Back to Journals » Clinical Interventions in Aging » Volume 21
Correlation of Cerebral Oxygen Saturation Change with Perioperative Complications in Elderly Patients Who Underwent Laparoscopic Partial Hepatectomy
Received 20 June 2025
Accepted for publication 28 December 2025
Published 9 January 2026 Volume 2026:21 548590
DOI https://doi.org/10.2147/CIA.S548590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Ting Li,1 Rennan Guo,2 Guiping Xu1
1Department of Anesthesiology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, People’s Republic of China; 2Department of Critical Care Medicine, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, People’s Republic of China
Correspondence: Guiping Xu, Department of Anesthesiology, People’s Hospital of Xinjiang Uygur Autonomous Region, No. 91 Tianchi Road, Urumqi, Xinjiang Uygur Autonomous Region, 830001, People’s Republic of China, Tel +86-13669948036, Email [email protected]
Background: Laparoscopic partial hepatectomy is a crucial treatment for primary liver cancer but is associated with risks such as bleeding and organ hypoperfusion due to controlled low central venous pressure (CLCVP). Regional cerebral oxygen saturation (rSO2), measured using near-infrared spectroscopy (NIRS), serves as a reliable indicator of cerebral perfusion. This study aims to investigate the relationship between intraoperative rSO2 changes, perioperative outcomes, and neurological complications.
Methods: This retrospective study analyzed 218 elderly patients undergoing laparoscopic partial hepatectomy, grouped based on intraoperative rSO2 reductions of ≥ 10% and ≥ 20%. Perioperative complications were assessed. Serum neuron-specific enolase (NSE) levels were measured on postoperative day 3 via enzyme-linked immunosorbent assay. Hemodynamic parameters, including mean arterial pressure (MAP), were monitored intraoperatively.
Results: Among the 218 patients, significant rSO2 reductions were linked to higher risks of neurological complications. Patients with ≥ 20% rSO2 reductions had increased incidences of delirium (30.5% vs 13.0%, p = 0.002), and elevated serum NSE levels (p < 0.05). Declines in MAP during critical intraoperative periods were associated with rSO2 reductions. Patients with marked rSO2 drops also experienced prolonged hospital stays.
Conclusion: Intraoperative rSO2 reductions, especially > 20%, are linked to adverse neurological outcomes and delayed recovery. Combined rSO2 and NSE monitoring offers a robust strategy to optimize cerebral perfusion and improve outcomes.
Keywords: perioperative complications NSE, rSO2, cerebral perfusion, outcome
Introduction
Primary liver cancer is the sixth most common cancer globally, with China accounting for over half of the global liver cancer burden, making it one of the countries with the highest liver cancer incidence and mortality rates.1 Surgical resection remains the most effective curative treatment for liver cancer.2 However, laparoscopic liver resection poses significant challenges due to factors such as liver stiffness, reduced compliance, coagulopathy, and collateral circulation in the abdominal cavity, all of which increase the risk of intraoperative bleeding. Minimizing intraoperative blood loss and improving the surgical field have become key focuses for anesthesiologists managing these procedures.3,4
Controlled low central venous pressure (CLCVP) has been widely adopted in clinical practice to reduce blood loss and improve the surgical field during liver surgeries.5 This technique involves restricting central venous pressure (CVP) to below 5 mm Hg6 while maintaining adequate cardiac output and arterial blood pressure using measures such as restrictive fluid management, appropriate anesthetic depth, vasopressors, and patient positioning.7,8 Despite its benefits, CLCVP can lead to hypoperfusion of critical organs, including the brain, kidneys, and heart, resulting in perioperative complications. Brain oxygen saturation (rSO2) monitoring, as demonstrated by several studies, provides a reliable and non-invasive method to assess cerebral perfusion levels during surgery.9,10
Previous research has primarily focused on the general benefits of CLCVP in reducing intraoperative bleeding and improving the surgical field, but the broader implications of this technique on systemic and organ-specific perfusion have been less explored.11 Many studies have reported adverse events associated with CLCVP, such as transient hypotension and decreased cerebral perfusion, but these studies often lack comprehensive assessments of neurological outcomes, such as postoperative delirium and cognitive dysfunction.12–14 Moreover, most studies rely on subjective clinical observations or crude markers, such as arterial blood pressure, to infer organ perfusion, which may not accurately reflect dynamic changes in cerebral oxygenation.15
Existing clinical tools for monitoring cerebral oxygenation, including near-infrared spectroscopy (NIRS)-based rSO2 monitoring, have demonstrated promise in providing real-time, non-invasive insights into cerebral perfusion.16 However, the application of rSO2 monitoring in liver surgeries, especially in elderly patients undergoing laparoscopic procedures, remains underutilized. While rSO2 monitoring can detect intraoperative cerebral desaturation events (CDEs), its correlation with neurological and systemic outcomes, such as postoperative delirium and cognitive dysfunction, is not yet fully understood.17 Additionally, biomarkers like neuron-specific enolase (NSE), which reflect neuronal injury, have rarely been integrated with rSO2 monitoring to provide a more comprehensive assessment of brain health during and after surgery.18,19
There is an unmet need to bridge these gaps in understanding the broader implications of CLCVP on cerebral oxygenation and neurological outcomes. A comprehensive approach that combines real-time rSO2 monitoring with biochemical markers, such as NSE, could provide deeper insights into the pathophysiology of brain hypoperfusion and its consequences in elderly surgical patients.20 Furthermore, evaluating rSO2 thresholds and their relationship with postoperative complications could lead to more precise perioperative management strategies to mitigate risks and improve recovery.21
The aim of this study was to investigate the association between intraoperative changes in rSO2 and perioperative outcomes in elderly patients undergoing laparoscopic partial hepatectomy.
