Back to Journals » Clinical Ophthalmology » Volume 19
Cosmetic Therapeutic Keratopigmentation
Authors Trindade BLC ![]() , Coelho IB, Magalhães LL, Crepaldi LA, Man Fu FM
, Coelho IB, Magalhães LL, Crepaldi LA, Man Fu FM ![]() , Da Glória LMR
, Da Glória LMR
Received 21 November 2024
Accepted for publication 10 February 2025
Published 13 February 2025 Volume 2025:19 Pages 527—534
DOI https://doi.org/10.2147/OPTH.S507490
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bruno Lovaglio Cançado Trindade,1– 3 Isadora Brito Coelho,1 Larissa Lima Magalhães,1 Letícia Arriel Crepaldi,1,2 Frederico Moreira Man Fu,2 Luiza Machado Ribeiro Da Glória2
1Cornea Department, Instituto de Olhos Ciências Médicas, Belo Horizonte, Brazil; 2Faculdade de Ciências Médicas de Minas Gerais, Belo Horizonte, Brazil; 3Cançado Trindade Eye Institute, Belo Horizonte, Brazil
Correspondence: Bruno Lovaglio Cançado Trindade, Cançado Trindade Eye Institute, Rua Manaus 595 – 30.150-350, Belo Horizonte, MG, Brazil, Email [email protected]
Purpose: To analyze indications safety and potential complications of cosmetic therapeutic corneal keratopigmentation to treat disfiguring aspect of opaque corneas.
Methods: Eight eyes of 8 consecutive patients were enrolled in therapeutic corneal keratopigmentation. Surgery was performed using manual technique, and a two-plane corneal dissection was performed. In the deeper pocket, brown pigment was injected to mimic iris color. In the more superficial and smaller pocket, black pigment was used to simulate pupillary opening.
Results: Seven out of 8 eyes had significant improvements in cosmesis after surgery. One patient did not have a major improvement due to significant superficial corneal neovascularization. In two eyes, there was pigment fading in the postoperative period, but no additional surgeries were performed. No complications were noted in any of the patients.
Conclusion: Therapeutic corneal keratopigmentation can lead to a significant change in ocular appearance and may improve self-esteem and overall life quality. Pigment fading and corneal neovascularization can be a potential problem. Careful patient selection and counseling are important to avoid patients seeking unachievable results.
Plain Language Summary: Blindness can lead to a disfiguring appearance caused by corneal opacification. In this study, we analyze the results of performing corneal tattoo to cover the “whiteish” aspect of the cornea and to restore a more natural look for the blind eye. This technique can be performed in eyes with opaque corneas requiring minimal additional surgical skills and can significantly improve patient’s self-esteem.
Keywords: keratopigmentation, corneal opacity, corneal tattoo, blind eye
Introduction
Blindness can be the end-stage of many ophthalmic conditions. Nevertheless, a sightless eye can compromise life-quality in more aspects than only the missing vision. The stigma related to a blind eye can cause social-life impairments and decrease in self-esteem.1,2 Irrespective of the baseline cause, a totally opaque cornea can damage personal appearance and may cause social reclusion. Many conditions can cause corneal opacities such as leukomas, scars, phthisis bulbi, among others. In these cases, the resulting corneal opacity can lead to a disfiguring look.3–5
Several treatment options exist for such conditions such as wearing sunglasses or tinted contact lenses, ocular prosthesis, keratoplasty and corneal keratopigmentation.6 All of them have limitations that preclude a widespread adoption for every patient. In most of these cases, the ocular surface is compromised, hence, the indication for contact-lens wear is not ideal. Ocular prosthesis can significantly improve cosmesis in atrophic eyes, but for cases of opaque corneas with a preserved globe volume, despite possible, their use can be challenging without performing prior evisceration or enucleation.7 Keratoplasty can be useful in restoring corneal transparency. However, the lack of corneal tissue availability can limit this application, especially in a blind eye. Moreover, such surgery might trigger other complications and phthisis bulbi itself, causing further compromise in ocular appearance.8
Corneal keratopigmentation is a procedure with a long track-record of safety for different conditions.1,2,4–6,9–14 It has been shown to be useful in covering iris defects such as in colobomas or iridotomies with good success. More recently, cosmetic “change of eye color” has been performed using corneal keratopigmentation with the assistance of femtosecond laser.15,16 However, for the purpose of this study, we will focus exclusively on the injection of pigment in the cornea for the purpose of restoring an adequate appearance in a blind eye.
