Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost-Effectiveness Analysis of Different Prenatal Screening Strategies for the Prevention of Severe Thalassemia in Thailand
Authors Malasai K, Jittikoon J, Talungchit P ![]() , Youngkong S, Udomsinprasert W
, Youngkong S, Udomsinprasert W ![]() , Chaikledkaew U
, Chaikledkaew U
Received 3 June 2025
Accepted for publication 24 October 2025
Published 15 November 2025 Volume 2025:17 Pages 835—848
DOI https://doi.org/10.2147/CEOR.S544493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Kwandao Malasai,1,2 Jiraphun Jittikoon,3 Pattarawalai Talungchit,4,5 Sitaporn Youngkong,5,6 Wanvisa Udomsinprasert,3 Usa Chaikledkaew5,6
1Social, Economic and Administrative Pharmacy Graduate Program, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 2Social Pharmacy Research Unit, Faculty of Pharmacy, Mahasarakham University, Maha Sarakham, Thailand; 3Department of Biochemistry, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand; 4Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 5Mahidol University Health Technology Assessment Graduate Program, Mahidol University, Bangkok, Thailand; 6Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, Thailand
Correspondence: Usa Chaikledkaew, Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, 447 Sri-Ayudhaya Road, Rachathewi, Phayathai, Bangkok, 10400, Thailand, Email [email protected]
Purpose: Three prenatal screening protocols are currently used in Thailand to prevent severe thalassemia in newborns; however, economic evaluation data to guide the selection of the most cost-effective strategy remain limited. This study aimed to conduct the cost-effectiveness of these screening strategies to support policy and clinical decision-making.
Patients and Methods: A decision-tree model was employed to evaluate the costs and outcomes associated with three prenatal screening algorithms: 1) a protocol starting with mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and the dichlorophenol indophenol precipitation (DCIP) test for pregnancies; 2) a protocol starting with MCV/MCH and hemoglobin (Hb) typing for pregnancies; and 3) a protocol starting with MCV/MCH and DCIP testing for couples based on a societal perspective. Results were presented as incremental cost-effectiveness ratios (ICERs) to compare the three prenatal screening strategies. Both one-way and probabilistic sensitivity analyses were performed to account for uncertainties in the parameters used.
Results: From a societal perspective, Strategies 2 and 3 were found to be cost-effective compared to Strategy 1. Screening 10,000 couples under Strategies 2 and 3 could prevent 60 and 49 additional cases of severe thalassemia, respectively, compared to Strategy 1. The ICERs for Strategies 2 and 3 were approximately 141,863 Baht (4,023 United States Dollar, USD) and 97,996 Baht (2,779 USD) per severe thalassemia case prevented, respectively. The most sensitive parameter for comparing Strategy 2 with Strategy 1 was the specificity of prenatal diagnosis for α-thalassemia.
Conclusion: Strategy 3 is the most cost-effective approach in Thailand. However, Strategy 2 may be implemented in hospitals with the capacity to perform Hb typing. These results offer significant value to policymakers by presenting strong evidence that could inform adjustments to the reimbursement framework in Thailand’s Universal Health Coverage benefit package, ultimately enhancing thalassemia management and prenatal care.
Keywords: cost-effectiveness, prenatal screening, severe thalassemia, Thailand
Introduction
Thalassemia is a common genetic disorder resulting from mutations in the genes responsible for producing the alpha or beta chains of hemoglobin (Hb), and affects approximately 18.28 per 100,000 people worldwide.1,2 The prevalence of α-thalassemia is 22.6% in Southeast Asia and 20.1% in Thailand.3 An estimated 1.5% of the worldwide population carries the β-thalassemia trait, with a higher prevalence in Southeast Asia such as 12.8% in Malaysia and 3–9% in Thailand.4 Based on gene frequencies, approximately 1.2% of newborns in Thailand are at risk for severe thalassemia, equating to an estimated 4,253 affected infants each year.5
Hb Bart’s hydrops fetalis or α-thalassemia major represents the most severe form of the disease, typically presenting with profound fetal anemia during intrauterine development, resulting in significant hypoxia and heart failure, which can lead to life-threatening complications.6,7 This condition is associated with a maternal mortality rate of nearly 50%.6 Other severe forms of thalassemia include homozygous β-thalassemia (β-thalassemia major) and β-thalassemia/Hb E, both of which are primarily characterized by severe anemia and required lifelong blood transfusions.8 These conditions are also associated with complications such as myocardial iron overload, splenomegaly, and cardiac complications.8 The survival rate for individuals with β-thalassemia major is approximately 0.75 in the 50–55 age group.9 In addition to the clinical burden, severe thalassemia imposes significant economic challenges. The estimated lifetime healthcare costs for transfusion-dependent β-thalassemia are 7.3 million United States Dollar (USD) for Thai and 7.1 million USD for US patients.5,10 Annual indirect costs are estimated at 230 USD, 295 USD, and 574 USD for Thai, Chinese, and Iranian patients with β-thalassemia major and β-thalassemia/Hb E, respectively.11–13 However, cost data regarding the treatment of Hb Bart’s hydrops fetalis remains limited. The total costs of screening were 34.7 to 536 USD per Indian couple and 73.5 to 192.2 USD per Thai couple.14,15
In 1989, a World Health Organization (WHO) working group convened and established guidelines for the control of Hb disorders, including carrier screening during pregnancy.16 Subsequently, in 1992, the Ministry of Public Health (MOPH) of Thailand implemented a thalassemia prevention and control program aimed at reducing the number of newborns affected by severe thalassemia.5 In 2009 and 2016, the Department of Medical Sciences under the MOPH issued updated guidelines for thalassemia prevention, each version outlining distinct protocols. The 2009 protocol recommended screening all pregnant women using the single-tube osmotic fragility (OF) test or red blood cell indices such as mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH), along with the dichlorophenol indophenol precipitation (DCIP) test. If any of these results were positive, the husband was invited to undergo the same tests. Couples who both tested positive for any screening test (OF, MCV, MCH, or DCIP) were then referred for Hb typing and/or deoxyribonucleic acid (DNA) analysis. High-risk couples defined as individuals with an increased risk of bearing a child affected by severe thalassemia were recommended to undergo prenatal diagnostic procedures to confirm the fetal condition.17 The 2016 guideline revised the protocol by introducing screening for all couples using the OF and DCIP tests or MCV/MCH and DCIP tests. If results were positive, further testing proceeded as outlined in the previous protocol.18 Additionally, some university hospitals, including Siriraj Hospital, adopted a different protocol ie, screening all pregnant women with MCV/MCH and Hb typing, omitting the OF and DCIP tests to reduce waiting times. If the pregnant woman’s results were positive, her partner was then tested using the same protocol. If both partners tested positive, further testing proceeded as described above. Currently, three screening strategies are employed in different contexts across Thailand, depending on factors such as regional prevalence of thalassemia carriers and the need to reduce waiting times.
