Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Cost-Effectiveness Analysis of Gemtuzumab Ozogamicin for First-Line Treatment of Patients with Cd-33 Positive Acute Myeloid Leukaemia in Spain
Authors Mareque M, Montesinos P, Font P, Guinea JM ![]() , de la Fuente A, Soto J
, de la Fuente A, Soto J ![]() , Oyagüez I
, Oyagüez I ![]() , Brockbank J
, Brockbank J ![]() , Iglesias T, Llinares J, Sierra J
, Iglesias T, Llinares J, Sierra J
Received 15 January 2021
Accepted for publication 7 April 2021
Published 22 April 2021 Volume 2021:13 Pages 263—277
DOI https://doi.org/10.2147/CEOR.S302097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Maria Mareque, 1 Pau Montesinos, 2 Patricia Font, 3 José María Guinea, 4 Adolfo de la Fuente, 5 Javier Soto, 6 Itziar Oyagüez, 1 James Brockbank, 7 Tamara Iglesias, 6 Julia Llinares, 6 Jorge Sierra 8
1Pharmacoeconomics & Outcomes Research Iberia (PORIB), Madrid, Spain; 2Hospital Universitario La Fe, Valencia, Spain; 3Hospital General Universitario Gregorio Marañón, Madrid, Spain; 4Organización Sanitaria Integrada Araba, País Vasco, Spain; 5Hospital MD Anderson, Madrid, Spain; 6Pfizer, Madrid, Spain; 7RTI Health Solutions, Manchester, UK; 8Hospital Universitario de La Santa Creu i Sant Pau, Barcelona, Spain
Correspondence: Maria Mareque
Pharmacoeconomics & Outcomes Research Iberia (PORIB), Paseo Joaquín Rodrigo 4-I, Pozuelo de Alarcón, Madrid, 28224, Spain
Tel + 34 91 715 91 47
Fax + 34 91 715 94 69
Email [email protected]
Objective: To assess the incremental cost–utility ratio (ICUR) of gemtuzumab ozogamicin (GO) + standard of care (SOC) vs SOC alone for treatment of patients with de novo AML from a Spanish Health Service perspective.
Methods: A cohort state-transition model, with 12 health-states, was used to estimate the lifetime accumulated cost and benefits in terms of quality-adjusted-life-years (QALYs) in AML patients with favourable, intermediate, and unknown cytogenetic profiles. Patient profile was defined based on the ALFA-0701 trial. Therapeutic regimens were defined by 5 haematologists. SOC was assumed to be idarubicin and cytarabine, the combination most used in Spain. QALYs were estimated by applying utilities for the time spent by the cohort in each health-state and utility decrements associated with adverse events (AE). Total cost (€,2020) included drug-acquisition, hematologic stem-cell transplantation, disease management, AE management and end-of-life costs. Unit costs were derived from local databases. All parameters were validated by haematologist. Costs and outcomes were discounted (3%/year).
Results: Higher cost/patient (€ 177,618 vs € 151,434) and greater QALYs (5,70 vs 4,62) were obtained with GO+SOC vs SOC. The ICUR was € 24,203/QALY gained.
Conclusion: This simulation suggests that GO + SOC could be a cost-effective option for treatment of patients with de novo AML in first line.
Keywords: cost-effectiveness, gemtuzumab ozogamicin, acute myeloid leukaemia, Spain
Corrigendum for this paper has been published
Introduction
Acute myeloid leukaemia (AML) is a heterogeneous neoplasm characterized by the clonal expansion of myeloid blasts in the peripheral blood, bone marrow and/or other tissues.1 In Europe, the incidence of this disease is estimated at 3.7 per 100,000 inhabitants per year.2 The incidence increases progressively with age, with the highest rates in the oldest patients.2–4
AML is an aggressive and rapidly progressing disease with a 5-year survival rate for adults of less than 30%.5 In addition, AML is associated with an important clinical and economic burden to patients, their caregivers, and the healthcare system.6,7
This disease is associated with different non-specific clinical manifestations, such as fatigue, dyspnoea, anorexia, fever, weight loss, infections, and bleeding, which are present at diagnosis of AML and during all treatments.8,9 Therefore, a proper diagnosis is clinically important in determining the appropriate therapeutic strategy for patients with AML.
The therapeutic management of AML depends fundamentally on patients’ physical condition which determines whether they can receive intensive chemotherapy, and on the cytogenetic profile of the patient, which determines the prognosis and the risk of relapse. With the advent of new techniques for the molecular diagnostic and the European Leukemia Network 2017 guidelines,10 the determination of genetic alterations which recurrently appear in AML (as NPM1 or FLT3) is becoming inceasingly important for the risk classification of AML patients, and therefore, for the selection of the best therapy for each type of AML.11 Currently, the standard recommendation for patients with AML who are candidates to receive an intensive treatment consists of induction, consolidation therapy followed by allogeneic (or less common autologous) hematologic stem cell transplantation when appropriate and feasible.10 The induction chemotherapy, aimed at achieving remission, is composed of cytarabine given by continuous infusion for 7 days and an anthracycline (such as daunorubicin or idarubicin) given daily for 3 days. Induction chemotherapy is followed by consolidation chemotherapy to maintain remission or eradicate any residual disease, which usually consists of various courses of cytarabine in different schemes.4,12
However, the therapeutic arsenal for AML has evolved rapidly in recent years, with the introduction of several targeted therapies. These new drugs led to changes in the disease landscape, creating a wider range of treatment options for these patients.13,14 One such example is gemtuzumab ozogamicin (GO), a recombinant humanized anti-CD33 monoclonal antibody linked to the antitumor antibiotic calicheamicin, which permits the drug to be targeted selectively to CD33-positive AML blast cells, preserving normal cells, and thus limiting non-haematological toxicity.15 GO administered in combination with standard of care (SOC) chemotherapy in ALFA-0701, a randomised, open-label, phase III trial of 278 patients aged 50–70 with previously untreated AML, significantly improved median event-free survival (EFS) and relapse-free survival (RFS) compared to SOC chemotherapy alone.16 In April 2018, GO was approved by the European Medicines Agency (EMA), indicated for combination therapy with daunorubicin (DNR) and cytarabine (AraC) for the treatment of patients aged 15 years and above with previously untreated, de novo CD33-positive AML, except acute promyelocytic leukaemia (APL).17
The aim of the present analysis was to assess the cost-effectiveness of adding GO to SOC first-line therapy in Spain, comparing the SOC alone for the management of patients with previously untreated de novo CD33-positive AML.
Materials and Methods
Model Structure
A cost-effectiveness model was used to evaluate the efficacy of GO plus SOC vs SOC alone for the management of patients with previously untreated de novo AML in Spain. To perform the analysis in the Spanish setting, a cohort state-transition model that had been previously validated was used.18–20
The structure of the model used for the present analysis captures the progression of the disease, using 12 mutually exclusive health states: induction chemotherapy, complete remission (CR) or complete remission with incomplete platelet recovery (CRp) (consolidation chemotherapy), CR or CRp (off treatment), relapse (salvage therapy), relapse (noncurative therapy), refractory (salvage therapy), refractory (noncurative therapy), haematopoietic stem-cell transplant (HSCT) procedure, post-HSCT CR or CRp [without graft versus host disease (GVHD)], post-HSCT CR or CRp (with GVHD), functionally cured (off treatment) and dead (Figure 1).
