Back to Journals » Local and Regional Anesthesia » Volume 19
Correlation Between Injected Volume and Cranial Spread in Broad-Aged Pediatric Caudal Anesthesia: A Retrospective Ultrasound-Guided Study
Authors Tsai FF ![]() , Hsieh MH, Huang HH, Liu CM
, Hsieh MH, Huang HH, Liu CM
Received 19 August 2025
Accepted for publication 22 January 2026
Published 13 February 2026 Volume 2026:19 561773
DOI https://doi.org/10.2147/LRA.S561773
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Stefan Wirz
Feng-Fang Tsai,1 Ming-Han Hsieh,2 Hsing-Hao Huang,1 Chih-Min Liu1
1Department of Anesthesiology, National Taiwan University Hospital, Taipei, Taiwan, Republic of China; 2Department of Anesthesiology, Taipei City Hospital Ho-Ping Branch, Taipei, Taiwan, Republic of China
Correspondence: Chih-Min Liu, Department of Anesthesiology, National Taiwan University Hospital, No. 7, Zhongshan S. Road, Zhongzheng District, Taipei, 10002, Taiwan, Republic of China, Tel +886 2 23123456 #62158, Email [email protected]
Purpose: Caudal block remains a standard regional anesthesia technique for pediatric lower abdominal and lower limb surgeries. The conventional weight-based Armitage formula does not consider patient body habitus, which can lead to under- or over-dosing—especially in lean or obese children. Ultrasound guidance permits visualization of epidural spread and may facilitate individualized dosing.
Patients and Methods: In this retrospective single-center study, anesthetic records of 25 pediatric patients (age 10– 106 months) undergoing ultrasound-guided caudal blocks for lower abdominal or lower extremity surgery were analyzed. Volumes of 0.25% levobupivacaine required to achieve cranial spread to vertebral levels S1, L2 and L1 were recorded. Univariate and multivariate linear regression models, incorporating weight, height, age, and BMI, were compared using adjusted R2, mean squared error (MSE), Akaike information criterion (AIC), and Bayesian information criterion (BIC) to determine the most predictive dosing formulae.
Results: Univariate regression revealed injected volume correlated strongest with weight: for S1 spread, volume = 0.1458 × weight (kg) (p = 0.006); for L2 spread, volume = 0.4898 × weight (kg) (p = 0.0079). The optimal multivariate model for S1-level spread combined weight and height: Volume (mL) = 0.1741 × weight (kg) − 0.0234 × height (cm) (adjusted R2 = 0.1369; lowest AIC/BIC). For L2-level spread, a weight-only model (volume = 0.5339 × weight [kg]) provided the best fit (adjusted R2 = 0.2112). Both models predicted lower volumes than the traditional Armitage guideline, reducing the likelihood of excessive cephalad spread.
Conclusion: In pediatric caudal anesthesia, a dosing formula that uses both weight and height improves prediction of the volume required for S1-level blocks, whereas a weight-based formula is adequate for L2-level spread. Real-time ultrasound guidance enhances procedural accuracy and safety by confirming epidural spread and detecting anatomical variation. These data support development of an individualized dosing nomogram for pediatric caudal anesthesia.
Keywords: pediatric, general anesthesia, caudal block, ultrasound
Introduction
Considering intra-operative and post-operative pain control in pediatric lower abdominal or lower extremity surgery, we usually combine general anesthesia and caudal block. Caudal block is a commonly used technique, especially in children younger than seven years of age. It has a favorable effect on reducing analgesic use perioperatively.1–3 The injected volume of caudal block was according to the Armitage formula (0.5 mL/kg: all sacral dermatomes are blocked; 1 mL/kg: all sacral and lumbar dermatomes are blocked; 1.25 mL/kg: the upper limit of anesthesia is at least mid-thoracic).4 However, the volume depends only on the body weight in this formula. Caudal blocks may be underdosed or overdosed in lean or obese children.
A caudal block is a commonly used pediatric epidural technique in which local anesthetic is injected into the caudal epidural space (via the sacro-coccygeal membrane/sacral hiatus) to provide analgesia for lower abdominal or lower-extremity surgery. Compared with the conventional caudal block, the number of needle punctures was lower, and the success rate of the first puncture was higher under ultrasound guidance.5,6 Otherwise, real-time ultrasound may also be helpful in estimating spread levels.7 Therefore, caudal block under ultrasound guidance is safer than traditional methods, and the level of drug spread may be assessed.8,9 Younger pediatric patients require a reduced dose for foot surgery,10 so we thus want to correlate the relationship between the injected volume and cranial spread. The aim of this retrospective case series study was to analyze the relationship between the injected volume and cranial spread level in pediatric caudal blocks.
