Back to Journals » Clinical Ophthalmology » Volume 20
Correlation Between SUN Scale Grades and AS-OCT Cell Counts in Pediatric Uveitis: A Retrospective Central 7-Frame Analysis
Authors Ibrahim AS, Tam T, Zhou S, Puvanachandra N, Ibrahim LS, Injarie A
Received 16 November 2025
Accepted for publication 30 January 2026
Published 11 March 2026 Volume 2026:20 575712
DOI https://doi.org/10.2147/OPTH.S575712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ali S Ibrahim, Trevor Tam, Sean Zhou, Narman Puvanachandra, Lena S Ibrahim, Anas Injarie
Department of Ophthalmology, Norfolk and Norwich University Hospital, Norwich, NR4 7UY, UK
Correspondence: Ali S Ibrahim, Department of Ophthalmology, Norfolk & Norwich University Hospital, Norwich, NR4 7UY, UK, Email [email protected]
Purpose: This study evaluated the correlation between the Standardization of Uveitis Nomenclature (SUN) scale and anterior chamber cell counts measured by anterior segment optical coherence tomography (AS-OCT) in pediatric uveitis. We hypothesized that analyzing the central 7 frames of AS-OCT scans would improve measurement consistency and accuracy, as this region may provide greater anatomical relevance than peripheral frames, while also simplifying image acquisition in children.
Patients and Methods: One hundred and thirteen clinical episodes from pediatric uveitis patients aged ≤ 16 years, over 28 months, were retrospectively analyzed. All patients underwent AS-OCT imaging on the same day as clinical review. Only scans with ≥ 9 frames were included. SUN Scale grades were: 0 (n=49), 0.5+ (n=22), 1+ (n=17), 2+ (n=15), and 3+ (n=10). Mean anterior chamber cell counts were calculated from the central 7 frames. Spearman’s rank correlation assessed the relationship between SUN grades and AS-OCT counts; analyses were performed in R.
Results: There was a strong positive correlation between SUN Scale grades and mean AS-OCT cell counts (ρ = 0.933, 95% CI 0.89– 0.96, p < 0.001). Restricting analysis to the central seven frames improved measurement reproducibility and reduced exclusions due to patient movement or scan misalignment. Intra-grader repeatability of manual cell counts was excellent (ICC = 0.968, 95% CI 0.93– 0.99), confirming high measurement reliability.
Conclusion: AS-OCT, particularly when focusing on the central 7 frames, provides a consistent and reproducible method for quantifying anterior chamber inflammation in pediatric uveitis. This approach offers enhanced accuracy and operational feasibility, supporting its integration into clinical practice to improve monitoring and management in children.
Plain Language Summary: Uveitis is inflammation inside the eye that can cause permanent vision loss if not recognized and treated early. Doctors currently assess inflammation by using a slit-lamp microscope to directly count the number of inflammatory cells in the anterior chamber. This method depends on the ophthalmologist’s judgement and can vary between examiners, especially when the patient moves or the view is obscured.
Optical coherence tomography (OCT) is an imaging technique that provides detailed cross-sectional scans of the eye and can offer a more objective way to visualize these inflammatory cells. However, in children, OCT imaging can be difficult because of limited cooperation and movement during scanning.
Our study explored whether analyzing only the central seven frames of each OCT scan could make the examination faster and easier for children, while still giving reliable information about inflammation. We compared these OCT-based cell counts with the standard clinical grades determined by consultant ophthalmologists at the slit lamp.
The results showed a strong correlation between OCT cell counts and clinical grades, suggesting that this shortened OCT method could provide a more objective and child-friendly approach to assessing uveitis in clinical practice. This means it can be performed by trained technicians rather than only doctors, which could allow more frequent and accessible check-ups for children with uveitis. In the future, artificial intelligence could further automate this process, helping detect inflammation earlier and enabling faster treatment for high-risk patients.