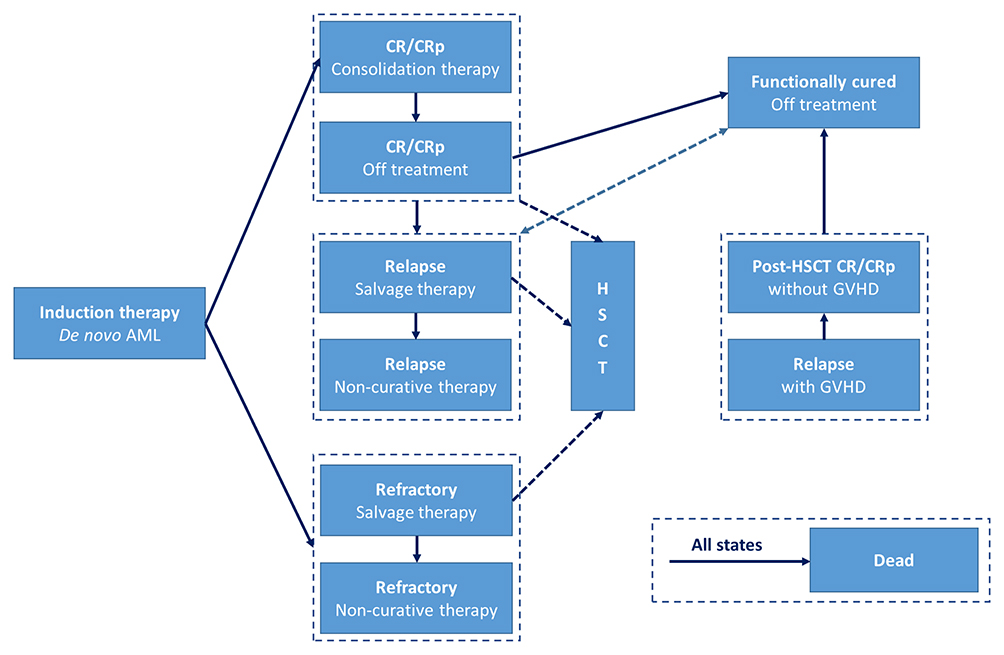 |
Figure 1 Model structure diagram. Abbreviations: AML, acute myeloid leukaemia; CR, complete remission; CRp, complete remission with incomplete platelet recovery; GVHD, graft versus host disease; HSCT, haematopoietic stem cell transplantation. |
The analysis was performed for the patient cohort using monthly cycles over a lifetime horizon (40 years). Upon entering the model, patients were initiated with first-line chemotherapy, receiving one or two induction courses, depending on their initial response to treatment. At the end of induction chemotherapy, patients were assessed and either attained CR or CRp or failed induction chemotherapy (refractory). Patients who achieved CR or CRp continued with up to two courses of consolidation chemotherapy; however, some patients received HSCT because it is considered beneficial for patients with certain risk profiles. Patients in CR or CRp who relapsed and patients who were refractory to induction chemotherapy moved to salvage or noncurative therapies (second-line treatments). From this group of patients, those who were deemed fit enough could receive salvage therapy with the aim of achieving a second-line CR or CRp and potentially curative HSCT. Finally, some relapsed patients who achieved second-line CR or CRp who did not receive HSCT but had prolonged survival were considered functionally cured.
This analysis was performed from the perspective of the Spanish National Health System (NHS) and an annual discount rate of 3.0% was applied to both costs and health outcomes, according to the available recommendations for the development of a cost-effectiveness analysis in Spain.21
A lifetime horizon, 40 years, was applied to estimate life years gained (LYG) and quality-adjusted life years (QALYs) gained and the total costs of the two therapies considered in the analysis.
The model structure, population, adverse event (AE) management, disease management and resource consumption were validated and agreed on by a panel of five haematologist experts with wide expertise and knowledge about AML. For this study, a structured questionnaire that included the parameters identified in the scientific published literature was developed and completed by the expert panel. Subsequently, a face-to-face consensus meeting was carried out with the panel of experts to validate and agree upon all the values used in the analysis to ensure that it was representative of the Spanish setting.
Population
The study population was selected based on those patients who had demonstrated benefit from adding GO to standard chemotherapy in the ALFA-0701 clinical trial.16,22 Based on the ALFA-0701 trial results, patients with unfavourable cytogenetic profiles (including monosomy 5 or del(5q), monosomy 7 or del(7q), t(6;11), t(9;22), 3q26 abnormalities but t(3;5), 11q23 abnormalities but t(9;11), and complex karyotypes with 3 abnormalities or more) did not show an apparent EFS benefit with GO added to SOC; therefore, previously untreated adult patients with de novo AML with favourable [t(8;21) and inv(16)/t(16;16)], intermediate (other anomalies as well as normal karyotypes), and unknown cytogenetic profiles who were eligible to receive intensive chemotherapy were included in the analysis.16,22
Data for the simulated cohort were modelled on the mean characteristics of patients participating in the ALFA-0701 trial.16 The baseline characteristics of the patients included in the analysis are described in Table 1.
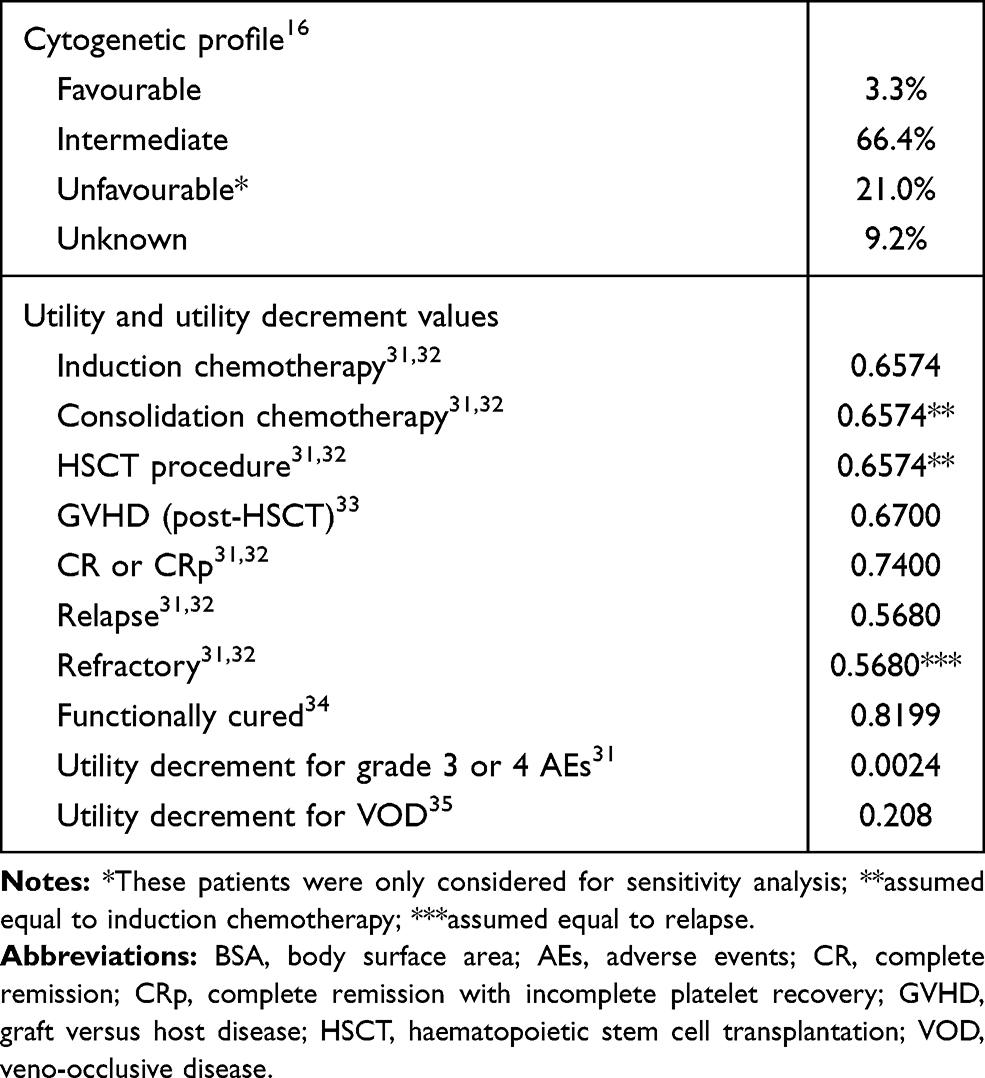 |
Table 1 Inputs Included in the Model |
Treatment Strategies
The therapeutic alternatives compared in the model included GO (Mylotarg®) combined with the most common SOC chemotherapy used in Spain (idarubicin and cytarabine) or SOC therapy alone.
For induction and consolidation treatments, the regimens, doses, and durations of treatment observed in the ALFA-0701 clinical trial16 and the consensus established by an expert panel according to clinical practice in Spain were adopted. For the salvage and noncurative treatments, the most frequent regimens and doses in clinical practice shown in the approved summaries of product characteristics23–29 were assumed. All treatment regimens and doses considered in the model were validated by the clinical expert panel.
Table 2 shows the regimens and doses of the therapies considered in each treatment phase as well as the proportion of patients achieving each treatment cycle.
