Back to Journals » Clinical Ophthalmology » Volume 19
Correlation Between Tear Film Stability and Myopia in Children
Authors Huang PW, Kuo YK, Chen NN ![]() , Li JH, Wu CH, Chen HM, Su KW, Sun CC
, Li JH, Wu CH, Chen HM, Su KW, Sun CC ![]()
Received 8 March 2025
Accepted for publication 29 May 2025
Published 10 July 2025 Volume 2025:19 Pages 2221—2228
DOI https://doi.org/10.2147/OPTH.S527012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pei-Wei Huang,1,2,* Yu-Kai Kuo,2,* Nan-Ni Chen,3 Ju-Hsien Li,2 Cheng‐Hsiu Wu,2 Ho-Min Chen,2 Kuan-Wen Su,4,5 Chi-Chin Sun2,6
1Department of Ophthalmology, Lo-Hsu Medical Foundation, Lotung Poh-Ai Hospital, Yilan, Taiwan; 2Department of Ophthalmology, Keelung Chang Gung Memorial Hospital, Keelung City, Taiwan; 3Department of Ophthalmology, Chiayi Chang Gung Memorial Hospital, Chiayi, Taiwan; 4Department of Paediatrics, Keelung Chang Gung Memorial Hospital, Keelung City, Taiwan; 5Department of Paediatrics, College of Medicine, Chang Gung University, Taoyuan, Taiwan; 6Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan
*These authors contributed equally to this work
Correspondence: Chi-Chin Sun, Department of Ophthalmology, Chang Gung Memorial Hospital, 222 Mai Chin Road, An Leh District, Keelung, Taiwan, Email [email protected]
Purpose: To investigate the correlation between dry eye and myopia in Taiwanese school children.
Methods: This retrospective cohort study enrolled children aged 5– 14-years-old between January 2021 and April 2022. The Ocular Surface Disease Index (OSDI) and an activity questionnaire were used to assess the severity of dry eye and the children’s lifestyle. Dry eye was assessed using Schirmer’s I test, tear break-up time (TBUT), corneal fluorescein staining, and the lid abnormality score. The correlation between dry eye and myopia was determined by linear regression analysis.
Results: In total, 31 non-myopic (mean age, 9.03 years) and 34 myopic (mean age, 8.44 years) children were included in the final analysis. Children with myopia had a significantly higher mean OSDI than children without myopia (4.79 ± 6.90 versus 1.68 ± 3.46, P = 0.024). The prevalence of dry eye disease was higher in myopic children (11.7%) than non-myopic children (3.2%) without significant difference. There were no significant differences in the Schirmer test, TBUT, corneal fluorescein staining score, or lid abnormality score between groups. Multiple regression analyses showed the OSDI was significantly associated with more negative spherical power (regression coefficient [B] = − 0.74, 95% confidence interval = − 1.48 to − 0.01, P = 0.048) and presence of myopia (B = 3.44, 95% CI = 0.72 to 6.16, P = 0.014) after adjusting for age.
Conclusion: Children with myopia have a higher OSDI and higher prevalence of dry eye than children without myopia. After adjusting for age, the OSDI was associated with more negative spherical power and the presence of myopia.
Keywords: dry eye, myopia, pediatric population, tear film stability
Introduction
Dry eye is a common disorder and the fifth most prevalent ocular condition among patients seeking eyecare.1 According to the International Dry Eye WorkShop (DWES II) in 2017, dry eye is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film accompanied by ocular symptoms.2 Dry eye is diagnosed based on clinical symptoms and signs, including the tear break-up time (TBUT), osmolarity, and ocular surface staining.3 Recent studies suggest that corneal epithelial thickness profiles may offer additional diagnostic value in differentiating dry eye from other conditions.4 The prevalence of dry eye increases with age and varies from 5% to 50%, depending on the diagnostic criteria used and population surveyed.5 In Taiwan, the annual crude incidence rate of dry eye increased from 1.46 per 1000 in 2001 to 4.26 per 1000 in 2015.6 However, only a limited number of studies have investigated the prevalence and characteristics of dry eye in children, due to children’s poorer ability to describe their symptoms, lack of attention and poorer cooperation of children with ophthalmic examination.7
Myopia causes blurred vision at a distance without correction. High axial myopia is also related to an increased risk of irreversible vision loss, including retinal detachment, choroidal neovascularization, cataracts, and glaucoma.8 The prevalence of myopia has markedly increased in children and young adults in East and Southeast Asia.9 In Taiwan, 86.1% of male military conscripts aged 18 to 24-years-old between 2010 and 2011 had myopia.10 The prevalence of high myopia (more than −6.0 D) among freshmen students at National Taiwan University increased from 23.5% in 1988 to 38.4% in 2005.11 Among school children, the prevalence of myopia increased from 5.37% to 25.41% for 7-year-olds and from 30.66% to 76.67% for 12-year-olds between 1983 and 2017.12 Hence, early detection of myopia and effective myopia-control strategies for children could benefit many patients.