Although our cost-benefit analysis (CBA) of prenatal screening strategies for thalassemia prevention has been previously conducted in Thailand,14 a cost-effectiveness analysis (CEA) remains essential to inform clinical and policy decision-making. Unlike CBA, which quantifies both costs and benefits in monetary terms, CEA compares alternative screening strategies based on their costs and clinical effectiveness. In this study, the outcome is expressed as the cost per severe thalassemia case averted, a measure that directly reflects the clinical objective of the screening program. Our previous CBA compared the costs and benefits of standard screening program with and without genetic testing, but did not evaluate all the screening strategies currently used in Thailand.14 At present, various screening protocols are implemented across different healthcare settings, resulting in variation in diagnostic methods, resource utilization, and operational complexity. Therefore, CEA enables a systematic comparison of these screening strategies and helps identify the most cost-effectiveness approach. The use of CEA provides clearer, more actionable evidence to support policy decisions and guide resource allocation.
Despite the fact that all screening tests are reimbursed through the Universal Health Coverage (UHC) benefit package, no evaluation of cost-effectiveness has been undertaken to compare the three prenatal screening modalities for thalassemia prevention either during pregnancy or for couples in Thailand. Such evidence could provide valuable evidence to support policymakers and healthcare providers in determining whether the most cost-effective prenatal thalassemia screening should be officially incorporated into national guidelines. Therefore, the aim of this study was to evaluate the cost-effectiveness of different prenatal screening strategies for the prevention of severe thalassemia in Thai pregnant women and couples.
Materials and Methods
Target Population
A cost-effectiveness analysis was conducted using a decision-analytical model to evaluate the cost and effectiveness of various prenatal screening strategies for the prevention of severe thalassemia from a societal perspective over a lifetime horizon. The model simulated cohorts of pregnant women, their risk-matched partners, and couples undergoing thalassemia carrier screening across all age groups and of Thai ethnicity, reflecting the population at risk given the national carrier prevalence of thalassemia. Three screening modalities were employed in accordance with the guidelines issued by the Department of Medical Sciences, MOPH,17,18 and the protocol of Siriraj Hospital.
Model Structure
A decision-tree model was developed to perform a cost-effectiveness analysis of three screening strategies (Figure 1). Three screening strategies were as follows: 1) screening strategy initiated with MCV/MCH and DCIP during pregnancy, 2) screening strategy initiated with MCV/MCH and Hb typing during pregnancy, and 3) screening strategy initiated with MCV/MCH and DCIP for the couple (Table 1). These three screening strategies were compared against each other. The model was developed and executed using Microsoft Office Excel 2019 (Microsoft Corp., Redmond, WA).
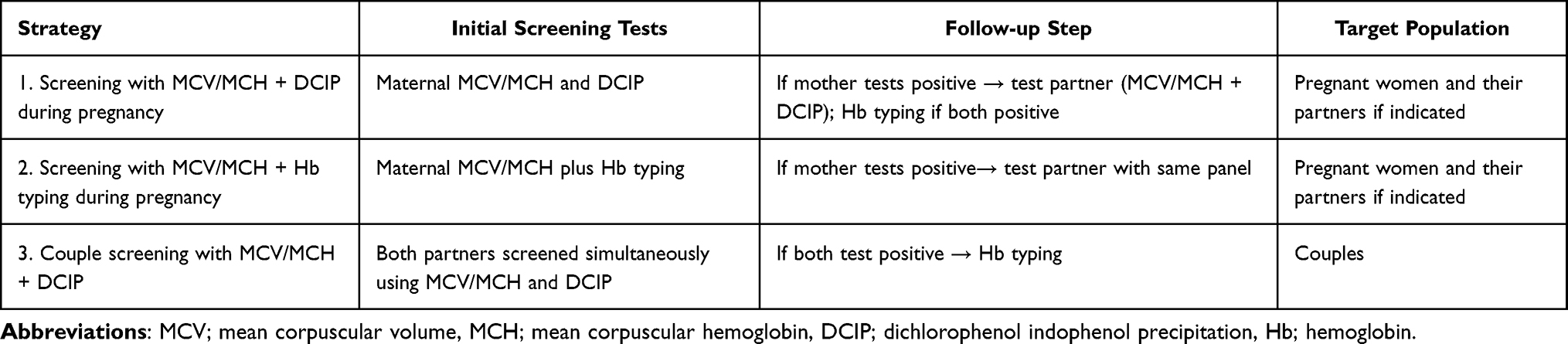 |
Table 1 Summary of Thalassemia Screening Strategies |
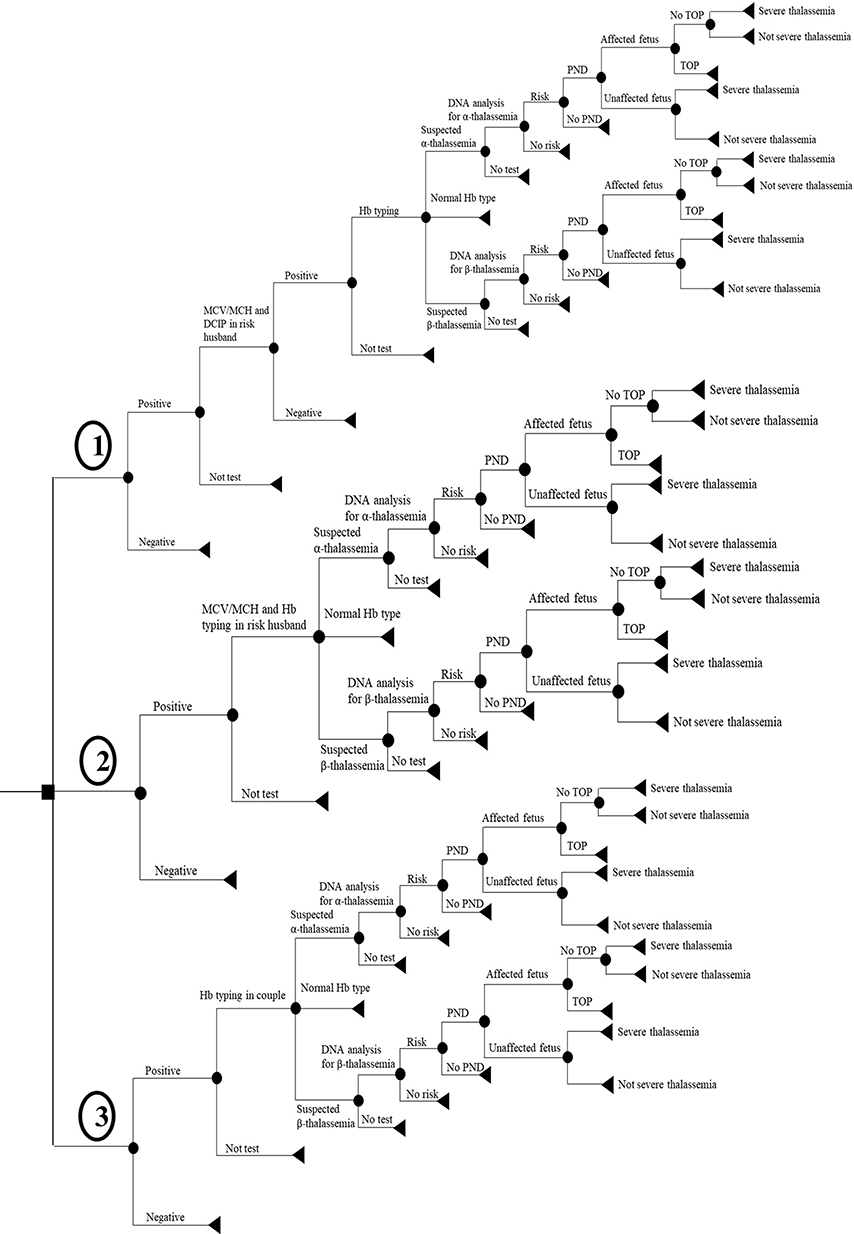 |