Different techniques have been described to perform the injection of pigment into the corneal stroma. Superficial manual or automated micropuncture of the stroma have been shown to deliver the dye to the anterior stroma ameliorating the cosmesis of corneal opacity.1,4,5 Nevertheless, this technique has relatively high rate of retouch (45%) due to the superficial positioning of the dye.1 Intrastromal dye injection is possible by creating a pocket either manually or with the use of femtosecond laser.4,5,14,15,17 The advantage of this technique is the fact that the dye is buried into the stroma leading to less color fading and discoloring. Moreover, it maintains ocular surface integrity with a low complication rate.5
Pigment composition may vary but are usually made of lactic acid, propanediol and other micronized minerals.5 They have many different colors and different shades of them but basic color can be described as black, brown and green.
We report the use of keratopigmentation using a combination of manual superficial puncturing and lamellar dissection to improve cosmesis in blind eyes. The purpose of this study is to report the indication and safety of such approach and to analyze the cosmetic results as well as potential complications.
Materials and Methods
This is a retrospective consecutive study that included patients with total/sub-total corneal opacity in a blind eye (no light perception) that were submitted to manual intrastromal corneal keratopigmentation at a tertiary public hospital in Belo Horizonte, Brazil. Eight eyes of eight patients were included between April 2020 and August 2024. The cause of loss of vision was recorded and it is shown in Table 1. Institution ethics committee (CEP - Faculdade Ciências Médicas de Minas Gerais) approval was obtained prior to