There are some shared risk factors for dry eye and myopia, including age, near work activity, and long-term use of 3C electronic products.5,7,13,14 Some treatments for myopia—including contact lenses and instillation of topical atropine—have also been proven to exacerbate dry eye.15,16 Patients with pathologic myopia have lower TBUT scores and more severe dry eye symptoms compared to healthy adult individuals.17 However, only a few studies have evaluated the relationship between dry eye and myopia, especially in children. Previous reports demonstrated that the prevalence of dry eye was higher in school children with myopia compared to children without myopia (around 10%).18,19 In addition, children with myopia have lower TBUT scores compared to emmetropic children.20 However, the precise relationship between dry eye and the presence of myopia in school-aged children remains unclear. Thus to address this knowledge gap, the current study compared a cohort of Taiwanese school children with and without myopia to elucidate the correlation between dry eye and myopia.
Material and Methods
Subjects
This cross-sectional study included children aged 5–14-years-old who had received an ophthalmic examination at Keelung Chang Gung Memorial Hospital, Keelung, Taiwan between January 2021 and April 2022. All of the subjects were enrolled from the Prediction of Allergies in Taiwanese Children (PATCH) birth cohort study, which contains the complete medical records and data on detailed physical examinations and serial blood analysis of the children since birth.21 The purpose of the PATCH study was explained to the parents of the participants and the parents provided written informed consent. This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (Approval No.: 201901822A3) and followed the tenets of the Declaration of Helsinki.
The inclusion criteria were school-aged children who could undergo a complete eye examination and had no previous ocular disease. We excluded children who (1) had any eye(s) with combined ocular diseases (eg, cataracts, congenital retinal diseases, amblyopia, or strabismus) (2), who did not give consent (3) who had a previous history of surgery or any other ocular disease except for refractive errors, (4) or had any systemic disease that may affect visual acuity.
Questionnaire
Before clinical examination, each child completed the Ocular Surface Disease Index (OSDI) questionnaire and an activity questionnaire to assess the severity of dry eye and the child’s lifestyle, respectively. If the participants were too young to complete the questionnaire by themselves, trained ophthalmology staff interviewed the child and completed the questionnaire with the help of the child’s parents.
The OSDI questionnaire consists of twelve items designed to assess ocular symptoms, vision-related function, and environmental triggers. Based on the OSDI, the changes in the ocular surface were defined as normal (0–12), mild (13–22), moderate (23–32), or severe (33–100).6 An OSDI of more than 12 was defined as the presence of dry eye symptoms.
The activity questionnaire consisted of 12 questions on the total number of hours per week spent on near work and outdoor activities, as well as the duration of exposure to the sun. Items of near work include writing, near practice, computer use, mobile phone use, and television watching. Parental myopia was evaluated by asking “Does at least one parent of the child have high myopia (spherical power of −5 diopters22 or higher)?”; the answers were recorded as “yes” and “no”. If the child was unable to answer specific questions (eg, regarding parental myopia), responses were obtained directly from the accompanying parent or legal guardian.
Ocular Examination and Data Collection
All children underwent a detailed ophthalmic examination that included best-corrected visual acuity, measured refractive state after complete cycloplegia together with corneal power (Auto Ref/ Keratometer ARK-1a/ARK-1; Nidek, Gamagori, Aichi, Japan), slit-lamp biomicroscopy (BQ 900, Haag-Streit AG, Koeniz, Switzerland), external eye photography, and axial length (AL) measurement (IOLMaster 500, Carl Zeiss Meditec AG, Jena, Germany). Best-corrected visual acuity (BCVA) was measured using a Snellen chart and converted into the logarithm of the minimal angle of resolution (logMAR) for statistical analysis. Three trained ophthalmologists performed the ocular examinations and collected the data. The spherical equivalent (SE) was defined as the spherical power plus half of the negative cylinder power. In the current study, myopia was defined as an SE of −0.5 D or higher. All results were collected for the left eye.
Dry Eye Parameters
Schirmer’s I test measures tear volume by placing a paper strip on the lateral third of the lower eyelid after drying the inferior fornix without topical anesthesia.6 The length of the moistened portion of the strip was measured after 5 minutes.
The TBUT was measured by application of a single fluorescein strip to the inferior palpebral conjunctiva after instilling a drop of normal saline. The mean time for three replicates was recorded to assess tear film stability.6
Corneal fluorescein staining was graded using the National Eye Institute/Industry grading (NEI) scale.23 Briefly, the NEI scale divides the cornea into five sections and assigns a value from 0 (absent) to 3 (severe) for each section, according to the amount, size, and confluence of punctate keratitis, with a maximum of 15 points.
The lid abnormality score was evaluated according to the grading scale proposed by Arita et al.24 Four lid margin abnormalities (irregularity, telangiectasia, plugged meibomian gland orifices, and replacement of the mucocutaneous junction) were scored from 0 to 4 according to the number of these abnormalities in the examined eye.
In the current study, the diagnosis of dry eye disease was based on (1) the presence of dry eye symptoms (OSDI ≥ 12), (2) abnormal tear production as determined by Schirmer’s I test (≤ 5 mm), and (3) abnormal tear film stability as determined by the TBUT (≤ 5 seconds).25,26
Statistical Analysis
The differences between the children with and without myopia were analyzed using Fisher’s exact test and the independent samples t-test for categorical and continuous data, respectively. Pearson’s correlation coefficient was used to assess the simple correlations between the OSDI and several variables, including age, time spent on near work or outdoor activities, spherical power, and AL. We also performed multiple linear regression analysis to evaluate the factors related to the OSDI via backward selection. Data were analyzed using SPSS (version 20.0; SPSS, Chicago, IL, USA). Statistical significance was defined as a two-tailed P-value of < 0.05.
