Back to Journals » Vascular Health and Risk Management » Volume 21
Correlation Between Activity Level of Renin-Angiotensin-Aldosterone System and Perfusion Index in Children with Postural Tachycardia Syndrome
Authors Zhang F ![]() , Pan J, Lin Z, Niu M
, Pan J, Lin Z, Niu M ![]()
Received 11 July 2025
Accepted for publication 24 October 2025
Published 6 November 2025 Volume 2025:21 Pages 927—936
DOI https://doi.org/10.2147/VHRM.S553129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Fengling Zhang, Jinyong Pan, Zhaotang Lin, Muqing Niu
Department of Pediatrics, The First Affiliated Hospital of Shihezi University, Shihezi, Xinjiang Uygur Autonomous Region, People’s Republic of China
Correspondence: Jinyong Pan, Department of Pediatrics, The First Affiliated Hospital of Shihezi University, Shihezi, Xinjiang Uygur Autonomous Region, People’s Republic of China, Email [email protected]
Objective: To evaluate the relationship between Renin-Angiotensin-Aldosterone System (RAAS) activity and Perfusion Index (PI) in children with Postural Tachycardia Syndrome (POTS), and to assess the diagnostic performance of Angiotensin II (AngII) and PI for POTS status.
Methods: A total of 65 children with POTS and 65 age- and sex-matched healthy controls were enrolled. Plasma renin, angiotensin I (AngI), AngII, and aldosterone were quantified via enzyme-linked immunosorbent assay, and PI was measured using a pulse oximetry-based monitor during head-up tilt testing. Statistical analyses included Receiver Operating Characteristic (ROC) curve analysis of AngII and PI for POTS status, binary logistic regression, and Pearson correlation.
Results: Compared to controls, children with POTS demonstrated a significantly lower PI (4.64 ± 1.54 vs 6.19 ± 1.64%; adjusted p < 0.005) and higher AngII levels (114.07 ± 7.69 vs 109.20 ± 10.44 pg/mL; adjusted p = 0.012). ROC analysis indicated that PI had a stronger diagnostic value (AUC = 0.753, 95% CI: 0.670– 0.836) than AngII (AUC = 0.654, 95% CI: 0.559– 0.749) in identifying POTS. In logistic regression, only PI remained an independent predictor of POTS (Odds Ratio = 0.577, 95% CI: 0.442– 0.755, p < 0.001). A significant inverse correlation was observed between AngII and PI (r = – 0.459, p < 0.001).
Conclusions: PI is a valuable, noninvasive clinical marker for POTS in children, demonstrating superior diagnostic utility compared to AngII. While elevated AngII retains clinical significance by reflecting underlying pathophysiology and disease severity, its independent predictive value is limited. The combined assessment of PI and AngII may enhance the pathophysiological understanding and management strategies for pediatric POTS.
Keywords: postural tachycardia syndrome in children, renin-angiotensin-aldosterone system, perfusion index
Introduction
Postural Tachycardia Syndrome (POTS) is one of the most common forms of Orthostatic Intolerance (OI) in children, accounting for approximately one-third of the causes of syncope in children. It is one of the main hemodynamic types of Neurally Mediated Syncope (NMS) in children and adolescents.1 The incidence of POTS in school-age children is high, about 6.8%. POTS is characterized by a rapid increase in heart rate (≥40 beats/min or ≥130 beats/min in children aged 6–12 years or ≥125 beats/min in adolescents aged 13–18 years) in the upright state, without a decrease in blood pressure (<20/10 mmHg). Most of them appear within 2.9–6.1 minutes after postural change.2
The Renin-Angiotensin-Aldosterone System (RAAS) plays a pivotal role in maintaining blood pressure and fluid homeostasis during postural changes by promoting vasoconstriction and increasing blood volume. Normally, standing triggers RAAS activation, resulting in the release of renin, formation of angiotensin II (AngII), and subsequent secretion of aldosterone, which together help preserve hemodynamic stability. However, in children with POTS, RAAS dysfunction—including impaired activation or an imbalance between the classic Angiotensin Converting Enzyme (ACE)—AngII -AngII Type 1 Receptor (AT1R) receptor axis vs ACE2-Ang (1–7)-Mas receptor axis-can lead to insufficient vasoconstriction and volume expansion during orthostatic stress, contributing to orthostatic intolerance and related symptoms.3
Perfusion Index (PI), a parameter obtained by non-invasive and continuous monitoring of pulse oximetry, is an indicator of peripheral blood flow perfusion, representing the ratio of pulsatile to nonpulsatile blood flow in peripheral tissues. It is regulated by the autonomic nervous system and can reflect the intensity of pulsatile blood flow in peripheral microvascular bed in real time. It is a sensitive index to evaluate the perfusion status of local tissues.4 PI is computed by the oximeter as the ratio of the pulsatile amplitude (AC) to the non-pulsatile baseline (DC) of the infrared plethysmographic signal (AC/DC × 100%). It reflects the relative magnitude of arterial pulsations at the sensor site and is commonly interpreted as a non-invasive surrogate of peripheral perfusion and vasomotor tone, not a direct flow meter.