Materials and Methods
This study was approved by the Research Ethics Committee of National Taiwan University Hospital (IRB/REC 201902050RINA). We respectfully requested a waiver of informed consent from Research Ethics Committee of National Taiwan University Hospital, Taipei City, Taiwan (R.O.C.) based on the following considerations: 1. This study is an observational study. During the retrospective collection of medical records, patient personal information (such as name and case number) was de-identified, and patient codes were re-edited before being analyzed with the collected medical records. Furthermore, “Application for Waiver of Informed Consent” was approved. The Ethics Committee’s official document also states, “IV. The Research Ethics Committee of this Institute agrees to waive informed consent for this case.”
This retrospective study was conducted by collecting medical and anesthetic records. Pediatric patients (ASA classification I–III) who underwent caudal block under ultrasound guidance for lower abdominal or lower extremity surgery between 2017/04/1-2018/12/31 were enrolled in this study. The exclusion criteria were as follows: (1) patients with extreme developmental (height or weight <3rd percentile or >97th percentile for age) and (2) abnormal congenital anatomy of the spine (eg, scoliosis).
The height and weight of the patients were recorded. Medical records in the operating room were collected, including electrocardiograms, non-invasive blood pressure, and pulse oximetry. General anesthesia was inducted by fentanyl (0.5~2mcg/kg), thiamylal sodium (4~8 mg/kg) and rocuronium bromide (0.6~1 mg/kg), in addition to adjunct medications atropine (0.01~0.02 mg/kg). A laryngeal mask airway was inserted for ventilation. Anesthesia was maintained using sevoflurane (MAC:1.0–1.5).
Spinal anatomy was identified via sonography using portable SonoSite X-Porte software 70.80.106.017 (FUJIFILM SonoSite Inc. Bothell, WA98021, USA), with a 38 mm wide 13–6 MHz linear array probe. According to the sonographic report, the 12th rib was identified to verify the spinous process of T12. The spinous processes of the L1–L5 and S1 vertebrae were also identified. After sterile preparation at the injection site, a 23G needle (BD PrecisionGlideTM, Becton, Dickinson and Company, NJ, USA) was inserted into the caudal epidural space through the sacrococcygeal membrane under real-time ultrasound guidance. After negative aspiration of blood, 0.25% chirocaine11 was injected manually at a rate of ~1 mL/3 seconds via ultrasound visualization. Real-time ultrasound showed progressive ventral epidural space distension as local anesthetic spread cephalad from the caudal epidural space (Figure 1). The injected chirocaine gradually widened the epidural space cranially). The patients’ medical records showed that chirocaine was injected into the epidural space, which gradually widened and extended cranially. The recorded injection volumes were documented at the points at which the widened epidural space reached S1, L2, and L1. The injection was discontinued when the epidural space at the first lumbar vertebra widened or when the total injected volume reached 1.25 mL/kg.
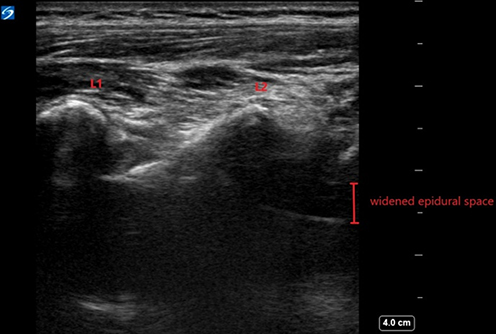 |
Figure 1 Image of the widened epidural space reached L2. Ultrasound imaging demonstrates widening of the ventral epidural space due to pooling of caudally injected local anesthetic; in some cases, the injectate accumulated at L2 without further cephalad progression to L1, resulting in epidural space expansion of approximately 4–5 mm. |
Statistics
Baseline characteristics are presented as means and standard deviations for continuous data and frequencies and percentages for categorical data. Univariate and multivariate linear regressions were used to estimate caudal block volume according to age, height, weight, and BMI. To determine the best fit of the models, we used the Akaike information criterion (AIC), Bayesian information criterion (BIC), and adjusted R2 values. All analyses were two-sided, and statistical significance was set at p < 0.05. Statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
This study enrolled 25 patients who underwent caudal block for scheduled lower abdominal or lower extremity surgery (Figure 2). Table 1 presents physical data obtained upon admission. The patients were aged between 10 and 106 months (average 54.2 ± 24.16 months). Patients’ height and weight were 100.6 ± 12.88 cm (75.0–121.3 cm) and 15.9 ± 4.45 kg (8.0–26.0 kg). The calculated BMI was 15.5±2.18 (10.4–20.82).
