Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Corticosteroid Phobia in Patients with Atopic Dermatitis: A Narrative Review
Received 30 October 2025
Accepted for publication 12 March 2026
Published 18 May 2026 Volume 2026:19 577749
DOI https://doi.org/10.2147/CCID.S577749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Xue Chen, Zhirun Wang
Medicine School of Lishui University, Lishui University, Lishui, Zhejiang Province, People’s Republic of China
Correspondence: Zhirun Wang, Email [email protected]
Abstract: Atopic dermatitis (AD) is a prevalent chronic inflammatory skin disease worldwide, often accompanied by the complex progression of atopic conditions. This article reviews the current state of fear regarding corticosteroid treatment among patients with AD, analyzes the influencing factors and its impact on treatment adherence, integrates epidemiological data and pathogenesis, and examines the clinical advantages and limitations of corticosteroids in AD management. By critically evaluating the effectiveness of existing health education, psychological interventions, and personalized care strategies, this article aims to identify current research gaps and provide evidence-based guidance for optimizing standardized care pathways and improving patient outcomes.
Keywords: atopic dermatitis, glucocorticoids, corticosteroid phobia, nursing strategies, review
Introduction
Atopic Dermatitis (AD) is a prevalent chronic inflammatory skin disease. In recent years, the incidence and prevalence of AD have continued to rise globally, with over 230 million AD patients worldwide, making it a significant challenge in the field of public health.1,2 Epidemiological investigations reveal3,4 that the global prevalence of AD shows a persistent upward trend, with approximately 11%–20% in pediatric populations and 5%–8% in adult populations. Characterized by intense pruritus and chronic eczematous lesions, AD follows a relapsing-remitting course that severely disrupts patients’ sleep, social interactions, work/study performance, and overall quality of life5–7. Regarding pathogenesis, the field has long proposed two central hypotheses:8 the outside-in and inside-out theories. The outside-in hypothesis emphasizes external factors (such as microbial infections, allergens, physical or chemical stimuli) in the initial stages of disease, while the inside-out hypothesis posits that internal immune dysregulation and genetic factors are the starting points. Current research generally suggests that the onset of AD results from the combined action of internal and external factors, involving gene defects, impaired skin barrier function, abnormal immune responses, and dysbiosis of the skin microbiome. These elements interact in complex networks and feedback loops to form a vicious cycle that drives the occurrence and progression of the disease. Topical corticosteroids (TCS) remain first-line therapeutics for AD management. Their mechanism of action involves suppressing immune responses and inflammatory mediator production, thereby exerting anti-inflammatory and anti-allergic effects to rapidly alleviate AD symptoms, rendering them widely applicable in clinical practice.9,10 However,healthcare professionals frequently observe patient reluctance, refusal, or non-standardized use of TCS in clinical settings.11 Numerous adult AD patients and pediatric caregivers exhibit psychological apprehension toward TCS, a phenomenon termed “Corticosteroid Phobia”12 This fear may lead to non-adherence, self-reduction of dosage or frequency, or complete discontinuation of treatment, potentially triggering disease recurrence, exacerbation, prolonged disease course, and detrimental impacts on patients’ physical/mental health and quality of life.13 An international study identified14 Taiwan, China as one of three regions with the highest levels of corticosteroid phobia globally. Current international research on corticosteroid phobia in AD patients remains relatively insufficient and underrecognized. Therefore, investigating the status and influencing factors of TCS-related fear in AD patients, along with identifying effective nursing strategies, holds crucial significance for enhancing treatment outcomes and patient quality of life. This review aims to systematically summarize the current status of corticosteroid phobia in patients with AD and its influencing factors, and to identify feasible nursing strategies to improve treatment outcomes and patients’ quality of life. By synthesizing existing literature, we will analyze the external and internal drivers of fear, cognitive and behavioral changes, as well as the impact of interactions among patients, caregivers, and healthcare providers on adherence. This review will summarize differences across various cultural and regional contexts, evaluate the effectiveness and generalizability of existing interventions, and propose clinical nursing assessment tools, intervention pathways, and directions for future research, aiming to provide clinical nurses with a systematic and practical reference framework to help identify, assess, and effectively intervene in corticosteroid phobia, thereby improving treatment outcomes and quality of life for patients with AD.
Current Status of Corticosteroid Phobia in Atopic Dermatitis Patients
The pathogenesis of AD centers on skin barrier dysfunction, with stepped therapeutic strategies: emollients for barrier repair and TCS for acute flares. However, TCS phobia among patients and caregivers significantly impedes treatment adherence.