Methods
Inclusion and Exclusion Criteria
The study was approved by the People’s Hospital of Xinjiang Uygur Autonomous Region, and informed written consent was obtained from all the analyzed patients. This study included elderly patients undergoing elective laparoscopic partial hepatectomy. The inclusion criteria were patients aged 60 years or older, classified as ASA II or III, with Child-Pugh liver function grades A or B. Patients were excluded if they had severe dysfunction of critical organs such as the heart or lungs, a history of cerebrovascular disease, significant coagulopathy, or neurological/psychiatric disorders. Additionally, patients with a preoperative Mini-Mental State Examination (MMSE) score below 24 or those unable to communicate normally were excluded from the study.
Controlled Low Central Venous Pressure (CLCVP) Protocol
All patients underwent controlled low central venous pressure (CLCVP), which was defined as maintaining central venous pressure (CVP) at 0–5 mm Hg while ensuring systolic arterial pressure remained at or above 90 mmHg or mean arterial pressure (MAP) at or above 60 mmHg. Various techniques were utilized to achieve and maintain this pressure range during surgery.
Anesthesia Protocol
After admission, standard monitoring, including electrocardiography (ECG), heart rate (HR), and peripheral arterial oxygen saturation (SpO2), was initiated. Patients were warmed using a thermal warming system, and nasopharyngeal temperature along with neurophysiological function were monitored. Radial artery cannulation was performed under local anesthesia for invasive blood pressure monitoring, and both peripheral and central venous access was established. Prior to anesthesia induction, all patients underwent radial artery cannulation for continuous invasive arterial blood pressure (IABP) monitoring, ensuring real-time hemodynamic assessment throughout the peri-induction and intraoperative period; this also enabled calculation of dynamic parameters such as stroke volume variation (SVV) and pulse pressure variation (PPV) for fluid management.
Local infiltration anesthesia was administered as part of multimodal analgesia and perioperative support exclusively at trocar insertion sites. The primary trocar at the umbilical region (used for laparoscopic camera access) received layered infiltration anesthesia targeting the skin, subcutaneous tissue, and anterior rectus sheath within a 2–3 cm radius of the incision. Additional 3–4 auxiliary ports (5–10 mm in diameter) were anesthetized similarly in a layer-by-layer manner (skin → subcutaneous → fascial layers). Ropivacaine was used for all infiltration procedures, with total dosage strictly limited to ≤2 mg/kg to prevent local anesthetic systemic toxicity. Anesthesia induction was achieved with sequential intravenous administration of midazolam (0.03 mg/kg), propofol (1.5–2.5 mg/kg), sufentanil (0.4–0.5 μg/kg), and cisatracurium besylate (0.15–0.2 mg/kg). Following successful tracheal intubation, mechanical ventilation was initiated with tidal volumes of 8–10 mL/kg, a respiratory rate of 10–14 breaths/min, a flow rate of 2 L/min, and an oxygen concentration of 60%. End-tidal carbon dioxide pressure was maintained at 35–40 mmHg, and the bispectral index (BIS) was targeted between 40 and 60. Before the surgical incision, 10–15 mL of 0.5% ropivacaine was administered for local infiltration. Anesthesia was maintained using intermittent doses of cisatracurium, sevoflurane inhalation, and remifentanil infusion. At the end of the surgery, anesthesia was discontinued, sevoflurane was flushed with an oxygen flow rate of 8 L/min, and residual neuromuscular blockade was reversed using neostigmine and atropine. All patients adhered to the CLCVP protocol during the surgery.
During anesthesia maintenance, sevoflurane concentration was maintained between 1.0–2.0%, titrated to achieve a BIS range of 40–60. The concentration was adjusted by 0.2–0.3% if BIS deviated outside this range. Remifentanil was continuously infused at 0.1–0.3 µg·kg−1·min−1 using a microinfusion pump, starting at 0.1 µg·kg−1·min−1. The total daily dosage did not exceed 10 µg/kg. Neostigmine was administered at 0.02–0.03 mg/kg (maximum 2.5 mg), combined with atropine in a 1:2 fixed ratio (0.01–0.015 mg/kg, maximum 1.2 mg). Both drugs were mixed, diluted with 5–10 mL saline, and slowly injected over 2–3 minutes. Quantitative neuromuscular monitoring guided reversal, and no empirical dosing was applied.
Postoperative Assessments
On postoperative day 3, all patients underwent assessments for delirium and postoperative cognitive dysfunction (POCD). Delirium was evaluated using the Confusion Assessment Method (CAM), which includes acute onset of mental status changes, inattention, disorganized thinking, and altered levels of consciousness. A diagnosis of delirium was made if the patient met the criteria for either acute onset and inattention plus disorganized thinking, or acute onset and inattention plus altered consciousness.