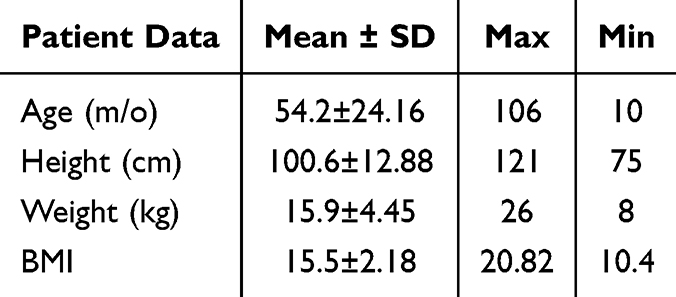 |
Table 1 Baseline Characteristics |
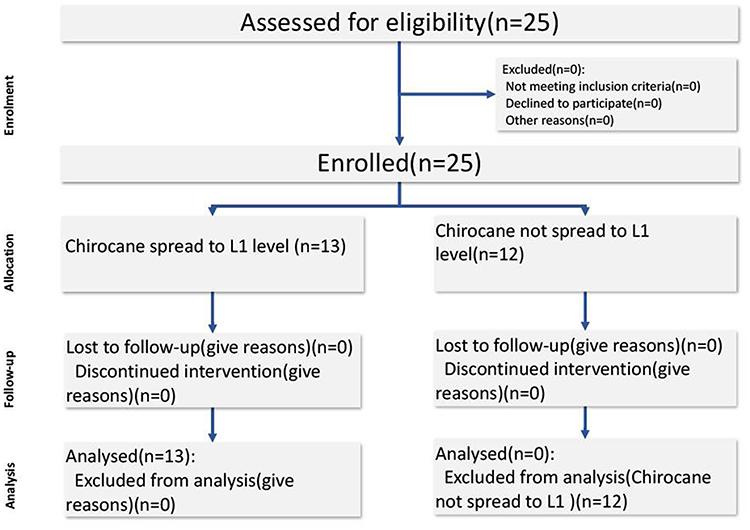 |
Figure 2 The inclusion flowchart. |
These 25 pediatric patients received real-time ultrasound guided caudal block; that is, they were successfully injected with local anesthetic (0.25% chirocaine) in the caudal epidural space. All of them reported chirocaine cranial spread to L2 level under ultrasound visualization. However, only 13 reported caudal injection was stopped due to Chirocaine spreading to L1 level before the 1.25mL/kg volume was achieved.
Univariate and multivariate linear regressions were used to estimate caudal block volume according to age, height, weight, and BMI. Table 2 shows the univariate analysis of S1 and L2 for the variables of interest in the 25 patients. We found that the injected volume was most correlated with weight. The injected volume reaching the S1 level was 0.1458 × weight (p=0.006), and the injected volume reaching L2 was 0.4898 × weight (p=0.0079). Figures 3 and 4 show that the linear regression of the volume estimated to reach S1 and L2 correlated with patient weight.
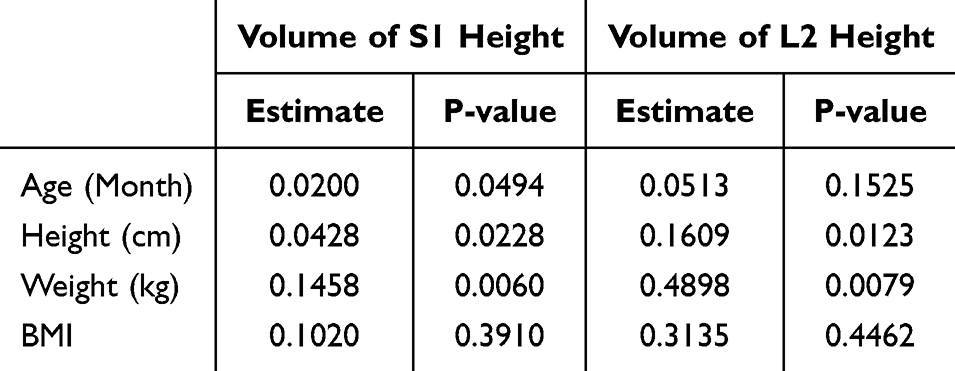 |
Table 2 Univariate Linear Regression Used to Estimate the Injected Volume Reached S1 and L2 |
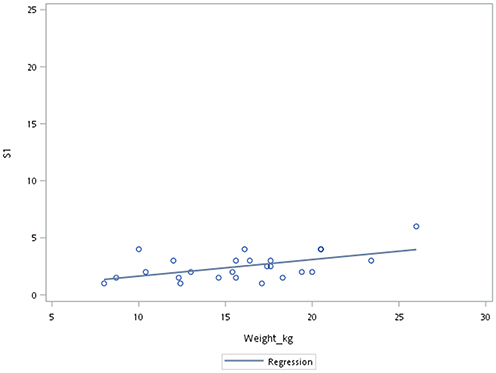 |
Figure 3 Dots were actually injected local anesthetic volume and weight. The line was linear regression of volume estimated to reach S1 correlated to weight. |
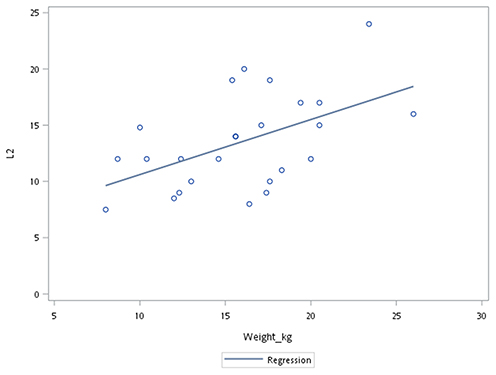 |
Figure 4 Dots were actually injected local anesthetic volume and weight. The line was linear regression of volume estimated to reach L2 correlated to weight. |
Thirteen patients were analyzed because chirocaine spread to the L1 level was confirmed using ultrasound. Table 3 shows the univariate analysis of S1, L2, and L1 for the variables of interest.