Multiple studies have shown that fear of corticosteroids exhibits significant differences among patients with AD and caregivers of children.15 High TCS phobia is also observed in non-AD chronic dermatosis caregivers (eg., young women with idiopathic granulomatous mastitis).16 Parental fear levels in AD children show substantial stratification: 51% display mild-to-moderate fear, while 49% reach severe intensity, indicating that therapeutic anxiety about corticosteroid regimens has become a central challenge in family health management.15 Cross-population comparisons reveal17 that adolescent AD patients exhibit significantly lower TCS fear than their caregivers, suggesting disease management responsibilities may amplify decision-making pressures in caregivers. This observation is consistent with research findings regarding the widespread cognitive biases about medication safety among nursing staff. Misunderstandings by healthcare providers themselves may exacerbate phobias; for example, only a small proportion of Southeast Asian respondents correctly understood the indications of TCS.18 The TOPICOP scale represents the first dedicated tool for quantifying TCS fear in AD patients and parents. Regional studies further elucidate cultural correlations in TCS phobia; TOPICOP scores among global patients and caregivers show significant cross-cultural differences.19,20 Stigmatization of “hormones” in Saudi Arabia elevates TOPICOP scores above global averages.21 International studies show22 that among 15 countries, China, Poland, and Ukraine have the highest TCS fear scores. These differences may reflect variations in doctor-patient communication patterns and systemic corticosteroid education in the healthcare system. Comparative analyses indicate comparable mean TOPICOP scores between AD and psoriasis patients,23 suggesting chronic dermatosis patients may share misconceptions about hormone therapies, though larger cohort validations remain necessary. Current findings indicate that corticosteroid phobia demonstrates widespread prevalence across countries and populations, though its severity varies significantly across demographic and geographic contexts. Corticosteroid phobia is both common and severe among patients with AD. Notably, there is a similar gradient of TCSawareness within the healthcare practitioner community: the medication-reserving attitude of nursing staff closely aligns with that of the children’s guardians, significantly higher than that of general practitioners and pediatric specialists.24–26 Given that guardians’ knowledge of TCS largely depends on professional guidance from healthcare providers, the cognitive tendencies of the medical team will significantly influence the effectiveness of treatment plan implementation through doctor–patient communication.27,28 To achieve effective application of TCS in care, it is recommended that relevant departments strengthen AD management training for healthcare personnel, promote systematic learning of TCS-related knowledge, and regularly assess training effectiveness to ensure that healthcare workers can educate caregivers on the efficacy and safety of TCS. By enhancing caregivers’ understanding and trust in TCS, reducing their fear, and increasing adherence, patient outcomes can be optimized, quality of life improved, and related economic burdens alleviated.
Future initiatives should prioritize collaborative patient-provider education frameworks (eg., TOPICOP-based personalized counseling). Consequently, healthcare providers must prioritize recognition of this phenomenon in AD patients and caregivers while developing targeted care strategies. Current international research predominantly focuses on cross-sectional investigations, lacking exploration into the evolutionary trajectories of fear dynamics or evidence-based intervention frameworks. Future studies should systematically investigate contributing factors and implementable interventions for corticosteroid phobia in AD populations, aiming to rectify cognitive biases, alleviate psychological distress, and enhance treatment adherence. Furthermore, rigorous randomized controlled trials are warranted to validate intervention efficacy, thereby establishing evidence-based foundations for optimizing therapeutic compliance and clinical outcomes in AD management.
Influencing Factors
The fear of corticosteroids in patients with AD is influenced by multiple factors that interact, collectively forming a complex picture of corticosteroid phobia. These primarily include treatment-related factors and patient-specific factors. Regarding treatment aspects, the potency of the corticosteroid used, duration of therapy, and application site may exacerbate patient concerns, with potent steroids or long-term use readily triggering cognitive biases about side effects such as skin atrophy. Among patient-specific factors, a lack of knowledge or misconceptions about steroid side effects is a core reason; some patients develop heightened resistance to treatment due to past inappropriate use leading to skin sensitivity or dependency. Furthermore, information sources and insufficient physician-patient communication further amplify fears, as patients might refuse standardized treatment without fully understanding the proper use of the medication. Psychological factors, such as an anxious disposition or helplessness induced by disease recurrence, are also related. Notably, differences in cultural background (societal perceptions stigmatizing “hormones”) and overprotective attitudes among parents of pediatric patients are equally significant. Targeted nursing care should integrate individualized education, stepwise treatment strategies, and psychological support to improve treatment adherence. Figure 1 illustrates the factors influencing corticosteroid fear in patients with AD.
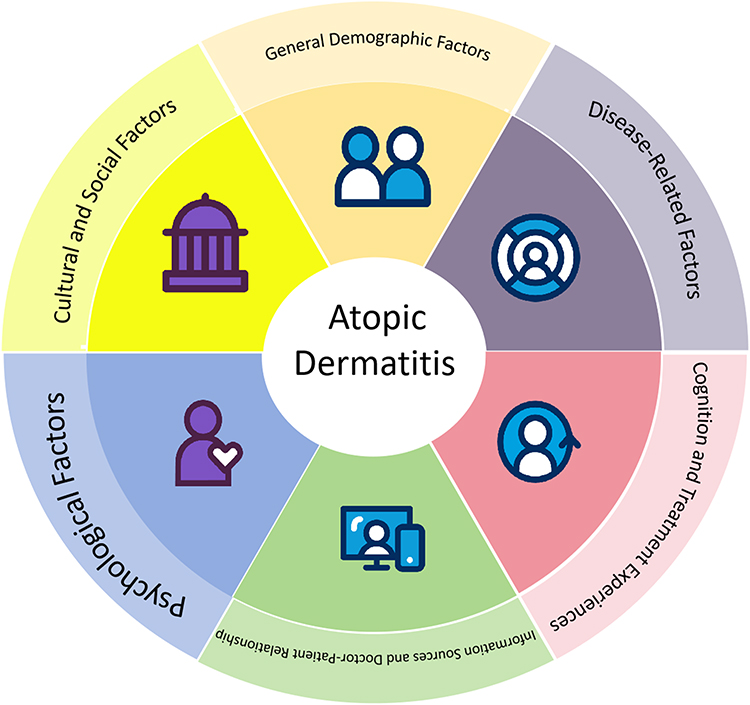 |
Figure 1 Factors influencing corticosteroid fear in patients with AD. |
General Demographic Factors
Studies indicate that fear of TCS among patients with AD demonstrates significant demographic variations, with influencing factors exhibiting multidimensional interactions. Regarding gender, female patients or caregivers exhibit significantly higher levels of TCS fear than males, prominently reflected in dimensions such as behavioral avoidance tendencies, fearful emotions, and TOPICOP global scores,28,29 suggesting that gender-specific differences may be associated with psychological cognitive variations in risk perception patterns and coping strategies. The relationship between age and TCS fear shows a consistent association: longitudinal study data indicate that TCS fear scores increase with patient age;18 This study observed that the elderly group had a lower rate of correct knowledge about TCS.30 Although the reasons for this difference may be multifaceted (such as educational background and channels of information acquisition), considering the potential impact of age-related cognitive decline on health decision-making,31,32 physiological cognitive impairment may be a noteworthy factor that could indirectly reinforce their irrational fear of medication.The impact of education level presents contradictory findings: while higher education groups demonstrate reduced TOPICOP scores through enhanced health information literacy,33,34 some studies indicate that this group develops a “knowledge paradox” due to excessive focus on medication risks, resulting in elevated fear scores compared to control groups.18 Furthermore, cross-cultural comparisons show that Asian patients score higher on TOPICOP dependency concern items than European patients, with a global score standard deviation reaching 18.7 points,22 potentially related to variations in pharmacist guidance coverage and stigmatization of corticosteroids across different regions globally. This evidence suggests that clinical practice requires establishing intervention systems with multidimensional assessment, implementing personalized fear management through cognitive restructuring, precise education, and culturally adapted strategies. Currently, the impact of factors like education level on TCS fear in AD patients has not reached a consistent conclusion and requires further investigation. Healthcare providers should maintain close attention to AD patients from multiple perspectives, engage in timely communication, and remain vigilant against the development of TCS fear.