POCD was assessed using the MMSE, which evaluates five cognitive domains: recall, language, memory, calculation, and orientation. Scores ranged from 0 to 30, with higher scores indicating better cognitive function. To account for diurnal variations, all evaluations were conducted by the same physician between 20:00 and 21:00. A decline of at least one standard deviation (SD) in MMSE score from preoperative to postoperative assessments was used as the diagnostic criterion for POCD. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Measurement of Serum NSE Levels
Serum neuron-specific enolase (NSE) levels, a marker of neuronal injury, were retrospectively measured on postoperative day 3 using enzyme-linked immunosorbent assay (ELISA), ie, serum samples collected on postoperative day 3 (POD3) were analyzed offline, rather than being tested immediately after collection. Elevated serum NSE levels are indicative of neuronal damage and were used to assess the extent of neurological injury in the study population.
Statistical Analysis
Statistical analysis was performed using SPSS software. Continuous variables were presented as mean ± standard deviation (SD) and compared between groups using unpaired t-tests or Mann–Whitney U-tests, as appropriate. Categorical variables were expressed as counts and percentages, and comparisons were made using Fisher’s exact test or chi-squared tests. A p-value of less than 0.05 was considered statistically significant. Receiver operating characteristic (ROC) curve analysis was conducted to evaluate the diagnostic performance of serum NSE levels for predicting POCD.
Results
Study Design and Patient Grouping
The study design is summarized in Figure 1. Out of 300 elderly patients who underwent laparoscopic partial hepatectomy, 82 were excluded based on predefined criteria, leaving 218 patients for analysis. These patients were categorized into groups based on the extent of intraoperative regional cerebral oxygen saturation (rSO2) reduction: 179 patients experienced an rSO2 decrease of ≥10% (D10), while 39 did not (ND10). Similarly, 95 patients experienced an rSO2 decrease of ≥20% (D20), while 123 did not (ND20). This stratification allowed for targeted analysis of clinical and perioperative outcomes in relation to rSO2 reductions.
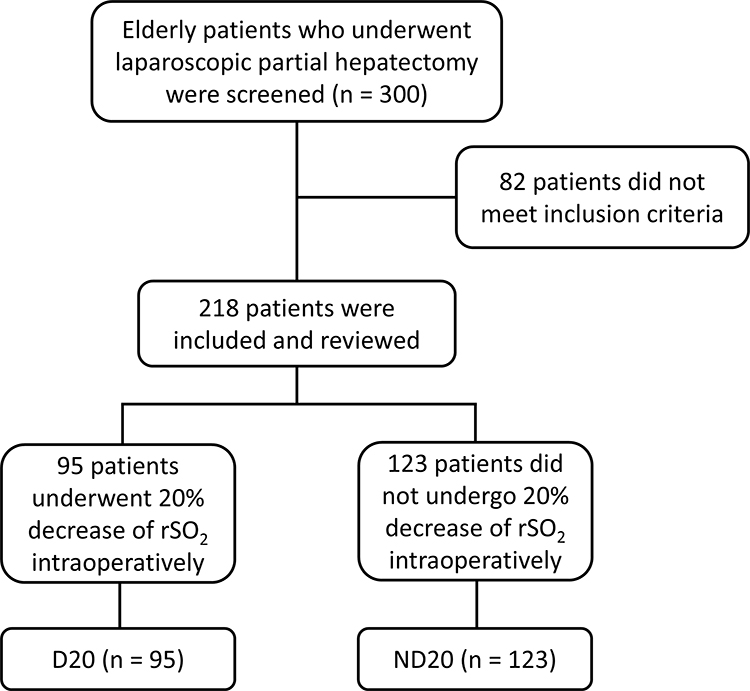 |
Figure 1 Inclusion and grouping of the retrospective study. |
Baseline and Perioperative Factors are Not Linked to rSO2 Reduction
Comparisons were made between groups to evaluate whether baseline demographic and surgical factors influenced rSO2 reductions. No significant differences were found between the D10 and ND10 groups (Table S1) or the D20 and ND20 groups (Table 1) in terms of age, body mass index (BMI), pre-existing conditions, operation time, intraoperative blood loss, or infusion quantities. These findings suggest that rSO2 reductions are not driven by these baseline or perioperative factors.
