Back to Journals » International Journal of Women's Health » Volume 17
Correlation Between Serum and Urine β-hCG in Gestational Trophoblastic Neoplasia: A Step Toward Non-Invasive Disease Monitoring
Authors Kurniadi A ![]() , Kusuma AY, Permadi W, Winarno GNA
, Kusuma AY, Permadi W, Winarno GNA ![]() , Hidayat YM
, Hidayat YM ![]() , Erfiandi F
, Erfiandi F ![]() , Kireina J
, Kireina J
Received 1 April 2025
Accepted for publication 27 August 2025
Published 21 November 2025 Volume 2025:17 Pages 4737—4743
DOI https://doi.org/10.2147/IJWH.S531752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Andi Kurniadi, Aria Yusti Kusuma, Wiryawan Permadi, Gatot Nyarumenteng Adhipurnawan Winarno, Yudi Mulyana Hidayat, Febia Erfiandi, Jessica Kireina
Department of Obstetrics and Gynaecology, Faculty of Medicine Universitas Padjajaran – Dr Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Andi Kurniadi, Department of Obstetrics and Gynaecology, Faculty of Medicine, Universitas Padjajaran – Dr Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +6281220286197, Email [email protected]
Purpose: Gestational Trophoblastic Neoplasia (GTN) are malignant trophoblastic proliferations requiring accurate monitoring to guide treatment and assess disease progression. Serum β-hCG is the standard biomarker for GTN monitoring, but it requires blood collection, which can be invasive and resource-intensive. Urinary β-hCG testing offers a non-invasive alternative, but its clinical reliability in GTN patients remains unclear. This study evaluates the correlation between urinary and serum β-hCG levels in GTN patients, aiming to determine the feasibility of urine β-hCG as a reliable non-invasive monitoring tool.
Patients and Methods: A cross-sectional study was conducted at Dr. Hasan Sadikin General Hospital, Bandung, from June 2024 to February 2025, involving 31 patients diagnosed with GTN. A total of 86 paired serum and urine β-hCG samples were analyzed using enzyme-linked immunosorbent assay (ELISA). Data normality was assessed using the Kolmogorov–Smirnov test. Pearson’s correlation and simple linear regression were used to evaluate the relationship between serum and urine β-hCG levels.
Results: Serum β-hCG levels were significantly higher than urine levels (P < 0.001), but a strong positive correlation was observed between the two (r = 0.985, P < 0.001), with a coefficient of determination (r2 = 96.9%).
Conclusion: Urinary β-hCG exhibits a strong correlation with serum β-hCG in GTN patients, supporting its potential as a non-invasive monitoring tool. However, hydration status, renal function, and possible assay interferences should be considered. Combining serum and urine β-hCG measurements remains the optimal approach for accurate disease monitoring.
Keywords: gestational trophoblastic neoplasia, β-hCG, urine β-hCG, serum β-hCG, tumor monitoring, non-invasive biomarker
Introduction
Gestational trophoblastic disease (GTD) is a spectrum of benign and malignant disorders arising from abnormal trophoblastic proliferation. Gestational Trophoblastic Neoplasia (GTN) include invasive moles, choriocarcinoma, placental site trophoblastic tumors (PSTT), and epithelioid trophoblastic tumors (ETT).1 Accurate diagnosis and monitoring are essential, as 15% to 20% of hydatidiform mole cases progress to malignancy, necessitating chemotherapy.2
GTN incidence varies globally, with higher rates reported in Asia compared to Western countries. The incidence of choriocarcinoma ranges from 2.4 to 4 per 100,000 deliveries in Western nations but reaches 9.2 per 40,000 pregnancies in Southeast Asia.3,4 A 2021 study in West Java reported that GTN constituted 64.64% of GTD cases.5 Despite historical high mortality rates, early detection and improved management have significantly increased survival rates.1
Human chorionic gonadotropin (hCG) is a glycoprotein hormone composed of two subunits—alpha and beta—and is secreted by trophoblastic tissues. It is considered as a key biomarker in GTD management, with β-hCG playing a crucial role in diagnosis, prognosis, and treatment monitoring. Unlike normal pregnancy, where hCG will predictably decline postpartum, β-hCG remains elevated in GTD, indicating tumor activity.6