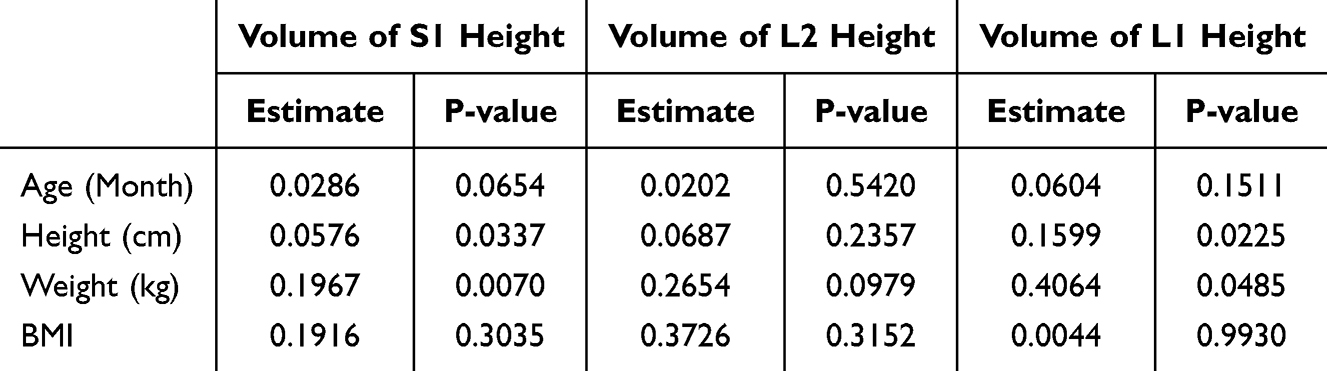 |
Table 3 Univariate Linear Regression Used to Estimate the Injected Volume Reached S1, L2 and L1 (Subgroup Analysis of 13 Patients) |
In this retrospective analysis, multivariable (combined weight with age, height, or BMI) linear regression models were developed to estimate the optimal volume of local anesthetic required for a pediatric caudal block, targeting specific cranial spread levels within the epidural space. Tables 4 and 5 show the multivariate linear regression used to estimate the adequate caudal block volume.