collecting all data (CAAE 81550824.0.0000.5134). All patients were informed about the purpose of the study, and patients’ consent was obtained from all subjects. The study was conducted in accordance with the tenets of the Declaration of Helsinki. All patients were evaluated before surgery with a full ophthalmic examination including B-scan. Conventional tattoo dyes (Spaulding & Rogers Mfg, Voorheesville, NY) were used in all the patients. In all cases, two stromal pockets were manually dissected. The thinnest point of the cornea was measured with ultrasonic pachymeter. A two-plane pocket creation was performed. The first one was deeper and would cover the entire cornea, from limbus to limbus. The second, a shallower pocket in the central cornea with a 3–4 mm diameter was created to mimic the pupil. For the dissection of the first deeper pocket, in case the thinnest corneal region was less than 600µm, the dissection was performed at 60% depth of the measured value. In case it was over 600µm, the deeper pocket was created at 350µm. The second smaller pocket was created at a shallower depth, 100µm over the larger pocket (around 200–250µm deep). Figure 1
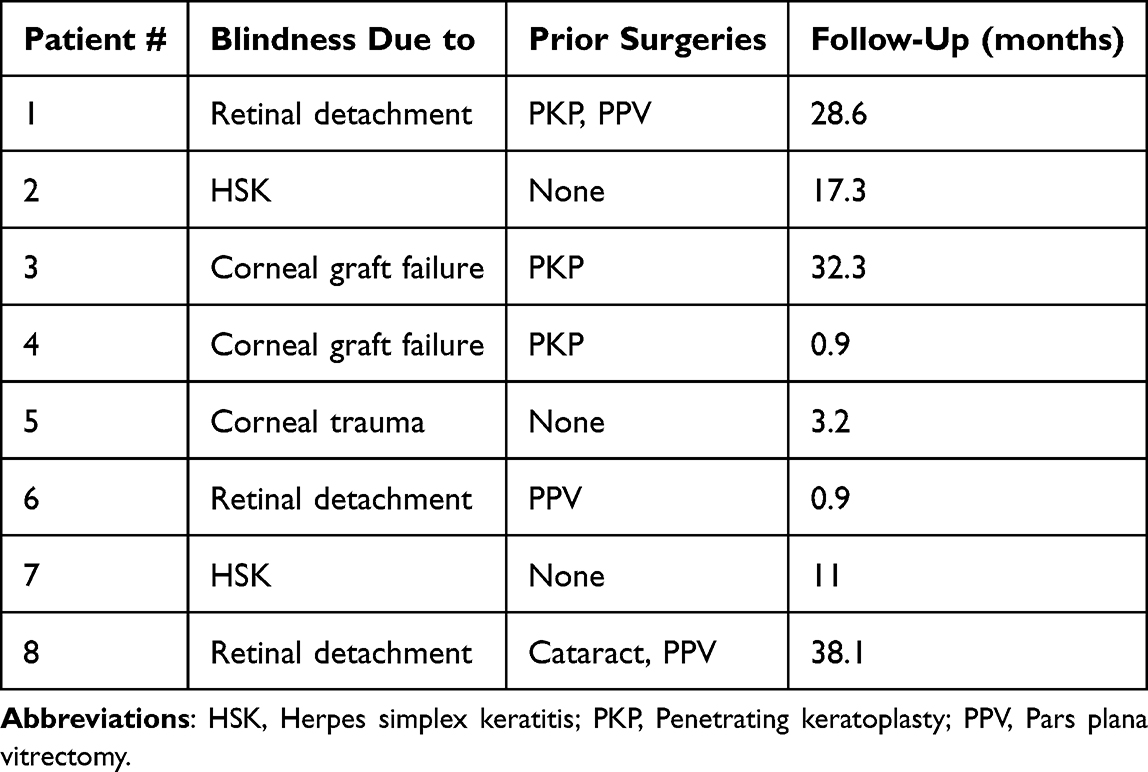 |
Table 1 Patients’ Ocular Characteristics |
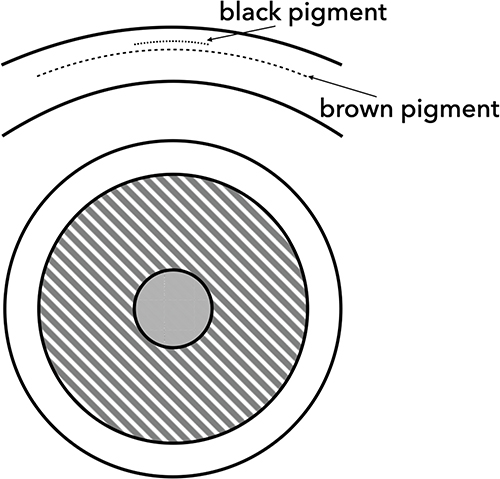 |
Figure 1 Diagram illustrating the two pockets created. The deeper pocket was used to inject the brown pigment whereas the black pigment was injected in the more superficial one. |
Both pockets were initiated with an adjustable diamond knife and dissected using a crescent blade and/or blunt corneal dissectors. The dark brown pigment (Color 8006 – Dark brown) was injected in the deeper pocket, and the black pigment (Color 8035 – Black #1) was injected at the superficial pocket to mimic pupil opening (Figure 2).