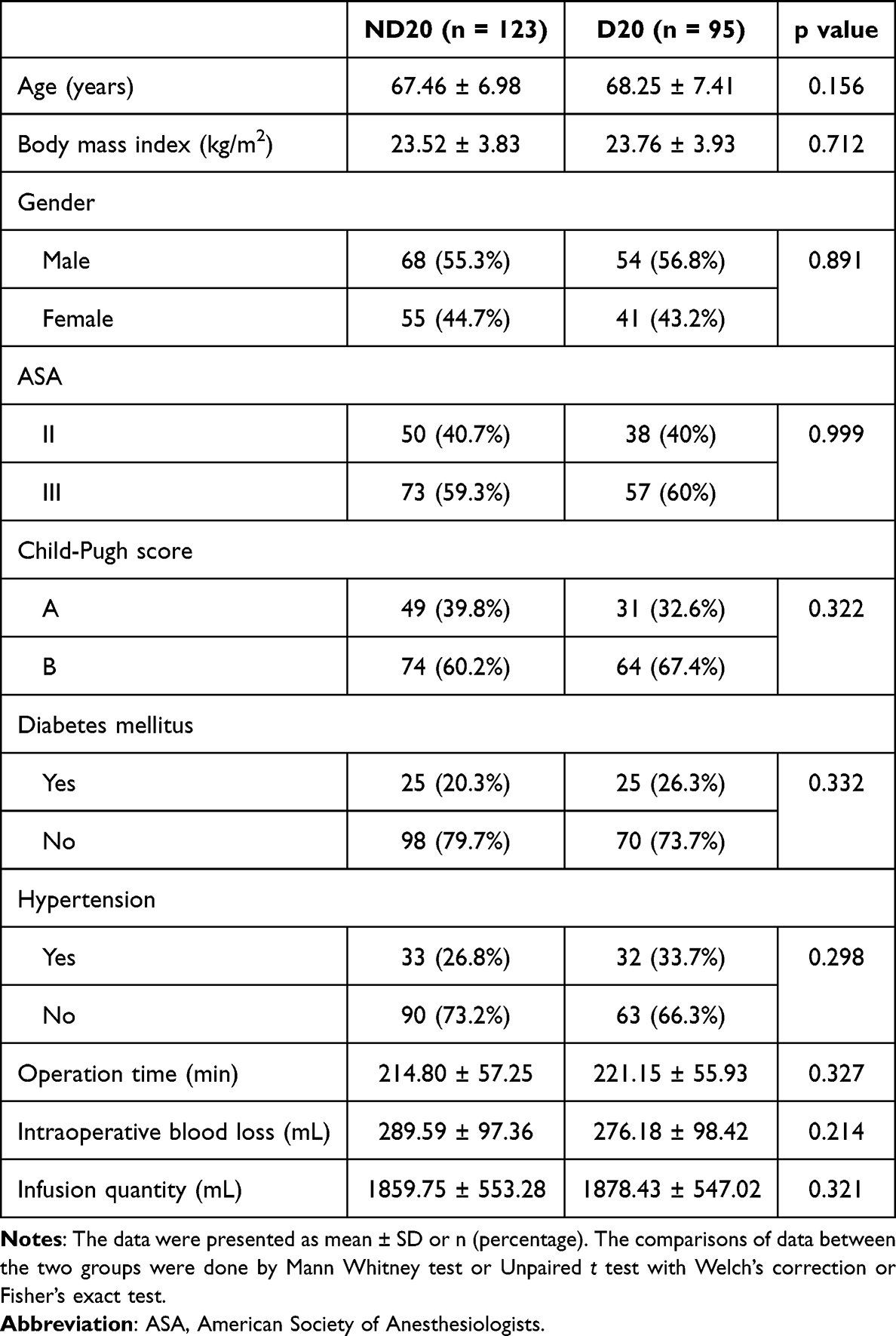 |
Table 1 Demographic and Clinical Factors of Elderly Patients Underwent Laparoscopic Partial Hepatectomy with 20% Decrease of rSO2 Intraoperatively (D20) or Not (ND20) |
Intraoperative rSO2 Reduction Is Associated with Decreased MAP
To further explore the impact of rSO2 reductions during surgery, intraoperative hemodynamic changes were compared. Among the 95 patients in the D20 group, 68 patients (71.6%) experienced MAP <66 mmHg at critical intraoperative timepoints (10 minutes after incision and 10 minutes post-hepatectomy). While heart rate remained similar across all groups and time points (Table S2), MAP was significantly lower in the D20 group compared to the ND20 group at key intraoperative time points, including 10 minutes after the operation began (p = 0.008) and 10 minutes post-hepatectomy (p = 0.014) (Table 2). The optimal MAP cutoff was determined to be <66 mmHg, with an AUC of 0.737 (95% CI: 0.645–0.851, p<0.001), sensitivity of 68.9%, and specificity of 71.2%. These results indicate a link between significant MAP reductions and cerebral hypoperfusion in patients with greater rSO2 decreases.