Disease-Related Factors
Disease Severity
Disease severity exhibits a specific relationship with the presentation of corticosteroid phobia. A study by Kew CH et al11 demonstrated that patients with severe AD had a 1.8-fold higher incidence rate of fear toward TCS compared to those with mild-to-moderate AD. However, cross-sectional studies revealed no significant statistical association between the level of TCS fear and AD severity scores.35 Notably, the impact of disease severity on TCS adherence manifested as follows: pediatric patients with severe AD exhibited significantly higher medication adherence rates than mild-to-moderate groups.36 This discrepancy may be attributed to the heightened treatment demand driven by intense symptoms associated with severe cutaneous inflammation, while mild patients, due to concerns about corticosteroid side effects, are more prone to actively avoid medication use. This phenomenon suggests that AD-specific chronic skin barrier dysfunction and the “itch-scratch” cycle may indirectly modulate patients’ cognitive conflict regarding TCS through a dynamic interplay between symptom burden and therapeutic necessity.
Disease Duration
Disease duration plays a complex and dualistic role in shaping TCS phobia among patients with AD. Longitudinal cohort studies indicate that early-onset AD significantly increases the risk of TCS-related fear in adulthood,13 a mechanism potentially involving dual pathways. On one hand, repeated exposure to TCS treatment during infancy may foster negative therapeutic memories through abnormal cortisol fluctuations. On the other hand, parental misconceptions about hormonal safety may influence pediatric psychological development via a “vicarious fear transmission” model. A study involving 100 pediatric patients, which assessed parental fear levels using the TOPICOP questionnaire, identified early disease onset and prior healthcare experiences as critical risk factors for severe parental phobia through multivariate analysis.15 Such pharmacophobia may trigger persistent treatment resistance via a neuro-conditioning mechanism of “risk perception-avoidance behavior.” Once established, this resistance can be further reinforced through a “side effect-fear” negative feedback loop, solidifying patient avoidance behaviors. Notably, the chronic relapsing-remitting pattern characteristic of AD may induce dynamic shifts in TCS perception across different disease phases. During acute flares, intense symptom relief demands may transiently lower fear thresholds, enhancing treatment compliance.37 Conversely, in remission phases, negative memories (eg., steroid withdrawal reactions or TCS-associated cutaneous atrophy) can reignite fear, leading to renewed TCS avoidance. Thus, disease duration not only shapes initial TCS perceptions but also perpetuates long-term phobia through accumulated therapeutic experiences and adverse drug reactions. Given the disease-specific nature of AD, its clinical features and dynamic disease course collectively establish a TCS-phobia-driving framework. Clinical care interventions require tailored medication education strategies aligned with disease staging, severity, and duration. For long-term TCS users, rigorous AD monitoring and optimized alternative regimens are essential to disrupt the “disease burden-treatment fear” vicious cycle.
Cognition and Treatment Experiences
Perception of side effects and previous treatment experiences are significant contributors to corticosteroid phobia. Studies indicate that patients’ subjective experiences of adverse drug reactions markedly exacerbate their fear. A cross-sectional study by Chiricozzi et al9 confirmed that individuals with prior adverse events from corticosteroid use face a 362-fold increased risk of developing medication-related fears.Regarding side effect perceptions, findings by Katoh et al38 revealed that 83.6% of patients harbor multiple concerns, with skin atrophy, telangiectasia, and cataract risks emerging as predominant worries. Notably, pediatric patients exhibit distinct cognitive biases—research39 highlighted that caregivers predominantly focus on skin thinning risks and potential systemic absorption impacts on growth and development. Additionally, a study40 demonstrated that female participants scored significantly higher on TCS knowledge assessments than males, while participants with dermatological conditions provided more accurate responses. This suggests that enhancing patient understanding of TCS may alleviate fear. During treatment, perceived efficacy critically influences medication adherence. Research by Chu et al41 found that patients discontinue treatment due to perceived suboptimal efficacy or shorter duration of action than anticipated, underscoring that unsatisfactory therapeutic outcomes are a primary driver of corticosteroid refusal.