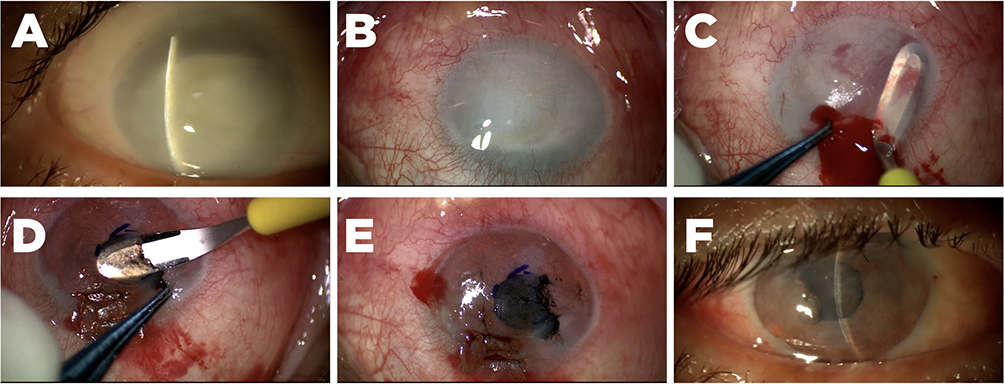 |
Figure 2 (A) Preoperative slit-lamp evaluation. Note the thick and diffusely opaque cornea. (B) Surgical microscope visualization in the beginning of the case. (C) Deeper pocket dissection. Note that dissection extends from limbus to limbus. (D) More superficial pocket dissection. (E) Final aspect at the end of surgery. (F) Slit-lamp appearance one week after the procedure. |
In some cases, due to focal areas of more opacified cornea, superficial manual micropuncturing of the cornea was performed to improve pigment expression. A bandage contact lens was placed and the end of the procedure. After surgery, patients were prescribed topical 0.3% moxifloxacin (Vigamox, Alcon, USA) as well as a tapering dose of 0.1% dexamethasone acetate (Maxidex, Alcon, USA) starting QID and reducing every week. Monocular and binocular pictures were taken, and a subjective grading of satisfaction after the procedure was performed by each patient.
Results
There was a significantly subjective cosmetic improvement in 7 out of 8 patients (87.5%) (Figures 3 and 4).
 |
Figure 3 Aspect before and after right eye keratopigmentation. |
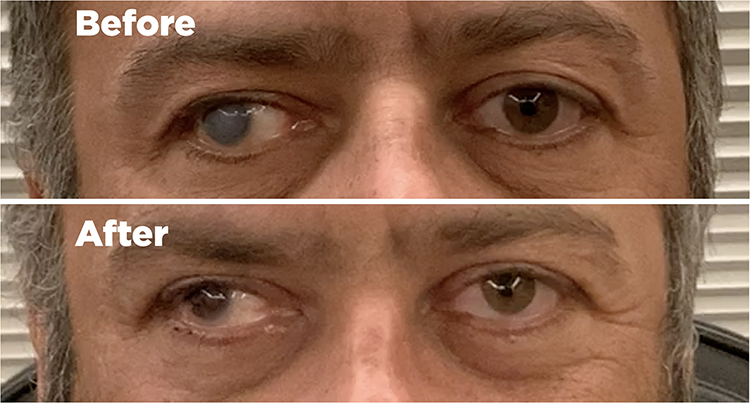 |
Figure 4 Aspect before and after right eye keratopigmentation. Note persistence of exotropia. |
In four patients, the lamellar technique was used in combination with focal areas of superficial micropuncturing. All eight corneas were reepithelialized within 5 to 7 days and no complications were noted in any of the surgeries performed. Mean follow-up was 17.8 months (ranging from 1 to 38 months). During the follow-up period, pigment clearing was observed in 2 patients during slit-lamp examination 6 months after the procedure (Figure 5).
 |
Figure 5 Pigment fading 6 months after procedure. This patient had a combination of lamellar dissection as well as micropuncturing of the central “pupil” area. The patient was still very satisfied with the result and no further procedure was performed. |
Nevertheless, none of them had noticed the clearing nor had any cosmetic complaints. This way, no further surgeries were performed. It is important to point out that the despite initial pigment clearing, the cosmesis of these two patients remained stable for the following follow-up period. In one patient, there was a very minor improvement of cosmesis due to a very vascularized corneal surface caused by longstanding limbal stem cells insufficiency. In this case, the pigment was not able to overcome the “pinkish” ocular surface. Figure 6 shows the subjective satisfaction after the procedure.