GTD monitoring can be performed through both serum and urine β-hCG tests. Serum β-hCG is widely used due to its sensitivity, but it requires invasive blood collection, trained personnel, and access to laboratory facilities—factors that can make it less feasible in low resource or remote settings. In contrast, urine β-hCG testing offers a non-invasive and more accessible alternative. Although both serum and urine β-hCG assays sometimes utilize the same immunoassay platforms in many tertiary care centers—resulting in comparable test charges— the overall cost of serum testing is often higher in low-resource settings due to the need for venipuncture supplies, trained phlebotomists, and sterile collection materials. This makes urine testing a more practical, non-invasive, and cost-effective alternative for GTD monitoring in settings with limited healthcare resources. Additionally, urine β-hCG testing avoids false-positive results caused by heterophilic antibodies, a limitation of serum assays.7
However, we must also consider the biological and biochemical characteristics of hCG and the sample matrices themselves that can contribute to variability in results between serum and urine β-hCG tests. There are several molecular forms of hCG, including: (1) intact hCG, (2) free β-subunit, (3) hyperglycosylated hCG (hCG-H), (4) nicked hCG, and (5) β-core fragment—each differs in structure, biological activity, and clearance.6 While intact hCG and free β-subunit are typically detected by both serum and urine assays, the presence of fragmented or modified forms such as β-core fragments and hyperglycosylated hCG can vary significantly between blood and urine.8 These molecular differences influence how various assays detect hCG and can eventually affect the correlation between serum and urine hCG titers, particularly in patients with malignant forms of trophoblastic disease, where hyperglycosylated or fragmented hCG predominates.
Furthermore, physiological factors can also influence how β-hCG appears in serum versus urine. Serum β-hCG reflects immediate hormonal production and circulates in a relatively stable, controlled environment. In contrast, urine β-hCG levels are influenced by renal filtration, hydration status, and urinary concentration, which may delay or dilute hCG appearance. Additionally, differences in sample handling and degradation of hCG fragments in urine can contribute to variability.9
Despite these potential variables, studies in general obstetric populations have suggested a strong correlation between urine and serum hCG levels.10–13 However, evidence in patients with GTN—a population in which hCG dynamics can differ significantly—is sparse. Understanding this correlation in GTN is essential for validating urine hCG as a reliable monitoring tool, particularly in resource-limited settings where access to venipuncture and laboratory support is restricted.
This study aims to fill that gap by evaluating the correlation between urinary and serum β-hCG levels in GTN patients at Dr. Hasan Sadikin General Hospital. As a major referral center in West Java, the hospital provides an optimal setting for evaluating the potential of urine β-hCG testing as a reliable, non-invasive alternative for patient management. Findings from this study may contribute to refining GTN monitoring protocols and improving accessibility to post-treatment surveillance, especially in resource-limited settings.
Materials and Methods
This is a cross-sectional study conducted at the Oncology Clinic of Department of Obstetrics and Gynecology, Dr. Hasan Sadikin General Hospital, Bandung from June 2024 to February 2025. This study included patients diagnosed with Gestational Trophoblastic Neoplasia (GTN), defined as the malignant spectrum of gestational trophoblastic disease (GTD), including invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumors (ETT). Patients with benign hydatidiform mole were not included in the analysis. All participants were diagnosed based on clinical findings, β-hCG levels, and histopathological confirmation when available.
We studied patients undergoing post-molar evacuation monitoring and treatment. Urine and serum β-hCG samples were collected at the same visit, either prior to initiation of chemotherapy or during scheduled follow-up visits in patients undergoing treatment. Samples were excluded if they were taken during spontaneous resolution of molar pregnancy without evidence of malignancy. Other exclusion criteria included patients with incomplete medical records, known kidney or thyroid disorders (which could affect β-hCG metabolism and excretion), loss to follow-up, or voluntary withdrawal from the study.