Information Sources and Doctor-Patient Relationship
The channels through which patients obtain TCS information and the credibility of these sources have a significant stratified effect on their fear levels.Notably, information pollution is particularly prominent in non-professional channels: social networks, traditional media, and anecdotal experiences from acquaintances have all been identified as independent risk factors for fear.42 Among these, 35% of patients developed persistent anxiety due to media reports exaggerating side effects.27 A study conducted in Malaysian healthcare institutions revealed43 that pharmacists face a triple dilemma when handling TCS consultations: ① patients’ pre-existing stigmatized perceptions of steroids; ② the conflict between irrational medication demands and TCS indications; ③ structural deficiencies in consultation support systems. This finding highlights the urgent need to enhance the precision and systematization of information delivery from the medical side.
The quality of the doctor-patient relationship exhibits a dose-response effect on corticosteroid phobia. Logistic regression analysis demonstrated41 that for every one-level decrease in a patient’s trust in their primary doctor, the probability of medication refusal increased by 2.3-fold. A longitudinal cohort study29 further found that patients who changed their healthcare institution three or more times per year had a 67% higher incidence of steroid phobia compared to those with consistent care providers, suggesting the potential value of continuous care in alleviating medication fear. This “trust deficit” phenomenon may be related to cognitive biases arising from disrupted continuity of care, manifesting as patients’ systematic skepticism toward treatment plans and diminished information integration capacity.
Implications for nursing practice: It is crucial to closely monitor the psychological dynamics of highly mobile patients and to strengthen the stability of the therapeutic alliance by constructing an intervention framework that integrates “knowledge-trust-behavior” into a unified whole.
Psychological Factors
Psychological factors play a significant role in the development and progression of TCS fear among AD patients. Studies indicate that individual psychological characteristics significantly influence the formation of TCS fear, with individuals exhibiting low symptom tolerance being more prone to developing fear of TCS. Furthermore, psychological dependency and a need for reassurance have been confirmed to be positively correlated with TCS fear.15 Notably, negative emotions such as anxiety and depression may exacerbate patients’ concerns regarding TCS fear through neuroendocrine mechanisms. A Vietnamese cross-sectional study involving 208 AD patients revealed41 that 11.1% of patients had anxiety symptoms, 5.3% had comorbid depressive disorders, and 1.44% presented with a mixed anxiety-depressive state. Further analysis found that the levels of anxiety and depression in AD patients were significantly correlated with itch intensity and the frequency of sleep disturbances. The persistence of negative psychological states may exacerbate TCS fear in AD patients through multiple pathways: on one hand, anxiety can heighten patients’ excessive focus on drug side effects, forming cognitive biases; on the other hand, depressive symptoms may lead to decreased treatment adherence, further reinforcing negative expectations towards TCS. Clinical observations indicate44 that sustained psychological stress can activate the hypothalamic-pituitary-adrenal (HPA) axis, causing abnormal fluctuations in cortisol levels, and this physiological stress response may amplify patients’ sensitivity to TCS. Notably, the interaction between catastrophic thinking about disease prognosis and somatic symptoms (such as skin burning or stinging sensations) may create a vicious cycle of “symptoms-anxiety-fear.” This highlights the need for healthcare professionals to establish a multidimensional psychological assessment system and implement targeted interventions addressing patients’ cognitive biases and emotional disorders.
Cultural and Social Factors
Research demonstrates that TCS phobia in AD patients exhibits multidimensional differences across countries and regions, shaped by cultural cognitive frameworks, healthcare system characteristics, and information dissemination pathways. An international multicenter study22 utilizing the TOPICOP scale revealed significant geographic specificity in total and subdomain scores, indicating transnational heterogeneity in TCS phobia drivers. This disparity stems from dual mechanisms: cultural backgrounds influence medication decisions by shaping risk perception patterns (eg., stigmatization of “hormonal drugs”),45 while insufficient evidence-based education in healthcare systems exacerbates cognitive biases.46,47 In some countries, inadequate medication literacy coverage in primary healthcare institutions forces patients to rely excessively on non-professional information sources.48,49
An empirical study10 involving 1507 adult AD patients and 525 child caregivers from different cultural backgrounds further clarified the influence of culture on TCS phobia.The TOPICOP score for adults was 42.5 ± 18.9, and the score for caregivers was 41.7 ± 18.69, providing empirical support for the prevalence of TCS fear. Notably, this study revealed high synchronization of cognitive biases between patients and caregivers—a phenomenon potentially rooted in transcultural societal preoccupations with “medication dependency” and risk communication disparities in multicultural clinical interactions, reflecting how “protective anxiety” within transcultural family-focused healthcare models inhibits treatment adherence.12 These findings suggest that TCS phobia severity may vary across cultural contexts.
Thus, establishing a culturally sensitive TCS phobia assessment framework, developing standardized cross-cultural risk communication guidelines, and improving medication literacy correction systems in healthcare are critical for eliminating TCS utilization barriers and optimizing chronic dermatological management.
Nursing Strategies for Corticosteroid Phobia in Patients with Atopic Dermatitis
In response to the phenomenon of corticosteroid phobia among patients with AD, healthcare professionals have explored multidimensional nursing strategies. Through stepwise medication education—aligned with the graded treatment principles outlined in the Chinese Guidelines for the Diagnosis and Management of Atopic Dermatitis—a full-cycle management approach has been established, spanning from standardized drug use to psychological support. Clinical practice has demonstrated that this comprehensive nursing model not only ensures treatment adherence but also reduces patients’ resistance to corticosteroids, significantly improving long-term disease management outcomes.