Figure 1 Structure of decision tree. 1) strategy of starting by MCV/MCH and DCIP for pregnancies, 2) strategy of starting by MCV/MCH and Hb typing for pregnancies, and 3) strategy of starting by MCV/MCH and DCIP for couple. Abbreviations: MCV; mean corpuscular volume, MCH; mean corpuscular hemoglobin, DCIP; dichlorophenol indophenol precipitation, Hb; hemoglobin, DNA; deoxyribonucleic acid, PND; prenatal diagnosis, TOP; termination of pregnancy. |
In the decision tree model, the starting point is located on the left side, representing the initial cohort of pregnant women or couples. For Strategy 1, all pregnant women undergo screening using MCV/MCH and DCIP. Results are classified as either positive or negative. If a woman tests positive, her at-risk husband is subsequently offered the same screening to determine whether both are thalassemia carriers. The partner may choose to accept or decline the test. If both partners test positive, they are offered Hb typing to identify the type of hemoglobin present, which may indicate α-thalassemia, β-thalassemia, or a normal Hb variant.
In Strategy 2, all pregnant women are screened using MCV/MCH and Hb typing, with results classified as either positive or negative. If a woman tests positive, her at-risk husband is offered the same test to determine whether both are thalassemia carriers, potentially indicating α-thalassemia, β-thalassemia, or a normal Hb type.
In Strategy 3, both partners are screened using MCV/MCH and DCIP, with results also classified as either positive or negative. If both test positive, they are offered Hb typing to identify the specific Hb variant, which may indicate α-thalassemia, β-thalassemia, or normal Hb type. However, if only one partner has a positive result on MCV/MCH and DCIP screening, no further testing is performed because the fetus is not considered at high risk for severe thalassemia.
In all three strategies, if either partner is suspected of being a carrier of α-thalassemia or β-thalassemia based on Hb typing, DNA analysis is performed to confirm carrier status. For high-risk couples, the pregnant woman is offered a prenatal diagnostic procedure to confirm the fetus’s thalassemia status. If the fetus is confirmed to be affected by severe thalassemia, the couple is given the option of termination of pregnancy (TOP) to prevent the birth of an affected child. If the couple declines TOP or if the fetus is a false negative, the child may be born with either severe or a non-severe thalassemia.
Model Parameters
The input parameters incorporated in the model were categorized into four classifications: probabilities, screening and diagnostic performance, costs, and outcomes. The values assigned to these parameters are detailed in Table 2.
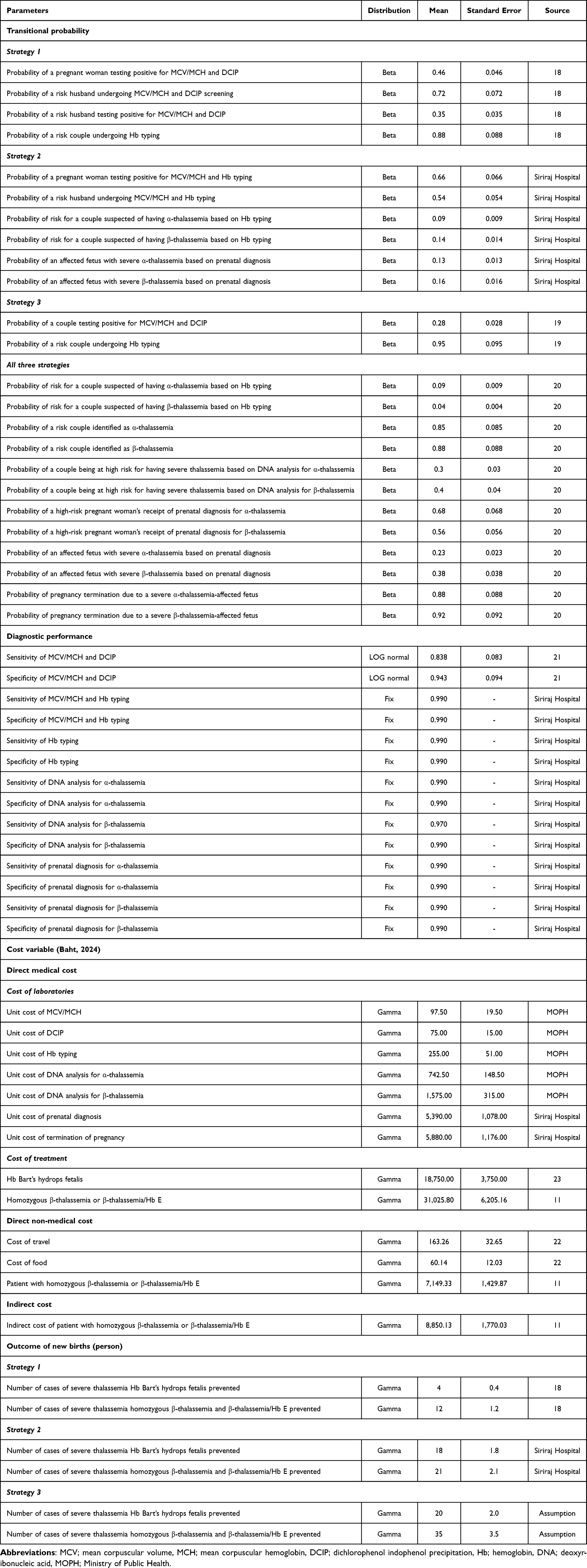 |
Table 2 Input Parameters |
Transitional Probabilities
The model included probability parameters such as the incidence of thalassemia carriers for each test, acceptance rates, the prevalence of severe thalassemia, and the rate of pregnancy termination. These values were derived from an evaluation report on thalassemia prevention and control during pregnancy across twenty health facilities in four regions of Thailand,19 the Siriraj Hospital database, and relevant published studies.20,21
Screening and Diagnostic Performance
Performance characteristics, including sensitivity and specificity, were obtained from a published study22 and the Siriraj Hospital database.