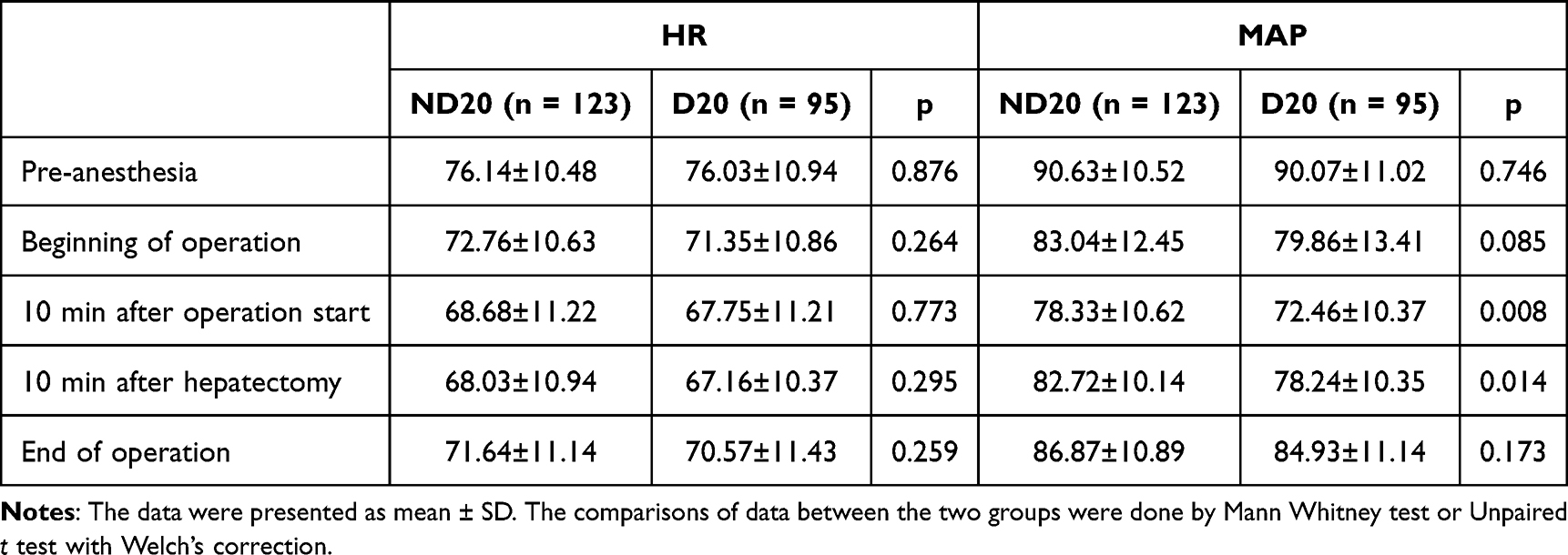 |
Table 2 Comparisons of Heart Rate (HR) and Mean Arterial Pressure (MAP) During the Operation Between Elderly Patients Underwent Laparoscopic Partial Hepatectomy with 20% Decrease of rSO2 Intraoperatively (D20) or Not (ND20) |
Neurological Complications are More Common with Greater rSO2 Reduction
The association between intraoperative rSO2 reductions and postoperative complications was then examined. While no significant differences were observed between D10 and ND10 groups in the incidence of postoperative complications (Table S3), the D20 group showed markedly higher rates of postoperative hypothermia, shivering, delirium on postoperative day 3, and POCD compared to the ND20 group (Table 3). These findings highlight the increased risk of neurological complications in patients with significant rSO2 reductions.
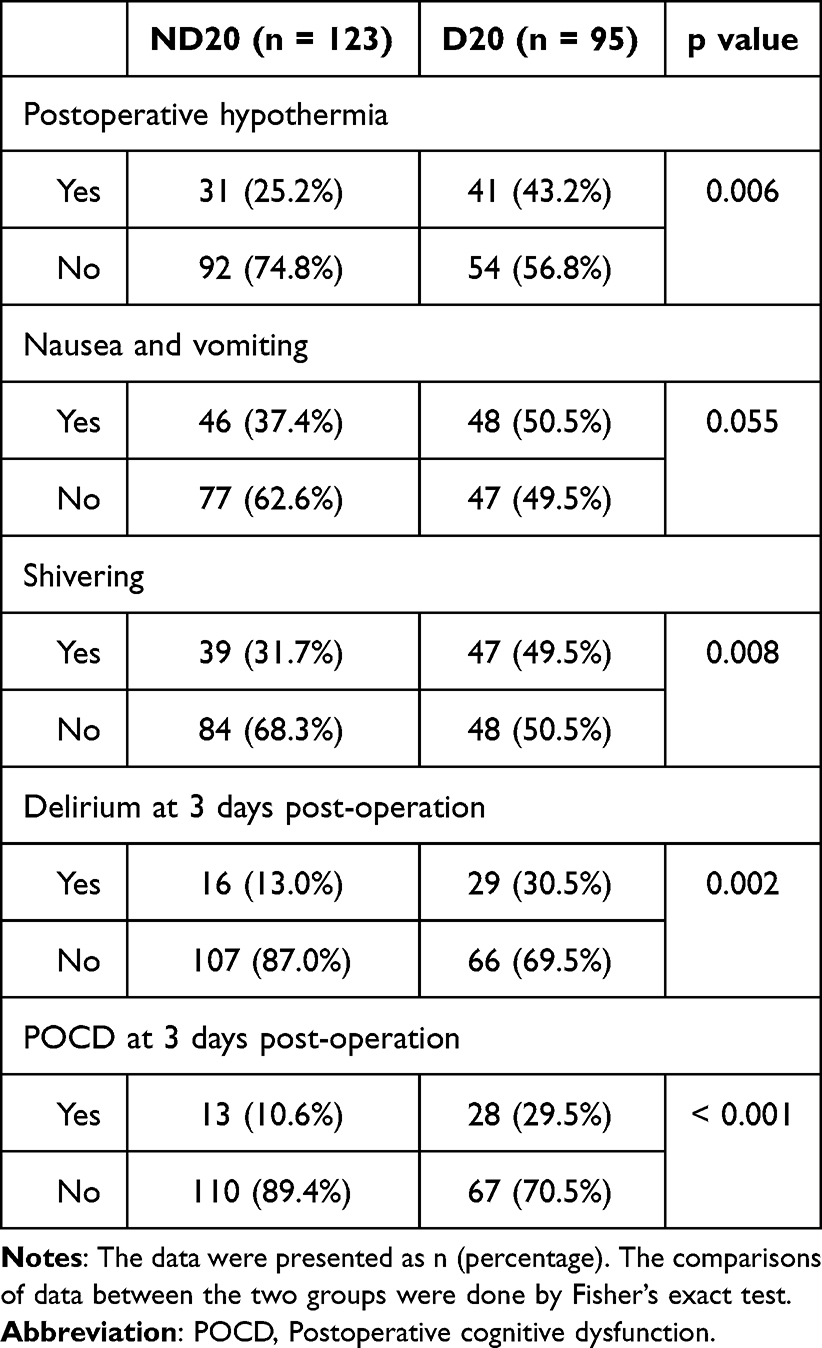 |
Table 3 Comparisons of Perioperative Complications Between Elderly Patients Underwent Laparoscopic Partial Hepatectomy with 20% Decrease of rSO2 Intraoperatively (D20) or Not (ND20) |
Recovery Is Delayed with Greater rSO2 Reduction
The impact of rSO2 reductions on recovery was assessed through postoperative hospital stay. While no significant difference in hospital stay was observed between the D10 and ND10 groups (Figure 2A), the D20 group exhibited significantly prolonged stays compared to ND20 (Figure 2B). This suggests that substantial rSO2 reductions during surgery may delay recovery and discharge.
 |
Figure 2 Comparisons of postoperative hospital stay (A) and serum NSE levels at 3 days post-operation (B) between elderly patients underwent laparoscopic partial hepatectomy with 20% decrease of rSO2 intraoperatively (D20) or not (ND20). The data were presented as mean ± SD. The comparisons of data between the two groups were done by Mann Whitney test. |
Neurological Injury Is Reflected by Increased Serum NSE Levels
Finally, serum neuron-specific enolase (NSE) levels, a marker of neuronal injury, were compared between groups. No significant difference was observed in postoperative hospital stay between D10 and ND10 groups (Figure S1A). On postoperative day 3, NSE levels were significantly higher in the D20 group compared to ND20 (p < 0.001) (Figure S1B). The elevated NSE levels in D20 patients correlate with the increased rates of delirium, providing further evidence of neurological injury linked to substantial rSO2 reductions.
Discussion
This study investigated the relationship between intraoperative reductions in rSO2 and perioperative outcomes, including neurological complications and biochemical markers, in elderly patients undergoing laparoscopic partial hepatectomy. The findings highlight the significant impact of intraoperative cerebral hypoperfusion, particularly when rSO2 reductions exceed 20%, on postoperative recovery and neurological outcomes.22