Enhancing Patient Education
The care of patients with corticosteroid phobia should prioritize enhanced patient education. Studies have demonstrated that educational interventions are effective in reducing corticosteroid phobia, as patients’ fears often stem from misconceptions about drug safety and side effects.13 A randomized controlled trial conducted by Choi et al50 revealed that targeted educational interventions significantly reduced patients’ TOPICOP scores. The mean TOPICOP score in the intervention group decreased from 41.9 at baseline to 37.1 at 1 month and 33.8 at 3 months, with improvements primarily observed in the knowledge domain rather than the fear and behavior domains. Evidence indicates51 that multimodal educational approaches—including instructional videos, personalized verbal counseling addressing specific patient concerns, and practical demonstrations of corticosteroid application—effectively improve patients’ competency in proper corticosteroid use. Such comprehensive strategies enhance patients’ understanding of corticosteroid mechanisms, correct usage, and potential risks, thereby mitigating unwarranted fears.
Furthermore, educational interventions targeting pharmacists combined with patient-centered consultations have proven effective in alleviating corticosteroid phobia. Data from one study showed that after a 3-month intervention, the TOPICOP scores of caregivers significantly decreased from 42 to 35, while pharmacists’ scores on the same scale declined from 33 to 25.52 These findings underscore the necessity for ongoing corticosteroid education not only for patients but also for healthcare professionals to optimize patient guidance and support.
Multiple studies emphasize the critical role of education in reducing corticosteroid phobia.52 Educational content should encompass proper corticosteroid administration techniques, potential side effects, and their management. Personalized verbal counseling tailored to individual patient concerns, paired with practical demonstrations of corticosteroid use, has been validated as an effective intervention.13 Healthcare providers should implement corticosteroid phobia screening, particularly in high-risk populations. Collectively, these findings highlight that integrating structured health education into the care of AD patients can substantially reduce the risk of corticosteroid phobia.
Provision of Accurate Information Sources
Studies have found that patients access information about corticosteroids from diverse sources, including physicians, friends and relatives, broadcast media, print media, and the internet.13 Multiple studies consistently indicate that healthcare professionals, particularly dermatologists and nurses, are the most reliable and trusted sources for obtaining corticosteroid-related information.11 However, the quality and accuracy of information from different sources may vary. Research shows that 35% of patients reported their corticosteroid phobia originated from information obtained through media.27 To mitigate the impact of misleading information, healthcare providers should proactively provide reliable information sources, such as the official websites of authoritative medical institutions or professionally reviewed patient education materials; encourage patients to prioritize obtaining information from healthcare professionals. The study indicates that individuals who acquired information on corticosteroid use from healthcare professionals were less likely to develop corticosteroid phobia;53 and guide patients on how to identify credible information online and avoid being misled by unsubstantiated claims.
Tailored Care Protocols
Given the multifactorial nature of corticosteroid phobia, healthcare providers should develop individualized care protocols based on patients’ specific circumstances. Studies indicate that corticosteroid phobia correlates with multiple factors, including gender, educational attainment, and disease severity.16,54 A study involving parents of children with AD identified disease severity and knowledge of potential adverse events as significant risk factors for corticosteroid phobia.55 Consequently, care protocols should incorporate the following considerations: a) disease severity; b) patients’ understanding of corticosteroids; c) educational background; d) age and gender; and e) cultural context and beliefs. By addressing these factors, clinicians can systematically target patients’ unique concerns and deliver more effective support.
Improving Doctor-Patient Communication
Effective doctor-patient communication is crucial for reducing corticosteroid fear. Studies show that physicians may overestimate patients’ concerns about using corticosteroids.56 This cognitive discrepancy may lead physicians to be overly cautious when prescribing corticosteroids, thereby exacerbating patients’ fear. To improve doctor-patient communication, nursing staff should in the future more actively encourage patients to express their concerns and questions about corticosteroids, listen patiently to patients’ worries, and provide detailed, understandable explanations, using visual aids to explain the mechanism of action and correct usage of corticosteroids, and regularly assess patients’ fear levels using the TOPICOP scale to timely adjust communication strategies.
Psychological Nursing
Corticosteroid fear is not only a medical issue but also involves psychological dimensions. Research indicates that psychological counseling and support can provide substantial help in managing corticosteroid fear; considering that corticosteroid fear may lead to anxiety and depression, offering psychological support is an important component of nursing care.57,58 Nursing staff should provide emotional support, help patients alleviate anxiety and fear, teach stress management techniques such as relaxation training or mindfulness meditation, assist patients in coping with treatment-related stress, and, when necessary, refer to mental health professionals to deliver more professional psychological support.
Monitoring and Follow-Up
Continuous monitoring and follow-up are crucial for managing corticosteroid phobia, as research demonstrates that through 20 months of sustained follow-up, patients’ symptoms improved with no related complications observed.59 Studies indicate that as corticosteroid phobia increases, treatment adherence significantly decreases.52 Therefore, nursing interventions should prioritize enhancing patients’ treatment adherence through regular follow-ups and implementing continuous care to strengthen disease management capabilities of both patients and their families. Healthcare professionals should regularly assess patients’ fear levels and treatment adherence, closely monitor therapeutic effects and potential side effects, and provide timely feedback to patients to bolster their confidence in treatment. Educational and support strategies should be adjusted according to patients’ responses, while encouraging patients to maintain records of symptoms and medication usage to facilitate better evaluation of treatment outcomes.
