Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Cost Assessment of Pediatric Haploidentical Hematopoietic Stem Cell Transplantation
Authors Achour L ![]() , Fazaa I
, Fazaa I ![]() , Drira C, Trabelsi Y, Ouederni M, Fradi I
, Drira C, Trabelsi Y, Ouederni M, Fradi I
Received 1 March 2025
Accepted for publication 20 June 2025
Published 30 September 2025 Volume 2025:17 Pages 653—659
DOI https://doi.org/10.2147/CEOR.S525645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Leila Achour,1,2 Ikram Fazaa,1,2 Chema Drira,1,2 Yosr Trabelsi,1 Monia Ouederni,3 Ines Fradi1,2
1Pharmacy Department, National Bone Morrow Transplant Center, Tunis, Tunisia; 2University of Tunis Manar, LR18ES39, Tunis, Tunisia; 3Pediatric Immuno-Hematology Department, National Bone Morrow Transplant Center, Tunis, Tunisia
Correspondence: Leila Achour, Pharmacy Department, National Bone Morrow Transplant Center, Tunis, Tunisia, Tel +216 3352892060, Email [email protected]
Purpose: Evaluate the costs related to the pediatric haplo-SCT and adult and pediatric geno-SCT at the CNGMO in order to establish a tailored reimbursement package by the Tunisian Health Insurance Fund.
Patients and Methods: This pharmaco-economic study compared the cost of pediatric haplo-SCT to adult and pediatric geno identical hematopoietic stem cell transplantation (geno-SCT) using the activity-based costing method. The cost assessment was conducted from the hospital’s perspective and considered direct medical and non-medical costs.
Results: The cost assessment indicated that pediatric patients incurred higher expenses than adult patients. Furthermore, haplo-SCT was more expensive than geno-SCT for pediatric patients. The conditioning regimens used before haplo-SCT are more intensive than other preparative regimens and typically require longer inpatient therefore resulting in more costs. Complications, such as infections during the early phase of neutropenia and late-onset issues following hematopoietic stem cell transplantation (HSCT), particularly graft-versus-host disease (GVHD) and cytomegalovirus (CMV) reactivation, significantly contribute to increased procedural costs.
Conclusion: This study sets the standards for new specific packages for haplo-SCT and geno-SCT in pediatric patients.
Keywords: haploidentical, stem cell transplant, pediatric, cost
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) still remains a curative approach for patients with both malignant and non-malignant hematologic pathologies.1
However, access to allo-HSCT is often limited due to the timely availability of a suitable HLA-matched related donor or adequately HLA-matched unrelated donor, which requires a register search that results in a considerable delay from diagnosis to treatment. The use of haploidentical hematopoietic stem cell transplantation (Haplo-SCT) is on the rise and is becoming a standard treatment option for patients who lack a matched donor.2
However, this highly specialized medical procedure requires expensive medical resources.
In Tunisia, the National Bone Marrow Transplant Center [Centre National de Greffe de MoelleOsseuse (CNGMO)] has initiated haplo-SCT for pediatric patients in 2018. It should be noted that the CNGMO used to receive a reimbursement by the Tunisian Health Insurance Fund [Caisse Nationale d’Assurance Maladie (CNAM)] for each HSCT, within a fixed global package amounting to $27,347 (2019 US Dollars) for geno identical hematopoietic stem cell transplantation (geno-SCT) and haplo-SCT for both adult and pediatric patients. The package covers all the necessary medical resources within the first year following the transplantation, including managing the complications.
Several studies have examined the financial impact of geno- and haplo SCT in adult patients. However, to our knowledge, no studies have been conducted on the pediatric population, either in Tunisia or elsewhere. The present study aims to evaluate the costs related to the pediatric haplo-SCT and pediatric and adult geno-SCT at the CNGMO in order to establish a tailored reimbursement package by the CNAM.