Keywords: anterior chamber cells, quantitative imaging, ocular inflammation assessment, non-invasive diagnostics, pediatric ophthalmology
Introduction
Uveitis is a significant cause of visual impairment and blindness in children, with a prevalence of approximately 5–10 cases per 100,000 children annually.1,2 Characterized by inflammation of the uveal tract, it necessitates accurate assessment of anterior chamber inflammation for effective management. The Standardization of Uveitis Nomenclature (SUN) scale, commonly used to grade anterior chamber cells, often suffers from subjective variability, leading to inconsistent assessments.3,4 Previous studies have attempted to address these limitations by exploring alternative grading systems, but these efforts have not fully resolved the inherent subjectivity.5
The subjectivity and variability inherent in the SUN scale’s clinical grading system highlight significant challenges in accurately assessing anterior uveitis. Factors such as slit lamp optics, the degree of illumination, and the examiner’s skill can significantly affect the accuracy of anterior chamber cell counts, leading to considerable intra-observer and inter-observer variability. Moreover, the SUN scale’s non-linear, stepwise grading system may fail to detect small yet clinically meaningful changes in inflammation, particularly within the higher grades such as 2+, 3+, and 4+. For instance, the broader range of cell counts in these higher grades makes it difficult to classify improvements in inflammation, which could result in the underestimation of a therapy’s effectiveness in both clinical practice and research.
Given these limitations, there is a need for more objective, reliable methods to assess anterior chamber inflammation in pediatric uveitis patients. Anterior Segment Optical Coherence Tomography (AS-OCT) offers a more objective alternative, providing detailed quantification of anterior chamber cells, which is essential for managing pediatric uveitis.6–8 Anterior segment optical coherence tomography (AS-OCT) provides a valuable alternative when slit-lamp examinations are limited by corneal opacity or oedema, offering detailed, high-resolution imaging of anterior segment inflammation. In vivo cross-sectional imaging from AS-OCT is particularly useful in these scenarios, where direct visualization through traditional methods is challenging.9 Recent advancements in AS-OCT technology have improved its axial resolution and consistency, reinforcing its role in both clinical and research settings.10 By providing a more precise assessment of anterior chamber inflammation, AS-OCT enables tailored treatment adjustments that may support early immunomodulatory agents and ultimately improve visual outcomes.11 Nevertheless, anterior segment optical coherence tomography is not without limitations, as accurate cell quantification may be challenging in the presence of dense corneal opacities, and differentiation between inflammatory cells and other hyper-reflective elements such as pigment dispersion or cellular debris can be difficult.
Anterior segment optical coherence tomography has previously been explored as a non-contact imaging method in evaluating the anterior segment of the pediatric population, noting its utility in cases where patient cooperation is limited.12 However, despite its proven diagnostic value, gaps remain regarding the repeatability of AS-OCT-derived metrics in pediatric populations with patient movement being a confounding factor.13 Our study hopes to address this gap by exclusively analyzing the central 7 frames of AS-OCT scans, based on the hypothesis that the central anterior chamber may offer greater anatomical relevance and more stable imaging conditions, potentially improving consistency. Focusing solely on these frames simplifies the imaging process, particularly beneficial for children who may struggle to remain still for prolonged periods. Additionally, restricting the analysis to 7 central frames would reduce the time required for cell counting, enhancing clinical feasibility without compromising on diagnostic value.
Our study examines the correlation between clinical assessment of AC cells through the SUN scale grades and AS-OCT cell counts from the central 7 frames.
Materials and Methods
Study Design
This retrospective observational study aimed to evaluate the correlation between SUN Scale grades and anterior chamber cell counts measured by AS-OCT in pediatric uveitis patients.
Participants
The study included 113 clinical episodes in pediatric uveitis patients aged 16 or under. Inclusion criteria required that patients had regular uveitis screenings and underwent AS-OCT imaging on the same day as their clinical review. Only AS-OCT scans containing a minimum of 9 frames were included in the analysis. The study was carried out in accordance with local General Data Protection Regulation (GDPR) guidelines and the principles of the Declaration of Helsinki.