Results
Medical records were collected for 69 eyes in 69 children. Four eyes from four children were excluded due to incomplete refractive data. A total of 31 non-myopic(average age, 9.03 ± 2.43 years) and 34 myopic (average age, 8.44 ± 2.18 years) children were included in the final analysis.
Table 1 summarizes the demographic data and refractive status of all children and the two groups. Compared to non-myopic children, myopic children had significantly higher negative spherical power (−1.65 ± 1.84 versus 0.77 ± 0.80 diopters, P < 0.001) and longer axial lengths (23.91 ± 1.04 versus 22.82 ± 0.92 mm, P < 0.001). There were no significant differences in the time spent on different activities or duration of sun exposure between the two groups.
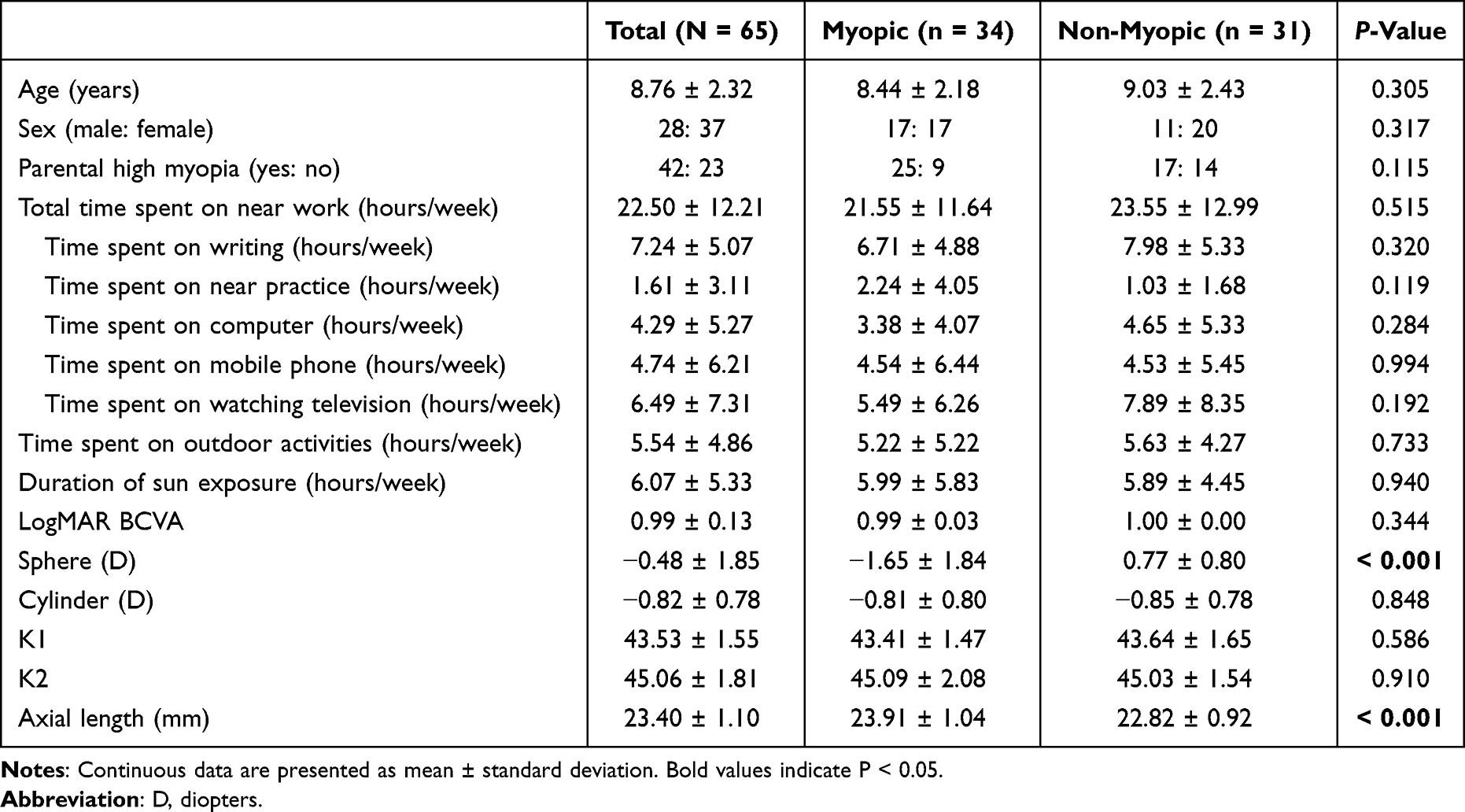 |
Table 1 Characteristics of the Children with and without Myopia |
Table 2 presents the dry eye parameters for children with and without myopia. In contrast to non-myopic children, myopic children had a significantly higher OSDI (4.79 ± 6.90 versus 1.68 ± 3.46, P = 0.024). Based on the criteria for the diagnosis of dry eye disease, a total of five children (7.7%) were diagnosed with dry eye (one non-myopic child and four children with myopia). The prevalence of dry eye disease was 11.7% in the myopic group and 3.2% in the non-myopic group, although the difference was not statistically significant (P = 0.358). There were no significant differences in the Schirmer test, TBUT, corneal fluorescein staining score, or lid abnormality score between groups.