Cost
Cost data including direct medical costs, direct non-medical costs, and indirect costs were adjusted to 2024 values using the consumer price index (CPI) and discounted at an annual rate of 3%. An exchange rate of 35.29 Baht per USD was applied (2024 prices).23 Direct medical costs comprised expenses for laboratory services and treatment. Direct non-medical costs covered out-of-pocket expenses related to medical procedures, such as transportation, meals for the pregnant woman and her partner, and informal care in cases where an infant was diagnosed with homozygous β-thalassemia or β-thalassemia/Hb E. Indirect costs were defined as the loss of productivity due to illness. All cost data were derived from the MOPH database, the Siriraj Hospital database, the Standard Cost List for Health Technology Assessment (HTA), a widely accepted reference cost list in Thailand,24 and published studies.11,25
Outcome
Health outcomes were measured by the number of severe thalassemia cases prevented, including Hb Bart’s hydrops fetalis, homozygous β-thalassemia, and β-thalassemia/Hb E. The prevention of severe thalassemia cases represents a long-term benefit over the lifetime horizon, contributing to a sustained reduction in disease burden and lifetime healthcare costs. The outcomes for Strategy 1 were derived from an evaluation report on thalassemia prevention and control in pregnancy,19 those for Strategy 2 were obtained from the Siriraj Hospital database. As outcomes for Strategy 3 have not been officially reported, they were estimated using the proportion of positive cases recorded in the National Health Security Office (NHSO) database and supplemented by expert opinion from three clinical experts.
Uncertainty Analysis
An evaluation of input parameter uncertainty was carried out through both one-way and probabilistic sensitivity analyses (PSA). The one-way sensitivity analysis, each parameter was varied within its 95% confidence interval (CI), and the corresponding range of incremental cost-effectiveness ratio (ICER) values was illustrated using a Tornado diagram. For the PSA, uncertainty across all parameters were evaluated simultaneously using 1,000 Monte Carlo simulations. Probabilities were modeled using beta distributions, screening performance measures using log-normal distributions and fixed values, and cost and outcome parameters using gamma distribution. The findings from the PSA were represented graphically through cost-effectiveness planes.
Results
Cost-Effectiveness Analysis