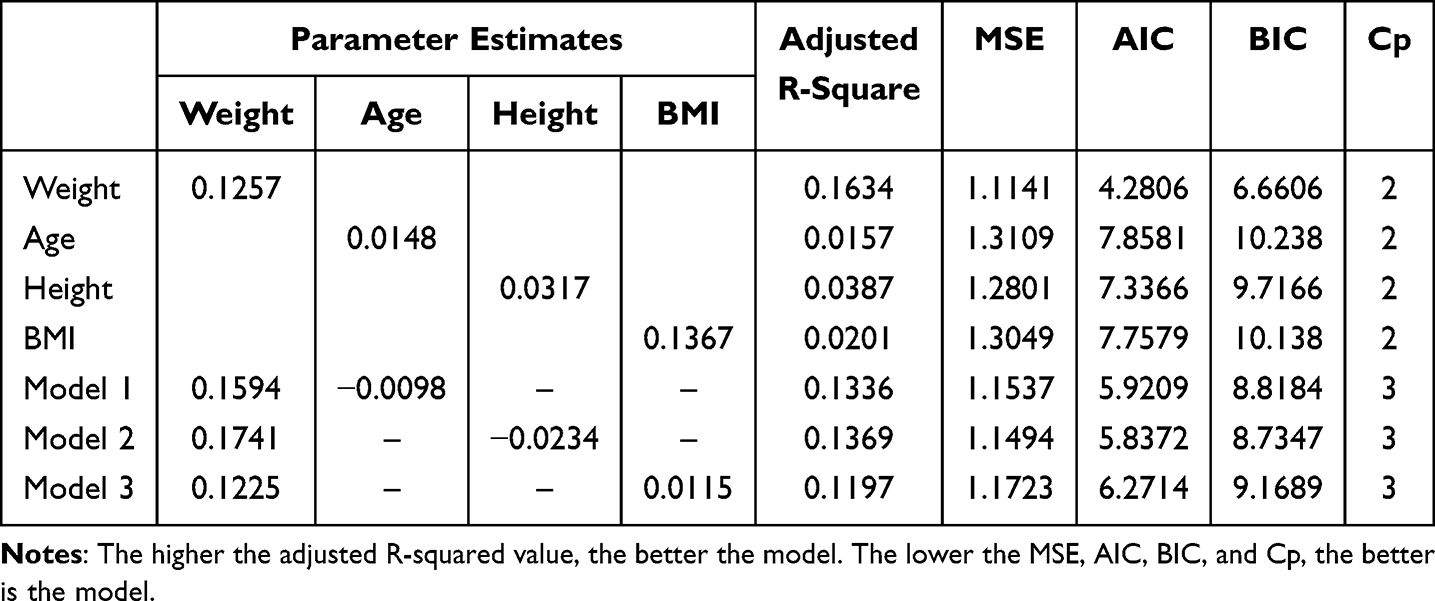 |
Table 4 Model Comparison of S1 Height |
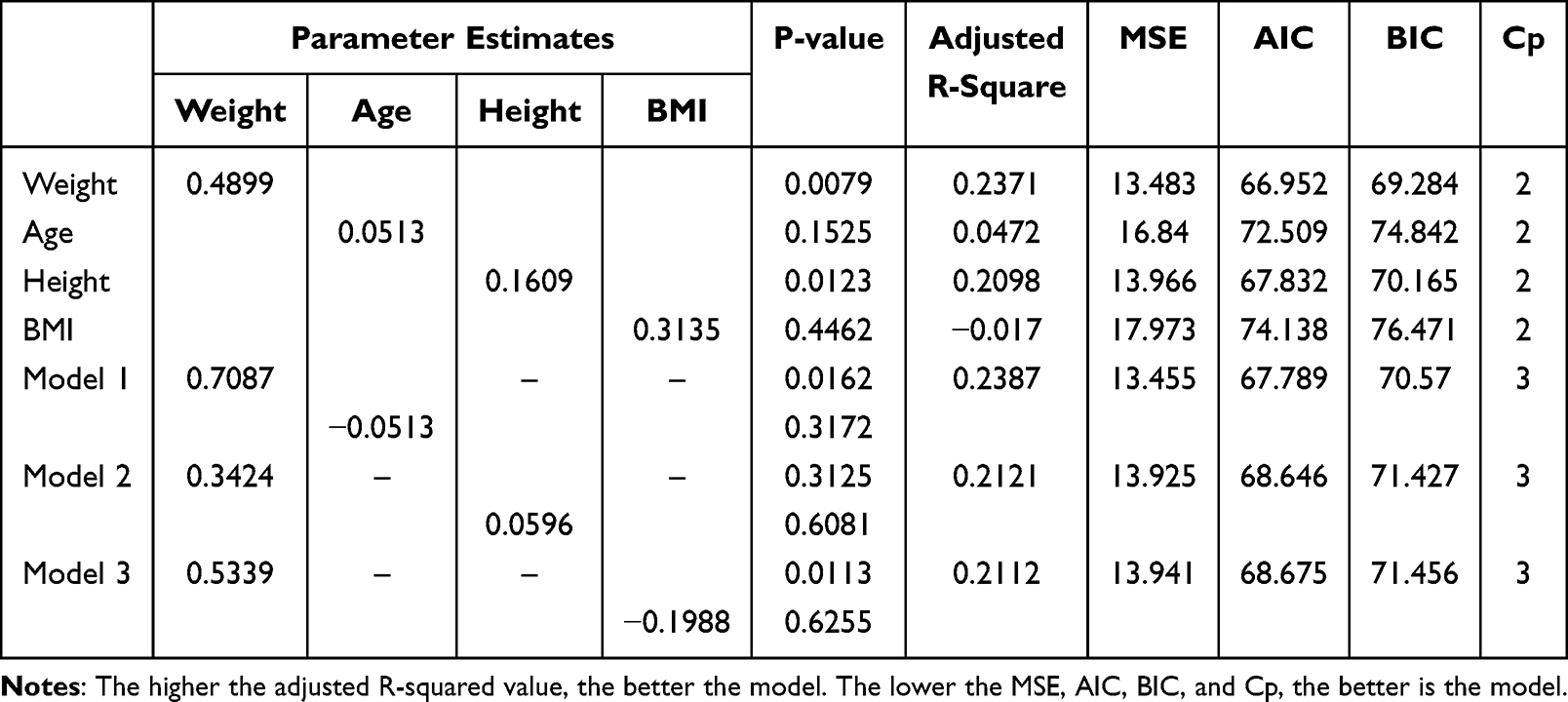 |
Table 5 Multivariable Linear Regression Used to Estimate the Injected Volume Reached L2 |
Considering the effect of age, in model 1 the volume needed to reach S1 height was 0.1594 times the patient’s weight. In model 2, it was 0.1741 times the patient’s weight after controlling for height. Finally, the volume to reach S1 height was 0.1225 times the weight of the patient if BMI was taken into account.