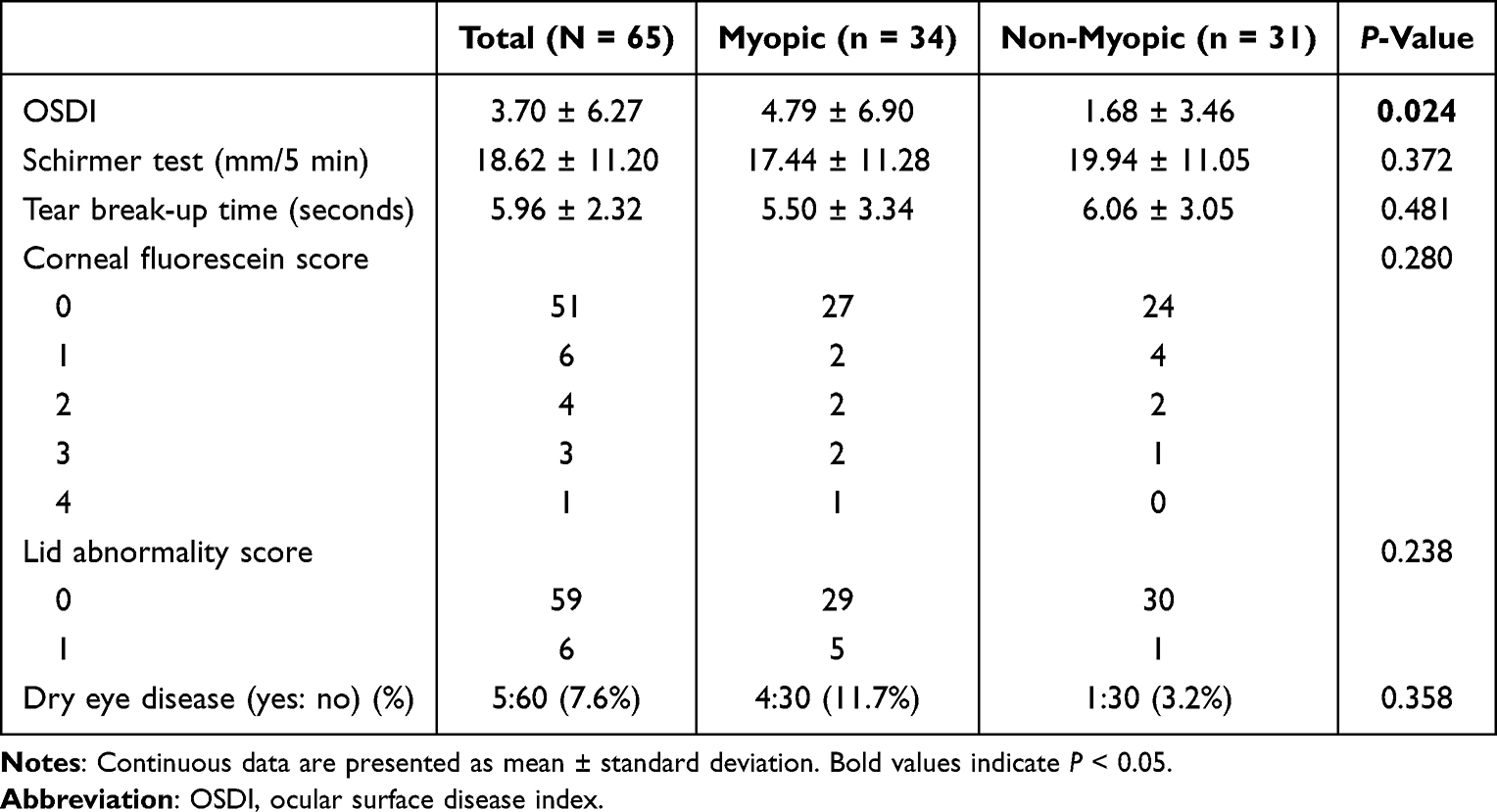 |
Table 2 Dry Eye Parameters in the Children with and without Myopia |
Table 3 shows the simple correlation analysis between the OSDI and myopic variables. The OSDI was significantly correlated associated with older age (Pearson’s correlation coefficient (r) = 0.25; P = 0.037) and more negative spherical power (r = −0.26; P = 0.036).