Ethical approval requirements were reviewed by the Research Operations Office at the Norfolk and Norwich University Hospital, which confirmed that formal Research Ethics Committee review was not required.
Data Collection
Standardization of Uveitis Nomenclature (SUN) Scale grades were documented from clinical notes following examination by a single pediatric consultant ophthalmologist. This was conducted at Norfolk and Norwich University Hospital, a UK secondary care teaching hospital. Patients were identified from pediatric ophthalmology clinics managing pediatric uveitis, with anterior segment optical coherence tomography performed as part of routine clinical care. Imaging episodes included in the analysis were collected between April 2023 and June 2024. Anterior segment optical coherence tomography imaging was performed using the Spectralis optical coherence tomography system (Heidelberg Engineering, Heidelberg, Germany), configured with the anterior segment module.14 Each AS-OCT scan consisted of a volumetric raster of 9–48 consecutive B-scans. The central seven B-scans (“frames”) were selected for analysis to represent the most stable and anatomically relevant portion of the anterior chamber, with the central frame identified as the one corresponding to the largest visible diameter of the pupil. A representative example of one of the central frames from the AS-OCT scan is shown in Figure 1. The device provides an axial resolution of 3.9 µm and a lateral resolution of 5.7 µm, with a scan depth of up to 16.6 mm, enabling detailed cross-sectional visualization of anterior chamber structures.14 A separate doctor, blinded to SUN Scale grades, manually performed cell counts to ensure objectivity and reduce bias. Image settings, including contrast, brightness and gamma, were not adjusted during analysis. Cells were counted using the original image parameters as captured at the time of acquisition, ensuring consistency and preventing visual bias during manual grading.
 |
Figure 1 Representative anterior segment optical coherence tomography (AS-OCT) image demonstrating inflammatory cells within the anterior chamber. Discrete hyper-reflective dots correspond to inflammatory cells. |
For each eye, the mean anterior chamber cell count was calculated by averaging manual counts from the central 7 frames. While individual frame counts varied as expected with physiological heterogeneity within the anterior chamber, averaging across multiple frames reduced random variability and provided a stable representative mean for each scan.
A cell was defined as a discrete, well-circumscribed hyperreflective dot within the anterior chamber on AS-OCT. Tiny, faint specks without clear borders were excluded to minimize misclassification, as these features may represent image noise, pigment dispersion, cellular debris, or motion artefact rather than true inflammatory cells. Counts were performed for each of the central 7 frames and the mean value across these frames was calculated for each scan.
Statistical Analysis
The Shapiro–Wilk test confirmed that the total anterior chamber cell count was not normally distributed (p < 0.05). Additional analysis revealed high skewness (2.57) and kurtosis (6.63), indicating a positively skewed distribution with heavy tails. Consequently, non-parametric statistical methods were applied.
Despite this, mean values were used rather than median values to summarize inflammatory burden per imaging episode, as cell counts were averaged across seven central frames to reflect overall cell load rather than a single-frame estimate.
Spearman’s rank correlation was used to assess the relationship between SUN Scale grades and mean cell counts. All statistical analyses were conducted using R software, with statistical significance set at p < 0.05.
To assess intra-grader repeatability, 25 anonymized AS-OCT scans were randomly selected and recounted by the same examiner six months after the initial grading. The intraclass correlation coefficient (ICC) for consistency was calculated using a two-way mixed-effects model. An ICC value above 0.9 was considered indicative of excellent reliability.
Results
Descriptive Statistics
We included 27 patients (113 clinical episodes) aged 3–16 years (median 10, interquartile range 4), of whom 17 were female (63%) and 10 were male (37%). The most common underlying diagnosis was juvenile idiopathic arthritis (JIA), followed by idiopathic uveitis and a single case of Blau syndrome. A total of 113 eye examinations were analyzed, comprising 32% male and 68% female eyes, with 45 right eyes and 68 left eyes. These represented the entire cohort of pediatric anterior uveitis patients seen at our centre during the study period.