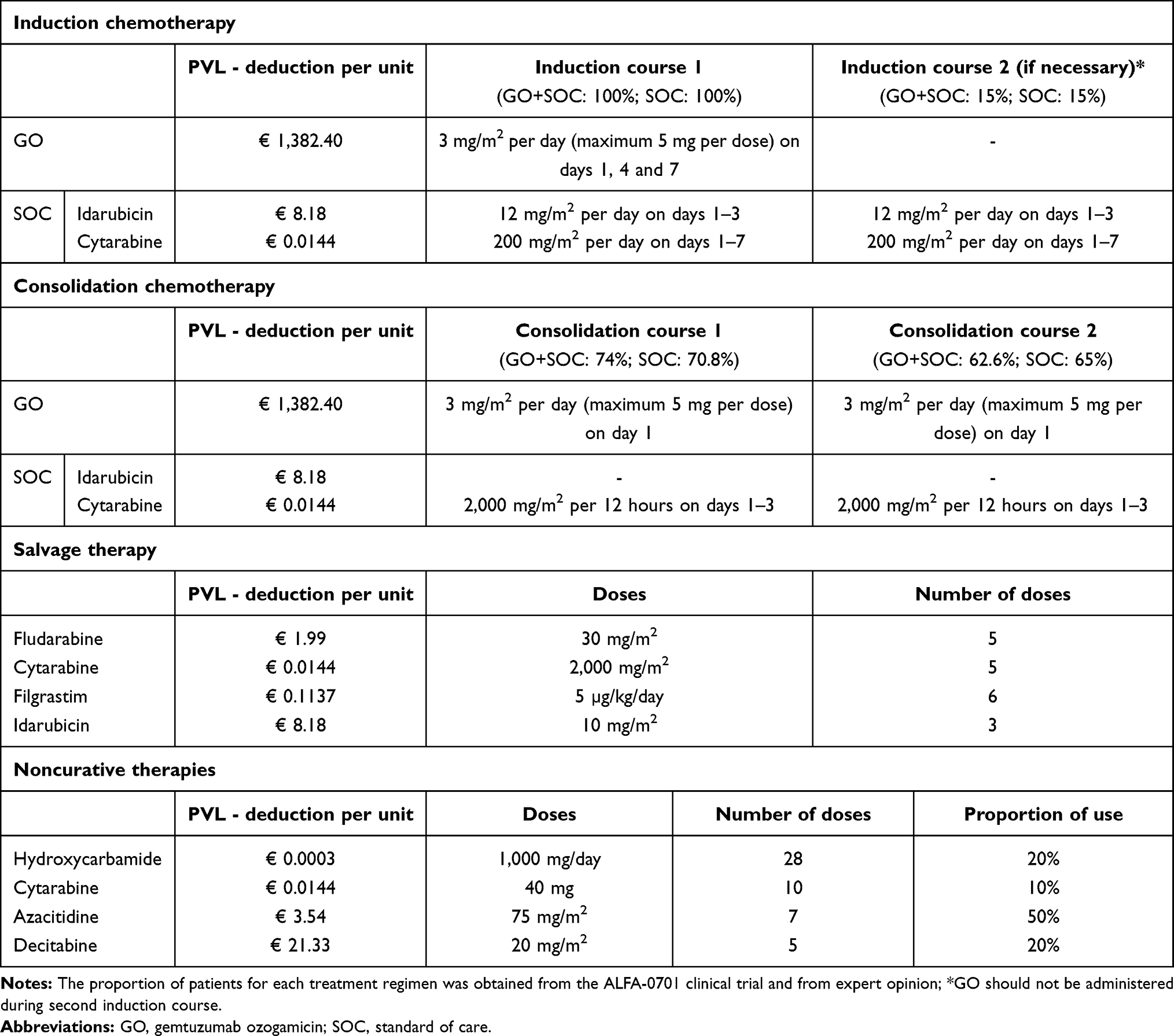 |
Table 2 Treatment Regimens Considered in the Analysis |
Clinical Data
To determine the distribution of patients across health states over time, parametric survival models were fitted to RFS and OS Kaplan–Meier curves from the ALFA-0701 trial and extrapolated over the model time horizon. An additive hazard ratio (HR) was applied to represent the excess mortality for cured patients with AML versus the general population.
ALFA-0701 (2007–002933-36)16 was ap hase 3, open-label multicenter study undertaken to investigate the addition of GO to standard front-line chemotherapy in patients with CD33 positive de novo AML. The primary endpoint of the study was EFS.
Patients aged 50–70 years with previously untreated de novo AML were randomly assigned to a control group with standard treatment (N=139) or to therapy with five doses of intravenous GO (3 mg/m2 on days 1, 4, and 7 during induction and day 1 of each of the two consolidation chemotherapy courses) (N=139).16
Patients achieving complete response with or without incomplete platelet recovery after induction chemotherapy was 104 (75%) in the control group and 113 (81%) in the GO group (odds ratio 1.46, 95% CI 0.20–2.59; p=0.25). At 2 years, EFS was estimated as 17.1% in the control group versus 40.8% in the GO group (HR 0.58, 0.43–0.78; p=0.0003), OS 41.9% versus 53.2%, respectively (0.69, 0.49–0.98; p=0.0368), and relapse-free survival (RFS) 22.7% versus 50.3%, respectively (0.52, 0.36–0.75; p=0.0003). Haematological toxicity, particularly persistent thrombocytopenia, was more common in the GO group than in the control group (22 [16%] vs 4 [3%]; p<0.0001), without an increase in the risk of death from toxicity.16
Additional publications of the trial results performed by a blinded independent review confirmed previous results.22 The final OS on April 30, 2013, favoured GO but was not statistically significant (HR 0.81; 95% CI: 0.60–1.09; P=0.16), and no differences in the early death rate were observed between arms. Moreover, the subgroup analyses showed that patients with favourable or intermediate cytogenetic risk (classified according to the International System for Human Cytogenetic Nomenclature criteria) at baseline had significantly longer EFS in the GO arm than in the control arm (HR: 0.46; 95% CI: 0.31–0.68; p<0.0001); however, this advantage in EFS with GO was not demonstrated for patients with poor cytogenetic risk (HR 1.11; 95% CI: 0.63–1.95; p=0.72).
Grade 3 and 4 AEs most commonly observed in the ALFA-0701 clinical trial (skin toxicity, mucosal toxicity, pain, nausea, vomiting and diarrhoea, pulmonary toxicity, cardiac rhythm disorder, other cardiac toxicity, central neurological toxicity, peripheral neurological toxicity, infections, haemorrhage and veno-occlusive disease (VOD)) were considered during the first model cycle15 (Table 3). Conservatively, no AEs related to subsequent-line therapies were considered.