AngII exerts rapid arteriolar vasoconstriction via AT1R, elevating vascular resistance and reducing microvascular perfusion, which should lower PI at the finger probe. Experimental work shows that AngII dynamically regulates skeletal-muscle microvascular blood volume, and vascular studies confirm its direct constrictor effects. In POTS, multiple cohorts report elevated circulating AngII, consistent with dysregulated RAAS and impaired volume expansion; therefore, a negative association between AngII and PI was hypothesized. By contrast, AngI is a precursor peptide whose relationship to end-organ perfusion depends on conversion to AngII (ACE), counter-regulation by ACE2 (ANG-(1-7)), and local tissue RAAS; arterial AngI may therefore decouple from peripheral vasomotor tone and show no clear link to PI.
Therefore, the aim of this study is to evaluate the level of RAAS activity and its correlation with the perfusion index under postural stress in patients with POTS, and to explore the feasibility of combining RAAS activity and PI as potential noninvasive auxiliary indicators for the diagnosis of POTS.
Subjects and Methods
Subjects
In this study, 65 children who were diagnosed with POTS by Head-Up Tilt Test (HUTT) in the Department of Pediatrics of the First Affiliated Hospital of Shihezi University, The Second Division of Xinjiang Production and Construction Corps, Third Division Hospital of Xinjiang Production and Construction Corps, The Fourth Division Hospital of the Xinjiang Production and Construction Corps and Manas County Hospital from August 2024 to July 15th 2025 were selected as the POTS group. Routine evaluation was performed, including detailed medical history investigation, comprehensive physical examination, 12-lead standard electrocardiogram and related laboratory tests. In addition, 65 healthy children who visited the Department of Pediatrics for physical examination during the same period and had no discomfort were selected as the control group. The control group underwent routine evaluation (age, gender, past history, family history, etc). This study was approved by the Ethics Committee of the First Affiliated Hospital of Shihezi University.
Inclusion Criteria
① The patients met the diagnostic criteria of POTS in the 2016 Chinese Medical Association Diagnostic Guidelines for Syncope in Children (2016 Revision);5② patients aged between 8 and 14 years old; ③ Complete clinical data; ④ Written informed consent was obtained from the guardians of the children.
Exclusion Criteria
Patients who met any of the following criteria were excluded: ① Previous history of surgery, metabolic diseases (such as chronic renal failure or insufficiency, hypertension, obesity, diabetes, etc), cardiovascular diseases (such as congenital heart disease, arrhythmia, etc), and nervous system diseases; ② Taking hormone drugs, RAAS inhibitors (angiotensin-converting enzyme inhibitors or angiotensin receptor antagonists, aldosterone antagonists, renin inhibitors, etc) within 3 months; ③ Uncooperative patients in HUTT; ④ Refused to sign the informed consent; And incomplete clinical data.