Full demographic and diagnostic characteristics at both patient and eye level are summarized in Table 1.
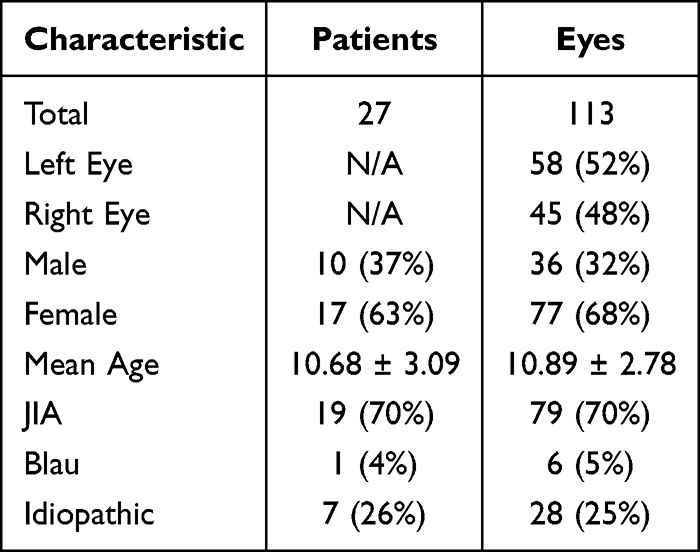 |
Table 1 Demographic and Disease Summary at Patient and Eye Levels |
SUN Scale grades ranged from 0 to 3+, with grade 0 representing 43% of episodes. SUN Scale Grades 0.5+, 1+, 2+ and 3+ were progressively less frequent, and no episodes were graded as 4+. A full breakdown is provided in Table 2.
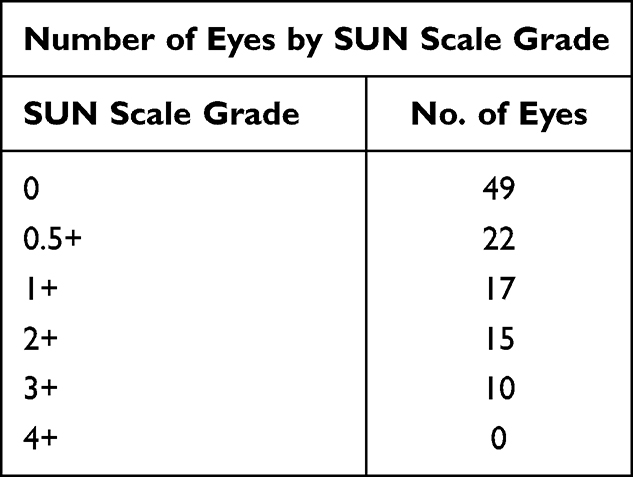 |
Table 2 Distribution of Eyes by SUN Scale Grade |
Correlation Analysis
The Spearman’s rank correlation coefficient between SUN Scale grades and mean AS-OCT cell counts was 0.933 (95% CI 0.89–0.96, p < 0.001), indicating a strong positive correlation. The progressive increase in mean AS-OCT cell counts with higher SUN grades is shown in Figure 2, and the distribution and variability of mean AS-OCT cell counts across SUN grades are illustrated in Figure 3.