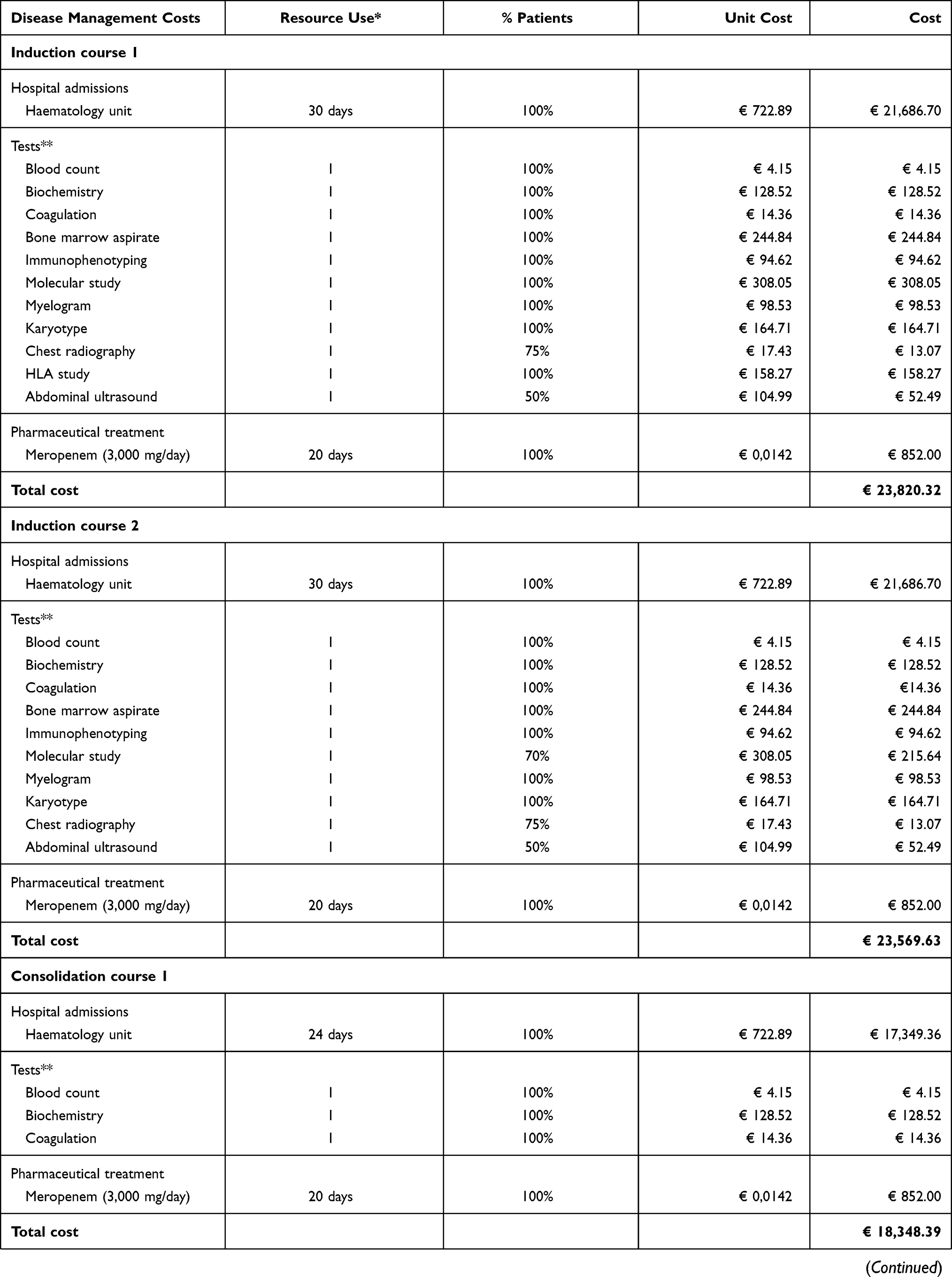 | 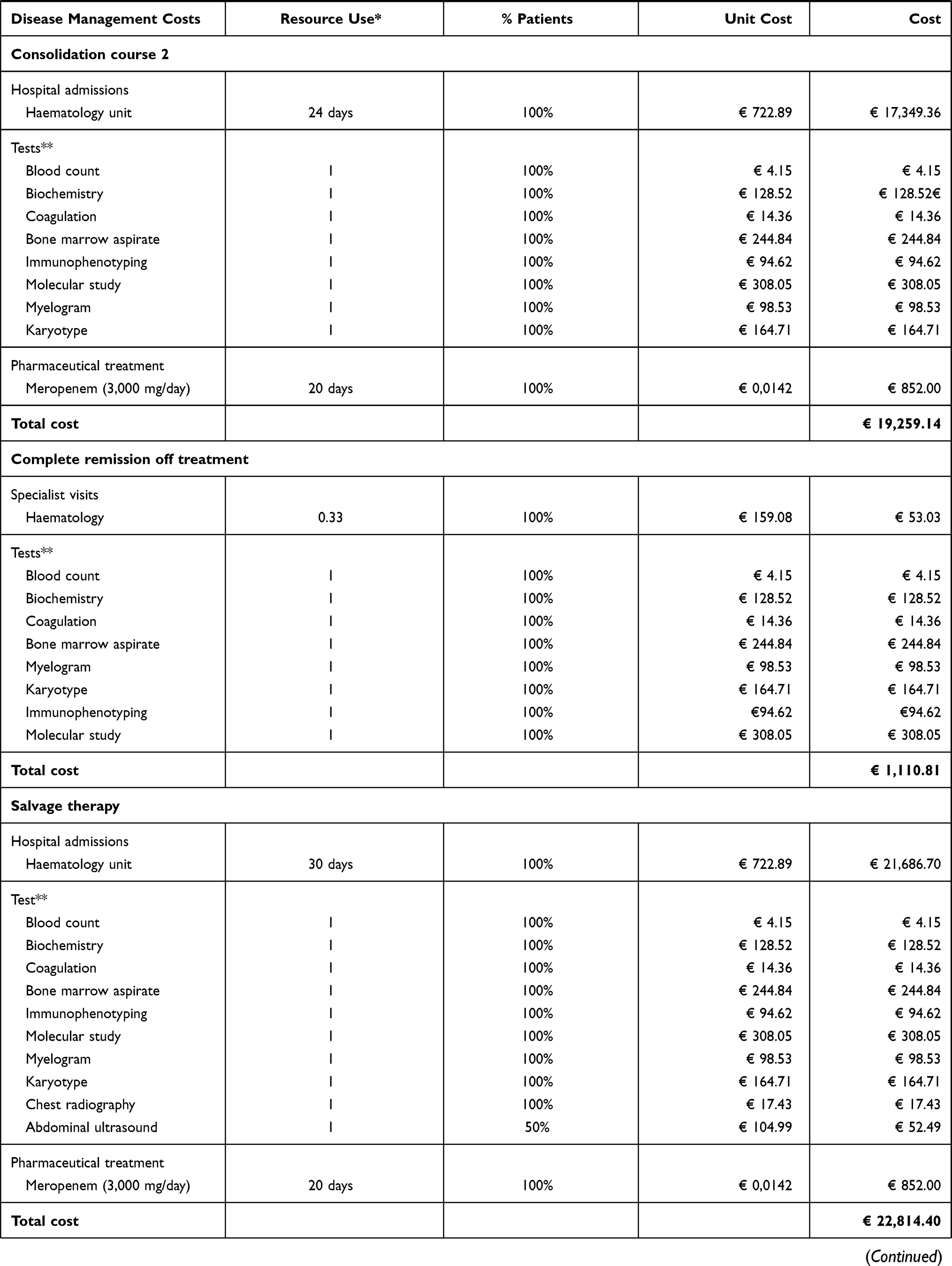 | 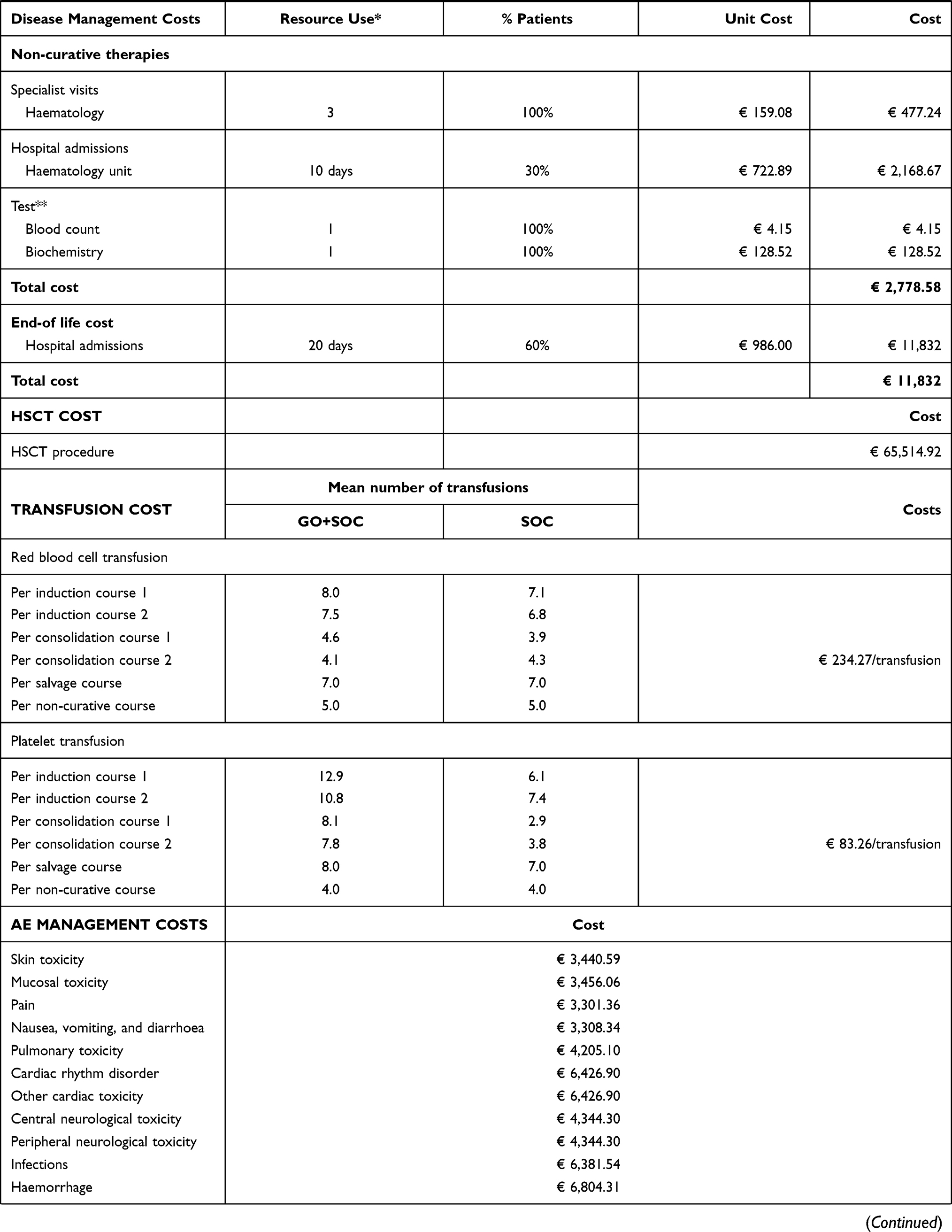 |  |
Table 3 Healthcare Direct Costs (€, 2020) |
In addition, acute and chronic GVHD was considered in the analysis since it is a clinically important complication that patients can develop after HSCT. The incidence of grade 3 or 4 acute GVHD for HSCT patients was estimated to be 15%, with a mean duration of 2.5 months, and the incidence of grade 3 or 4 chronic GVHD was estimated to be 20%, with a mean duration of 12 months based on expert panel opinion. Probability of HSCT was calculated from the ALFA-0701 clinical trial.16
Mortality
All-cause mortality data were applied to show the annual probability of death by age and sex, derived from the Spanish mortality tables.30 In addition, patients with AML carry a higher risk of dying from causes other than the general population; therefore, mortality related to AML and its associated complications were considered in the analysis.16
Utilities and Disutilities
To estimate the QALYs, different utility values were considered depending on the health states of the patients. The term “utility” refers to the quality perceived by patients based on their health status and receives a value between 1 (perfect health) and 0 (state of health equivalent to death).
The utility values were obtained from the scientific literature31–34 using the scores of the EuroQol 5-Dimensions (EQ-5D) questionnaire were applied to the different health states (Table 1).
Moreover, a decrease in utility (disutility) was applied for AEs. A mean one-off utility decrement of 0.0024 for all grade 3 or 4 AEs apart from VOD was applied in the model.32 For VOD, a decrease in utility of 0.20835 was applied for a mean duration of 26.8 days.36
Resource Use and Costs
In line with the perspective of the analysis, only costs related to direct healthcare resource consumption were considered. These included pharmaceutical costs, disease management costs per health state, HSCT costs, AE management costs and end-of-life costs.
The pharmaceutical costs reflected drug acquisition, which was estimated based on ex-factory prices published in the Spanish General Council of Official Pharmaceutical Colleges catalogue,37 applying the national mandatory deductions38 (Table 2).
Disease management costs were estimated based on the healthcare resource consumption for referral to specialist visits, hospital admissions, diagnostic and laboratory tests, and concomitant treatments, which were provided by a haematology expert panel with wide expertise and knowledge about AML (Table 3).
In relation to transfusion costs, red blood cell and platelet transfusions were considered in the analysis. Total costs were estimated by multiplying the mean number of transfusions reported in the ALFA-0701 study16 by the cost per transfusion (Table 3).