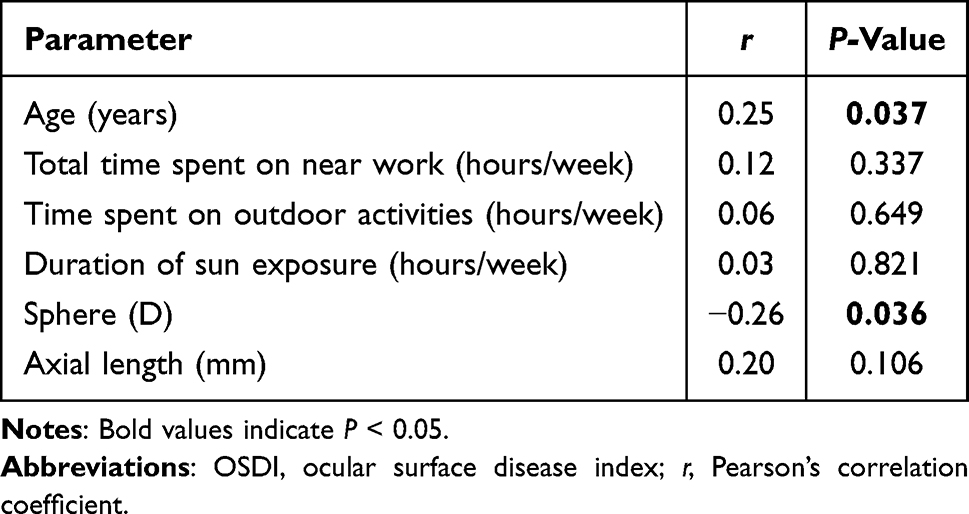 |
Table 3 Correlation Analysis of the OSDI and Myopic Variables |
Multiple regression analyses of the OSDI and myopic variables (Tables 4 and 5) revealed the OSDI was significantly associated with more negative spherical power (B = −0.74, 95% CI = −1.48 to −0.01, P = 0.048) and the presence of myopia (B = 3.44, 95% CI = 0.72 to 6.16, P = 0.014) after adjusting for age.
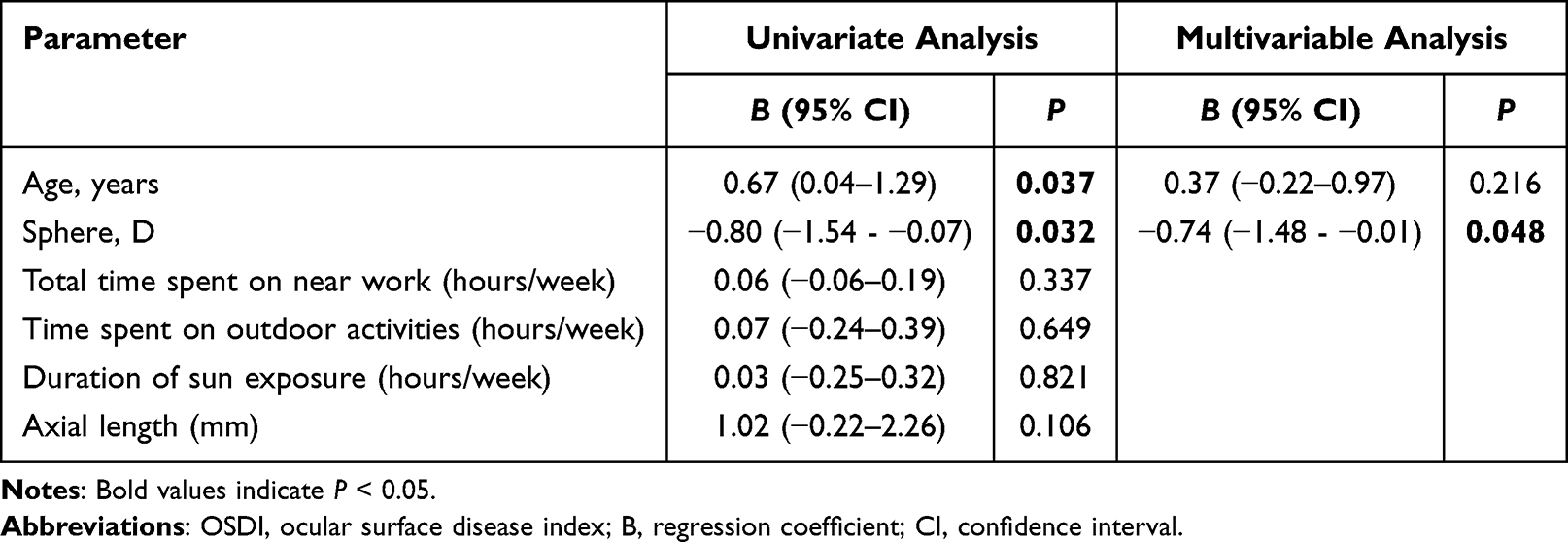 |
Table 4 Linear Regression Analysis of the OSDI and Myopic Variable |
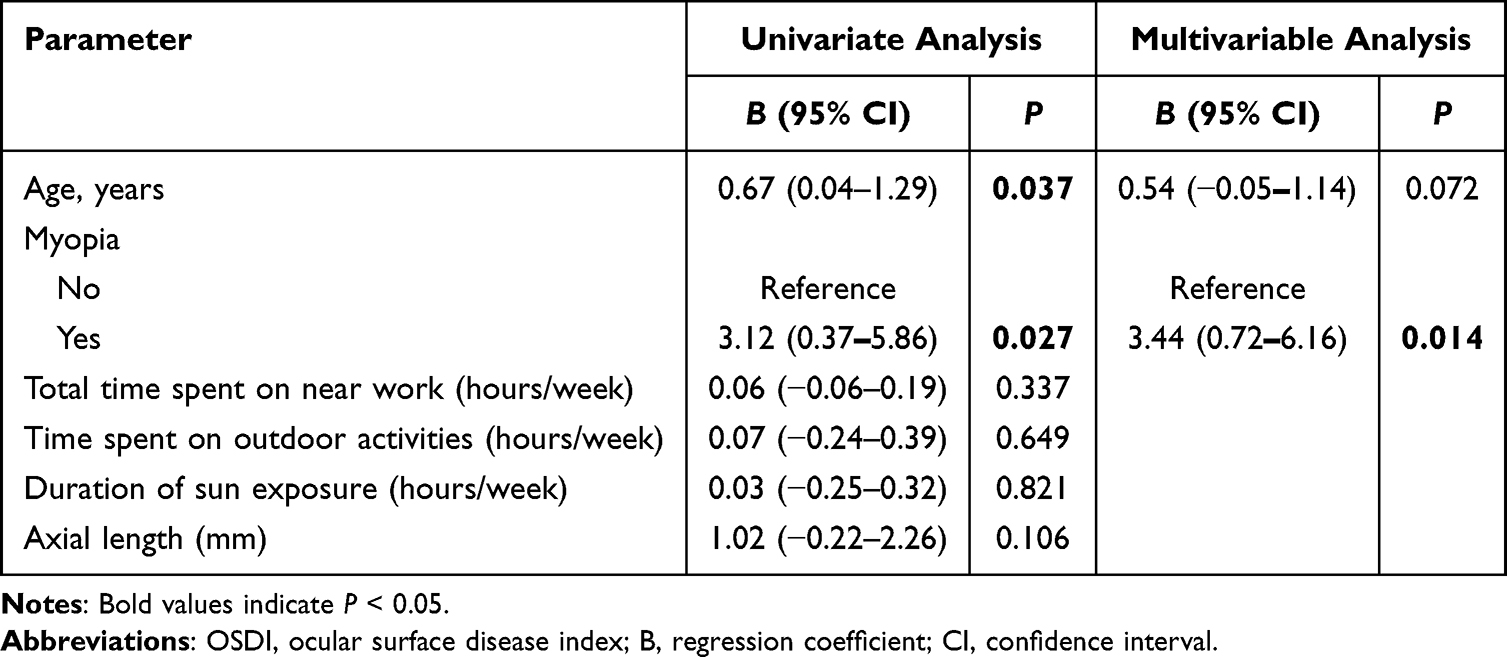 |
Table 5 Linear Regression Analysis of the OSDI and Myopic Variables |
Discussion
To the best of our knowledge, this is the first cross-sectional study to explore the correlation between dry eye and myopia in school-aged children (5–14 years). We found dry eye disease was more prevalent in myopic children than in non-myopic children (11.7% versus 3.2%, P = 0.358). Moreover, the group with myopia had a higher OSDI than the group without myopia. In addition, the OSDI was significantly correlated with older age and more negative spherical power. After adjusting for age, the OSDI remained significantly associated with negative spherical power and the presence of myopia.
Previous studies investigated the relationship between myopia and dry eye.17,20 However, most studies only focused on adult populations. In this cohort, 11.7% of myopic children were diagnosed with dry eye disease, which is slightly lower than the rates reported in previous studies.18,19 This difference may possibly be due to the use of different diagnostic methods. Wang et al found the prevalence of dry eye in Chinese myopic teenagers was 18.95%; however, they diagnosed dry eye using keratography.19 In a cross-sectional study conducted by Wang et al, the prevalence of dry eye in myopic children was 15.9%, and they observed dry eye was associated with picky eating and eye rubbing.18 Based on Table 2, although subjective symptoms OSDI differed significantly, objective measures such as TBUT and Schirmer’s test did not show significant differences. This suggests that early subjective symptoms of ocular discomfort may precede measurable tear dysfunction in myopic children.