Our results demonstrate that reductions in rSO2 are associated with increased risks of postoperative delirium and POCD. This finding underscores the importance of continuous intraoperative rSO2 monitoring as a non-invasive, real-time tool to identify cerebral hypoperfusion. The sensitivity of rSO2 in detecting early CDEs provides an opportunity for timely intervention to mitigate adverse outcomes. For example, several practical strategies can be employed: using NIRS-guided goal-directed therapy, maintaining normocapnia and normoxia, avoiding deep hypotension and over-sedation, ensuring neuromuscular reversal with TOF monitoring, and conducting early postoperative neurological assessments. These measures offer a clinically actionable approach to enhance perioperative neuroprotection in elderly patients. While the use of NIRS for rSO2 monitoring has been well-established in cardiac and thoracic surgeries, this study highlights its applicability in liver resection surgeries, particularly in the elderly population who are at higher risk of hypoperfusion-related complications.23 Serial monitoring of serum NSE levels throughout the perioperative period—rather than relying solely on a single POD3 measurement—may provide a more accurate and dynamic reflection of evolving neuronal injury, allowing clinicians to correlate biochemical markers with intraoperative cerebral desaturation patterns (eg, rSO2 decline), assess the timing and magnitude of neuronal stress, and implement timely neuroprotective interventions.
The use of CLCVP is integral in reducing intraoperative blood loss and improving the surgical field. However, as shown in this study, the technique may inadvertently lead to reduced cerebral perfusion. Significant reductions in MAP, observed particularly in patients with greater rSO2 declines, further contribute to hypoperfusion risks. This dual-edged nature of CLCVP emphasizes the need for balanced anesthetic and hemodynamic management strategies. Optimizing fluid therapy, titrating vasopressors, and maintaining MAP within adequate ranges while adhering to CLCVP protocols may help minimize the risks of cerebral hypoperfusion.24 Although the absolute difference in MAP between groups was approximately 6 mmHg, even such modest reductions may be clinically meaningful in elderly patients with impaired cerebral autoregulation. In this population, small drops in MAP can disproportionately reduce cerebral perfusion pressure, leading to measurable declines in rSO2 and potential postoperative neurological impairment. Previous studies on CLCVP have largely focused on its role in reducing intraoperative blood loss, with limited emphasis on its broader systemic and neurological effects. While some studies have reported adverse hemodynamic events, few have directly correlated these with neurological outcomes or biochemical markers. This study addresses these gaps by providing a detailed analysis of rSO2 reductions, perioperative neurological outcomes, and serum NSE levels in the context of liver resection surgeries.25 Additionally, the study contributes to the growing body of evidence supporting the use of NIRS technology for intraoperative cerebral monitoring.