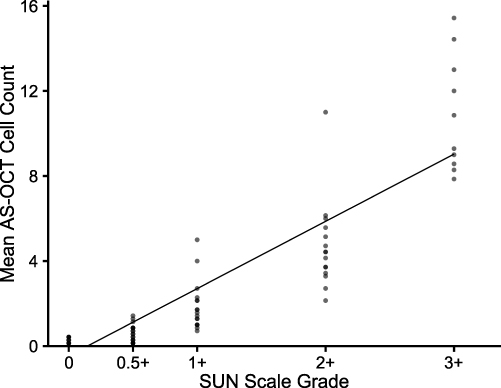 |
Figure 2 Relationship between mean anterior segment optical coherence tomography (AS-OCT) cell count and clinical Standardisation of Uveitis Nomenclature (SUN) scale grade. Each point represents an individual imaging episode. |
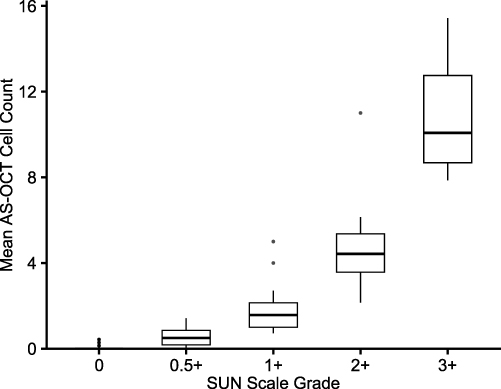 |
Figure 3 Box-and-whisker plot showing the distribution of mean anterior chamber cell counts measured on anterior segment optical coherence tomography (AS-OCT) across Standardisation of Uveitis Nomenclature (SUN) scale grades. Boxes represent the interquartile range with the median indicated; whiskers denote the range, and points indicate outliers. |
Intra-grader repeatability was excellent, with an ICC of 0.968 (95% CI 0.93–0.986, p < 0.001), demonstrating strong consistency between repeated measurements over a six-month interval.
Discussion
This study demonstrated a positive correlation between SUN scale grades and mean anterior chamber cell counts obtained by manually counting from AS-OCT images in pediatric uveitis patients. The exclusive focus on the central 7 frames of AS-OCT scans proved to be an effective approach, particularly in the challenging context of scanning a pediatric population. Despite the inherent difficulties associated with this demographic, strong correlations in the assessment of anterior chamber inflammation were still obtained, underscoring the effectiveness of this method. If an 11-frame analysis had been used, approximately 25–30% of scans would have been excluded due to a combination of non-centralized imaging and variability in total frame numbers (ranging from 9 to 48). This variability meant that identifying 11 true central frames was not always possible. By concentrating on the central 7 frames, we were able to include 113 of the 121 AS-OCT scans available to us, avoiding unnecessary exclusions and highlighting the practicality and reliability of this focused method in achieving consistent and meaningful clinical results.
In this study, AS-OCT demonstrated a high agreement with SUN Scale (98%) for detecting anterior chamber inflammation, with only 1 false negative identified – a case graded 0.5+ on the SUN scale. This low rate of false negatives is crucial in the context of pediatric uveitis, where missing a case of inflammation can delay treatment and lead to more severe outcomes. The ability of AS-OCT to accurately detect inflammation in nearly all cases supports its use as a reliable screening tool. As there is no objective gold standard for anterior chamber inflammatory activity, and both slit-lamp SUN grading and manual AS-OCT cell quantification involve observer-dependent interpretation, performance metrics such as sensitivity should be interpreted with caution. We therefore reported agreement relative to clinical SUN grading rather than true diagnostic sensitivity.
To confirm the robustness of manual AS-OCT cell counting, intra-grader repeatability was assessed on a random subset of scans regraded several months later by the same examiner. The results demonstrated excellent consistency between repeated measurements, supporting the reproducibility of the manual counting approach and reinforcing the reliability of the 7-frame method for quantifying anterior chamber inflammation.
However, 11 false positives were identified where AS-OCT detected inflammation that the SUN scale did not. These cases had very low mean cell counts (0.14–0.29), suggesting possible subclinical inflammation below the detection threshold of slit-lamp examination. Without longitudinal follow-up, it is unclear whether these cases would have progressed to a clinical flare or represented artefacts. While false positives may lead to additional follow-ups, the potential for early intervention in genuine cases could still outweigh the risk of unnecessary treatment. In the future, such findings could form the basis of a protocol whereby patients with low-grade AS-OCT activity but no clinical signs are recalled earlier for repeat imaging, allowing progression to be detected sooner.