We measured urine and serum β-hCG levels using enzyme-linked immunosorbent assay (ELISA) method at the Clinical Pathology Laboratory of Dr. Hasan Sadikin General Hospital. Standardized protocols were followed to ensure analytical accuracy and minimize inter-sample variability.
Statistical analysis was performed using the Kolmogorov–Smirnov test. Normally distributed data were analyzed with paired t-test to compare urine and serum β-hCG levels, while non-normally distributed data were assessed using Wilcoxon signed-rank test. The correlation between urine and serum β-hCG levels was evaluated using Pearson’s correlation test for normally distributed data or Spearman’s rank correlation test for non-normally distributed data. Additionally, simple linear regression analysis was performed to assess the predictive relationship between the two variables. A significance level of p < 0.05 was considered statistically significant.
Result
There were 31 patients included in this study, with a total of 86 samples. Patient characteristics, serum β-hCG levels, and urine β-hCG levels were analyzed. Table 1 presents the demographic and clinical characteristics of the study population. The median age of the study subjects was 39 years (range: 21–52 years). Most patients were in stage 1 GTN (n=19, 61.3%), with a relatively even distribution between low-risk (n=16, 51.6%) and high-risk (n=15, 48.4%) FIGO scores. Chemoresistance was observed in 25.8% (n=8) of cases.
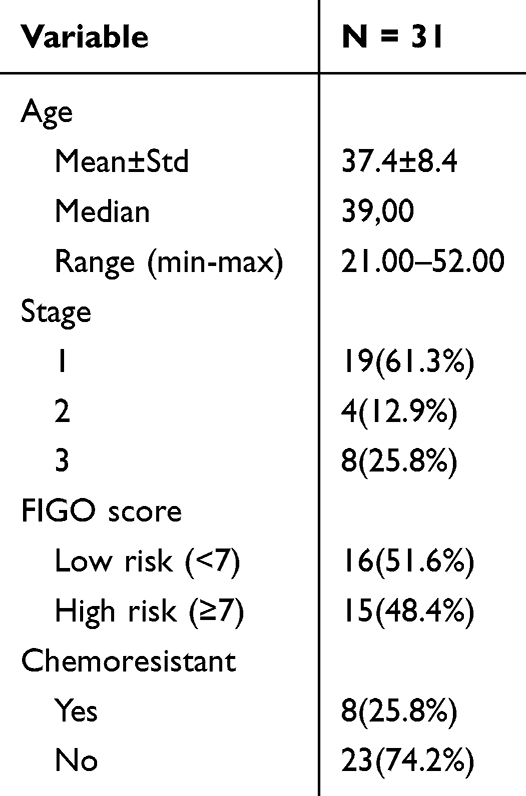 |
Table 1 Characteristics of Study Subjects |
A total of 86 blood and urine β-hCG samples were analyzed. Table 2 presents both blood and urine β-hCG levels of study population. The mean β-hCG level in blood was 1,530.6 IU/L (range: 2.3–28,564.5 IU/L), while mean urine β-hCG level was 400.01 IU/L (range: 0.15–7,090.9 IU/L). The Kolmogorov–Smirnov normality test indicated that both variables were not normally distributed (P<0.001), necessitating logarithmic transformation. Post-transformation, the data met normality assumptions (p=0.159 for blood, p=0.537 for urine) (Table 2).