Summary and Outlook
AD is a chronic and relapsing disease for which there is currently no cure, with disease outcomes being highly correlated with TCS usage; investigating the issue of TCS fear among caregivers is of significant practical importance for advancing the disease management of pediatric AD patients. The widespread phenomenon of TCS fear among AD patients and their guardians has become a major barrier affecting treatment adherence and disease control efficacy. This irrational medication avoidance behavior not only increases the risk of disease recurrence but may also lead to complications such as secondary infections, imposing a dual physical and psychological burden on both patients and their families. This article systematically reviews the current status and influencing factors of TCS fear in AD patients and summarizes evidence-based hierarchical intervention strategies to provide a theoretical reference for developing precise clinical nursing plans. Healthcare professionals need to establish a patient-centered communication model and deliver differentiated medication guidance tailored to patients and guardians with varying educational levels. Notably, the anxiety and decision-making conflicts experienced by guardians of pediatric patients present unique challenges, necessitating the development of specialized psychological support programs for families of children with AD. Currently, research on the development of quantitative assessment tools for TCS fear and long-term intervention outcomes remains insufficient in domestic settings. This review highlights the global clinical significance of corticosteroid phobia in AD management, transcending geographical and cultural boundaries.Future research should focus on the following directions: first, establishing a multidimensional fear assessment indicator system and developing dynamic monitoring tools integrated with artificial intelligence technology; second, conducting cross-regional cultural comparison studies to reveal phenotypic differences in TCS fear across different healthcare environments; and third, constructing a multidisciplinary collaborative intervention pathway involving “physicians, nurses, pharmacists, and psychologists.” Through innovation in both theory and practice, the ultimate goal is to achieve dual improvements in treatment benefits and quality of life for AD patients.
Author Contributions
All authors made significant contributions to the work reported, whether in conception, research design, execution, analysis, and interpretation, or in all of these aspects; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal for submission; and agreed to take responsibility for all aspects of the work.
Funding
This study did not receive any external funding.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109–11. doi:10.1016/S0140-6736(15)00149-X
2. GBD. 2021 Asthma and Allergic Diseases Collaborators. Global, regional, and national burden of asthma and atopic dermatitis, 1990–2021, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Respir Med. 2025;13(5):425–446. doi:10.1016/S2213-2600(25)00003-7.
3. Tian J, Zhang D, Yang Y, et al. Global epidemiology of atopic dermatitis: a comprehensive systematic analysis and modelling study. Br J Dermatol. 2023;190(1):55–61. doi:10.1093/bjd/ljad339
4. Shin YH, Hwang J, Kwon R, et al. Global, regional, and national burden of allergic disorders and their risk factors in 204 countries and territories, from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Allergy. 2023;78(8):2232–2254. doi:10.1111/all.15807
5. Meledathu S, Naidu MP, Brunner PM. Update on atopic dermatitis. J Allergy Clin Immunol. 2025;155(4):1124–1132. doi:10.1016/j.jaci.2025.01.0135
6. Guttman-Yassky E, Renert-Yuval Y, Brunner PM. Atopic dermatitis. Lancet. 2025;405(10478):583–596. doi:10.1016/S0140-6736(24)02519-4
7. Dharmage SC, Lowe AJ, Matheson MC, Burgess JA, Allen KJ, Abramson MJ. Atopic dermatitis and the atopic march revisited. Allergy. 2014;69(1):17–27. doi:10.1111/all.12268
8. Hatano Y, Elias PM. “Outside-to-inside,” “inside-to-outside,” and “intrinsic” endogenous pathogenic mechanisms in atopic dermatitis: keratinocytes as the key functional cells involved in both permeability barrier dysfunction and immunological alterations. Front Immunol. 2023;14:1239251. doi:10.3389/fimmu.2023.1239251
9. Chiricozzi A, Comberiati P, D’Auria E, Zuccotti G, Peroni DG. Topical corticosteroids for pediatric atopic dermatitis: thoughtful tips for practice. Pharmacol Res. 2020;158:104878. doi:10.1016/j.phrs.2020.104878
10. Gooderham MJ, Hong HCH, Lynde C, et al. Canadian Consensus Guidelines for the Management of Atopic Dermatitis with Topical Therapies. Dermatol Ther. 2025;15(6):1467–1485. doi:10.1007/s13555-025-01386-2
11. Kew CH, Ahmad Basir KF, Low DW, Loh KC. Breaking through the steroid stigma: a single-centre study on topical corticosteroid perception and adherence in dermatology patients and caregivers. Med J Malaysia. 2023;78(4):437–444.
12. Nakahara T, Murota H, Noto S, et al. Observational Study of Corticosteroid Phobia Using the TOPICOP Score among Adults and Caregivers of Children with Atopic Dermatitis in Japan. Dermatol Ther. 2025;15(7):1851–1865. doi:10.1007/s13555-025-01439-6
13. Rajagopalan M, Chitkara AJ, Dalwai S, et al. Burden of Disease, Unmet Needs in the Diagnosis and Management of Atopic Dermatitis: an Indian Expert Consensus. Clin Cosmet Invest Dermatol. 2021;14:1755–1765. doi:10.2147/CCID.S327593
14. Chan TC, Wu NL, Wong LS, et al. Taiwanese Dermatological Association consensus for the management of atopic dermatitis: a 2020 update. J Formos Med Assoc. 2021;120(1 Pt 2):429–442. doi:10.1016/j.jfma.2020.06.008