The findings of this study align with previous research that has also reported strong correlations between AS-OCT cell counts and clinical inflammation activity however, many prior studies did not specifically focus on the central frames of the AS-OCT scans.12,13,15 The strong correlation observed in this study may be attributed to the use of higher resolution cornea scans and/or the targeted analysis of the central 7 frames, which likely provided a more accurate reflection of anterior chamber inflammation by reducing the variability introduced by peripheral frames.
Tsui et al demonstrated that both single-line and eight-line radial AS-OCT acquisition protocols yield comparable results when quantifying anterior chamber cells in children with uveitis, confirming the overall feasibility of AS-OCT for pediatric inflammatory assessment16 However, their analysis compared acquisition modes rather than within-scan consistency, and relied on single-frame measurements that are highly sensitive to small positional or motion artefacts. In addition, their protocol required repeated acquisitions when scans were unclear due to motion or corneal reflex artefacts, which limits real-world applicability in young or uncooperative children. In contrast, our study used the Heidelberg Spectralis anterior-segment module, which offers higher image resolution and scan density than the Optovue system used by Tsui et al, enabling more detailed visualization of the anterior chamber16 Our frame-based averaging approach struck a balance between reducing peripheral distortion and frame-to-frame variability, allowing reliable analysis without the need for repeated scanning. While a strong overall correlation was observed, partial overlap remained between the 1+ and 2+ SUN categories. This pattern likely reflects increased inflammatory cell density at higher grades, which facilitates clearer discrimination between true inflammatory cells and background artefact on AS-OCT, whereas sparse cell counts at lower grades approach the detection limits of both slit-lamp examination and OCT, resulting in greater overlap. This effect is also reported by Tsui et al, which likely reflects not only biological and imaging variability but also the inherent subjectivity and non-linearity of the SUN scale grading system itself.16
The results suggest that AS-OCT, particularly with a focus on the central 7 frames, can serve as a valuable tool in the clinical assessment of pediatric uveitis. This approach offers more consistent and objective measurements of anterior chamber inflammation, which could improve the reliability of clinical evaluations and enhance patient outcomes. The findings support the routine integration of AS-OCT into pediatric uveitis management, especially in cases where traditional slit lamp examinations are hindered by factors such as corneal opacity or patient non-cooperation.
In addition to its clinical value, AS-OCT offers significant patient-centered benefits. By providing clear visual evidence of anterior chamber inflammation, AS-OCT enhances patient understanding and engagement in their care. This visual clarity often leads to better treatment compliance, as patients can see the direct impact of their therapies, such as a reduction in inflammation. Moreover, AS-OCT can alleviate anxiety by offering reassurance through visible confirmation of disease status, whether showing improvement or stability. This transparency reduces uncertainty, particularly in pediatric patients, where clear communication is essential.
The use of AS-OCT by trained non-medical personnel could significantly reduce waiting times and ease the burden on clinicians. This could streamline the screening and diagnostic process while maintaining a high level of agreement and reliability in detecting and monitoring anterior chamber inflammation, especially in resource-limited settings. Future studies could explore inter- and intra-grader variability between ophthalmologists and trained non-medical personnel to formally evaluate the consistency of AS-OCT cell counting and its potential for wider clinical deployment.
This study’s limitations include the uneven distribution of episodes across SUN scale grades, with a notable absence of data for higher SUN grades, which may affect the generalizability of the findings. Additionally, the exclusive focus on the central 7 frames of AS-OCT scans, while beneficial for repeatability, may overlook inflammatory activity occurring in the peripheral frames. The relatively small number of eyes at higher grades of inflammation (+3 and +4 SUN ACC) is a common limitation in studies of anterior uveitis, reflecting the “real-world” distribution of disease severity.15 Another key limitation of this study is its cross-sectional design, which captures data at a single point in time. This approach limits our ability to assess how AS-OCT measurements and SUN Scale grades correlate over time or respond to treatment. Longitudinal studies are needed to evaluate the utility of AS-OCT for monitoring disease progression, treatment response and long-term outcomes in pediatric uveitis. Future research should focus on repeated AS-OCT measurements to better understand their role in ongoing patient management.