This base case analysis included pregnant women of all ages, their high-risk partners, and couples undergoing prenatal screening and diagnosis, with outcomes measured in terms of thalassemia cases prevented. The estimated total costs and health outcomes from a societal perspective are presented in Table 3. Both Strategy 2 and Strategy 3 resulted in higher costs compared with Strategy 1, with additional costs of 853.40 Baht (24.20 USD) and 475.60 Baht (13.49 USD), respectively. However, when screening 10,000 couples, Strategy 2 and Strategy 3 identified 60 and 49 additional cases of severe thalassemia, respectively, compared to Strategy 1. The ICERs for Strategy 2 and Strategy 3 were approximately 141,863 Baht (4,023 USD) and 97,996 Baht (2,779 USD) per severe thalassemia case prevented, respectively. Furthermore, Strategy 2 also incurred higher costs than Strategy 3, with an additional cost of 377.80 Baht (10.71 USD). When screening 10,000 couples, Strategy 2 identified 12 more cases of severe thalassemia compared to Strategy 3. The resulting ICER for Strategy 2, when compared directly to Strategy 3, was approximately 325,013 Baht (9,218 USD) per severe thalassemia case prevented.
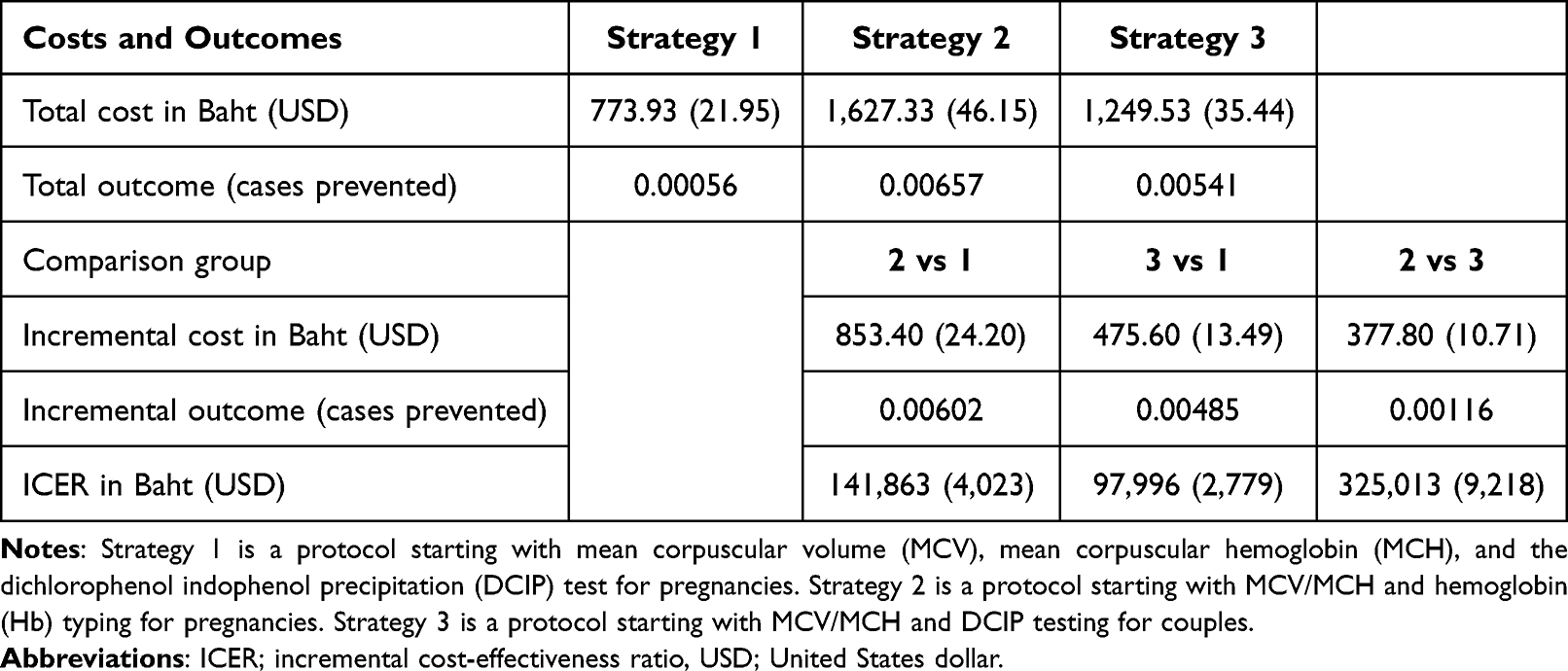 |
Table 3 Cost-Effectiveness Results |
Uncertainty Analysis
The results of the one-way sensitivity analysis are illustrated using Tornado diagrams in Figures 2–4. For Strategy 2 versus Strategy 1, the ICER was most sensitive to the specificity of prenatal diagnosis for α-thalassemia, followed by the probability of pregnancy termination in cases of severe α- and β-thalassemia-affected fetus (Figure 2). When comparing Strategy 3 to Strategy 1, the ICER was most sensitive to the probability of pregnancy termination for fetuses affected by severe α-thalassemia, followed by the specificity of prenatal diagnosis for α-thalassemia, and the probability of termination for β-thalassemia-affected fetuses (Figure 3). In the comparison between Strategy 2 and Strategy 3, the ICER was most influenced by the specificity of prenatal diagnosis for β-thalassemia, followed by the probability of a couple testing positive on MCV/MCH and DCIP, and the probability of pregnancy termination due to severe α-thalassemia-affected fetus (Figure 4).
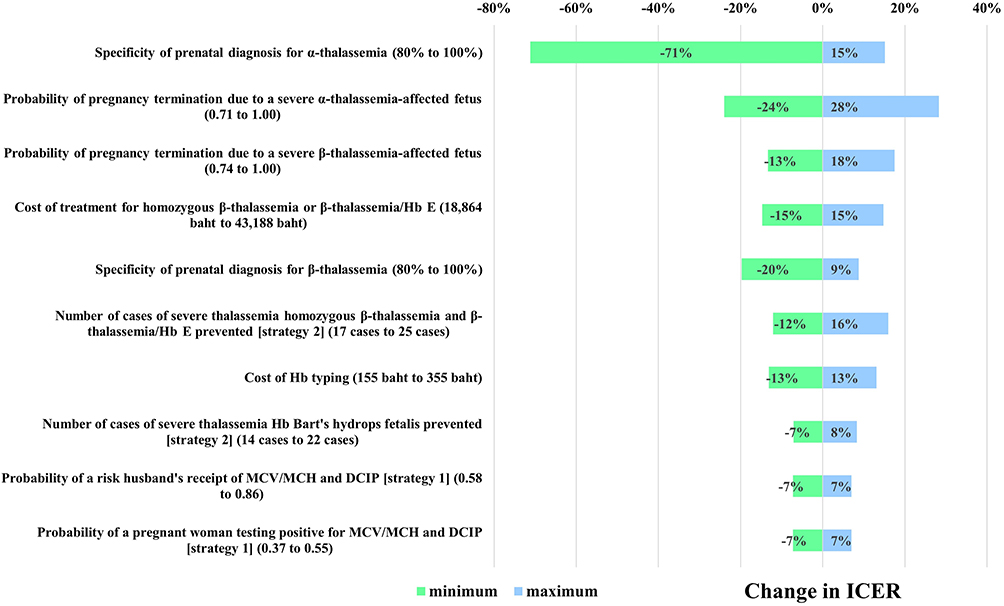 |
Figure 2 Tornado diagram of Strategy 2 versus Strategy 1. Abbreviation: ICER, incremental cost-effectiveness ratio. |
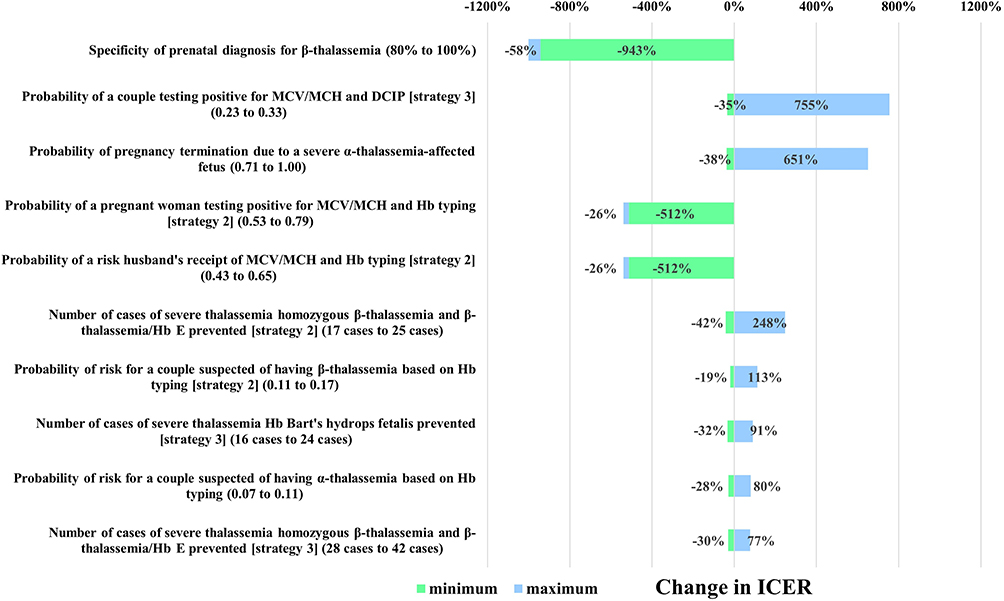 |
Figure 3 Tornado diagram of Strategy 3 versus Strategy 1. Abbreviation: ICER, incremental cost-effectiveness ratio. |
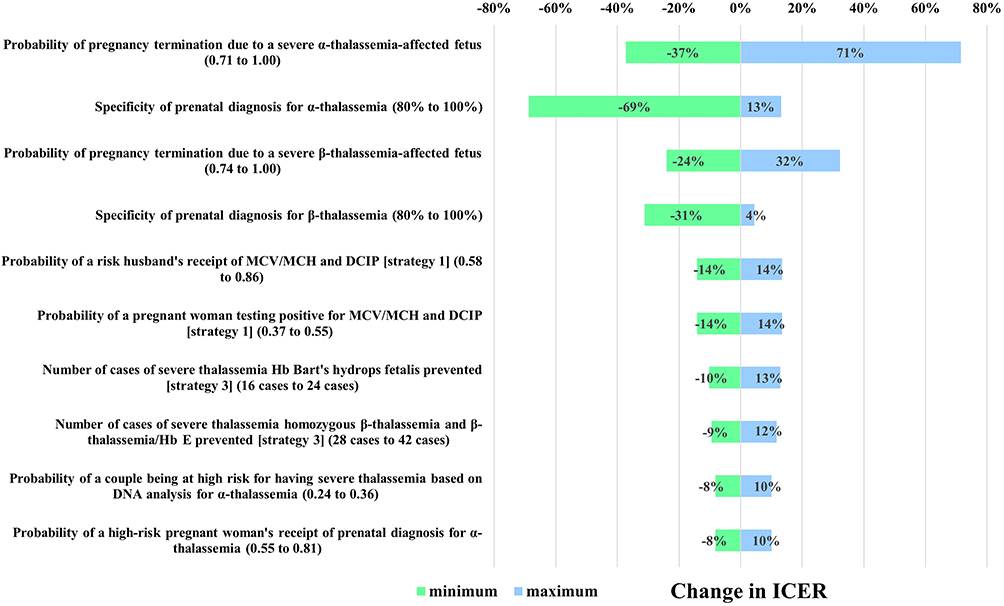 |
Figure 4 Tornado diagram of Strategy 2 versus Strategy 3. Abbreviation: ICER, incremental cost-effectiveness ratio. |
Figure 5 illustrates the cost-effectiveness plane, where the majority of simulations fall within the northeast quadrant. The average ICERs were 141,861 Baht (4,023 USD), 98,313 Baht (2,788 USD), and 328,259 Baht (9,310 USD) per severe thalassemia case prevented for Strategy 2 compared with Strategy 1, Strategy 3 compared with Strategy 1, and Strategy 2 compared with Strategy 3, respectively.
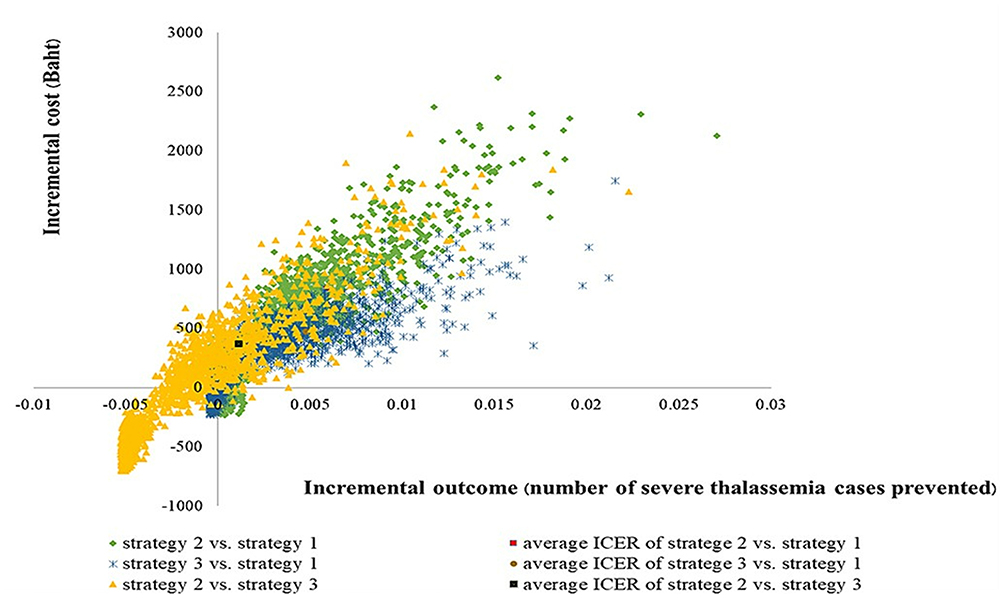 |
Figure 5 Cost-effectiveness plane. |
Discussion
