might take several years and require essential resources such as human and budget.19
The results of CEA of MMS compared to IFA in this study demonstrated that MMS can be considered a cost-effective intervention. In recommending new interventions, WHO has suggested using 1 to 3 GDP per capita as the cost-effective threshold; however, some have reasoned that this WHO threshold may still be too expensive and that thresholds of half GDP per capita are more acceptable. The average GDP per capita (2020 USD) in 2019 for low-income countries was USD 780 while that for LMICs was USD 2180.27,30 Applying WHO cost-effectiveness guidelines, transitioning from IFA to MMS is very cost-effective. It is additionally a beneficial intervention despite being applied in a pessimistic scenario or low-resource setting. It should be incorporated into a policy-maker framework. These recommendations should lead to policy-making that prioritizes pregnant women’s health. Making a good start in life during pregnancy is essential for living a healthy and longer life.37 Health improvements could be considered high in LMICs and globally if compared to economic ventures. Transitioning from IFA to MMS is the best scenario for improving maternal and child health that is possible to be implemented and adapted to specific country contexts and populations.24–26,38,39 Transitioning from IFA to MMS should be initiated to analyze methods to accelerate and then maintain national MMS coverage, adherence, and measurable health impact in each country.40
All five studies indicated that replacing IFA with MMS tablets would probably result in increased additional costs. Additional costs related to MMS procurement are one of the determinant factors of cost-effectiveness. Various factors can impact the prices of MMS, including regulation for procuring MMS, the volume and continuity of purchasing agreements for MMS, packaging types and tablet counts, and MMS coverage level for the population in each country.12,32,41–44 The capability to produce MMS locally for each LMIC should be started to acquire better pricing and increase MMS coverage.12,45
The results of this review are essential to policymakers. The results of this review provide scientific evidence that MMS is a cost-effective intervention compared to IFA for pregnant women despite being implemented in a pessimistic scenario or low-resource setting. Therefore, policymakers will be more capable to interpret and prioritize programs focused on improving mother and child health. Health improvements provided during pregnancy and the early years might reduce the risk of low-grade health and disease, increasing life chances.37
The CHEERS checklist was applied in this review to evaluate the quality of reporting in the included studies. The quality of reporting is an essential component of economic evaluation studies since it ensures accountability. The majority of the research already met the criteria listed in the checklist.
To the best of our knowledge, this study is one of the first reviews assessing the cost-effectiveness analysis of MMS compared to IFA. Systematic methods were implemented to identify relevant studies from electronic databases.
Certainly, this systematic review has some limitations. Firstly, even though systematic approaches were used in both the literature search and screening, it is possible that some studies published in languages other than English were not taken into account. Second, the limited number of studies discussing the cost-effectiveness analysis of MMS compared to IFA, consequently the evidence acquired is limited to only a few studies.
Conclusion
In some countries, maternal and child health remains a burden due to micronutrient deficiencies. Adequate intake of micronutrients is required during pregnancy. The transitioning IFA to MMS for pregnant women performs to be a cost-effective intervention depending on the scenario. MMS price and micronutrient deficiency-related disease burden are important determinants in assessing cost-effectiveness.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shenoy S, Sharma P, Rao A, et al. Evidence-based interventions to reduce maternal malnutrition in low and middle-income countries: a systematic review. Front Health Serv. 2023;3:1155928. doi:10.3389/frhs.2023.1155928
2. Bourassa MW, Osendarp SJM, Adu-Afarwuah S, et al. Review of the evidence regarding the use of antenatal multiple micronutrient supplementation in low- and middle-income countries. Ann N Y Acad Sci. 2019;1444(1):6–21. doi:10.1111/nyas.14121
3. Tuncalp Ö, Rogers LM, Lawrie TA, et al. WHO recommendations on antenatal nutrition: an update on multiple micronutrient supplements. BMJ Glob Heal. 2020;5(7):e003375. doi:10.1136/bmjgh-2020-003375
4. Gomes F, Askari S, Black RE, et al. Antenatal multiple micronutrient supplements versus iron-folic acid supplements and birth outcomes: analysis by gestational age assessment method. Matern Child Nutr. 2023;19(3). doi:10.1111/mcn.13509
5. Berti C, Gaffey MF, Bhutta ZA, Cetin I. Multiple‐micronutrient supplementation: evidence from large‐scale prenatal programmes on coverage, compliance and impact. Matern Child Nutr. 2018;14:e12531. doi:10.1111/mcn.12531
6. World Health Organization. WHO antenatal care recommendations for a positive pregnancy experience. nutritional intervention update: multiple micronutrient supplements during pregnancy. WHO; 2020.