Materials and Methods
This is a descriptive pharmacoeconomic study carried out using the activity-based costing method. The cost assessment was conducted from the hospital’s (CNGMO) perspective included direct medical and non-medical costs from transplant up to 1 year. The monetary valuation was based on 2019 US Dollars.
First the process of HCT has been broken down into a sequence of activities that take part throughout the first year of this procedure. Thus, costs were divided into three phases: pre-transplantation, initial hospitalization, and follow-up:
The pre-transplantation phase included donor and recipient laboratory testing, graft harvesting and treatment.
The initial hospitalization phase included the full hospitalization in the transplant unit, conditioning protocols (Table 1), parenteral nutrition and hydration products, medical devices, investigations and biological tests and blood products (BPs) administration.
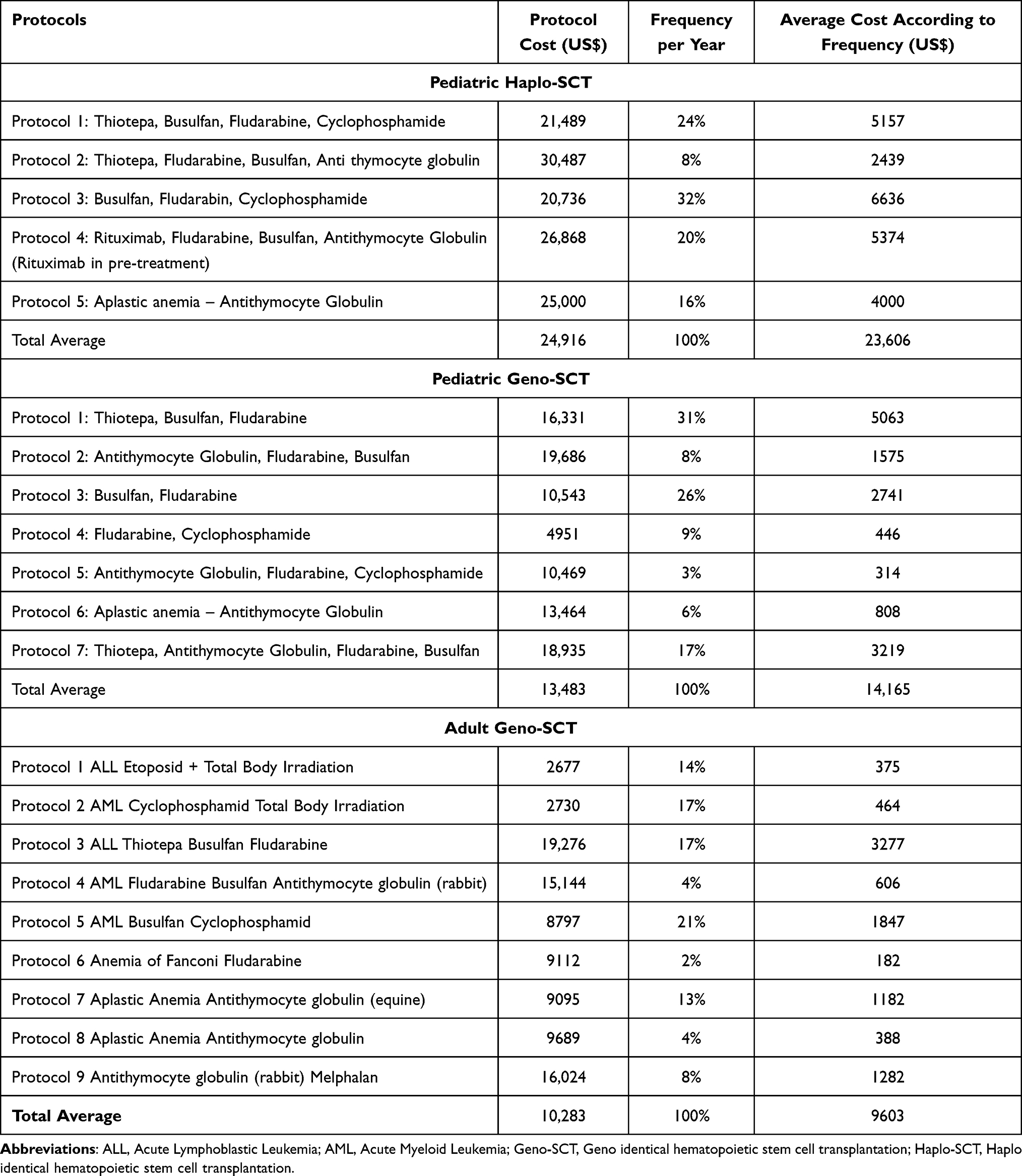 |
Table 1 Frequencies of the Conditioning Regimens |
The follow-up phase included outpatient consultations, imaging, laboratory test, the full hospitalization, medication and blood products administration. It also included complication treatment for Graft Versus Host Disease (GVHD) and cytomegalovirus reactivation (CMV) as well as post-acute care.