Regarding HSCT costs, only the cost of the transplantation procedure was considered, assuming that it covers complications and follow-up and the post-transplantation recovery period. The model applied a one-time cost for the transplantation procedure and recovery period whenever patients entered the HSCT health state (Table 3).
Grade 3 or 4 AE-related costs were calculated by multiplying the number of AEs reported in the ALFA-0701 study16 with the estimates of the cost per event. The cost of VOD was calculated from the healthcare resource consumption incurred for hospitalizations, which was provided by an expert panel (Table 3).
End-of-life costs were estimated from the consumption of healthcare resources provided by a clinical expert panel (Table 3).
All unitary costs were obtained from a local national database of healthcare costs.39 Costs were expressed in Euros for the year 2020 and adjusted for inflation using the Spanish healthcare consumer price index as necessary.40
Sensitivity Analysis
One-way sensitivity analysis (OWSA) and probabilistic sensitivity analysis (PSA) were performed to assess the robustness of the model and the uncertainty of the base case results for each of the treatment strategies analysed.
For the OWSA, the following parameters were varied: time horizon (20 years), discount rate (0% and 5%), mean BSA of 1.70 m2 which is representative of the Spanish population,41 proportion of patients for all cytogenetic profiles (3.32% favourable, 66.42% intermediate, 21.03% unfavourable and 9.23% unknown), costs such as health state medical resources and AEs were varied by ±20%, and health-state utility values were modified by ±20%.
In the PSA, 1,000 Monte Carlo simulations were performed. The value of each key model parameter was varied within a specific probability distribution assigned to each parameter. Bayesian posterior distributions were applied for survival function parameters, log-normal distributions for HR, and gamma distributions for costs and utility values.
Results
Base Case
Over a lifetime horizon, GO in combination with anthracycline and cytarabine was associated with 7.81 LYG and 5.70 QALYs gained per patient, which were higher than the results obtained in patients treated with SOC alone (6.37 LYG/patient and 4.62 QALYs/patient).
The estimated total cost for achieving these gains in health outcomes was € 177,618 and € 15,134 per patient with GO plus SOC and SOC alone, respectively.
The incremental cost–utility ratio (ICUR) for GO plus SOC versus the SOC alone was € 24,203 per additional QALY (Table 4).
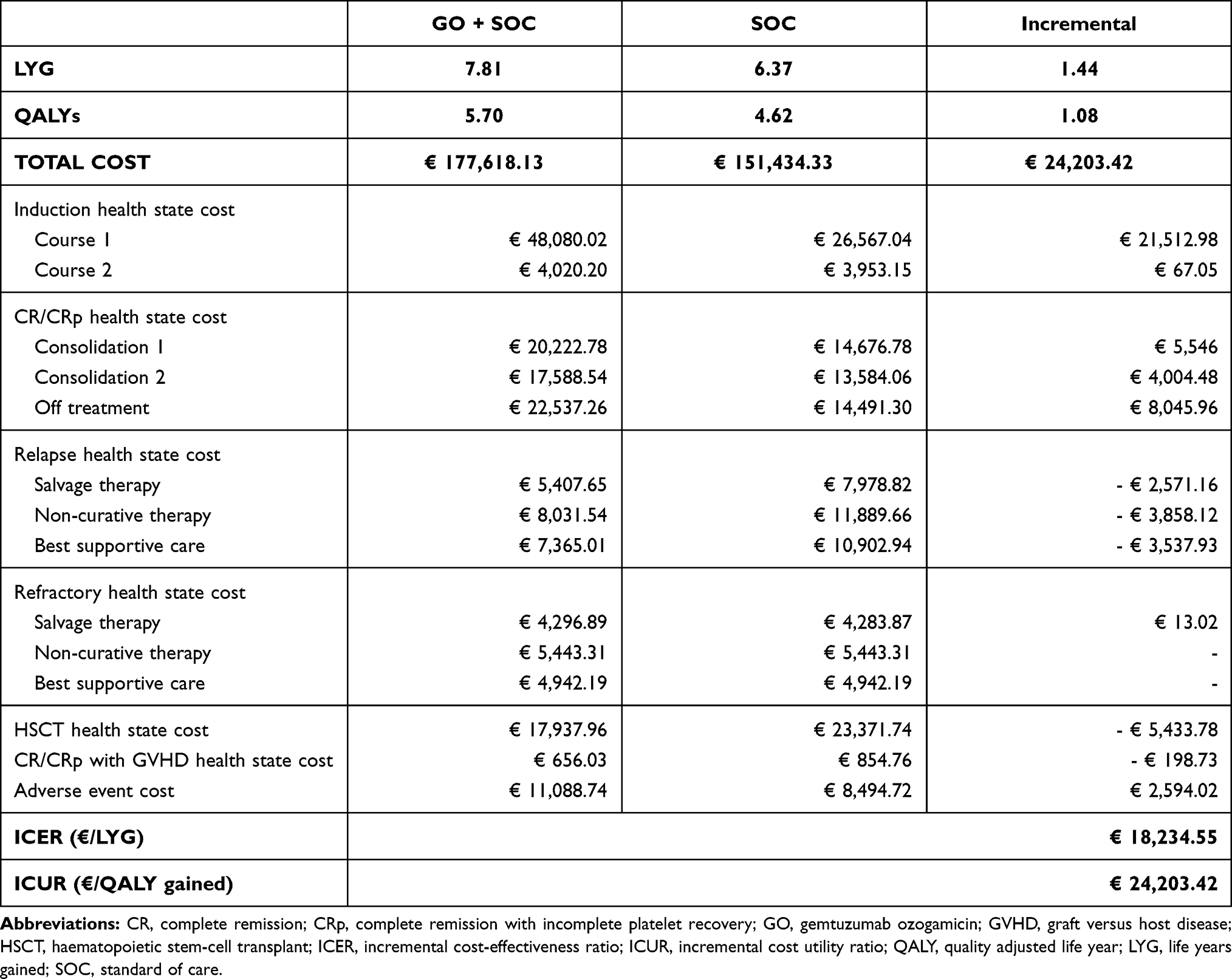 |
Table 4 Base Case Results of the Cost-Effectiveness Analysis |
Therefore, according to the most widely accepted willingness-to-pay threshold in Spain (€ 10,000–30,000/QALY),42 the treatment of AML patients with GO added to standard induction chemotherapy (anthracycline and cytarabine) can be considered a cost-effective strategy compared with SOC alone (Table 4).