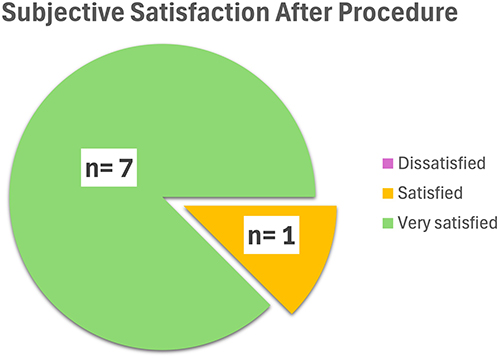 |
Figure 6 Patient’s subjective satisfaction after having been submitted to cosmetic therapeutic keratopigmentation. |
Discussion
Keratopigmentation is a procedure that has been introduced many years ago. It can be used to treat debilitating glare caused by sectoral iris defects or to cover corneal scars. More recently, the use of corneal tattoo has been reported as a way to block the natural color of the iris and to promote a pseudo-cosmetic change of the eye color in healthy eyes.9,15,16 We report the use of corneal pigmentation in eight patients as a mean to restore cosmetic acceptance in blind and disfigured eyes.
Total corneal leukoma and/or corneal opacity in a blind eye can cause significant social impairment and lead to decrease in self-esteem and public interactions. The use of keratopigmentation to treat these eyes has been reported for years from different groups.1,2,4,5 Different techniques can be used to insert the pigments in the cornea. A superficial micropuncturing technique can be performed either manually, using a bent 30-G needle or automated devices with multiple needles to inject the dye into the anterior stroma. Lamellar techniques can also be performed by sharp/blunt manual dissection or by using a femtosecond laser. Despite the femtosecond laser being able to produce a more precise and cosmetic dissection of the cornea, the altered anatomy and reduced corneal transparency can limit its use. Moreover, the added cost of the laser can be prohibitive for some patients. In our series, a combination of manual micropuncturing and manual lamellar dissection techniques was used with an overall good result.
It is important to point out that many of these longstanding blind eyes may eventually develop sensory exotropia.18 The cosmetic improvement of corneal keratopigmentation will obviously not correct for the outward drift of the eye. In fact, it may even make it more obvious after coloring the cornea. Correction of the strabismus may be performed later with surgery or even with botulinum toxin muscle injection.19 Patients must be aware of this prior to any intervention to avoid unrealistic expectations.
Globe volume might be reduced in pre- and phthisic eyes. Besides the obvious difference in globe size, hypotony might make corneal lamellar dissection more challenging, and maintaining a proper plane can be more difficult.
Ocular surface integrity is important to maintain a good overall eye health. In poorly seeing eyes, it is not uncommon to have concomitant ocular surface diseases. Moreover, for many of these patients, the condition that led to visual loss may play a role in the ocular surface. A neurotrophic cornea may not heal well after surgery, and the expected benefits of these procedures should be weighed against their potential risks.20 Limbal stem cell deficiency is also commonly present in eyes with longstanding ocular surface diseases.21–23 Corneal neovascularization can lead to poor outcome of keratopigmentation. The presence of superficial vascularization may give the eye a “pinkish” appearance that may persist even after pigment deposition into the cornea. These superficial vessels tend to produce a worse outcome than the deeper stromal vessels that can be more easily covered by the tattoo dies. In our series, we had one patient with significant superficial neovascularization that did not have a cosmetic improvement with the corneal tattoo procedure. For patients with chronic superficial corneal neovessels, we advise that proper counseling and informed expectations have to be carefully addressed before proceeding with surgery.
Lamellar techniques are usually performed in a two-plane approach. A color matching the contralateral iris color is injected in the deeper pocket dissected from limbus to limbus. A black dye is then injected in the more superficial pocket that was created in the central 3–4mm of the cornea to mimic the pupil. Due to the opaque nature of the corneal stroma, the deeper the dissected pockets are, the less cosmetically visible the pigments are going to be. This way, deeper pockets usually lead to a persistence of the opaque corneal appearance and would not render a good cosmetic result. In our patients, we performed lamellar dissection at a depth of 300–350µm. At this depth, we were able to achieve a good result while still maintaining a safe distance from the surface. In some cases, due to more pronounced opacified regions of the cornea, we opted for a superficial micropuncturing over these areas to better cover these opacities. This was achieved by puncturing the surface of the cornea covered with the dye with a bent 30-G needle.