Research Methods
To standardize testing conditions and minimize the influence of confounding factors, all participants and their guardians were instructed to ensure the child adhered to the following protocols before the study: fasting for at least 8 hours, abstaining from caffeinated beverages and strenuous physical activity for 24 hours. All experimental procedures, including the head-up tilt test and blood sample collection, were performed in a controlled laboratory environment in the morning (8:00–11:00 AM) to mitigate the effects of diurnal variation on physiological parameters.
- Blood specimen collection: children in both groups had no fever, did not take drugs or foods that affect endothelial function, and avoided menstrual period within 2 weeks before blood collection. Blood samples (3–5 mL) were collected from elbow vein at 60° tilt and added into EDTA-Na2 anticoagulant tubes, and timely detected. The ELISA kits for renin, angiotensin and aldosterone were produced by Shanghai Jianglai Biological Engineering Co, LTD, item number: JL12316.
- For Renin (Sandwich ELISA): 100 µL of standards or undiluted plasma samples were added to the antibody-pre-coated microplate wells and incubated for 90 minutes at 37°C. After washing, 100 µL of biotinylated detection antibody was added and incubated for 60 minutes at 37°C. Following another wash, 100 µL of horseradish peroxidase (HRP)-conjugated streptavidin was added and incubated for 30 minutes at 37°C. After a final wash, 90 µL of tetramethylbenzidine (TMB) substrate was added and incubated for 15–20 minutes at 37°C in the dark. The reaction was stopped by adding 50 µL of stop solution, and the absorbance was immediately measured at 450 nm using a microplate reader (BioTek Epoch 2).
- For Aldosterone, AngI, and AngII (Competitive ELISA): 50 µL of standards or plasma samples (Aldosterone: undiluted; AngI: 1:2 dilution; AngII: 1:4 dilution, as per kit instructions) were added to the pre-coated wells, followed immediately by 50 µL of the HRP-conjugated antigen. The plate was incubated for 60 minutes at 37°C. After thorough washing, 100 µL of TMB substrate was added and incubated for 15–20 minutes at 37°C in the dark. The reaction was stopped with 50 µL of stop solution, and absorbance was read at 450 nm.
- Determination of PI: A multi-parameter monitor (Philips IntelliVue MX550) with a children’s finger cuff probe was used. The measurement was carried out in strict dark (ambient illuminance <5 lux, probe hood wrapped), constant temperature (24.0±0.5°C) and constant humidity (50±3%RH) conditions. The blood oxygen probe was fixed at the end of the ring finger of the left hand (less limb movement on the dominant hand), and the arm was naturally placed flat on the support frame, at the same height as the heart. The subjects underwent tilt test at 60°position, and the raw PI data were continuously recorded.
Statistical Methods
We implemented blinding procedures at key stages to minimize bias. The physicians performing and interpreting the head-up tilt tests (HUTT) for diagnosis were blinded to all subsequent laboratory and perfusion data. For ELISA analysis, all plasma samples were de-identified and randomized, and the laboratory personnel were blinded to the clinical groups. Perfusion Index (PI) measurement was objective and operator-independent, as it was automatically generated by the monitor. Finally, the statistician performed all analyses using an anonymized dataset, with group identities revealed only after the completion of statistical testing.
All analyses were performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). Data distribution was assessed by the Kolmogorov–Smirnov test. Continuous variables conforming to normality are presented as mean ± SD and were compared by independent-samples t test; non-normal variables are reported as median (P25, P75) and compared by Mann–Whitney U-test. Categorical data are expressed as counts and proportions and were analyzed byχ2test. To control the family-wise error rate across multiple comparisons, p values for the five demographic and the five biochemical/perfusion parameters were adjusted using the Holm–Bonferroni step-down procedure (m = 5, overall α = 0.05), with adjusted p < 0.05 considered statistically significant. Receiver operating characteristic (ROC) curve analyses were conducted to evaluate the diagnostic performance of Ang II and PI for POTS and for low perfusion (PI ≤ 5.35%), reporting area under the curve (AUC), optimal cut-off (Youden index), sensitivity, and specificity. A combined Ang II + PI predictive model was constructed using binary logistic regression, with regression coefficients (B), standard errors (SE), Wald χ2, odds ratios (OR) and 95% confidence intervals (CI) presented, and model discrimination assessed by Receiver operating characteristic area under the curve. Pearson correlation analysis was used to examine the relationship between Ang II and PI. All tests were two-tailed.