While the overall correlation was strong, a degree of overlap was observed between SUN grades +1 and +2, with corresponding AS-OCT cell counts showing limited separation. This likely reflects the narrow numeric range between these SUN categories (6–25 mean cell count) and the inherent variability of slit-lamp grading rather than a limitation of AS-OCT itself. The continuous nature of OCT quantification may in fact, offer a more physiologically accurate measure of inflammation. Future studies with larger datasets and more balanced grade distributions could further clarify whether AS-OCT can reliably distinguish these intermediate disease states.
Etherton et al investigated the use of AS-OCT for both quantitative and qualitative assessment of anterior chamber inflammation in childhood uveitis13 Their findings highlight the potential for future integration of artificial intelligence in AS-OCT analysis, with algorithms capable of automatically identifying and quantifying inflammatory markers. Similarly, Pillar et al demonstrated the feasibility of fully automated cell quantification using swept-source AS-OCT and deep-learning models, showing strong agreement with manual grading and clinical activity scores15 However, only 7% of eyes in their cohort had inflammation graded 2+ or above, limiting generalizability to more active disease. These developments collectively point toward a future in which automated AS-OCT analysis could reduce the variability and time demands of manual grading, support earlier detection, and enable more personalized treatment as well as potentially extending to community-based screening programmes.
Future research should also explore the development of a dedicated AS-OCT scanning protocol tailored specifically for anterior uveitis. A predefined preset, similar to the focused 7-frame method used in this study could improve consistency, reduce acquisition time and simplify interpretation. This would be particularly beneficial in pediatric settings, where patient cooperation can be limited. The integration of automated cell quantification within such a protocol could further streamline the diagnostic process and eliminate reliance on subjective clinical grading altogether.
Building on these developments, future studies may also consider creating a new classification system that combines AS-OCT-derived metrics with the SUN scale. A joint AS-OCT-SUN framework could enhance diagnostic precision and longitudinal monitoring. Validation in larger and more diverse patient cohorts particularly among those with higher SUN grades will be necessary to confirm its effectiveness in clinical practice.
Conclusion
This study demonstrates a strong and statistically significant positive correlation between SUN scale grades and mean cell counts measured by AS-OCT in pediatric uveitis patients. The use of only the central 7 frames of the AS-OCT scans, combined with blinding of the doctor performing the cell counts strengthens the robustness of these findings by reducing the risk of bias.
These findings support the use of AS-OCT as an objective method for assessing pediatric anterior uveitis which may enhance the reliability of clinical evaluations and improve patient outcomes, particularly in children who may often be asymptomatic at disease onset and exacerbations or children who are uncooperative during clinical examinations. However, this highlights the need for longitudinal studies validating its role in disease and treatment monitoring.
Data Sharing Statement
The data supporting the findings of this study are derived from patient records and OCT imaging at Norfolk and Norwich University Hospital. Due to patient confidentiality and data protection regulations, the data are not publicly available. De-identified data may be available from the corresponding author upon reasonable request.
Ethical Considerations
This study was conducted in accordance with the tenets of the Declaration of Helsinki and local GDPR regulations. The project involved analysis of anonymised imaging data collected as part of routine clinical care, so individual informed consent was not required.
Prior to commencing the work, the Research Operations Office at the Norfolk and Norwich University Hospital (NNUH) reviewed the proposal and confirmed that it did not require formal review by a Research Ethics Committee.
The NHS Health Research Authority / NIHR “Is My Study Research?” toolkit was also completed, and it indicated that the project did not require formal ethics committee review.