Pigment fading can occur after keratopigmentation. Pigment color change has also been reported in the literature, possibly caused by corneal neovascularization.24 Retreatments can be performed by either injecting more dye in the previously dissected pockets or with the use of superficial micropuncturing technique. In our series, two patients presented with pigment fading six months after surgery. It is important to emphasize that the fading did not progress overtime. Instead, it became stable in the following visits. None of the patients complained of any cosmetic change and were still pleased with the outcome. This way, no retreatments were required.
Limitations of our study include a small number of subjects as well as a heterogenous group of baseline ocular disease.
All of our cases had a contralateral dark-colored eye. In our opinion, the impact of corneal opacities is more important in these patients since the difference to the other healthy eye will be even more pronounced. The edematous/opacified cornea usually exhibits a “blueish hue” that can be less noticed in light-colored patients. It is important to consider that this procedure, especially using the manual technique, is tailored for improvement of cosmesis but it will rarely match exactly the color of the fellow healthy eye. Additionally, the previously mentioned conditions such as strabismus, globe volume reduction and superficial neovascularization may prevent a perfect cosmetic matching between eyes. Showing clinical images of results of similar conditions can help counsel patients and gauge if their expectations can be achieved. Unrealistic expectations should be identified and addressed before surgery is considered. Moreover, the outcome of corneal pigmentation is only adequate at a reasonable social distance with a reasonable lighting condition. Slit-lamp analysis of the eye may reveal imperfections that will not compromise the overall outcome.
This way, the ideal case for this technique is a patient with a blind eye, with an opaque and thick cornea, without any corneal superficial neovascularization, with a preserved ocular alignment, a contralateral dark-colored iris and with adequate expectations. For these cases, keratopigmentation can provide a significant improvement of cosmesis. This is not a strict guideline since this procedure can still benefit different patients. The final goal is to provide a more cosmetic pleasing appearance and to improve self-esteem.
Conclusion
More research is still needed to develop new pigment technologies and more successful solutions to corneal superficial neovascularization and limbal stem-cell failure. Nevertheless, keratopigmentation can provide a significant improvement of ocular cosmesis in blind eyes. Manual techniques of lamellar and superficial micropuncturing can be combined to obtain a better outcome. This technique can be safely performed in these sick eyes to provide a social positive impact on these patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Shymali O, Rodriguez AE, Amesty MA, Alio JL. Superficial keratopigmentation: an alternative solution for patients with cosmetically or functionally impaired eyes. Cornea. 2019;38(1):54–61. doi:10.1097/ICO.0000000000001753
2. Doganay D, Doganay S, Cankaya C. Corneal tattooing for esthetic purposes in patients with corneal opacities. Indian J Ophthalmol. 2020;68(6):1033–1036. doi:10.4103/ijo.IJO_1502_19
3. Bonaque-Gonzalez S, Trujillo-Sevilla JM. Comment on: keratopigmentation; a comprehensive review. Eye. 2021;35(1):354. doi:10.1038/s41433-020-0828-x
4. Galvis V, Tello A. Keratopigmentation: techniques and results. Br J Ophthalmol. 2012;96(9):1270. [author reply 1270-1271]. doi:10.1136/bjophthalmol-2012-301795
5. Hasani H, Es’haghi A, Rafatnia S, Alilou S, Abolmaali M. Keratopigmentation: a comprehensive review. Eye. 2020;34(6):1039–1046. doi:10.1038/s41433-019-0750-2
6. Balgos JD, Amesty MA, Rodriguez AE, Al-Shymali O, Abumustafa S, Alio JL. Keratopigmentation combined with strabismus surgery to restore cosmesis in eyes with disabling corneal scarring and squint. Br J Ophthalmol. 2020;104(6):785–789. doi:10.1136/bjophthalmol-2019-314539
7. Dortzbach RK, Woog JJ. Choice of procedure. enucleation, evisceration, or prosthetic fitting over globes. Ophthalmology. 1985;92(9):1249–1255. doi:10.1016/S0161-6420(85)33886-1
8. Tanaka M, Ando M, Kitagawa H, et al. Penetrating keratoplasty surgery combined with vitrectomy after failing previous corneal surgery. Retina. 2003;23(1):41–47. doi:10.1097/00006982-200302000-00007
9. D’Oria F, Alio JL, Rodriguez AE, Amesty MA, Abu-Mustafa SK. Cosmetic keratopigmentation in sighted eyes: medium- and long-term clinical evaluation. Cornea. 2021;40(3):327–333. doi:10.1097/ICO.0000000000002417