Results
Demographic Characteristics
Demographic characteristics, including age, gender, height, weight, and body mass index (BMI), were comparable between the POTS group and the healthy control group after Holm-Bonferroni correction for multiple comparisons (all adjusted *p* ≥ 0.05). This confirms that the two groups were well matched, and any observed differences in biochemical or hemodynamic parameters are unlikely to be attributed to these baseline variables (Table 1).
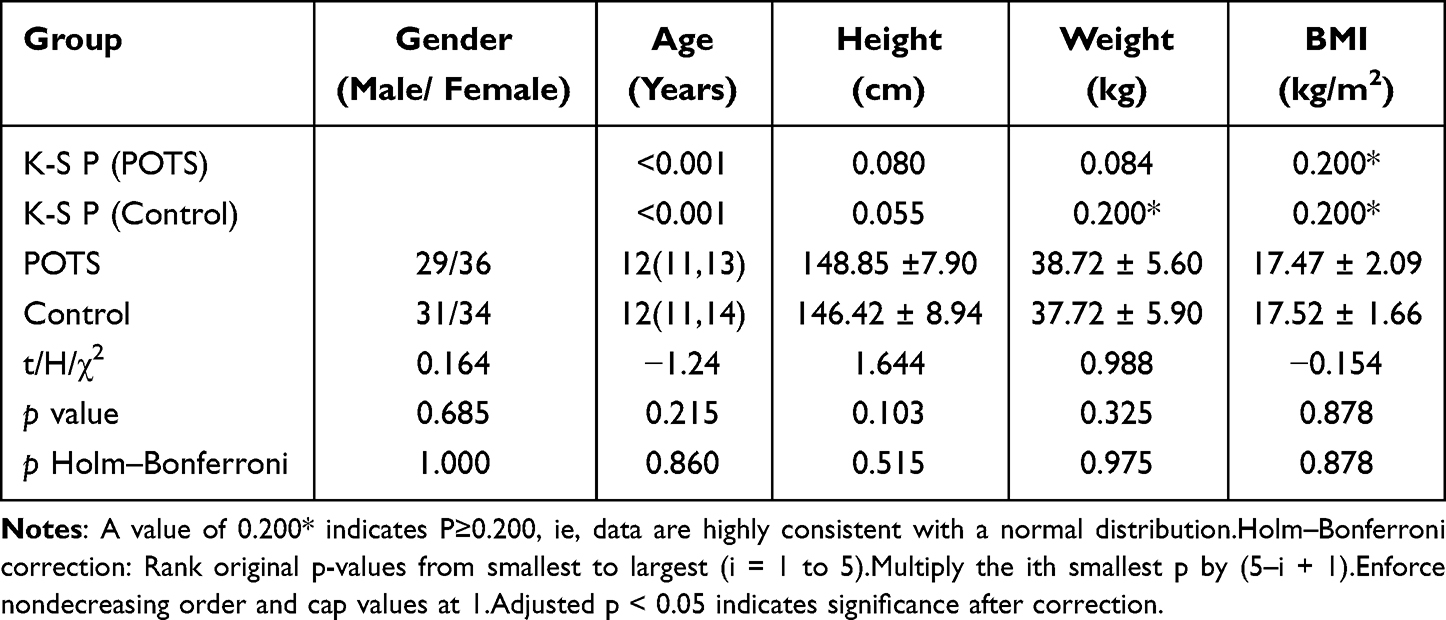 |
Table 1 Demographic Characteristics of Children with POTS and Controls ( |

Comparison of Plasma Renin, Angiotensin I (AngI), AngII, Aldosterone Levels and PI Between POTS Group and Control Group
As hypothesized, children with POTS exhibited significant alterations in key study parameters compared to controls. Plasma Angiotensin II (AngII) levels were significantly higher in the POTS group (114.07 ± 7.69 pg/mL) than in the control group (109.20 ± 10.44 pg/mL; adjusted *p* = 0.012). Concurrently, the Perfusion Index (PI) was markedly lower in POTS patients (4.64 ± 1.54%) compared to healthy children (6.19 ± 1.64%; adjusted *p* < 0.005). In contrast, no significant differences were observed between the groups in plasma levels of renin, Angiotensin I (AngI), or aldosterone (all adjusted *p* > 0.05) (Table 2).