Disclosure
Mr Sean Zhou reports personal fees for educational supports from Roche and Bausch and Lomb. He is also the director of Intelligent MedPrep, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gentile P, Ragusa E, Bolletta E, et al. Epidemiology of pediatric uveitis. Ocul Immunol Inflamm. 2023;31(10):2050–9. doi:10.1080/09273948.2023.2271988
2. Solebo AL, McLoone E, Petrushkin H, et al. Incidence, sociodemographic and presenting clinical features of childhood non-infectious uveitis: findings from the UK national inception cohort study. Br J Ophthalmol. 2025:
3. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. results of the first international workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
4. Oo HH, Mohan M, Song W, et al. Anterior chamber inflammation grading methods: a critical review. Surv Ophthalmol. 2024;69(2):253–264. doi:10.1016/j.survophthal.2023.10.005
5. de Smet MD, Haim-Langford D, Neumann R, et al. Tarsier anterior chamber cell grading: improving the SUN grading scheme with a visual analog scale. Ocul Immunol Inflamm. 2022;30(7–8):1686–1691. doi:10.1080/09273948.2021.1934036
6. Li Y, Lowder C, Zhang X, Huang D. Anterior chamber cell grading by optical coherence tomography. Invest Ophthalmol Vis Sci. 2013;54(1):258. doi:10.1167/iovs.12-10477
7. Invernizzi A, Marchi S, Aldigeri R, et al. Objective quantification of anterior chamber inflammation. Ophthalmology. 2017;124(11):1670–1677. doi:10.1016/j.ophtha.2017.05.013
8. Sharma S, Lowder CY, Vasanji A, Baynes K, Kaiser PK, Srivastava SK. Automated analysis of anterior chamber inflammation by spectral-domain optical coherence tomography. Ophthalmology. 2015;122(7):1464–1470. doi:10.1016/j.ophtha.2015.02.032
9. Regatieri CV, Alwassia A, Zhang JY, Vora R, Duker JS. Use of optical coherence tomography in the diagnosis and management of uveitis. Int Ophthalmol Clin. 2012;52(4):33–43. doi:10.1097/IIO.0b013e318265d439
10. Shan J, DeBoer C, Xu BY. Anterior segment optical coherence tomography: applications for clinical care and scientific research. Asia-Pac J Ophthalmol. 2019;8(2):146–157. doi:10.22608/APO.201910
11. Sharon Y, Goren L, Barayev E, Neumann R, Chu DS, Kramer M. Recurrent and chronic anterior uveitis: long-term outcome and treatment strategies. Indian J Ophthalmol. 2023. doi:10.4103/IJO.IJO_1042_23
12. Cauduro RS, Do A FC, Morales MSÁ, et al. Application of anterior segment optical coherence tomography in pediatric ophthalmology. J Ophthalmol. 2012;2012:1–6. doi:10.1155/2012/313120
13. Etherton K, Rahi JS, Petrushkin H, et al. Quantitative and qualitative assessment of anterior segment optical coherence tomography capture of disease state in childhood anterior uveitis. Br J Ophthalmol. 2023;107(7):966–972. doi:10.1136/bjophthalmol-2021-320448
14. Engineering H. SPECTRALIS Technical Data Sheet. 2021. Available from: https://arfamex.com/wp-content/uploads/2021/12/200279-002-INT-AE18_SPECTRALIS-Technical-Data-Sheet_EN.pdf.
15. Pillar S, Kadomoto S, Chen K, et al. Automated quantification of anterior chamber cells using swept-source anterior segment optical coherence tomography. J Ophthalmic Inflamm Infect. 2025;15(1):3. doi:10.1186/s12348-025-00456-y
16. Tsui E, Chen JL, Jackson NJ, et al. Quantification of anterior chamber cells in children with uveitis using anterior segment optical coherence tomography. Am J Ophthalmol. 2022;241:254–261. doi:10.1016/j.ajo.2022.05.012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.