This study is the first to evaluate the cost-effectiveness of three currently implemented prenatal thalassemia screening strategies for Thai pregnant women and couples, providing important insights into the economic and clinical impact of each approach. Our findings indicated that while both Strategy 2 (screening all pregnant women with MCV/MCH and Hb typing) and Strategy 3 (MCV/MCH and DCIP testing for couples) incurred higher costs compared to Strategy 1 (MCV/MCH and DCIP testing for pregnant women only), they also prevented significantly more cases of severe thalassemia. Remarkably, Strategy 3 emerged as the most cost-effective option compared to Strategy 1, with an ICER of 97,966 Baht (2,779 USD) per severe thalassemia case prevented, followed by Strategy 2 (ICER= 141,863 Baht; 4,023 USD). When directly compared with Strategy 3, Strategy 2 yielded a substantially higher ICER of 325,013 Baht (9,218 USD) per severe thalassemia case prevented.
Our findings suggested that Strategy 3 would be the most cost-effective approach. This may be attributed to the early and simultaneous screening of both partners, which increases the likelihood of identifying high-risk couples early in pregnancy. Early detection facilitates timely referral for genetic counseling and prenatal diagnosis, supporting couples in making educated choices about their reproductive options. Additionally, this strategy reduces the need for follow-up testing and minimizes delays in clinical decision-making, factors that may enhance the clinical effectiveness and overall efficiency of the screening program. From a public health perspective, preventing births of infants with severe thalassemia not only reduces clinical morbidity and mortality, but also mitigates the long-term financial strain on the healthcare system and affected families. As demonstrated in previous studies, the lifetime cost of managing a child with transfusion-dependent β-thalassemia or Hb Bart’s hydrops fetalis represents a significant economic and societal burden.5,10 The current findings reinforce the cost-saving potential of effective prenatal screening strategies by avoiding the substantial expenses associated with lifelong disease management, even if initial screening costs are higher.
Furthermore, the one-way sensitivity analysis revealed that, when comparing Strategy 2 to Strategy 1, the specificity of prenatal diagnosis for α-thalassemia was the most influential parameter. In contrast, for Strategy 3 versus Strategy 1, the probability of pregnancy termination in cases of severe α-thalassemia had the greatest impact. Additionally, when comparing Strategy 2 to Strategy 3, the specificity of prenatal diagnosis for β-thalassemia emerged as the most sensitive parameter. These findings underscored the importance of diagnostic accuracy, not only in shaping the model’s clinical outcomes but also in highlighting reflect real-world challenges such as social and cultural barriers that influence the acceptability of pregnancy termination in confirmed cases of fetal thalassemia.