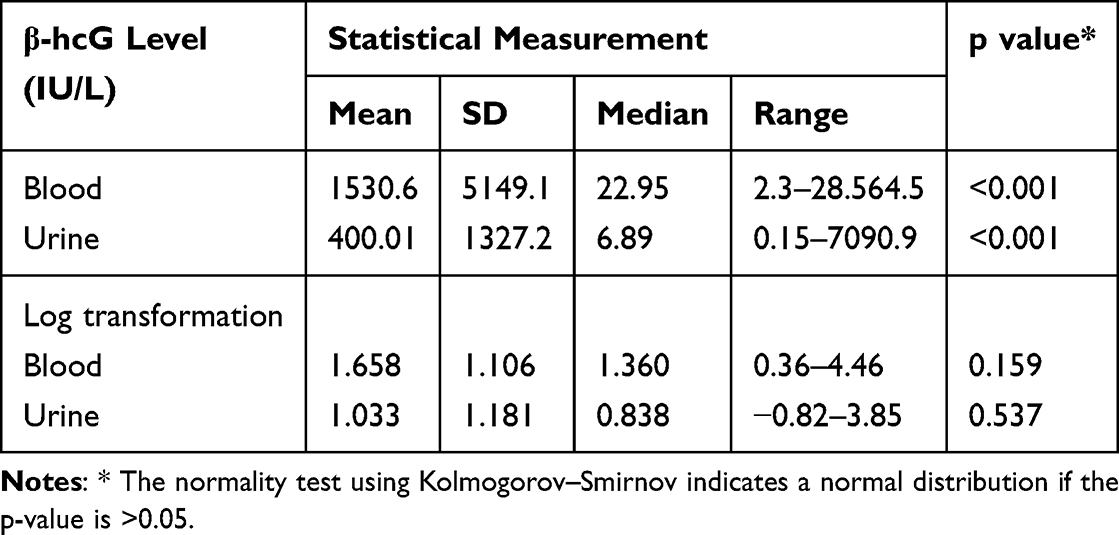 |
Table 2 Overview of β-hCG Levels in Blood and Urine |
We found a significant difference between β-hCG levels in blood and urine (P<0.001) as shown in Table 3. We then performed Pearson correlation test and found a strong positive correlation (r = 0.985, P < 0.001) between β-hCG levels in blood and urine, with a coefficient of determination (r2 = 96.9%), as detailed in Table 4 and Figure 1.
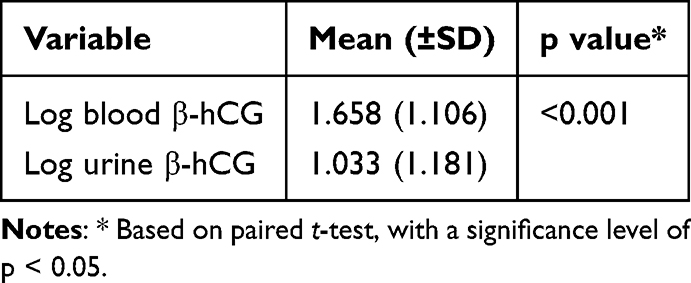 |
Table 3 Comparison of β-hCG Levels in Blood and Urine |
 |
Table 4 Correlation Between β-hCG Levels in Blood and Urine in Patients with Gestational Trophoblastic Neoplasia |
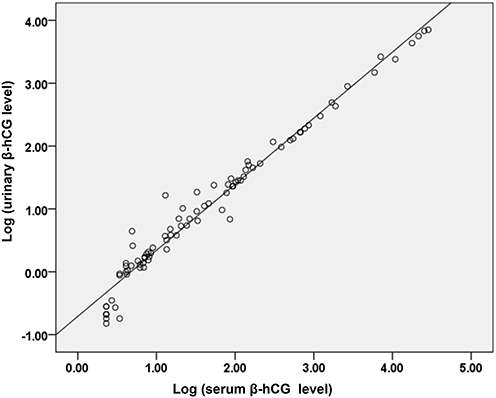 |
Figure 1 Correlation between β-hCG levels in blood and urine. |
Simple linear regression yielded the equation:
Log(β-hCG blood) = 0.706 + 0.922 * log(β-hCG urine)
The coefficient of determination (R2 = 96.9%) suggests that blood β-hCG levels explain 96.9% of the variance in urine β-hCG levels, with 3.1% attributable to other factors. These findings highlight the strong correlation between serum and urine β-hCG levels in GTN patients, supporting the potential role of urine β-hCG as an alternative monitoring tool.