The cost evaluation excluded the costs of relapse.
The cost of biological analysis (virology, bacteriology, hematology, and biochemistry) was obtained through the national codification system for public structures, where each test code is assigned a specific price. The prices of medicines were collected from supplier invoices. In order to calculate the recommended drug dosages, a weight of 40 kilograms and a body surface of 1.28 m2 were assumed as mean parameters. The cost of conditioning protocols was calculated for each type implemented by adult and pediatric units. A Frequency-weighted average protocol cost was considered according to the frequencies of protocols used in 2019. The cost of medical devices was determined using the prices negotiated through the tender conducted by the CNGMO. A mean hospital length of stay is 45 days for adult allo-HSCT, 60 days for pediatric allo-HSCT and 90 days for Haplo-SCT according to previous studies made in the center.3 The cost per hospitalization day was assessed by considering the average salaries of medical and paramedical staff, the estimated time each category of staff spends with the patient, catering and patient meals, and general expenses including gas, electricity, sterilization, hygiene materials and maintenance (the annual maintenance expenses were divided by the number of hospitalization days in the adult or pediatric unit). In the follow-up phase, costs were estimated for patients without complications as well as for those with complications related to GVHD and CMV reactivation occurring separately or together. The total follow-up cost was estimated considering the frequency of each complication.
Results
The cost assessment showed that Pediatric geno-SCT is more expensive than the adult and that pediatric haplo-SCT cost is significantly higher. Indeed, the total estimated costs were $58,440 for adult geno-SCT, $86,446 for pediatric geno-SCT and $111,303 for pediatric haplo-SCT. Table 2 shows the costs included in the different phases of the procedure for the adult and pediatric geno-SCT and haplo-SCT.