15. Herzum A, Occella C, Gariazzo L, Pastorino C, Viglizzo G. Corticophobia among Parents of Children with Atopic Dermatitis: assessing Major and Minor Risk Factors for High TOPICOP Scores. J Clin Med. 2023;12(21):6813. doi:10.3390/jcm12216813
16. Lin W, Wang Q, Liu J, Tan Q. Corticosteroid Phobia: a Key Barrier to Treatment in Young Women with Idiopathic Granulomatous Mastitis. Int J Womens Health. 2025;17:167–177. doi:10.2147/IJWH.S500846
17. Tangthanapalakul A, Chantawarangul K, Wananukul S, Tempark T, Chatproedprai S. Topical corticosteroid phobia in adolescents with eczema and caregivers of children and adolescents with eczema: a cross-sectional survey. Pediatr Dermatol. 2023;40(1):135–138. doi:10.1111/pde.15183
18. Barakat M, Abdulrazzaq SB, Alzaghari LF, Ramatillah D, Muhammad RF, Elnaem MH. Assessment of Knowledge, Perception, Experience, and Phobia Toward Corticosteroids Among the General Public in Two Southeast Asian Countries. Inquiry. 2025;62:469580251333968. doi:10.1177/00469580251333968
19. Alakeel A, Al Sheikh A, Alraddadi AA, et al. Management of Atopic Dermatitis in Adults in Saudi Arabia: consensus Recommendations from the Dermatological Expert Group. Clin Cosmet Invest Dermatol. 2022;15:1435–1445. doi:10.2147/CCID.S357178
20. Li Z, Mai X, Liao Y, et al. Exploring Treatment Adherence in Children Aged 0–6 With Atopic Dermatitis: a Pilot Cross-Sectional Study in China. Pediatr Dermatol. 2025;42(4):760–766. doi:10.1111/pde.15968
21. Magboul MA, Fadel HA, Al-Johani AG, et al. Topical corticosteroid phobia among the general population in the western region of Saudi Arabia. J Family Med Prim Care. 2025;14(3):1085–1090. doi:10.4103/jfmpc.jfmpc_1355_24
22. Stalder JF, Aubert H, Anthoine E, et al. Topical corticosteroid phobia in atopic dermatitis: international feasibility study of the TOPICOP score. Allergy. 2017;72(11):1713–1719. doi:10.1111/all.13189
23. Starbek Zorko M, Benko M, Rakuša M, Prunk Zdravković T. Evaluation of corticophobia in patients with atopic dermatitis and psoriasis using the TOPICOP© score. Acta Dermatovenerol Alp Pannonica Adriat. 2023;32(4):135–139.
24. Li AW, Yin ES, Antaya RJ. Topical Corticosteroid Phobia in Atopic Dermatitis: a Systematic Review. JAMA Dermatol. 2017;153(10):1036–1042. doi:10.1001/jamadermatol.2017.2437
25. Bos B, Antonescu I, Osinga H, Veenje S, de Jong K, de Vries TW. Corticosteroid phobia (corticophobia) in parents of young children with atopic dermatitis and their health care providers. Pediatr Dermatol. 2019;36(1):100–104. doi:10.1111/pde.13698
26. Gustavsen HE, Gjersvik P. Topical corticosteroid phobia among parents of children with atopic dermatitis in a semirural area of Norway. J Eur Acad Dermatol Venereol. 2016;30(1):168. doi:10.1111/jdv.12670
27. Masood S, Jalil P, Awan S, Ghulam U, Kerawala SR. Assessment of topical steroid phobia in dermatology patients, a cross-sectional study from an urban area of Pakistan. J DermatolTreat. 2022;33(4):2331–2334. doi:10.1080/09546634.2021.1959505
28. Choi E, Chandran NS, Tan C. Corticosteroid phobia: a questionnaire study using TOPICOP score. Singapore Med J. 2020;61(3):149–153. doi:10.11622/smedj.2019110
29. Contento M, Cline A, Russo M. Steroid Phobia: a Review of Prevalence, Risk Factors, and Interventions. Am J Clin Dermatol. 2021;22(6):837–851. doi:10.1007/s40257-021-00623-6
30. Alamri RA, Al Satti HS. Knowledge and Attitudes Towards Topical Corticosteroids Among Previous Users in the General Population of Saudi Arabia. Cureus. 2024;16(3):e55373. doi:10.7759/cureus.55373
31. Rafhi E, Stupans I, Stevens JE, Soo Park J, Wang KN. The influence of beliefs and health literacy on medication-related outcomes in older adults: a cross-sectional study. Res Social Adm Pharm. 2025;21(1):47–55. doi:10.1016/j.sapharm.2024.10.003
32. Chow BC, Jiao J, Duong TV, et al. Health literacy mediates the relationships of cognitive and physical functions with health-related quality of life in older adults. Front Public Health. 2024;12:1355392. doi:10.3389/fpubh.2024.1355392
33. Jaworek A, Szafraniec K, Pastuszczak M, Zalewski A, Wojas-Pelc A. The knowledge of issues associated with topical corticosteroids using in patients with atopic dermatitis. Pol Merkur Lekarski. 2019;46(276):243–247.
34. Gerner T, Haugaard JH, Vestergaard C, et al. Healthcare utilization in Danish children with atopic dermatitis and parental topical corticosteroid phobia. Pediatr Allergy Immunol. 2021;32(2):331–341. doi:10.1111/pai.13394
35. Gomes TF, Kieselova K, Guiote V, Henrique M, Santiago F. A low level of health literacy is a predictor of corticophobia in atopic dermatitis. An Bras Dermatol. 2022;97(6):704–709. doi:10.1016/j.abd.2021.11.007
36. Liew ELF, Mohamed Shah N, Chong WW, Selvarajah L, Sulaiman US, Ponnuthurai N. Predictors of Topical Corticosteroid Adherence Among Caregivers of Children with Atopic Eczema. Patient Prefer Adherence. 2025;19:1593–1601. doi:10.2147/PPA.S498527
37. Wollenberg A, Christen-Zäch S, Taieb A, et al. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol. 2020;34(12):2717–2744. doi:10.1111/jdv.16892
38. Katoh N, Ohya Y, Ikeda M, et al. Japanese guidelines for atopic dermatitis 2020. Allergol Int. 2020;69(3):356–369. doi:10.1016/j.alit.2020.02.006
39. Wilson F, Harnik E, Gore C. A labelling system improves parental comfort and willingness to use topical corticosteroids for paediatric atopic dermatitis. Skin Health Dis. 2020;1(1):e11. doi:10.1002/ski2.11
40. Nie Z, Fan P, Zhou Y, Han S. Knowledge, attitudes, and practices in adult patients and parents of pediatric atopic dermatitis patients: a cross-sectional study. Front Public Health. 2024;12:1460044. doi:10.3389/fpubh.2024.1460044
41. AAAAI/ACAAI JTF Atopic Dermatitis Guideline Panel, Chu DK, Schneider L. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE- and Institute of Medicine-based recommendations. Ann Allergy Asthma Immunol. 2024;132(3):274–312. doi:10.1016/j.anai.2023.11.009.