Sensitivity Analysis
In the OWSA, the addition of GO to SOC (anthracycline and cytarabine) was a cost-effective in eight of nine scenarios tested. The ICUR values ranged between € 17,703 and € 34,418 for each additional QALY gained with the GO+SOC treatment versus SOC alone. The parameters having the most influence on the results were the inclusion of the unfavourable cytogenetic profile, followed by the discount rate (Figure 2).
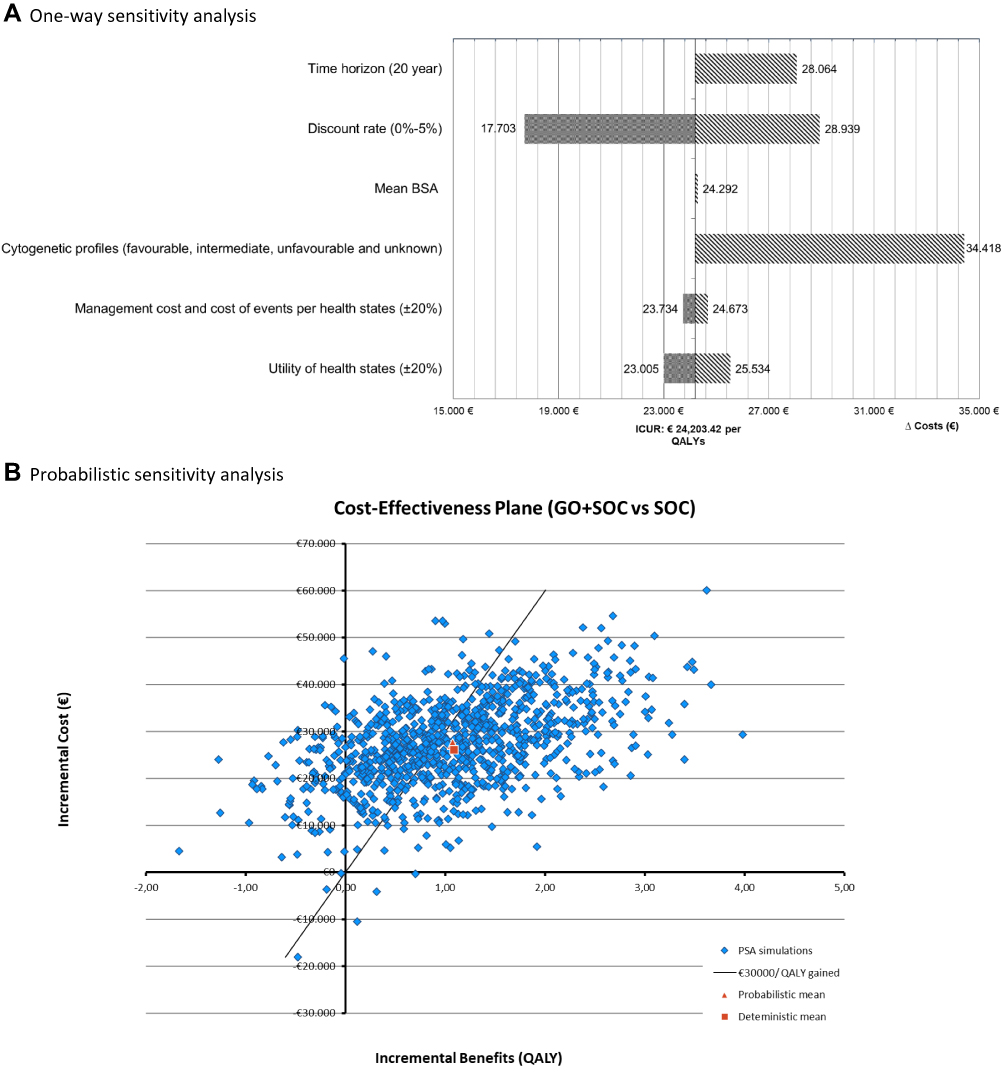 |
Figure 2 Results of one-way and probabilistic sensitivity analysis. (A) One-way sensitivity analysis. (B) Probabilistic sensitivity analysis. |
The results of the PSA showed that of 1,000 iterations carried out, 55.9% showed an ICUR below a willingness-to-pay threshold of €30,000/QALY. The GO plus SOC therapy can be considered a cost-effective alternative with a mean ICUR of € 25,556 (95% CI € 23,698 – € 27,710) compared to SOC alone (Figure 2).
The results of both the deterministic and probabilistic analyses are described in Figure 2.
Discussion
Economic evaluations aim to provide information to health decision-makers that could be useful for the adoption of new therapies and their inclusion in the reimbursement process of health systems.