This study found elevated serum NSE levels in patients with significant rSO2 reductions, correlating with increased rates of delirium. NSE serves as a sensitive biochemical marker of neuronal injury and provides additional insight into the extent of brain damage. The combination of rSO2 monitoring and NSE measurement offers a comprehensive approach to evaluating cerebral perfusion and neurological injury.26 Future studies should explore the integration of these tools in clinical practice to improve early detection and management of perioperative neurological complications. Importantly, the interpretation of cerebral oxygen saturation measurements is significantly influenced by the probe location. The frontal lobe placement of rSO2 sensors, as used in this study, primarily reflects regional cortical perfusion and may not fully represent global cerebral oxygenation status. Therefore, caution should be exercised when generalizing our findings, as variations in probe positioning (eg, global vs regional monitoring) could yield different cerebral perfusion patterns and clinical implications.
To translate rSO2 monitoring into actionable intraoperative strategies, we propose several proactive interventions aimed at mitigating cerebral hypoperfusion. First, maintaining a mean arterial pressure (MAP) above the identified threshold of 66 mmHg is essential during key phases of surgery, particularly under low CVP conditions. This can be achieved through targeted vasopressor support and precise fluid management. Second, anesthetic depth should be continuously adjusted in response to real-time BIS and rSO2 trends to prevent excessive vasodilation and secondary hypotension. Third, adopting individualized cerebral oxygenation thresholds—normalized to baseline rSO2 values—allows for earlier recognition of hypoperfusion risk. Finally, any significant rSO2 decline should prompt immediate reassessment of systemic hemodynamics, ventilatory status (eg, PaCO2), and patient positioning to optimize cerebral perfusion. These recommendations would support an integrated, patient-specific neuroprotective approach during elderly laparoscopic hepatectomy.
Several limitations must be acknowledged. First, the retrospective design may introduce selection bias, limiting the generalizability of the findings. Second, while rSO2 and NSE levels were valuable markers, other potential contributors to perioperative neurological complications, such as inflammation or pre-existing cognitive impairment, were not fully assessed. Third, the sample size, though adequate for subgroup analysis, may limit the statistical power for detecting smaller effect sizes. Future prospective studies with larger cohorts and more comprehensive evaluations of neurological outcomes are warranted. This study opens avenues for further research into the optimization of CLCVP protocols to balance the benefits of reduced intraoperative bleeding with the risks of cerebral hypoperfusion. Investigating alternative strategies, such as individualized rSO2 thresholds and combined use of NIRS with biochemical markers like NSE, could enhance patient outcomes. Further, although our study utilized a static CVP threshold to guide fluid restriction, future studies may benefit from incorporating dynamic parameters such as pulse pressure variation (PPV), which offer more physiologically responsive indicators of fluid responsiveness in mechanically ventilated patients. Additionally, prospective trials incorporating neurocognitive assessments at multiple time points may provide a deeper understanding of the long-term impact of intraoperative cerebral desaturation.
Conclusions
Intraoperative reductions in rSO2 are associated with adverse perioperative outcomes, including neurological complications and delayed recovery, in elderly patients undergoing laparoscopic partial hepatectomy. Combining rSO2 monitoring with serum NSE measurement offers a robust approach to detecting and managing cerebral hypoperfusion. These findings emphasize the need for integrated perioperative strategies to optimize cerebral perfusion, reduce complications, and improve recovery in this high-risk population.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The study was approved by the People’s Hospital of Xinjiang Uygur Autonomous Region, and informed written consent was obtained from all the analyzed patients. The study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Informed Consent
All patients signed the informed consent.