Our findings align with a study conducted by Laoarayawat et al21 in Thailand, demonstrating that the semi-accelerated screening protocol, beginning with MCV/MCH testing for couples, followed by Hb typing for those with positive results was more cost-effective than conventional screening approaches, such as Strategy 1. Additionally, six economic evaluations have shown that prenatal screening programs for thalassemia prevention are more cost-effective than no screening, particularly from a healthcare provider perspective.26–31 Although our previous CBA study indicated that a standard screening program with genetic testing could result in cost savings of approximately 490 USD per severe thalassemia case prevented, when compared to screening without DNA analysis from a societal perspective,14 no prior studies have systematically compared all three prenatal screening strategies as performed in the present study. This CEA study was conducted to address that gap, enabling a comprehensive comparison and identifying the most cost-effective approach to inform both clinical practice and policy decision-making.
Thailand has made considerable progress in implementing national policies for thalassemia prevention, with screening guidelines introduced in 1992 and updated in 2009 and 2016. However, variation in screening protocols across regions and institutions driven by resource availability, logistical constraints, and local clinical preferences continues to challenge the standardization of care. Currently, both Strategy 1 and Strategy 3, endorsed by the Department of Medical Sciences, MOPH, are widely used in health facilities throughout Thailand. Strategy 1 is primarily implemented in primary care hospitals, while Strategy 3 is employed in several hospitals in the northern and northeastern regions, where the prevalence of thalassemia is higher.17,18 In contrast, Siriraj Hospital, a leading university hospital, has adopted Strategy 2. This study provides timely, evidence-based support for harmonizing prenatal screening protocols. Given that all three strategies are already covered by the UHC benefit package, policymakers should consider formally adopting Strategy 3, the most cost-effective approach, as the national standard to maximize both clinical and economic benefits.
Although Strategies 2 and 3 are more effective than strategy 1, access to Hb typing and genetic testing continues to be restricted in general, tertiary, and university hospital settings. A national survey conducted across 95 hospitals in Thailand revealed that Hb typing was accessible in only 67.4% of the facilities, whereas genetic testing was available in merely 24.2%.25 Therefore, Strategy 3 should be implemented in the official national prenatal screening guidelines for thalassemia prevention, particularly in light of recent data indicating an increasing prevalence of thalassemia in central Thailand, partly due to migration.4,5 However, Strategy 2 may be suitable for implementing in hospitals with adequate laboratory capacity and specialized personnel. Therefore, access to prenatal thalassemia diagnosis may vary across regions due to differences in availability of diagnostic facilities and trained personnel. Ensuring equitable access is essential to maximize the public health impact of screening programs and to prevent disparities in health outcomes.
Although this study presents noteworthy findings, it is essential to acknowledge several limitations. First, the outcomes for Strategy 3 were based on government reports and expert opinions, which may introduce bias due to assumptions rather than empirical data. Second, the effectiveness data for Strategy 2 were derived from a single hospital located in the central region of Thailand, a region with a low to moderate prevalence of thalassemia. This may have led to an underestimation of the potential benefits in higher-prevalence regions. Nevertheless, a comprehensive uncertainty analysis was conducted to assess the reliability of the findings. Future research should prioritize the collection of real-world data across diverse healthcare settings and geographic regions in Thailand to further validate these findings.
Conclusion
To our knowledge, this is the first study to comprehensively evaluate the cost-effectiveness of three currently implemented prenatal thalassemia screening strategies in Thailand. Our findings highlight that Strategy 3, screening with MCV/MCH and DCIP testing for couples, is the most cost-effective approach for preventing severe thalassemia, offering significant clinical and economic benefits. By enabling earlier identification of high-risk pregnancies, this strategy facilitates timely genetic counseling and informed decision-making, consequently lessening the impact of the disease on families involved and the healthcare system. Given that all three strategies are covered under the UHC benefit package, our results provide strong evidence to support the formal adoption of Strategy 3 as the national standard. While the recommended screening strategies are expected to reduce the burden of severe thalassemia, their implementation may face challenges such as limited access to diagnostic facilities in some regions, variability in public awareness, and resource constraints that could affect program uptake and effectiveness. Policymakers should consider investing in infrastructure and workforce development to ensure equitable access to effective screening services nationwide. Finally, harmonizing prenatal screening protocols based on evidence-driven, cost-effective approaches will play a critical role in reducing the incidence and societal burden of severe thalassemia in Thailand.
Ethics Approval
We based our analysis on data derived from previous published studies. This study was approved by the Institutional Review Board (IRB) of the Faculty of Dentistry and the Faculty of Pharmacy, Mahidol University (MU-MOU CoA. 2023/042.0808), and the ethics committee granted a waiver for the requirement of informed consent. All procedures were carried out in compliance with International Guidelines for Human Research Protection such as the Declaration of Helsinki, Belmont Report, CIOMS Guidelines and International Conference on Harmonization in Good Clinical Practice (ICH-GCP).
Acknowledgment
The authors wish to convey their profound gratitude to the Social, Economic and Administrative Pharmacy (SEAP) Graduate Program at Mahidol University for their invaluable support in research activities and the provision of essential facilities. This study was funded by the Health Systems Research Institute (HSRI) and Mahidol University (Fundamental Fund: fiscal year 2024 by National Science Research and Innovation Fund (NSRF). It is hereby acknowledged that the funding entity exerted no influence over the data analysis, interpretation of results, formulation of conclusions, or the preparation of this manuscript. The first author respectfully extends profound gratitude to Mahasarakham University for the award of a Ph.D. scholarship. Furthermore, the authors express their deep appreciation to the Siriraj Thalassemia Center, Faculty of Medicine Siriraj Hospital, Mahidol University, for their generous support in facilitating data collection throughout the course of this study.
Disclosure
No conflicts of interest are reported by the authors in relation to this study.