Discussion
This study aims to evaluate the correlation between urinary and serum β-hCG levels specifically in patients with Gestational Trophoblastic Neoplasia (GTN). While similar studies have been conducted in pregnant women, none have specifically assessed this correlation in GTN patients.9
Gestational Trophoblastic Neoplasia (GTN) is a malignant type of Gestational Trophoblastic Disease (GTD), occurring weeks to years after pregnancy.6 Despite a global decline in incidence due to improved early detection, the prevalence remains relatively high in Asia (~2 per 1000 pregnancies).1 There were 31 GTN cases identified in our study, with a mean patient age of 38 years, most diagnosed at FIGO stage 1 (63%) and classified as low-risk (51.6%). These findings align with studies by Yamamoto et al (Japan) and Kong et al (China), which reported similar patient demographics and disease distribution.14,15
GTN is highly sensitive to chemotherapy, with 74.2% of patients in this study responding without chemoresistance. Comparable results were observed in Singhai et al’s (India) study, where most patients were low-risk (51.7%), though chemoresistance was paradoxically more common in low-risk patients (28.4%). Factors such as tumor size, pre-treatment β-hCG levels, age, metastatic status, and FIGO stage influence chemoresistance.14 Interestingly, this study found chemoresistant patients had lower β-hCG levels and were in earlier stages, mirroring findings by Strohl et al (USA, 2016).16
β-hCG is the gold standard biomarker for diagnosing and monitoring GTN, typically measured weekly in serum for the first year, followed by urine-based testing in long-term follow-up (as practiced at Charing Cross Hospital, London).17 The need for continuous β-hCG monitoring is essential, as persistently high or rising levels indicate possible disease progression or chemoresistance.
In this study, the correlation between serum and urine β-hCG was strong (r = 0.985), though urinary β-hCG levels were consistently lower than serum levels, likely due to renal clearance, hydration status, and urine sample timing. This aligns with Bobdiwala et al, who demonstrated that creatinine-adjusted urinary β-hCG closely mirrored serum levels in pregnancy-related conditions.18 Morning urine samples are generally recommended due to peak hCG concentrations, but in this study, urine samples were collected randomly, potentially introducing variability.7
Additionally, renal function and hydration status influence urinary β-hCG accuracy. Gockley et al (1994–2015 study) showed that factors like obesity, BMI, and hormonal contraception impact hCG regression dynamics, though not significantly affecting clinical monitoring.19 Future research should explore how renal clearance variability affects urinary β-hCG interpretation in GTN patients.
While both serum and urine β-hCG testing offers its own advantages, they are not without limitations. False-positive serum β-hCG results can occur due to heterophile antibodies (phantom hCG), as seen in Usui et al (Japan, 2024), where a post-molar patient had persistently elevated serum β-hCG but negative urine results.20 Urine β-hCG can thus help differentiate true trophoblastic disease from assay interference.
Conversely, false-negative urine β-hCG results can arise due to the prozone effect (hook effect), where excessively high hCG saturates antibodies, leading to undetectable levels. This occurs when overwhelming concentrations of β-hCG saturate both the capture and tracer antibodies in immunoassays, leading to signal reduction and subsequent false-negative findings.8,21 Sah et al (Nepal, 2024) reported a case of false-negative urine β-hCG despite high serum levels, underscoring the importance of combined serum and urine testing in GTD diagnosis and follow-up.22
Another factor influencing urinary β-hCG levels is chemotherapy, particularly methotrexate-based regimens, which influences β-hCG levels by inducing tumor cell apoptosis. Furthermore, methotrexate toxicity can also impact renal clearance, potentially altering urinary β-hCG measurements. This is supported by a research by Hamed et al, which found that high-dose methotrexate can cause nephrotoxicity, necessitating folinic acid rescue (leucovorin) to mitigate toxicity effects.16,23
Given these limitations, many referral centers (as highlighted by Joyce et al, Lukinovic et al) choose to use both serum and urine β-hCG for optimal monitoring.24,25 This is particularly relevant in perimenopausal women, those with ovarian failure, germ cell tumors, or exogenous hCG exposure (eg, fertility treatments, bodybuilding drugs), where false positives can complicate diagnosis.20,24
Our study provides strong evidence supporting urine β-hCG as a reliable alternative to serum β-hCG for GTN monitoring, especially in resource-limited settings where repeated serum testing may not be feasible. However, the need for standardized urinary β-hCG cutoffs remains a challenge. Another limitation of this study is the relatively short enrolment period (8 months), which may affect the generalizability of the findings. As this was a single-center study, the sample reflects the referral pattern and case volume of our institution during that specific timeframe. Larger multicenter studies with longer enrolment durations would be beneficial to validate these findings.