The association between dry eye and increased higher-order aberrations, which may lead to further development of myopia, has also been investigated.27 On the other hand, decreased tear film stability caused by dry eye increases the risk of higher-order aberrations.28 In a study conducted in Japan, Yotsukura et al reported that more severe dry eye symptoms correlated with higher myopic refraction and longer axial length in elementary and junior high school students, respectively.29 This finding is consistent with our results, as we found the OSDI was significantly associated with negative spherical power and the presence of myopia, and an intensive educational environment with both more near-work and fewer outdoor activities also contributes to this finding. Consistent with our findings, Harza et al reported that myopic individuals exhibited tear film instability and structural changes including reduced tear film breakup time, higher order aberrations, and alterations in choroidal thickness. These findings further support the hypothesis that anatomical and physiological changes in myopic eyes may contribute to dry eye symptoms, even in pediatric populations.30
Orthokeratology and atropine are the main treatment strategies to reduce the progression of myopia in children. Some studies have pointed out that orthokeratology may alter tear stability by thinning the tear film lipid layer due to loss of the meibomian glands, conjunctival fold, and metaplasia and a reduction in goblet cell density.31,32 However, the mechanisms that lead to lens-induced tear film instability remain controversial.32–35 We were unable to conduct subgroup analysis based on treatments for myopia due to the limited numbers of patient. Hence, further thorough investigations of larger cohorts with subgroup analysis are needed to clarify the relationship between treatments for myopia and tear stability.
Studies have demonstrated a strong correlation between dry eye and the rate of smartphone use among pediatric populations.36 In contrast, we found outdoor activity protected against pediatric dry eye. We observed no significant differences in the daily activities between myopic and non-myopic children, though this analysis may be limited by the small sample size. Differences in findings regarding screen time may be attributable to environmental, genetic, and methodological factors. Previous research also demonstrated that myopia is associated with being underweight rather than normal or high body mass index.37 In general, parents and ophthalmologists should pay close attention and take caution regarding the duration of near activities for children.