 |
Table 2 Comparison of Plasma Renin, AngI, AngII, Aldosterone Levels and PI When POTS Children and Control Group Tilted 60° ( |

Diagnostic Performance of AngII and PI Separately for POTS
We evaluated the potential of AngII and PI as diagnostic biomarkers for POTS using Receiver Operating Characteristic (ROC) curve analysis.
AngII demonstrated a moderate ability to discriminate POTS patients from controls, with an Area Under the Curve (AUC) of 0.654 (95% CI: 0.559–0.749, *p* = 0.002). At the optimal cutoff value of 110.13 pg/mL, the sensitivity was 72.3% and the specificity was 58.5%.
PI showed better diagnostic performance than AngII, with an AUC of 0.753 (95% CI: 0.670–0.836, *p* < 0.001). The optimal PI cutoff was 5.35%, yielding a sensitivity of 67.7% and a specificity of 67.7% (Figure 1).
 |
Figure 1 Receiver operating characteristic Curve of AngII or PI for the POTS. |
Diagnostic Performance of the Combined AngII and PI Model for POTS: Binary Logistic Regression and Receiver Operating Characteristic Analysis
Binary logistic regression showed that AngII was not significantly associated with POTS (B = 0.0202, SE = 0.0238, Waldχ2= 0.717, p = 0.397), yielding an odds ratio (OR) of 1.020 (95% CI: 0.974–1.069). In contrast, PI emerged as a strong independent predictor (B = –0.5491, SE = 0.1367, Wald χ2 = 16.125, p < 0.001), with an OR of 0.577 (95% CI: 0.442–0.755), indicating that each one‐unit increase in PI reduced the odds of POTS by approximately 42.3% (Table 3).
 |
Table 3 Binary Logistic Regression Analysis of AngII and PI for Prediction of POTS |
The combined predictive model achieved an area under the Receiver operating characteristic curve (area under the curve) of 0.750 (Figure 2).
 |
Figure 2 Receiver operating characteristic curve of combined model (AngII and PI). |
Correlation Analysis Between Angiotensin II and PI Values
Pearson’s correlation analysis revealed a moderate, statistically significant inverse relationship between AngII and PI (r = –0.459, p < 0.001), indicating that higher AngII levels were associated with lower PI values (Figure 3).
 |
Figure 3 Correlation between Angiotensin II and PI. |
Receiver Operating Characteristic Curve of Angiotensin II for Predicting Hypoperfusion State
In our cohort, the PI cutoff for hypoperfusion (PI ≤ 5.35%) was determined from the Receiver operating characteristic analysis of PI for diagnosing POTS, thereby optimizing the balance between sensitivity and specificity. Receiver operating characteristic analysis was performed to evaluate the diagnostic accuracy of AngII for identifying low perfusion (PI ≤ 5.35). Under nonparametric assumptions, the area under the curve was 0.702 (SE = 0.048; asymptotic p < 0.001; 95% CI: 0.608–0.796), indicating moderate discriminative ability. The optimal threshold, determined by the maximum Youden index, was 112.44 pg/mL, at which sensitivity was 70.5%, specificity was 29.5%, and the Youden index was 0.391 (Figure 4).