Funding
The study was supported by the Hospital Project of the People’s Hospital of Xinjiang Uygur Autonomous Region (#20220225).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–10. doi:10.3322/caac.21492
2. Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70:145–164. doi:10.3322/caac.21601
3. Wakabayashi G, Cherqui D, Geller DA, et al. Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg. 2015;261:619–629. doi:10.1097/SLA.0000000000001184
4. Han HS, Yoon YS, Cho JY, Hwang DW. Laparoscopic liver resection for hepatocellular carcinoma: korean experiences. Liver Cancer. 2013;2:25–30. doi:10.1159/000346224
5. Cherqui D, Husson E, Hammoud R, et al. Laparoscopic liver resections: a feasibility study in 30 patients. Ann Surg. 2000;232:753–762. doi:10.1097/00000658-200012000-00004
6. Yu L, Sun H, Jin H, Tan H. The effect of low central venous pressure on hepatic surgical field bleeding and serum lactate in patients undergoing partial hepatectomy: a prospective randomized controlled trial. BMC Surg. 2020;20:25. doi:10.1186/s12893-020-0689-z
7. Wang F, Sun D, Zhang N, Chen Z. The efficacy and safety of controlled low central venous pressure for liver resection: a systematic review and meta-analysis. Gland Surg. 2020;9:311–320. doi:10.21037/gs.2020.03.07
8. Liu TS, Shen QH, Zhou XY, et al. Application of controlled low central venous pressure during hepatectomy: a systematic review and meta-analysis. J Clin Anesth. 2021;75:110467. doi:10.1016/j.jclinane.2021.110467
9. Ding X, Zha T, Abudurousuli G, et al. Effects of regional cerebral oxygen saturation monitoring on postoperative cognitive dysfunction in older patients: a systematic review and meta-analysis. BMC Geriatr. 2023;23:123. doi:10.1186/s12877-023-03804-6
10. Robba C, Battaglini D, Rasulo F, Lobo FA, Matta B. The importance of monitoring cerebral oxygenation in non brain injured patients. J Clin Monit Comput. 2023;37:943–949. doi:10.1007/s10877-023-01002-8
11. Ye H, Wu H, Li B, Zuo P, Chen C. Application of cardiovascular interventions to decrease blood loss during hepatectomy: a systematic review and meta-analysis. BMC Anesthesiol. 2023;23:89. doi:10.1186/s12871-023-02042-y
12. Lv H, Xiong C, Wu B, et al. Effects of targeted mild hypercapnia versus normocapnia on cerebral oxygen saturation in patients undergoing laparoscopic hepatectomy under low central venous pressure: a prospective, randomized controlled study. BMC Anesthesiol. 2023;23:257. doi:10.1186/s12871-023-02220-y
13. Nanashima A, Hiyoshi M, Imamura N, et al. Measuring intraoperative anesthetic parameters during hepatectomy with inferior vena cava clamping. Langenbecks Arch Surg. 2023;408:455. doi:10.1007/s00423-023-03172-0
14. Vu EL, Brown CHT, Brady KM, Hogue CW. Monitoring of cerebral blood flow autoregulation: physiologic basis, measurement, and clinical implications. Br J Anaesth. 2024;132:1260–1273. doi:10.1016/j.bja.2024.01.043
15. Thooft A, Favory R, Salgado DR, et al. Effects of changes in arterial pressure on organ perfusion during septic shock. Crit Care. 2011;15:R222. doi:10.1186/cc10462
16. Soh S, Shim JK, Song JW, Kim KN, Noh HY, Kwak YL. Postoperative delirium in elderly patients undergoing major spinal surgery: role of cerebral oximetry. J Neurosurg Anesthesiol. 2017;29:426–432. doi:10.1097/ANA.0000000000000363
17. Lois Schick M. Assessment and monitoring of the perianesthesia patient. In: Drain’s PeriAnesthesia Nursing-E-Book: A Critical Care Approach. 2012:352.
18. Robba C, Taccone FS, Citerio G. Monitoring cerebral oxygenation in acute brain-injured patients. Intensive Care Med. 2022;48:1463–1466. doi:10.1007/s00134-022-06788-w
19. Yang H, Xue FS, Shao LJ, Hou HJ. Use of serum neuron-specific enolase level to predict adverse neurologic outcomes after aortic surgery. Thorac Cardiovasc Surg. 2020;68:291–292. doi:10.1055/s-0039-1685541
20. de Boode W-P, Noori S, van Laere D, Dempsey E, Seri I. Comprehensive, real-time hemodynamic monitoring and data acquisition: an essential component of the development of individualized neonatal intensive care. In: Neonatology Questions and Controversies: Neonatal Hemodynamics-E-Book. Elsevier Health Sciences; 2023:260.
21. Saberi K, Sharifi S, Orandi A. Can underlying co-morbidities affect cerebral oximetry in cardiac surgery patients? Acta Med Iran. 2024:117–128.
22. Oncu K, Saylan S. Effects of haemodynamic changes caused by different pneumoperitoneum pressures on cerebral oxygenation in laparoscopic cholecystectomy: prospective randomised controlled trial. J Coll Physicians Surg Pak. 2024;34:16–21. doi:10.29271/jcpsp.2024.01.16
23. Bennett SR, Smith N, Bennett MR. Cerebral oximetry in adult cardiac surgery to reduce the incidence of neurological impairment and hospital length-of-stay: a prospective, randomized, controlled trial. J Intensive Care Soc. 2022;23:109–116. doi:10.1177/1751143720977280
24. Mu Z, Gao J, Xin C, Wu K, Dong Y, Ge Y. Effects of controlled low central venous pressure on cerebral blood flow in patients undergoing open hepatectomy. Chin J Anesthesiol. 2022:1469–1472.
25. Hu T, Collin Y, Lapointe R, et al. Preliminary experience in combined somatic and cerebral oximetry monitoring in liver transplantation. J Cardiothorac Vasc Anesth. 2018;32:73–84. doi:10.1053/j.jvca.2017.07.019
26. Jakkula P, Hastbacka J, Reinikainen M, et al. Near-infrared spectroscopy after out-of-hospital cardiac arrest. Crit Care. 2019;23:171. doi:10.1186/s13054-019-2428-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.