In 2018, the EMA granted the authorization of GO to be used for the treatment of previously untreated, de novo CD33-positive AML, except APL, for patients aged 15 years and above, in combination with daunorubicin and cytarabine, and in July 2019, marketing authorization was issued.43
Usually, the inclusion of new treatment options frequently represents an increase in pharmaceutical costs, which can be compensated for or even lead to savings in the total costs by a lower use of resources for patient management. In the case of GO, previous studies have been performed with different higher dose concerns in terms of safety.44,45 To minimize toxicity, the ALFA-0701 study16 presented a new fractionated dose regimen in combination with 3+7, using 3 mg/m2 of GO on D1, D4, D7, allowing safer administration of higher cumulative doses (9 mg/m2). The ALFA-0701 study classified patients according to the current European Leukemia Net (ELN) 2010 at the moment of the study. Under cytogenetic risk classification, only 3% of the total patients included in the study were classified as favourable cytogenetic risk (t(8;21) and inv(16)/t(16;16)).16 Subgroup analysis showed that patients with favourable or intermediate cytogenetic risk had a significantly longer EFS in the GO arm versus the control arm (HR: 0.46, p>0.0001), which was not observed in patients with poor cytogenetic risk (HR: 1.11, p=0.72).22
Recently, Fournier et al. retrospectively analysed data from patients enrolled in the ALFA-0701 trial using the most recent ELN 2017 risk classification. In this work, the benefit of GO was confirmed in patients with favourable and intermediate risk, while it did not influence the outcome of patients within the adverse risk subgroup.11 Another study46 has examined post-transplant outcomes and the occurrence of hepatic VOD or sinusoidal obstruction syndrome (SOS) in patients who received HSCT as follow-up therapy in ALFA-0701, which was recommended for patients in first complete remission with matched donor, except those with AML with core-binding factor or normal karyotype and AML NPM1+/FLT3-ITDwt or CEBPA+. The results indicate that fractionated dose GO as part of induction and consolidation chemotherapy for AML does not induce excess VOD/SOS after transplantation or mortality and therefore does not preclude the use of HSCT as consolidation therapy. Furthermore, a meta-analysis of individual patient data from 5 randomized controlled trials showed the benefit of GO added to conventional induction therapy. In this article, the addition of GO significantly reduced the risk of relapse (OR 0.81 p=0.0001) and, at 6 years, the absolute survival benefit was especially significant in patients with favourable cytogenetic features (20.7% p=0.0006) but also with intermediate cytogenetic features (5.7% p=0.005).47
In the present study, the addition of GO to SOC for first-line treatment for CD33+ AML patients with favourable/intermediate or unknown cytogenetics increased the pharmaceutical cost (€ 31,179); however, due to its higher effectiveness, the final management costs were reduced (€ 5,715), mainly by transplantations avoided (32 GO+SOC vs 53 SOC).22 The results obtained with the present simulation suggest that the cost per additional QALYs gained with GO in combination with SOC compared to SOC alone (€ 24,203/QALYs) remains between € 10,000 - € 30,000 per QALY, a threshold frequently used as reference value in economic evaluations performed in Spain.42
To our knowledge, this is the first cost-effectiveness/utility analysis of GO plus SOC in newly diagnosed patients with CD-33 positive AML conducted from the perspective of the Spanish NHS. Therefore, in the Spanish context, it is not possible to compare the results with other studies. Nevertheless, the results of the study are in line with those from other published economic analyses in other settings. A cost-effectiveness study was published recently in the United Kingdom using the same model as in the present analysis.48 This study showed that GO in combination with SOC (daunorubicin + cytarabine) is a cost-effective first-line treatment option for adult patients with AML versus SOC alone, leading to an ICUR of £13,561/QALY gained.
A conservative assumption was made, in that the base case patients with favourable, intermediate, and unknown cytogenetic profiles were considered. This cytogenetic subgrouping was employed since, based on the ALFA-0701 study,16 the addition of GO was not associated with an additional survival benefit for patients with an unfavourable cytogenetic profile. Nevertheless, a sensitivity analysis was performed to test the results in the total population with AML, which was slightly above the willingness-to-pay threshold used as a reference.43
The present model has several limitations, some of which are inherent to this type of pharmacoeconomic analysis. Primarily, the theoretical nature of any modelling might not be an accurate representation of daily clinical practice. In this study, the source used to include efficacy in the model was the ALFA-0701 clinical trial,16 a study that only considered the intensive treatment candidate population (excluding patients with comorbidities or other conditions that doesn´t allow to receive intensive chemotherapy) and de novo AML (excluding patient had secondary or post-treatment AML). RFS and OS data are limited at a median follow-up of 60 months, and parametric survival functions were required to extrapolate the Kaplan-Meier trial curves. Additionally, in the analysis, equivalence was assumed between SOC chemotherapy used in the ALFA-0701 trial16 (daunorubicin + cytarabine) and the most common combination used in Spain (idarubicin + cytarabine). Several studies identified in the literature, using either daunorubicin at 60 or 90 mg/m2 or idarubicin at 12 mg/m2 have shown similar rates of CR and survival.49,50 These data were validated and agreed upon by the panel of experts.
Another possible limitation is related to the use of data extracted from the literature of studies conducted in other countries, where studies conducted, specifically in Spain were not identified. The utility and disutility values used in the model were derived from international literature,32–35 which were validated by the expert panel to ensure that these values are representative of the Spanish AML population.
Finally, the parameters used in the analysis have been extracted from different sources; however, all variables are based on official sources or on publications with a high level of clinical evidence and have been validated by an expert panel. Regarding the consumption of healthcare resources included for the consolidation courses, a conservative scenario was assumed considering that the courses are carried out in the hospital. In some centres, these treatments are carried out in an outpatient setting, which would notably reduce the total cost associated with this health state.
Despite the limitations described, the results of the SA confirmed that the uncertainty associated with the parameters used in the model does not represent a significant deviation from the results obtained in the base case.
The results of the present simulation suggest that GO added to standard AML induction chemotherapy (anthracycline and cytarabine) could be considered as a cost-effective option for the first-line treatment of patients with CD33+ AML with favourable, intermediate and unknown cytogenetic profiles in Spain.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request and with permission of Pfizer.
Ethics Statement
Not applicable. Ethics approval is considered unnecessary according to national regulations since it is not a study but an economic evaluation. As our work is not related to patients since it is not a study, informed consent does not apply.
Funding
This study was funded by Pfizer Spain.
Disclosure
Pau Montesinos, Patricia Font, Jorge Sierra, Adolfo de la Fuente and José María Guinea have received honoraria from Pfizer for advocacy tasks related to this project. Patricia Font is also the advisory board for BMS and Menarini. Jorge Sierra reports personal fees from Novartis, Astellas, Jazz Pharmaceuticals, and AbbVie, during the conduct of the study. María Mareque and Itziar Oyagüez are currently employed at PORIB, a consultant company specialized in economic evaluation of health interventions, which received financial support from Pfizer for the development of this study. Javier Soto, Tamara Iglesias and Julia Llinares are employees of Pfizer Spain. James Brockbank is employed of RTI Health Solutions. The authors report no other conflicts of interest in this work.
References
1. Tallman MS, Wang ES, Altman JK, et al. Acute myeloid leukemia, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(6):721–749. doi:10.6004/jnccn.2019.0028
2. Visser O, Trama A, Maynadié M, et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur J Cancer. 2012;48(17):3257–3266. doi:10.1016/j.ejca.2012.05.024
3. Deschler B, Lübbert M. Acute myeloid leukemia: epidemiology and etiology. Cancer. 2006;107(9):2099–2107. doi:10.1002/cncr.22233
4. De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 2016;6(7):e441. doi:10.1038/bcj.2016.50
5. National Cancer Institute. Cancer stat facts: acute myeloid leukemia (AML); 2020. Available from: https://seer.cancer.gov/statfacts/html/amyl.html.
6. Horvath Walsh LE, Rider A, Piercy J, et al. Real-world impact of physician and patient discordance on health-related quality of life in US patients with acute myeloid leukemia. Oncol Ther. 2019;7(1):67–81. doi:10.1007/s40487-019-0094-x
7. Pandya BJ, Chen CC, Medeiros BC, et al. Economic and clinical burden of acute myeloid leukemia episodes of care in the United States: a retrospective analysis of a commercial payer database. J Manag Care Spec Pharm. 2020;26(7):849–859. doi:10.18553/jmcp.2020.19220
8. Ferrara F, Schiffer CA. Acute myeloid leukaemia in adults. Lancet. 2013;381(9865):484–495. doi:10.1016/S0140-6736(12)61727-9
9. Loh KP, Pardee TS, Klepin HD. Acute myeloid leukemia in older adults. Geriatric Oncology. 2020:501–520.
10. Döhner H, Estey EH, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447.
11. Fournier E, Duployez N, Ducourneau B, et al. Mutational profile and benefit of gemtuzumab ozogamicin in acute myeloid leukemia. Blood. 2020;135(8):542–546. doi:10.1182/blood.2019003471
12. Milligan DW, Grimwade D, Cullis JO, et al. Guidelines on the management of acute myeloid leukaemia in adults. Br J Haematol. 2006;135:450–474. doi:10.1111/j.1365-2141.2006.06314.x
13. Talati C, Sweet K. Recently approved therapies in acute myeloid leukemia: a complex treatment landscape. Leuk Res. 2018;73:58–66. doi:10.1016/j.leukres.2018.09.001
14. Dombret H, Gardin C. An update of current treatments for adult acute myeloid leukemia. Blood. 2016;127(1):53–61. doi:10.1182/blood-2015-08-604520
15. Thol F, Schlenk RF. Gemtuzumab ozogamicin in acute myeloid leukemia revisited. Expert Opin Biol Ther. 2014;14(8):1185–1195. doi:10.1517/14712598.2014.922534
16. Castaigne S, Pautas C, Terré C, et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet. 2012;379(9825):1508–1516. doi:10.1016/S0140-6736(12)60485-1
17. European Medicines Agency. Mylotarg 5 mg powder for solution for infusion summary of product characteristics. London: European Medicines Agency; 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/mylotarg-epar-product-information_es.pdf.