7. Massari M, Novielli C, Mandò C, et al. Multiple micronutrients and docosahexaenoic acid supplementation during pregnancy: a randomized controlled study. Nutrients. 2020;12(8):1–16. doi:10.3390/nu12082432
8. Petry CJ, Ong KK, Hughes IA, Dunger DB. Multiple micronutrient supplementation during pregnancy and increased birth weight and skinfold thicknesses in the offspring: the Cambridge baby growth study. Nutrients. 2020;12(11):1–13. doi:10.3390/nu12113466
9. Priliani L, Prado EL, Restuadi R, Waturangi DE, Shankar AH, Malik SG. Maternal multiple micronutrient supplementation stabilizes mitochondrial DNA copy number in pregnant women in Lombok, Indonesia. J Nutr. 2019;149(8):1309–1316. doi:10.1093/jn/nxz064
10. Sudfeld CR, Bliznashka L, Salifou A, et al. Evaluation of multiple micronutrient supplementation and medium-quantity lipid-based nutrient supplementation in pregnancy on child development in rural Niger: a secondary analysis of a cluster randomized controlled trial. PLoS Med. 2022;19(5):1–17. doi:10.1371/journal.pmed.1003984
11. Moore SE, Fulford AJ, Darboe MK, Jobarteh ML, Jarjou LM, Prentice AM. A randomized trial to investigate the effects of pre-natal and infant nutritional supplementation on infant immune development in rural Gambia: the ENID trial: early Nutrition and Immune Development. BMC Pregnancy Childbirth. 2012;12:107. doi:10.1186/1471-2393-12-107
12. Engle-Stone R, Kumordzie SM, Meinzen-Dick L, Vosti SA. Replacing iron-folic acid with multiple micronutrient supplements among pregnant women in Bangladesh and Burkina Faso: costs, impacts, and cost-effectiveness. Ann N Y Acad Sci. 2019;1444(1):35–51. doi:10.1111/nyas.14132
13. West KP, Shamim AA, Mehra S, et al. Effect of Maternal multiple micronutrient vs iron-folic acid supplementation on infant mortality and adverse birth outcomes in rural Bangladesh: the JiVitA-3 randomized trial. JAMA. 2014;312(24):2649–2658. doi:10.1001/jama.2014.16819
14. Aguayo VM, Koné D, Bamba SI, et al. Acceptability of multiple micronutrient supplements by pregnant and lactating women in Mali. Public Health Nutr. 2005;8(1):33–37. doi:10.1079/PHN2005665
15. Allen LH, Peerson JM, Adou P, et al. Impact of multiple micronutrient versus iron-folic acid supplements on maternal anemia and micronutrient status in pregnancy. Food Nutr Bull. 2009;30(4 SUPPL):527–532. doi:10.1177/15648265090304S407
16. Haider BA, Yakoob MY, Bhutta ZA. Effect of multiple micronutrient supplementation during pregnancy on maternal and birth outcomes. BMC Public Health. 2011;11(SUPPL. 3). doi:10.1186/1471-2458-11-S3-S19
17. Liu JM, Mei Z, Ye R, Serdula MK, Ren A, Cogswell ME. Micronutrient supplementation and pregnancy outcomes: double-blind randomized controlled trial in China. JAMA Intern Med. 2013;173(4):276–282. doi:10.1001/jamainternmed.2013.1632
18. Devakumar D, Fall CHD, Sachdev HS, et al. Maternal antenatal multiple micronutrient supplementation for long-term health benefits in children: a systematic review and meta-analysis. BMC Med. 2016;14(1). doi:10.1186/s12916-016-0633-3
19. Meinzen-dick L, Vosti SA. The evidence base cost-effectiveness of replacing iron-folic acid with multiple micronutrient supplements.
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372(71).doi:10.1136/bmj.n71
21. Husereau D, Drummond M, Petrou S, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Value Heal. 2013;16:e1–5. doi:10.1016/j.jval.2013.02.010
22. Low income | Data [Internet]. [cited November 18, 2023]. Available from: https://data.worldbank.org/income-level/low-income.
23. Lower middle income | data [Internet]. [cited November 19, 2023]. Available from: https://data.worldbank.org/income-level/lower-middle-income.