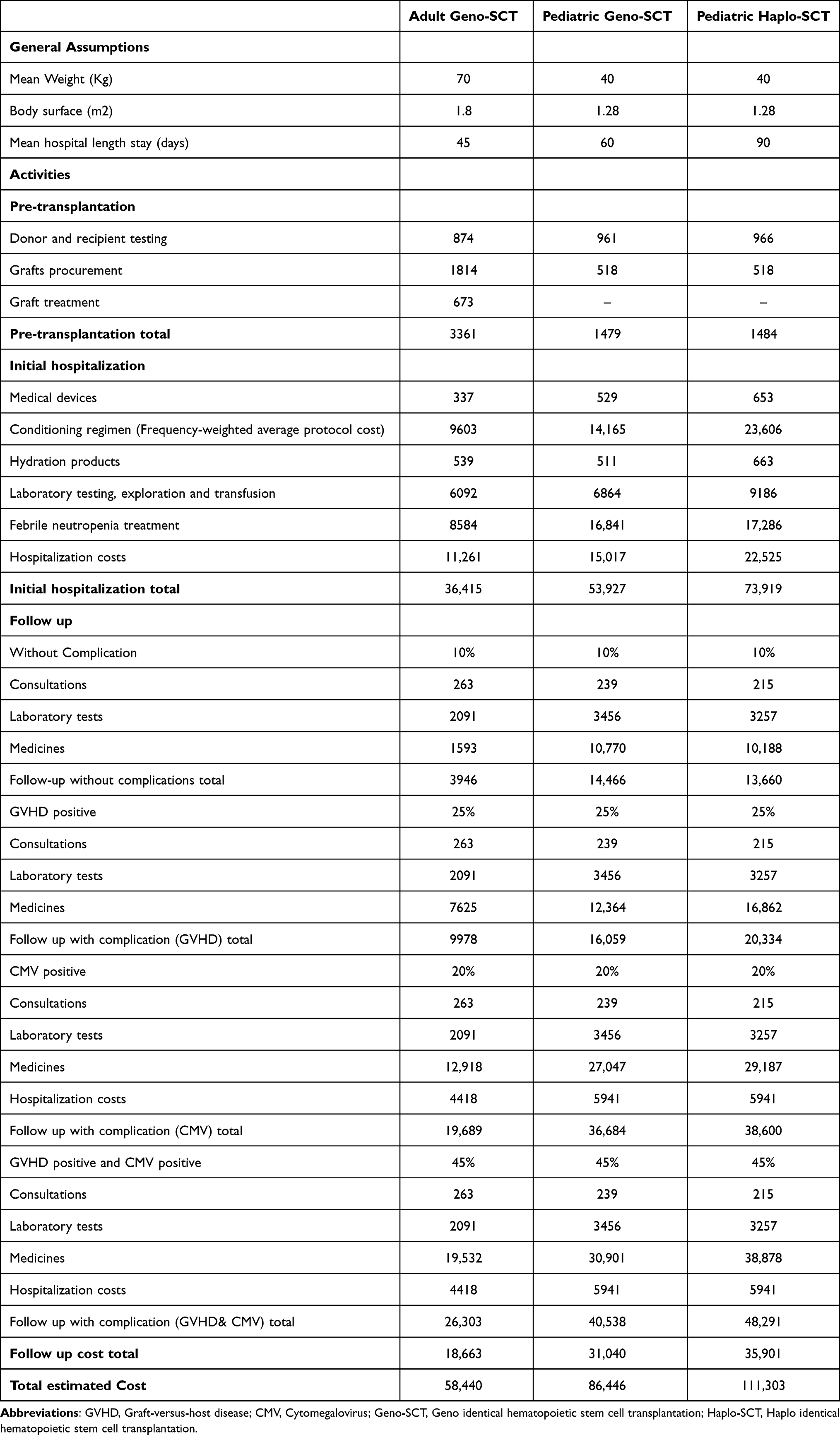 |
Table 2 Adult and Pediatric Geno-SCT and Haplo-SCT Discounted Costs from Transplant up to 1 year in US Dollars |
Pre-transplantation costs accounted for 6%, 2% and 1% for adult geno-SCT, pediatric geno-SCT and Pediatric haplo-SCT, respectively. Initial hospitalization phase was the costliest one and represented 62%, 62% and 66% of the total estimated cost for adult geno-SCT, pediatric geno-SCT and Pediatric haplo-SCT, respectively.
The costs of the follow-up phase exhibit significant variability depending on the occurrence of GVHD or CMV complications. As shown in Table 2, these costs can range from $13,660 without complications to $48,891 for patients with both GVHD and CMV.