18. Kurosawa S, Yamaguchi T, Miyawaki S, et al. A Markov decision analysis of allogeneic hematopoietic cell transplantation versus chemotherapy in patients with acute myeloid leukemia in first remission. Blood. 2011;117(7):2113–2120. doi:10.1182/blood-2010-05-285502
19. Leunis A, Redekop WK, van Montfort KA, et al. The development and validation of a decision-analytic model representing the full disease course of acute myeloid leukemia. Pharmacoeconomics. 2013;31(7):605–621. doi:10.1007/s40273-013-0058-1
20. Wang HI, Aas E, Howell D, et al. Long-term medical costs and life expectancy of acute myeloid leukemia: a probabilistic decision model. Value Health. 2014;17(2):205–214. doi:10.1016/j.jval.2013.12.007
21. López Bastida J, Oliva J, Antoñanzas F, et al. Spanish recommendations on economic evaluation of health technologies. Eur J Health Econ. 2010;11:513–520. doi:10.1007/s10198-010-0244-4
22. Lambert J, Pautas C, Terré C, et al. Gemtuzumab ozogamicin for de novo acute myeloid leukemia: final efficacy and safety updates from the open-label, phase III ALFA-0701 trial. Haematologica. 2019;104(1):113–119. doi:10.3324/haematol.2018.188888
23. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics forFludarabina 50 mg polvo para solución inyectable y para perfusión EFG [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/60616/60616_ft.pdf. Accesssed April 12, 2021
24. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics forCitarabina Pfizer 500 mg polvo y disolvente para solución inyectable y para perfusión [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/49154/49154_ft.pdf.
25. European Medicines Agency. Summary of product characteristics for Filgrastim HEXAL 30 MU/0,5 mL solución inyectable o para perfusión en jeringa precargada. Londres: Agencia Europea de Medicamentos; 2020. Available from: https://www.ema.europa.eu/en/documents/product-information/filgrastim-hexal-epar-product-information_es.pdf.
26. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics forIdarubicina Sandoz 1 mg/mL concentrado para solución para perfusión [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/75242/FichaTecnica_75242.html.pdf.
27. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics for Hydrea 500 mg cápsulas duras [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/61633/FichaTecnica_61633.html.pdf.
28. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics forVidaza 25 mg/mL polvo para suspensión inyectable [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/08488001/FT_08488001.pdf.
29. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics forDacogen 50 mg polvo para concentrado para solución para perfusión [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/112792001/FT_112792001.pdf.
30. National Institute of Statistics (Instituto Nacional de Estadística; INE). 2018 mortality tables of Spanish population. National results. INEbase. Madrid: Instituto Nacional de Estadística. Available from: http://www.ine.es.
31. National Institute for Health and Care Excellence (NICE). Technology appraisal No. 399. Azacitidine for treating acute myeloid leukaemia with more than 30% bone marrow blasts. Company evidence submission. Data on file (provided by Pfizer). November 25, 2015.
32. McKenzie L, van der Pol M. Mapping the EORTC QLQ C-30 onto the EQ-5D instrument: the potential to estimate QALYs without generic preference data. Value Health. 2009;12(1):167–171. doi:10.1111/j.1524-4733.2008.00405.x
33. Kurosawa S, Yamaguchi H, Yamaguchi T, et al. Decision analysis of postremission therapy in cytogenetically intermediate-risk acute myeloid leukemia: the impact of FLT3 internal tandem duplication, nucleophosmin, and CCAAT/enhancer binding protein alpha. Biol Blood Marrow Transplant. 2016;22(6):1125–1132. doi:10.1016/j.bbmt.2016.03.015
34. Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509–518. doi:10.1111/j.1524-4733.2010.00700.x
35. Scottish Medicines Consortium. Defibrotide, 80mg/mL, concentrate for solution for infusion (Defitelio®). SMC No. (967/14). May 9, 2014. Available from: https://www.scottishmedicines.org.uk/media/1543/defibrotide__defitelio__final_may_2014_for_website.pdf. Accessed April 16, 2021
36. Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard of care in relapsed or refractory acute lymphoblastic leukemia: final report and long-term survival follow-up from the randomized, phase 3 INO-VATE study. Cancer. 2019;125(14):2474–2487. doi:10.1002/cncr.32116
37. Consejo General de Colegios Oficiales de Farmacéuticos. Base de datos del Conocimiento Sanitario - Bot Plus 2.0 [Health Knowledge database – bot Plus 2.0] [Internet]. Madrid: Consejo General de Colegios Oficiales de Farmacéuticos; 2020. Available from: https://botplusweb.portalfarma.com/.
38. Ministry of Health, Social Services and Equality. Informative list of medicines affected by the deductions established in Royal Decree Law 8/2010 of 20 May, which adopts extraordinary measures to reduce the public deficit. [Internet]. Madrid: ; 2010. Available from: http://www.msssi.gob.es/profesionales/farmacia/pdf/DeduccionesJulio2019.pdf.
39. Oblikue Consulting. Base de datos de costes sanitarios eSalud [eSalud health cost database] [Internet]. Barcelona: Oblikue Consulting; 2020. Available from: http://www.oblikue.com/bddcostes/.
40. National Institute of Statistics (Instituto Nacional de Estadísitica; INE). Available from: http://www.ine.es.
41. Ortega Eslava A, Marín Gil R, Fraga Fuentes MD, et al. Guidelines on economic evaluation and budgetary impact in drug assessment reports. Practical guide associated with the MADRE v 4.0 programme. Madrid: SEFH (ed.); 2016. Available from: http://gruposdetrabajo.sefh.es/genesis/index.php?option=com_content&view=article&id=11&Itemid=13.
42. Vallejo-Torres L, García-Lorenzo B, Rivero-Arias O, Pinto-Prades JL. The societal monetary value of a QALY associated with EQ-5D-3L health gains. Eur J Health Econ. 2020;21(3):363–379. doi:10.1007/s10198-019-01140-4
43. Spanish Agency of Medicine and Sanitary Products. Summary of product characteristics for Mylotarg 5 mg polvo para concentrado para solución para perfusión [Internet]. Madrid: Spanish Agency of Medicine and Sanitary Products.; 2020. Available from: https://cima.aemps.es/cima/pdfs/es/ft/1181277001/FT_1181277001.pdf.
44. Larson RA, Sievers EL, Stadtmauer EA, et al. Final report of the efficacy and safety of gemtuzumab ozogamicin (Mylotarg) in patients with CD33-positive acute myeloid leukemia in first recurrence. Cancer. 2005;104(7):1442–1452. doi:10.1002/cncr.21326
45. Petersdorf SH, Kopecky KJ, Slovak M, et al. A phase 3 study of gemtuzumab ozogamicin during induction and postconsolidation therapy in younger patients with acute myeloid leukemia. Blood. 2013;121(24):4854–4860. doi:10.1182/blood-2013-01-466706
46. Pautas C, Raffoux E, Lambert J, et al. Outcomes following hematopoietic stem cell transplantation in patients treated with standard chemotherapy with or without gemtuzumab ozogamicin for acute myeloid leukemia. Bone Marrow Transplant. 2021. doi:10.1038/s41409-020-01207-4
47. Hills RK, Castaigne S, Appelbaum FR, et al. Addition of gemtuzumab ozogamicin to induction chemotherapy in adult patients with acute myeloid leukaemia: a meta-analysis of individual patient data from randomised controlled trials. Lancet Oncol. 2014;15(9):986–996. doi:10.1016/S1470-2045(14)70281-5
48. Mokgokong R, Mamolo C, Cappelleri JC, et al. Cost-effectiveness of gemtuzumab ozogamicin in combination with standard of care chemotherapy (daunorubicin and cytarabine) for first-line treatment of acute myeloid leukaemia.
49. Gong Q, Zhou L, Xu S, et al. High doses of daunorubicin during induction therapy of newly diagnosed acute myeloid leukemia: a systematic review and meta-analysis of prospective clinical trials. PLoS One. 2015;10(5):e0125612. doi:10.1371/journal.pone.0125612
50. Li X, Xu S, Tan Y, Chen J. The effects of idarubicin versus other anthracyclines for induction therapy of patients with newly diagnosed leukaemia. Cochrane Database Syst Rev. 2015;6:CD010432.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.