Conclusion
We found a strong correlation between serum and urinary β-hCG levels in GTN patients, suggesting that urinary β-hCG could serve as a non-invasive alternative for long-term disease monitoring. However, factors such as hydration status, renal function, and potential assay interference must be considered to optimize diagnostic accuracy. Combining serum and urine β-hCG measurements remains the best approach for accurate disease assessment and monitoring. Future studies involving larger, multicenter cohorts and longitudinal designs are needed to validate these findings and to assess the utility of urine β-hCG in GTN monitoring.
Data Sharing Statement
Anonymised data are available upon reasonable written request to the corresponding author.
Ethical Approval
The study was conducted according to the Declaration of Helsinki. Ethical approval of this study was granted by the Health Research Ethics Committee of Dr Hasan Sadikin Hospital Bandung with approval number: DP.04.03/D.XIV.6.5/384/2024.
Patient Consent
Written informed consent was obtained from all study participants prior to engaging in any study-related procedures. The participant data were anonymised and their confidentiality was maintained.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jagtap SV, Aher V, Gadhiya S, Jagtap SS. Gestational trophoblastic disease - clinicopathological study at Tertiary Care Hospital. J Clin Diagn Res. 2017;11(8):EC27–EC30. doi:10.7860/JCDR/2017/27232.10458
2. Shaaban AM, Rezvani M, Haroun RR, et al. Gestational trophoblastic disease: clinical and imaging features. RadioGraphics. 2017;37(2):681–700. doi:10.1148/rg.2017160140
3. Amalina MAF, Wang SM, AL-Naggar RA, Thanikasalam K. Epidemiology of gestational choriocarcinoma: a systematic review. OALib. 2023;10(03):1–11. doi:10.4236/oalib.1109923
4. Nasr AMA, Ahmed YAM, Gafar AAM, et al. Prevalence and risk factors of Choriocarcinoma in Saudi Arabia: a systematic review. Clin Cancer Investig J. 2022;11(6):4–8. doi:10.51847/nczqkf18st
5. Ramadhan MB, Salima S, Kurniadi A, Winarn GNA, Harsono AB. Profil dan Karakteristik Penderita tumor Trofoblas gestasional di RSUP Dr. Hasan Sadikin Periode 2021. Indones J Obstet Gynecol Sci. 2022;5(2):296. doi:10.24198/obgynia/v5n2.380
6. Williams A. Differential diagnosis of elevated human chorionic gonadotropin in women. Case Rep Women’s Heal. 2023;37:e00471. doi:10.1016/j.crwh.2022.e00471
7. Oyatogun O, Sandhu M, Barata-Kirby S, Tuller E, Schust DJ. A rational diagnostic approach to the “phantom hCG” and other clinical scenarios in which a patient is thought to be pregnant but is not. Ther Adv Reprod Heal. 2021;15:26334941211016412. doi:10.1177/26334941211016412
8. Herskovits AZ, Chen Y, Latifi N, Ta RM, Kriegel G. False-negative urine human chorionic gonadotropin testing in the clinical laboratory. Lab Med. 2019;51(1):86–93. doi:10.1093/labmed/lmz039
9. Bobdiwala S, Harvey R, Abdallah Y, et al. The potential use of urinary hCG measurements in the management of pregnancies of unknown location. Hum Fertil. 2020;25(2):256–263. doi:10.1080/14647273.2020.1777590
10. Lertkhachonsuk R. Quantitative urine hCG and urine pregnancy test in gestational trophoblastic disease patients with low hCG titer. J Med Assoc Thai. 2015;98(Suppl 1):S36–41.