Discussion
Haplo-SCT has become a significant treatment option for patients lacking a fully matched donor. This evaluation aim to assess the costs related to the pediatric haplo-SCT and pediatric and adult geno-SCT at the CNGMO in order to establish a tailored reimbursement package by the CNAM. In this study, we employed an activity-based costing method, which is considered the most common analytical approach in costing methodologies in health care because it provides a more detailed and accurate view of costs and therefore a better decision-making.4
Our cost assessment revealed that pediatric geno-SCT is more expensive than adult geno-SCT, and that the cost of pediatric haploidentical SCT (haplo-SCT) is significantly higher than both. Specifically, the total estimated costs were $58,440 for adult geno-SCT, $86,446 for pediatric geno-SCT, and $111,303 for pediatric haplo-SCT. The higher cost of pediatric haplo-SCT can be largely attributed to two main factors: the use of more expensive syrup formulations, which are necessary for young patients unable to take standard tablets, and a longer duration of hospitalization required for haploidentical procedures.
Several studies were conducted in the adult population, notably the one carried out in 2013, which estimated the direct costs of allograft during the first-year post-transplant.5 Another study conducted at the same center estimated the direct costs during the second year post-allograft.5 A retrospective analysis conducted in Marseille assessed the cost-effectiveness of haplo-SCT compared to matched unrelated donor transplantation in patients over 55 years old with hematological malignancies. The study found that haplo-SCT was more cost-effective, with a mean overall survival of 19.4 months and a mean cost of $108,134 compared to 15.1 months and $166,510 for matched unrelated donor transplantation. The incremental cost-effectiveness ratio was $163 per life year gained. In another study, researchers analyzed the costs of haplo-SCT, matched related donor (MRD), and matched unrelated donor (MUD) transplants. They found that the pre-transplant costs for MUD were significantly higher ($38) compared to MRD ($16) and haplo-SCT ($18). During the transplant phase, haplo-SCT incurred higher costs due to longer hospital stays and increased medication use. Overall, the total costs for haplo-SCT ($124) were similar to those for MUD ($127).6
These studies indicate that while haplo-SCT may have higher upfront costs, particularly during the transplant phase, it can be a cost-effective option, especially when considering the availability of donors and the potential for improved survival outcomes.
Furthermore, several studies have evaluated the efficacy and safety of haploSCT in pediatric patients. In 2021 study in Frontiers in Pediatrics compared haplo-SCT with geno-SCT in children with acute leukemia. The retrospective analysis found no significant differences in treatment outcomes, suggesting that haplo-SCT is a viable alternative to matched donor transplants.7 Another study, published in Bone Marrow Transplantation journal, evaluated the feasibility of haplo-SCT with post-transplantation cyclophosphamide (PTCy) in children with advanced pediatric malignancies. The research indicated that this approach is well-tolerated and can be performed universally, offering a promising treatment option for this patient group.8
However, most studies focus on the clinical outcomes, survival rates, and complications associated with children haplo-SCT, and no cost estimation study has been conducted worldwide. This makes our study unique and crucial, as it not only addresses an important gap in the literature but also provides valuable data to evaluate the cost-effectiveness and economic sustainability of haplo-SCT.
This cost assessment contributed to an update in the reimbursement policy by the CNAM, leading to individualized reimbursement amounts for each type of transplantation (see Table 3). The newly defined coverage system includes two main components:
- The transplantation phase, covering the pre-transplant period and the initial hospitalization, lasting up to three months.
- The follow-up phase, which extends up to one year following the end of the initial hospitalization. This phase includes the core post-transplant treatments such as immunosuppressive therapy, antimicrobial prophylaxis, growth factors, and other necessary supportive care but no complications (CMV, GVH, Neutropenia, …)
 |
Table 3 Coverage Packages Agreed Upon Between the CNGMO and the National Health Insurance (CNAM) in 2020 |
This distinction was necessary due to the high frequency and varying likelihood of post-transplant complications (such as CMV positive GVHD positive, CMV positive, GVHD positive, or cases without complications).
Nevertheless, this study presented some limitations. It was conducted shortly after the implementation of haploidentical transplantation in our center. As a result, the study was performed using the ABC method with an insufficient follow-up of real-world data. Further studies can be conducted with a larger number of patients and by including other perspectives (societal, etc).