24. Shaheen R, Persson LÅ, Ahmed S, Streatfield PK, Lindholm L. Cost-effectiveness of invitation to food supplementation early in pregnancy combined with multiple micronutrients on infant survival: analysis of data from MINIMat randomized trial, Bangladesh. BMC Pregnancy Childbirth. 2015;15:125. doi:10.1186/s12884-015-0551-y
25. Svefors P, Selling KE, Shaheen R, Khan AI, Persson L-Å, Lindholm L. Cost-effectiveness of prenatal food and micronutrient interventions on under-five mortality and stunting: analysis of data from the MINIMat randomized trial, Bangladesh. PLoS One. 2018;13(2):e0191260. doi:10.1371/journal.pone.0191260
26. Kashi B, Godin CM, Kurzawa ZA, Verney AMJ, Busch-Hallen JF, De-Regil LM. Multiple micronutrient supplements are more cost-effective than iron and folic acid: modeling results from 3 high-burden Asian countries. J Nutr. 2019;149(7):1222–1229. doi:10.1093/jn/nxz052
27. Young N, Bowman A, Swedin K, et al. Cost-effectiveness of antenatal multiple micronutrients and balanced energy protein supplementation compared to iron and folic acid supplementation in India, Pakistan, Mali, and Tanzania: a dynamic microsimulation study. PLoS Med. 2022;19(2):e1003902. doi:10.1371/journal.pmed.1003902
28. Smith ER, Shankar AH, Wu LSF, et al. Modifiers of the effect of maternal multiple micronutrient supplementation on stillbirth, birth outcomes, and infant mortality: a meta-analysis of individual patient data from 17 randomised trials in low-income and middle-income countries. Lancet Glob Heal. 2017;5(11):e1090–100. doi:10.1016/S2214-109X(17)30371-6
29. Haider BA, Bhutta ZA. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst Rev. 2012;11(11):CD004905. doi:10.1002/14651858.CD004905.pub3
30. Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S. Thresholds for the cost–effectiveness of interventions: alternative approaches. Bull World Health Organ. 2015;93(2):118–124. doi:10.2471/BLT.14.138206
31. Supadmi W, Suwantika AA, Perwitasari DA, Abdulah R. Economic evaluations of dengue vaccination in Southeast Asia Region: evidence from a systematic review. Value Heal Reg Issues. 2019;18:132–144. doi:10.1016/j.vhri.2019.02.004
32. Zakiyah N, Insani WN, Suwantika AA, van der Schans J, Postma MJ. Pneumococcal vaccination for children in Asian countries: a systematic review of economic evaluation studies. Vaccines. 2020;8(3):1–18. doi:10.3390/vaccines8030426
33. Gomes F, Bourassa MW, Adu-Afarwuah S, et al. Setting research priorities on multiple micronutrient supplementation in pregnancy. Ann N Y Acad Sci. 2020;1465(1):76–88. doi:10.1111/nyas.14267
34. Briggs A, Sculpher M, Claxton K. Decision Modelling for Health Economic Evaluation. New York City, NY, United States: Oxford University Press Inc; 2006.
35. Kesehatan RIK. Pedoman Penerapan Kajian Farmakoekonomi. Jakarta: Kementerian Kesehatan Republik Indonesia; 2013.
36. Black RE, Dewey KG. Benefits of supplementation with multiple micronutrients in pregnancy. Ann N Y Acad Sci. 2019;1444(1):3–5. doi:10.1111/nyas.14088
37. Dundas R, Boroujerdi M, Browne S, et al. Evaluation of the Healthy Start voucher scheme on maternal vitamin use and child breastfeeding: a natural experiment using data linkage. Public Health Res. 2023;11(11):1–101.
38. Keats EC, Haider BA, Tam E, Bhutta ZA. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst Rev. 2019;2019(3).
39. Nutrition International. Policy Brief - Cost-Effectiveness of Transitioning From Iron and Folic Acid to Multiple Micronutrient Supplementation for Pregnancy. 2019:1–6
40. Hurley K, Achadi EL, Ajello C, et al. Prevention of child wasting in Asia: possible role for multiple micronutrient supplementation in pregnancy. Field Exch. 2020;2020(63):76–80.
41. UNICEF. Multiple Micronutrient Powder Supply and Market Update. Copenhagen, Denmark: UNICEF Supply Division; 2021.
42. MMA-TAG, MNF. Expert consensus on an open-access United Nations International Multiple Micronutrient Antenatal preparation-multiple micronutrient supplement product specification. Ann N Y Acad Sci. 2020;1470(1):3–13. doi:10.1111/nyas.14322
43. Paulden M, O’Mahony J, McCabe C. Determinants of change in the cost-effectiveness threshold. Med Decis Mak. 2017;37(2):264–276. doi:10.1177/0272989X16662242
44. Garcia-Casal MN, Estevez D, De-Regil LM. Multiple micronutrient supplements in pregnancy: implementation considerations for integration as part of quality services in routine antenatal care. Objectives, results, and conclusions of the meeting. Matern Child Nutr. 2018;14. doi:10.1111/mcn.12704
45. Monterrosa EC, Beesabathuni K, van Zutphen KG, et al. Situation analysis of procurement and production of multiple micronutrient supplements in 12 lower and upper middle-income countries. Matern Child Nutr. 2018;14. doi:10.1111/mcn.12500
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cost-Effectiveness Analysis and Priority Setting in the Transition from Iron-Folic Acid (IFA) to Multiple Micronutrient Supplementation (MMS) for Pregnant Women in Indonesia
Alfiani F, Utami AM, Zakiyah N, Daud NAA, Suwantika AA, Puspitasari IM
ClinicoEconomics and Outcomes Research 2025, 17:809-820
Published Date: 11 November 2025