42. Nickles MA, Coale AT, Henderson WJA, Brown KE, Morrell DS, Nieman EL. Steroid phobia on social media platforms. Pediatr Dermatol. 2023;40(3):479–482. doi:10.1111/pde.15269
43. Nathan AD, Shankar PR, Sreeramareddy CT. Topical corticosteroid counselling among Malaysian community pharmacists: a qualitative interview study. BMC Prim Care. 2023;24(1):119. doi:10.1186/s12875-023-02071-z
44. Lightman SL, Birnie MT, Conway-Campbell BL. Dynamics of ACTH and Cortisol Secretion and Implications for Disease. Endocr Rev. 2020;41(3):bnaa002. doi:10.1210/endrev/bnaa002
45. Phan S, Hajek A, Rangel SM, et al. Stigma underlies the mental health burden of pediatric atopic dermatitis: a cohort study. J Am Acad Dermatol. 2025;92(5):1088–1091. doi:10.1016/j.jaad.2024.12.032
46. Setia S, Loo E, Shinde SP, Singh M, Wong CH, Thakkar K. Redefining the Role of Medical Affairs Professionals as Innovators and Leaders in Industry-Led Medical Education. Pharmaceut Med. 2024;38(3):167–177. doi:10.1007/s40290-024-00522-1
47. Cheng Y, Shao W, Li L, Ding Y, Zou X. Effects of Interactive Health Education Combined With Evidence-based Pain Management Nursing on Disease Cognition, Postoperative Pain and Post-traumatic Growth in Patients Undergoing Laparoscopic Salpingectomy. Ann Ital Chir. 2025;96(5):664–672. doi:10.62713/aic.3945
48. Luo W, Liu J, Yang H, Qiu W, Huang J, Liu X. Stratified patterns of healthcare-seeking behavior among older adults in Fujian, China: exploring the behavioral foundations of health inequality. BMC Health Serv Res. 2025;26(1):113. doi:10.1186/s12913-025-13882-4
49. Frey E, Bonfiglioli C, Frawley J. Parents’ Use of Social Media for Health Information Before and After a Consultation With Health Care Professionals: australian Cross-Sectional Study. JMIR Pediatr Parent. 2023;6:e48012. doi:10.2196/48012
50. Choi E, Tan KW, Tang F, Tan C, Chandran NS. Efficacy of targeted education in reducing topical steroid phobia: a randomized clinical trial. J Am Acad Dermatol. 2020;83(6):1681–1687. doi:10.1016/j.jaad.2020.02.079
51. Brunner C, Schlüer AB, Znoj H, et al. Video-Based Education with Storytelling Reduces Parents’ Fear of Topical Corticosteroid Use in Children with Atopic Dermatitis: a Randomized Controlled Trial (The EduDerm Study Part II). Adv Skin Wound Care. 2023;36(8):414–419. doi:10.1097/ASW.0000000000000002
52. Koster ES, Philbert D, Zheng X, Moradi N, de Vries TW, Bouvy ML. Reducing corticosteroid phobia in pharmacy staff and parents of children with atopic dermatitis. Int J Clin Pharm. 2021;43(5):1237–1244. doi:10.1007/s11096-021-01241-2
53. Delpero E, Sriharan A, Selk A. Steroid Phobia in Patients With Vulvar Lichen Sclerosus. J Low Genit Tract Dis. 2023;27(3):286–290. doi:10.1097/LGT.0000000000000753
54. Christensen MO, Sieborg J, Nymand LK, et al. Prevalence and clinical impact of topical corticosteroid phobia among patients with chronic hand eczema-Findings from the Danish Skin Cohort. J Am Acad Dermatol. 2024;91(6):1094–1103. doi:10.1016/j.jaad.2024.07.1503
55. Lee JY, Her Y, Kim CW, Kim SS. Topical Corticosteroid Phobia among Parents of Children with Atopic Eczema in Korea. Ann Dermatol. 2015;27(5):499–506. doi:10.5021/ad.2015.27.5.499
56. Johnson Girard V, Hill A, Glaser E, Lussier MT. Optimizing Communication About Topical Corticosteroids: a Quality Improvement Study. J Cutan Med Surg. 2020;24(3):240–248. doi:10.1177/1203475420908250
57. Barbarot S, Aubert H, Vibet MA, et al. Effectiveness of a nurse-led one-to-one education programme in addition to standard care in children with atopic dermatitis: a multicentre randomized control trial. Br J Dermatol. 2024;191(2):177–186. doi:10.1093/bjd/ljae111
58. LeBovidge JS, Schneider LC. Depression and anxiety in patients with atopic dermatitis: recognizing and addressing mental health burden. Ann Allergy Asthma Immunol. 2025;134(5):506–515. doi:10.1016/j.anai.2025.02.017
59. Yew YW, Alagappan U, Aw D, et al. Updated consensus guidelines for management of moderate-to-severe atopic dermatitis in Singapore: integrating biologics, Janus kinase inhibitors and conventional therapies. Ann Acad Med Singap. 2024;53(11):670–682. doi:10.47102/annals-acadmedsg.2024158
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.