Conclusion
The cost assessment showed that pediatric patients had higher costs than adult patients and that haplo-SCT is more expensive than geno-SCT for pediatric patients. This can be partly attributed to the longer average length of initial hospitalization for pediatric haplo-SCT compared to both pediatric and adult geno-SCT. Conditioning regimens for haplo-SCT are more intensive than other preparative regimens and generally require longer inpatient stays and thus increasing costs. Complications, such as infections during the early phase of neutropenia and late-onset complications following hematopoietic SCT, particularly GVHD and CMV reactivation, contribute to increased procedural costs.
By quantifying the costs involved, our study will help in comparing haplo-SCT with other forms of transplantation, especially in low-resource settings where financial considerations are particularly important.
This study facilitated the establishment of new specific packages for geno-identical and haplo-identical hematopoietic stem cell transplantation in pediatric patients. Furthermore, the package for pediatric haplo-SCT has nearly doubled from the initially applied $27,347. Additionally, medications for complications can be invoiced separately from the packages based on actual usage for each patient. Future research should compare the estimated costs using activity-based costing with real-world costs.
Abbreviations
CNGMO, National Bone Marrow Transplant Center; CNAM, the Tunisian Health Insurance Fund; allo-HSCT, Allogeneic hematopoietic stem cell transplantation; Haplo-SCT, Haploidentical hematopoietic stem cell transplantation; Geno-SCT, Genoidentical hematopoietic stem cell transplantation.
Ethical
No ethical approval or review by an institutional review board (IRB) or ethics committee was required for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gyurkocza B, Rezvani A, Storb RF. Allogeneic hematopoietic cell transplantation: the state of the art. Expert Rev Hematol. 2010;3(3):285–299. doi:10.1586/ehm.10.21
2. Arcuri LJ, Aguiar MTM, Ribeiro AAF, Pacheco AGF. Haploidentical transplantation with post-transplant cyclophosphamide versus unrelated donor hematopoietic stem cell transplantation: a systematic review and meta-analysis. Biol Blood Marrow Transplant. 2019;25(12):2422–2430. doi:10.1016/j.bbmt.2019.07.028
3. Achour L, Drira C, Sboui MZ, et al. Economic analysis of allogeneic hematopoietic stem cell transplantation in the bone marrow transplant center of Tunisia. J Mark Access Health Policy. 2023;11(1):2236851. doi:10.1080/20016689.2023.2236851
4. Jalalabadi F, Milewicz AL, Shah SR, Hollier LH, Reece EM. Activity-based costing. Semin Plast Surg. 2018;32(4):182–186. doi:10.1055/s-0038-1672208
5. Razgallah Khrouf M, Achour L, Thabti A, et al. Direct cost analysis of the second year post-allogeneic hematopoietic stem cell transplantation in the bone marrow transplant centre of Tunisia. J Mark Access Health Policy. 2017;5(1):1335161. doi:10.1080/20016689.2017.1335161
6. Debals-Gonthier M, Siani C, Faucher C, et al. Cost-effectiveness analysis of haploidentical vs matched unrelated allogeneic hematopoietic stem cells transplantation in patients older than 55 years. Bone Marrow Transplant. 2018;53(9):1096–1104. doi:10.1038/s41409-018-0133-5
7. Cho BS, Min GJ, Park S, et al. Haploidentical vs matched unrelated donor transplantation for acute myeloid leukemia in remission: a prospective comparative study. Am J Hematol. 2021;96(1):98–109. doi:10.1002/ajh.25993
8. Li Y, Wang N, Zhang X, et al. Post-transplantation cyclophosphamide as GVHD prophylaxis in allogenic hematopoietic stem cell transplantation: recent advances and modification. Blood Rev. 2023;62:101078. doi:10.1016/j.blre.2023.101078
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.