References
1. Musallam KM, Lombard L, Kistler KD, et al. Epidemiology of clinically significant forms of alpha- and beta-thalassemia: a global map of evidence and gaps. Am J Hematol. 2023;98(9):1436–1451. doi:10.1002/ajh.27006
2. Tuo Y, Li Y, Li Y, et al. Global, regional, and national burden of thalassemia, 1990–2021: a systematic analysis for the global burden of disease study 2021. EClinicalMedicine. 2024;72:102619. doi:10.1016/j.eclinm.2024.102619
3. Goh LPW, Chong ETJ, Lee PC. Prevalence of Alpha(alpha)-thalassemia in Southeast Asia (2010–2020): a meta-analysis involving 83,674 subjects. Int J Environ Res Public Health. 2020;17(20):7354. doi:10.3390/ijerph17207354
4. Kattamis A, Forni GL, Aydinok Y, Viprakasit V. Changing patterns in the epidemiology of beta-thalassemia. Eur J Haematol. 2020;105(6):692–703. doi:10.1111/ejh.13512
5. Paiboonsukwong K, Jopang Y, Winichagoon P, Fucharoen S. Thalassemia in Thailand. Hemoglobin. 2022;46(1):53–57. doi:10.1080/03630269.2022.2025824
6. Jatavan P, Chattipakorn N, Tongsong T. Fetal hemoglobin Bart’s hydrops fetalis: pathophysiology, prenatal diagnosis and possibility of intrauterine treatment. J Matern Fetal Neonatal Med. 2018;31(7):946–957. doi:10.1080/14767058.2017.1301423
7. Songdej D, Babbs C, Higgs DR, Consortium BI. An international registry of survivors with Hb Bart’s hydrops fetalis syndrome. Blood. 2017;129(10):1251–1259. doi:10.1182/blood-2016-08-697110
8. Koohi F, Kazemi T, Miri-Moghaddam E. Cardiac complications and iron overload in beta thalassemia major patients-a systematic review and meta-analysis. Ann Hematol. 2019;98(6):1323–1331. doi:10.1007/s00277-019-03618-w
9. Ansari-Moghaddam A, Adineh HA, Zareban I, Mohammadi M, Maghsoodlu M. The survival rate of patients with beta-thalassemia major and intermedia and its trends in recent years in Iran. Epidemiol Health. 2018;40:e2018048. doi:10.4178/epih.e2018048
10. Udeze C, Evans KA, Yang Y, et al. Economic and clinical burden of managing transfusion-dependent beta-thalassemia in the United States. J Med Econ. 2023;26(1):924–932. doi:10.1080/13696998.2023.2235928
11. Riewpaiboon A, Nuchprayoon I, Torcharus K, Indaratna K, Thavorncharoensap M, Ubol BO. Economic burden of beta-thalassemia/Hb E and beta-thalassemia major in Thai children. BMC Res Notes. 2010;3:29. doi:10.1186/1756-0500-3-29
12. Zhen X, Ming J, Zhang R, et al. Economic burden of adult patients with beta-thalassaemia major in mainland China. Orphanet J Rare Dis. 2023;18(1):252. doi:10.1186/s13023-023-02858-4
13. Esmaeilzadeh F, Azarkeivan A, Emamgholipour S, et al. Economic burden of thalassemia major in Iran, 2015. J Res Health Sci. 2016;16(3):111–115.
14. Malasai K, Jittikoon J, Udomsinprasert W, et al. Cost-benefit analysis of genetic testing as a prenatal diagnostic tool for thalassemia: a single-center study from Central Thailand. Clinicoecon Outcomes Res. 2025;17:33–43. doi:10.2147/CEOR.S500802
15. Gupta R, Radhakrishnan N, Shankar R, Ray S. Comparative analysis of the cost of thalassemia screening vs treatment in different healthcare sectors in Delhi National Capital Region. Indian J Public Health Res Dev. 2025;16(2):254–260. doi:10.37506/beprt342
16. Modell B. Guidelines for the control of haemoglobin disorders. Available from: https://iris.who.int/handle/10665/66665.
17. Laboratory guidelines for the diagnosis of thalassemia and hemoglobin abnormalities (Department of Medical Sciences, Ministry of Public Health); 2009.
18. Guidelines for laboratory testing to support the control and prevention of thalassemia (Department of Medical Sciences, Ministry of Public Health); 2016.
19. Health Intervention and Technology Assessment Program. An evaluation of thalassemia prevention and control in pregnancy program. Available from: https://www.hitap.net/documents/174625. Accessed March 30, 2025.
20. Tongsong T, Charoenkwan P, Sirivatanapa P, et al. Effectiveness of the model for prenatal control of severe thalassemia. Prenat Diagn. 2013;33(5):477–483. doi:10.1002/pd.4095
21. Bn LT, Dilokthornsakul P, Wong P, Upakdee N. Cost-effectiveness analysis of prenatal screening program for thalassemia between semi-accelerated screening step and current program. Rama Med J. 2020;43(1):13–23. doi:10.33165/rmj.2020.43.1.227046
22. Nillakupt K, Nathalang O, Arnutti P, et al. Prevalence and hematological parameters of thalassemia in Tha Kradarn subdistrict Chachoengsao Province, Thailand. J Med Assoc Thai. 2012;95(Suppl 5):S124–32.
23. The World Bank. Official exchange rate (per US$, period average) - Thailand. Available from: https://data.worldbank.org/indicator/PA.NUS.FCRF?locations=TH.
24. Riewpaiboon A. Standard cost lists for health economic evaluation in Thailand. J Med Assoc Thai. 2014;97(Suppl 5):S127–34.
25. Guidelines for the care of thalassemia patients in general practice (Department of Medical science, Ministry of Public Health); 2017.
26. Ostrowsky JT, Lippman A, Scriver CR. Cost-benefit analysis of a thalassemia disease prevention program. Am J Public Health. 1985;75(7):732–736. doi:10.2105/ajph.75.7.732
27. Ginsberg G, Tulchinsky T, Filon D, Goldfarb A, Abramov L, Rachmilevitz EA. Cost-benefit analysis of a national thalassaemia prevention programme in Israel. J Med Screen. 1998;5(3):120–126. doi:10.1136/jms.5.3.120
28. Cronin EK, Normand C, Henthorn JS, Graham V, Davies SC. Organisation and cost-effectiveness of antenatal haemoglobinopathy screening and follow up in a community-based programme. BJOG. 2000;107(4):486–491. doi:10.1111/j.1471-0528.2000.tb13267.x
29. Leung KY, Lee CP, Tang MH, et al. Cost-effectiveness of prenatal screening for thalassaemia in Hong Kong. Prenat Diagn. 2004;24(11):899–907. doi:10.1002/pd.1035
30. Bryan S, Dormandy E, Roberts T, et al. Screening for sickle cell and thalassaemia in primary care: a cost-effectiveness study. Br J Gen Pract. 2011;61(591):e620–7. doi:10.3399/bjgp11X601325
31. Application No.1531–Alpha Thalassaemia genetic testing (Australian Government); 2019.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.