To achieve spread to the S1 vertebral level, the best-performing model (model 2) incorporated body weight and height as predictors. The resulting formula, estimated volume (mL) = 0.1741 × weight (kg) − 0.0234 × height (cm), demonstrated the most favorable statistical parameters with an adjusted R2 of 0.1369, a mean squared error (MSE) of 1.1494, and the lowest AIC and BIC values among the models tested.
For spread to the L2 vertebral level (Table 5), considering the effect of age, the volume needed to reach L2 height was 0.7087 times the patient’s weight. For model 2, the volume needed to reach L2 height was 0.3424 times the patient’s weight after controlling for height. Finally, the volume needed to reach L2 height was 0.5339 times the patient’s weight if BMI was taken into account. The optimal model was a simplified weight-based formula, with an estimated volume (mL) of 0.5339 × weight (kg).
Discussion
According to our univariate linear regression results, the traditional estimate of 0.5 mL/kg may lead to overdosing, especially in lean children. Patient’s weight should play the most important role in decision of injected volume at the lower level (S1); however, as volume increased, weight was not the only factor that affected it. This study suggests a meaningful improvement in predictive accuracy by accounting for patient height and weight. Our model showed the highest explanatory power (adjusted R2 = 0.2112) and maintained a relatively low MSE (13.941), offering both statistical robustness and practical applicability in clinical settings. These findings indicate that a weight-only model may suffice for predicting L2 level spread, whereas volume estimation for S1-level caudal blocks benefits from the inclusion of body height to enhance individual tailoring. Using a formula based on body weight, with a coefficient of approximately 0.15–0.22 depending on the population, offers more precise dosing to reach S1 level while minimizing the risk of spread beyond the target level.
Previous research10 has often focused on homogeneous cohorts, which may limit the generalizability of results. By including children with diverse body sizes and at different developmental stages, our findings are more representative of real-world pediatric anesthesia practice and offer wider clinical applicability. Notably, we utilized multivariate linear regression models to account for multiple patient variables (eg, weight and height), which significantly improved predictive accuracy over traditional univariate approaches or fixed weight-based formulas such as Armitage.12,13 This statistical strength enables the use of a more precise and individualized volume estimation strategy.
Real-time ultrasound observation of dural displacement confirmed the success of the caudal block. Failure of ultrasound observation may be due to suboptimal probe position or increased ossification of the vertebrae.14 Under real-time ultrasound guidance, we confirmed that the local anesthetic had been injected into the caudal epidural space, and determined cranial spread level by widening the epidural space. In children, ligamentum flavum visibility declined with increasing vertebral level and markedly decreased at the thoracic level in children.15 Because secondary spread of the caudal block may reach a higher spinal level after we stopped injecting local anesthetic and because of the difficulty of ultrasound visualization of the thoracic level, we observed dural displacement until L1 level was reached. However, only 13 of the 25 patients who received a caudal block with an injectate reached L1 level. Before reaching L1 level, the injected volume reached the upper limit (1.25 mL/kg) in the remaining 12 patients. One possible reason for this may be the horizontal intra-segmental redistribution.16 Additionally, we noticed soft tissue in the epidural space. Chirocaine spreading was blocked by soft tissue. In certain patients (Figure 5), the injectate pooled at the L2 level and did not advance to L1, producing a marked increase in epidural space width (approximately 4–5 mm). Figure 6 show a widened epidural space with soft tissue blocking cranial spread.
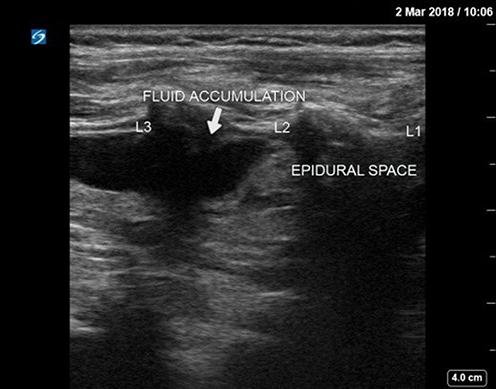 |
Figure 5 Longitudinal ultrasound image of the pediatric lumbar spine (L1–L3) during caudal epidural injection. The epidural space is visualized as a hypoechoic (black) band; cephalad is to the right and caudad to the left. Compared with the normal epidural space width (~1–2 mm), a small volume of injectate is seen accumulating between L2 and L3, resulting in mild widening of the epidural space. |
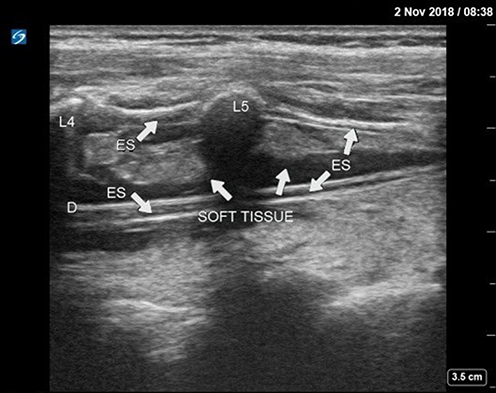 |
Figure 6 Longitudinal ultrasound image of the pediatric lumbar spine (L4–L5). The epidural space (ES) is seen as a gray band underneath to the dura mater (D); gray–hypoechoic soft tissue within the intrathecal space corresponds to the cauda equina. L4 and L5 indicate the respective spinous processes. |
Because chirocaine is of a similar intraoperative quality to racemic bupivacaine but has minimal hemodynamic variability and no significant complications, we chose it as the local anesthetic for caudal block. The speed of injection may or may not affect cranial spread level.17,18 It is difficult to maintain a steady rate by manually pushing the drug. However, push drugs with infusion pumps may encounter the problem of high pressures. High pressure may result from a thin extension line or soft-tissue blockage in the epidural space. According to most study designs, we attempted to push the drug manually at a rate of ~1 mL/3 sec.