10. Mannis MJ, Eghbali K, Schwab IR. Keratopigmentation: a review of corneal tattooing. Cornea. 1999;18(6):633–637.
11. Mohan S, Tripathi A, Patel N, Gupta V, Midha T. Intrastromal keratopigmentation: a boon for unsightly corneal scars. Int Ophthalmol. 2023;43(8):2787–2794. doi:10.1007/s10792-023-02700-7
12. Ravindra MS, Meda DR. A novel indigenous technique for corneal tattooing using self-prepared do-it-yourself carbon soot pigment. Indian J Ophthalmol. 2021;69(9):2516–2520. doi:10.4103/ijo.IJO_2759_20
13. Rodriguez AE, Amesty MA, El Bahrawy M, Rey S, Alio Del Barrio J, Alio JL. Superficial automated keratopigmentation for iris and pupil simulation using micronized mineral pigments and a new puncturing device: experimental study. Cornea. 2017;36(9):1069–1075. doi:10.1097/ICO.0000000000001249
14. Yin HY, Walter KA. Long-term outcome of femtosecond laser-assisted keratopigmentation: using intacs channels for precise pigment deposition within the cornea. Cornea. 2021;40(10):1330–1335. doi:10.1097/ICO.0000000000002667
15. Alio JL, Rodriguez AE, El Bahrawy M, Angelov A, Zein G. Keratopigmentation to change the apparent color of the human eye: a novel indication for corneal tattooing. Cornea. 2016;35(4):431–437. doi:10.1097/ICO.0000000000000745
16. D’Oria F, Abu-Mustafa SK, Alio JL. Cosmetic change of the apparent color of the eye: a review on surgical alternatives, outcomes and complications. Ophthalmol Ther. 2022;11(2):465–477. doi:10.1007/s40123-022-00458-2
17. Ziak P, Kapitanova K, Halicka J, Mojzis P. Keratopigmentation (Corneal Tattoo) - our first experience. Cesk Slov Oftalmol. 2019;74(4):140–144. doi:10.31348/2018/1/3-4-2018
18. Khorrami-Nejad M, Alghurab A, Akbari MR, Azizi E, Masoomian B. Sensory strabismus; a literature review. J Binocul Vis Ocul Motil. 2024;74(1):32–40. doi:10.1080/2576117X.2024.2319569
19. Binenbaum G, Chang MY, Heidary G, et al. Botulinum toxin injection for the treatment of strabismus: a report by the American Academy of Ophthalmology. Ophthalmology. 2021;128(12):1766–1776. doi:10.1016/j.ophtha.2021.05.009
20. Dua HS, Said DG, Messmer EM, et al. Neurotrophic keratopathy. Prog Retin Eye Res. 2018;66:107–131. doi:10.1016/j.preteyeres.2018.04.003
21. Carreno-Galeano JT, Dohlman TH, Yin J, Dana R. Limbal stem cell deficiency associated with herpes keratitis. Cornea. 2021;40(8):967–971. doi:10.1097/ICO.0000000000002557
22. Donthineni PR, Varma S, Kethiri A, et al. Histopathological characteristics of limbal stem cell deficiency secondary to chronic vernal keratoconjunctivitis. Cornea. 2022;41(6):722–728. doi:10.1097/ICO.0000000000002775
23. Atallah MR, Palioura S, Perez VL, Amescua G. Limbal stem cell transplantation: current perspectives. Clin Ophthalmol. 2016;10:593–602. doi:10.2147/OPTH.S83676
24. Alio JL, Al-Shymali O, Amesty MA, Rodriguez AE. Keratopigmentation with micronised mineral pigments: complications and outcomes in a series of 234 eyes. Br J Ophthalmol. 2018;102(6):742–747. doi:10.1136/bjophthalmol-2017-310591
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.