The limitations of the current study include the small sample size, retrospective cross-sectional design, and subjective grading system for dry eye. However, all children underwent detailed ocular examinations as part of continuous follow-up at the same hospital (PATCH study) and a single ophthalmologist (P.W. Huang) graded the corneal fluorescein staining and lid abnormality score. These strengths help to compensate for data loss and the subjective grading system. Moreover, allergic conjunctivitis has a higher prevalence in children than adults and may be confused for dry eye symptoms,[25] which makes the diagnosis of dry eye more difficult. However, we diagnosed dry eye disease in children based on a combination of the OSDI, Schirmer’s I test, and the TBUT, which may improve diagnostic accuracy. Nevertheless, larger-scale studies are necessary to validate these findings.
In conclusion, children with myopia had a higher OSDI and higher prevalence of dry eye than children without myopia. After adjusting for age, the OSDI was associated with more negative spherical power and myopia. In general, further long-term, larger sample sizes and large-scale longitudinal studies of dry eye disease in myopic children are warranted to confirm these preliminary findings in the future.
Ethics Statement
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (Approval No.: 201901822A3) and followed the tenets of the Declaration of Helsinki.
Acknowledgments
The wish to acknowledge the support of the Maintenance Project of the Center of data science and Biostatistics (Grant CGRPG2F0011) at Keelung Chang Gung Memorial Hospital for assistance with study design and monitoring and data analysis and interpretation.
Author Contributions
Pei-Wei Huang and Yu-Kai Kuo contributed equally to this work and should be considered co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Chang Gung Memorial Hospital (CMRPG2J0211 and CMRPG2J0212). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have nothing to disclose regarding financial or nonfinancial conflicts of interest with respect to this manuscript.
References
1. Bradley JL, Ozer Stillman I, Pivneva I, Guerin A, Evans AM, Dana R. Dry eye disease ranking among common reasons for seeking eye care in a large US claims database. Clin Ophthalmol. 2019;13:225–232. doi:10.2147/OPTH.S188314
2. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
3. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocul Surf. 2017;15(3):539–574. doi:10.1016/j.jtos.2017.05.001
4. Rattan S, Anwar D. Comparison of corneal epithelial thickness profile in dry eye patients, keratoconus suspect, and healthy eyes. Eur J Ophthalmol. 2020;30(6):1506–1511. doi:10.1177/1120672120952034
5. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
6. Kuo Y-K, Lin I-C, Chien L-N, et al. Dry Eye Disease: a Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits. J Clin Med. 2019;8(8):1227. doi:10.3390/jcm8081227
7. Alves M, Dias AC, Rocha EM. Dry eye in childhood: epidemiological and clinical aspects. Ocul Surf. 2008;6(1):44–51. doi:10.1016/s1542-0124(12)70104-0
8. Cf L, Liu L, Lai CC, et al. Multimodal imaging including spectral-domain optical coherence tomography and confocal near-infrared reflectance for characterization of lacquer cracks in highly myopic eyes. Eye. 2014;28(12):1437–1445. doi:10.1038/eye.2014.221
9. Wolffsohn JS, Flitcroft DI, Gifford KL, et al. IMI - Myopia Control Reports Overview and Introduction. Invest Ophthalmol Visual Sci. 2019;60(3):M1–M19. doi:10.1167/iovs.18-25980
10. Lee -Y-Y, Lo C-T, Sheu S-J, Lin JL. What Factors are Associated with Myopia in Young Adults? A Survey Study in Taiwan Military Conscripts. Invest Ophthalmol Visual Sci. 2013;54(2):1026–1033. doi:10.1167/iovs.12-10480
11. Wang TJ, Chiang TH, Wang TH, Lin LL, Shih YF. Changes of the ocular refraction among freshmen in National Taiwan University between 1988 and 2005. Eye (Lond). 2009;23(5):1168–1169. doi:10.1038/eye.2008.184
12. Tsai T-H, Liu Y-L, Ma IH, et al. Evolution of the Prevalence of Myopia among Taiwanese Schoolchildren: a Review of Survey Data from 1983 through 2017. Ophthalmology. 2021;128(2):290–301. doi:10.1016/j.ophtha.2020.07.017
13. Moon JH, Lee MY, Moon NJ. Association between video display terminal use and dry eye disease in school children. J Pediatr Ophthalmol Strabismus. 2014;51(2):87–92. doi:10.3928/01913913-20140128-01
14. Morgan IG, Wu PC, Ostrin LA, et al. IMI Risk Factors for Myopia. Invest Ophthalmol Vis Sci. 2021;62(5):3. doi:10.1167/iovs.62.5.3