In some cases, after injection of 1.25 mL/kg chirocaine, fluid accumulated below the soft tissue. It was predicted that the effect of caudal block may be limited,19 and we firmly believe that soft tissue in the epidural space caused variable cranial spread of the injected local anesthetic. Thus, real-time ultrasound guidance is necessary to ensure that cranial spread does not occur.
Moreover, the integration of real-time ultrasound guidance enhanced procedural precision and enabled direct visualization of the cephalad spread of the local anesthetic within the epidural space.20,21 This not only improved first-attempt success rates but also allowed for objective verification of block height, a common limitation in earlier studies relying on indirect clinical signs.22 Together, these advantages support the development of a practical nomogram for pediatric caudal anesthesia that is adaptable to diverse patient morphologies.
This study offers valuable insights into the optimization of caudal block volume estimation across a broad pediatric age spectrum, ranging from infants to adolescents. Unlike many previous studies that focused on narrow age groups,1,10 our analysis included children with a wide variety of body weights, heights, and developmental stages, thus enhancing the clinical applicability of the results to real-world pediatric anesthesia. The use of multivariate linear regression further strengthened our model’s predictive power, allowing for simultaneous consideration of key patient characteristics, such as weight and height. This approach outperformed traditional univariate models and weight-based formulas, such as the Armitage model, offering a more nuanced and individualized method for determining drug volume. The integration of real-time ultrasound imaging to directly observe epidural drug spread also enabled objective confirmation of the block level in addition to procedural reliability. These strengths collectively support the development of a tailored nomogram for volume prediction under caudal anesthesia, particularly suited for a heterogeneous pediatric population.
In this study, only 25 pediatric patients were enrolled. Some anesthesiologists performed caudal blocks under ultrasound guidance but only recorded the total local anesthetic dose they used or failed to trace the process of cranial spread. Additional patient data may have allowed our results to be more convincing. Moreover, this study’s single-center retrospective design and limited sample size constrain its external validity. Noting that power is likely inadequate for small-to-moderate associations in small group (n=13) and that the analysis should be interpreted cautiously. Future prospective multicenter trials are needed to validate the proposed volume prediction formula and to confirm its safety and effectiveness across broader populations.23
Conclusion
In conclusion, the volume required to inject the caudal block was less than the volume recommended using the Armitage formula. We recommend a chirocaine volume (mL) of 0.1741 × weight (kg) − 0.0234 × height (cm) to reach S1 level and, for S2 level, 0.5339 × weight (kg). In addition, real-time ultrasound guidance is necessary to ensure cranial spread level.
Acknowledgments
We acknowledge the support of the Clinical Trial Center Statistical Consulting Unit of the National Taiwan University Hospital, which provided the statistics for this study. We also thank our statistical analysts Shang-Jie Tsai and Yi-Chun Yeh for their assistance with data analysis and manuscript preparation. We also express gratitude to George Jun-Jia Chen for assisting in the editing and formatting of images.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Wiegele M, Marhofer P, Lönnqvist PA. Caudal epidural blocks in paediatric patients: a review and practical considerations. Br J Anaesth. 2019;122(4):509–9. doi:10.1016/j.bja.2018.11.030
2. Villalobos MA, Veneziano G, Miller R, et al. Evaluation of postoperative analgesia in pediatric patients after Hip surgery: lumbar plexus versus caudal epidural analgesia. J Pain Res. 2019;12:997–1001. doi:10.2147/JPR.S191945
3. Alizadeh F, Heydari SM, Nejadgashti R. Effectiveness of caudal epidural block on intraoperative blood loss during hypospadias repair: a randomized clinical trial. J Pediatr Urol. 2018;14(5):420.e1–420.e5. doi:10.1016/j.jpurol.2018.03.025