11. Gnoth C, Johnson S. Strips of hope: accuracy of home pregnancy tests and new developments. Geburtshilfe Frauenheilkd. 2014;74(7):661–669. doi:10.1055/s-0034-1368589
12. Norman RJ, Menabawey M, Lowings C, Buck RH, Chard T. Relationship between blood and urine concentrations of intact human chorionic gonadotropin and its free subunits in early pregnancy. Obstet Gynecol. 1987;69(4):590–593.
13. Anderson J, Ghaffarian KR. Early pregnancy diagnosis. In: StatPearls. StatPearls Publishing; 2023.
14. Yamamoto E, Nishino K, Niimi K, Ino K. Epidemiologic study on gestational trophoblastic diseases in Japan. J Gynecol Oncol. 2022;33(6):e72–e72. doi:10.3802/jgo.2022.33.e72
15. Kong Y, Zong L, Cheng H, et al. Management and risk factors of recurrent gestational trophoblastic neoplasia: an update from 2004 to 2017. Cancer Med. 2020;9(7):2590–2599. doi:10.1002/cam4.2901
16. Strohl AE, Lurain JR. Postmolar choriocarcinoma: an independent risk factor for chemotherapy resistance in low-risk gestational trophoblastic neoplasia. Gynecol Oncol. 2016;141(2):276–280. doi:10.1016/j.ygyno.2016.02.014
17. NHS. Molar pregnancy clinic guide for clinicians Gestational trophoblastic disease (GTD) service at Charing Cross Hospital; 2016. Available from: https://www.imperial.nhs.uk/~/media/website/services/cancer-services/gestational-trophoblastic-disease/gtd-clinic-guide-for-clinicians.pdf?la=en.
18. Parker VL, Winter MC, Tidy JA, et al. PREDICT-GTN 1: can we improve the FIGO scoring system in gestational trophoblastic neoplasia? Int J Cancer. 2023;152(5):986–997. doi:10.1002/ijc.34352
19. Gockley AA, Lin LH, Davis M, et al. Impact of clinical characteristics on human chorionic gonadotropin regression after molar pregnancy. Clinics. 2021;76:e2830. doi:10.6061/CLINICS/2021/E2830
20. Usui H, Sato A, Katayama E, Nakamura N, Koga K. A phantom human chorionic gonadotropin in the case of molar pregnancy. Oxford Med Case Rep. 2024;2024(5):omae038–omae038. doi:10.1093/omcr/omae038
21. Anderson Z, Larson E, Khan M, Bell M. False negative urine pregnancy testing with complete molar pregnancy: an example of the hook effect. S D Med. 2016;69(2):55–57.
22. Sah SK, Shah P, Sherpa AD. False low beta-hCG in a complete hydatidiform molar pregnancy: a case of hook effect. Med Phoenix. 2024;9(1):41–43. doi:10.3126/medphoenix.v9i1.67256
23. Hamed KM, Dighriri IM, Baomar AF, et al. Overview of methotrexate toxicity: a comprehensive literature review. Cureus. 2022;14(9):e29518–e29518. doi:10.7759/cureus.29518
24. Joyce CM, Fitzgerald B, McCarthy TV, Coulter J, O’Donoghue K. Advances in the diagnosis and early management of gestational trophoblastic disease. BMJ Med. 2022;1(1):e000321–e000321. doi:10.1136/bmjmed-2022-000321
25. Lukinovic N, Malovrh EP, Takac I, Sobocan M, Knez J. Advances in diagnostics and management of gestational trophoblastic disease. Radiol Oncol. 2022;56(4):430–439. doi:10.2478/raon-2022-0038
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.