15. Arita R, Itoh K, Inoue K, Kuchiba A, Yamaguchi T, Amano S. Contact lens wear is associated with decrease of meibomian glands. Ophthalmology. 2009;116(3):379–384. doi:10.1016/j.ophtha.2008.10.012
16. Baudouin C, Labbe A, Liang H, Pauly A, Brignole-Baudouin F. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312–334. doi:10.1016/j.preteyeres.2010.03.001
17. Ilhan N, Ilhan O, Ayhan TE, et al. Is there a relationship between pathologic myopia and dry eye syndrome? Cornea. 2014;33(2):169–171. doi:10.1097/ICO.0000000000000033
18. Wang N, Zhuang X, Zhong X, Zhang J, Li G, Li S. Questionnaire Analysis on Incidence and Risk Factors of Dry Eye in Children From a Myopia Outpatient Clinic. Front Med Lausanne. 2022;9:846709. doi:10.3389/fmed.2022.846709
19. Wang X, Lu X, Yang J, et al. Evaluation of Dry Eye and Meibomian Gland Dysfunction in Teenagers with Myopia through Noninvasive Keratograph. J Ophthalmol. 2016;2016:6761206. doi:10.1155/2016/6761206
20. Fahmy RM, Aldarwesh A. Correlation between dry eye and refractive error in Saudi young adults using noninvasive Keratograph 4. Indian J Ophthalmol. 2018;66(5):653–656. doi:10.4103/ijo.IJO_1103_17
21. Yao TC, Ou LS, Yeh KW, et al. Associations of age, gender, and BMI with prevalence of allergic diseases in children: PATCH study. J Asthma. 2011;48(5):503–510. doi:10.3109/02770903.2011.576743
22. Chen D, Lam AK, Cho P. Posterior corneal curvature change and recovery after 6 months of overnight orthokeratology treatment. Ophthalmic Physiol Opt. 2010;30(3):274–280. doi:10.1111/j.1475-1313.2010.00710.x
23. Lemp MA. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995;21(4):221–232.
24. Arita R, Itoh K, Maeda S, et al. Proposed diagnostic criteria for obstructive meibomian gland dysfunction. Ophthalmology. 2009;116(11):2058–63e1. doi:10.1016/j.ophtha.2009.04.037
25. Arita R, Morishige N, Koh S, et al. Increased Tear Fluid Production as a Compensatory Response to Meibomian Gland Loss: a Multicenter Cross-sectional Study. Ophthalmology. 2015;122(5):925–933. doi:10.1016/j.ophtha.2014.12.018
26. Jung JW, Kim JY, Chin HS, Suh YJ, Kim TI, Seo KY. Assessment of meibomian glands and tear film in post-refractive surgery patients. Clin Exp Ophthalmol. 2017;45(9):857–866. doi:10.1111/ceo.12993
27. Vasudevan B, Fisher B, Case B, Lam P, Wayman J. Progression of lower and higher-order aberrations: a longitudinal study. BMC Ophthalmol. 2015;15(1):11. doi:10.1186/1471-2415-15-11
28. Koh S. Mechanisms of Visual Disturbance in Dry Eye. Cornea. 2016;35(1):S83–s88. doi:10.1097/ico.0000000000000998
29. Yotsukura E, Torii H, Inokuchi M, et al. Current Prevalence of Myopia and Association of Myopia With Environmental Factors Among Schoolchildren in Japan. JAMA Ophthal. 2019;137(11):1233–1239. doi:10.1001/jamaophthalmol.2019.3103
30. Hazra D, Yotsukura E, Torii H, et al. Relation between dry eye and myopia based on tear film breakup time, higher order aberration, choroidal thickness, and axial length. Sci Rep. 2022;12(1):10891. doi:10.1038/s41598-022-15023-x
31. Efron N, Jones L, Bron AJ, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the Contact Lens Interactions With the Ocular Surface and Adnexa Subcommittee. Invest Ophthalmol Visual Sci. 2013;54(11):TFOS98–TFOS122. doi:10.1167/iovs.13-13187
32. Wang X, Li J, Zhang R, et al. The Influence of Overnight Orthokeratology on Ocular Surface and Meibomian Gland Dysfunction in Teenagers with Myopia. J Ophthalmol. 2019;2019:5142628. doi:10.1155/2019/5142628
33. Cho WH, Fang PC, Yu HJ, Lin PW, Huang HM, Kuo MT. Analysis of tear film spatial instability for pediatric myopia under treatment. Sci Rep. 2020;10(1):14789. doi:10.1038/s41598-020-71710-7
34. Xie W, Zhang X, Xu Y, Yao YF. Assessment of Tear Film and Bulbar Redness by Keratograph 5M in Pediatric Patients After Orthokeratology. Eye Contact Lens. 2018;44(Suppl 2):S382–s386. doi:10.1097/icl.0000000000000501
35. Zhu Z, Zhang H, Yue J, Liu S, Li Z, Wang L. Antimicrobial efficacy of corneal cross-linking in vitro and in vivo for Fusarium solani: a potential new treatment for fungal keratitis. BMC Ophthalmol. 2018;18(1):65. doi:10.1186/s12886-018-0727-0
36. Moon JH, Kim KW, Moon NJ. Smartphone use is a risk factor for pediatric dry eye disease according to region and age: a case control study. BMC Ophthalmol. 2016;16(1):188. doi:10.1186/s12886-016-0364-4
37. Rattan S, Alrubaie A, Salih S, Abdalla S, Hussein S, Tariq F. A correlation between body mass index and refractive errors. Acta Facultatis Medicae Naissensis. 2023;40(2):199–207. doi:10.5937/afmnai40-40667
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.