4. Armitage EN. Caudal block in children. Anaesthesia. 1979;34:396.
5. Karaca O, Pinar HU, Gokmen Z, Dogan R. Ultrasound-guided versus conventional caudal block in children: a prospective randomized study. Eur J Pediatr Surg. 2019;29:533–538. doi:10.1055/s-0038-1676980
6. Adler AC, Belon CA, Guffey DM, Minard CG, Patel NV, Chandrakantan A. Real-time ultrasound improves accuracy of caudal block in children. Anesth Analg. 2019;129:1761–1766. doi:10.1213/ANE.0000000000004341
7. Shin S, Kim JY, Kim WO, Kim SH, Kil HK. Ultrasound visibility of spinal structures and local anesthetic spread in children undergoing caudal block. Ultrasound Med Biol. 2014;40(11):2630–2636. doi:10.1016/j.ultrasmedbio.2014.06.020
8. Wang LZ, Hu XX, Zhang YF, Chang XY. Randomized comparison of caudal block using sacral hiatus injection under ultrasound guidance with traditional sacral canal injection in children. Pediatr Anesth. 2013;23:395–400. doi:10.1111/pan.12104
9. Brenner L, Marhofer P, Kettner SC, et al. Ultrasound assessment of cranial spread during caudal blockade in children: effect of different volumes of local anesthetics. Br J Anaesth. 2011;107(2):229–235. doi:10.1093/bja/aer128
10. Kim HJ, Kim H, Lee S, Koh WU, Park SS, Ro Y. Reconsidering injection volume for caudal epidural block in young pediatric patients: a dynamic flow tracking experimental study. Reg Anesth Pain Med. 2024;49(5):355–360. doi:10.1136/rapm-2023-104409
11. Sharma J, Gupta R, Kumari A, Mahajan L, Singh J. A comparative study of 0.25% levobupivacaine, 0.25% ropivacaine, and 0.25% bupivacaine in paediatric single shot caudal block. Anesthesiol Res Pract. 2018;2018. doi:10.1155/2018/1486261
12. Jöhr M, Berger TM. Caudal blocks. Paediatr Anaesth. 2012;22(1):44–50. doi:10.1111/j.1460-9592.2011.03669.x
13. Greaney D, Everett T. Paediatric regional anaesthesia: updates in central neuraxial techniques and thoracic and abdominal blocks BJA educ. 2019;19(4):126–134. doi:10.1016/j.bjae.2018.12.003
14. Roberts SA, Guruswamy V, Galvez I. Caudal injectate can be reliably imaged using portable ultrasound—a preliminary study. Paediatr Anaesth. 2005;15:948–952. doi:10.1111/j.1460-9592.2005.01606.x
15. Kil HK, Cho JE, Kim WO, Koo BN, Han SW, Kim JY. Prepuncture ultrasound-measured distance: an accurate reflection of epidural depth in infants and small children. Reg Anesth Pain Med. 2007;32(2):102–106. doi:10.1016/j.rapm.2006.10.005
16. Lundblad M, Eksborg S, Lönnqvist PA. Secondary spread of caudal block as assessed by ultrasonography. Br J Anaesth. 2012;108(4):675–681. doi:10.1093/bja/aer513
17. Sen O, Donmez NF, Ornek D, Kalayci D, Arslan M, Dikmen B. Effects of epidural needle rotation and different speeds of injection on the distribution of epidural block. Rev Bras Anestesiol. 2012;62(6):852–862. doi:10.1016/S0034-7094(12)70185-X
18. Griffiths RB, Horton WA, Jones IG, Blake D. Speed of injection and spread of bupivacaine in the epidural space. Anaesthesia. 1987;42(2):160–163. doi:10.1111/j.1365-2044.1987.tb02990.x
19. Higuchi H, Adachi Y, Kazama T. Factors affecting the spread and duration of epidural anesthesia with ropivacaine. Anesthesiology. 2004;101:451–460. doi:10.1097/00000542-200408000-00027
20. Kao SC, Lin CS. Caudal epidural block: an updated review of anatomy and techniques. Biomed Res Int. 2017(2017):9217145. doi:10.1155/2017/9217145
21. Kil HK. Caudal and epidural blocks in infants and small children: historical perspective and ultrasound-guided approaches. Korean J Anesthesiol. 2018;71(6):430–439. doi:10.4097/kja.d.18.00109
22. Tsui BC, et al. Caudal epidural anesthesia: the effect of volume and dose on analgesia. Reg Anesth Pain Med. 2000;25(5):451–455.
23. Shawahna R, Jaber M, Maqboul I, et al. A multicenter survey of pediatric caudal epidural anesthesia practices in resource-limited settings. Sci Rep. 2025;15:16166. doi:10.1038/s41598-025-00275-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.