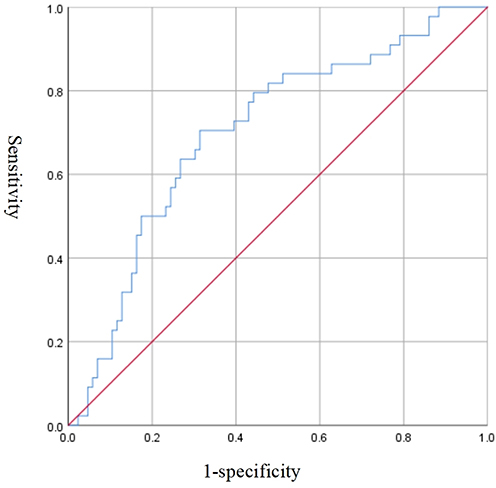 |
Figure 4 Receiver operating characteristic Curve: Angiotensin I Predicting Low Perfusion (PI ≤ 5.35). |
Discussion
Our study demonstrates two principal findings in children with POTS: first, a significant dysregulation of the RAAS, characterized by a selective elevation of AngII without a concomitant rise in renin or aldosterone; and second, a marked reduction in peripheral perfusion as measured by PI. The moderate inverse correlation between AngII and PI (r= −0.459) provides a crucial pathophysiological link, suggesting that RAAS overactivity, possibly via unopposed AT1R-mediated vasoconstriction, contributes to microcirculatory deficits. Conceptually, these findings position PI not just as a hemodynamic parameter but as a practical, noninvasive clinical tool for screening and monitoring POTS, outperforming AngII in diagnostic accuracy (AUC 0.753 vs 0.654) and emerging as a strong independent predictor. The clinical implication is immediate: PI can be integrated into tilt-testing protocols for real-time, objective assessment of perfusion status. Meanwhile, elevated AngII, while less diagnostically powerful, offers mechanistic insight for stratifying patients and future targeted interventions, moving beyond syndromic diagnosis toward pathophysiology-guided management.
This study explored the relationship between RAAS activity, particularly AngII and PI in children with POTS, focusing on their diagnostic value and clinical significance.
The RAAS plays a core physiological role in maintaining blood pressure stability and blood volume regulation, mainly by regulating vascular tone and sodium and water retention in response to blood flow redistribution caused by postural change.6 Normally, when the human body changes from supine to upright positions, blood pressure receptor sensitivity decreases, and renin secretion increases, initiating the RAAS cascade that promotes the production of angiotensin I and its conversion to angiotensin II via ACE.7 Ang II, a key effector molecule in the RAAS, is a potent vasoconstrictor that promotes sympathetic activity, inhibits parasympathetic conduction, induces heart rate increase, and peripheral vasoconstriction by activating angiotensin type 1 receptors (AT1R).8 Additionally, Ang II stimulates aldosterone release, promoting the reabsorption of sodium and water in the distal tubule and increasing blood volume, thus helping maintain stable blood pressure.9 However, these regulatory mechanisms are often dysregulated in patients with POTS. The present study found that although Ang II was significantly increased in the POTS group, other downstream factors of the RAAS such as renin and aldosterone did not concurrently increase, suggesting the existence of a “renin-aldosterone paradox”.10 This paradox may result from decreased ACE2 activity, which impairs conversion of Ang II into the vasodilator Ang-(1-7), leading to Ang II accumulation, sustained vasoconstriction, peripheral hypoperfusion, and excessive heart rate response—key clinical manifestations of POTS.11,12
The PI is the ratio of pulsatile to nonpulsatile blood flow, commonly used to monitor microcirculatory perfusion status.13,14 In pediatric research and clinical practice, PI has been increasingly used to assess the functional status of the circulatory system due to its non-invasive, rapid, and sensitive characteristics.15 PI values are influenced by stroke volume, vascular resistance, and local microcirculatory dynamics, making it a comprehensive indicator of tissue perfusion.16,17 In the present study, children with POTS had significantly lower PI values compared to controls, indicating impaired peripheral tissue perfusion under tilt stimulation. This hypoperfusion state may be attributable to vasoconstriction caused by RAAS hyperactivation. Ang II directly increases vascular tone and enhances sympathetic tone through central mechanisms, exacerbating local small-vessel constriction and reducing pulsatile blood flow, thus decreasing PI.18,19 Therefore, the role of Ang II in POTS extends beyond systemic circulation, potentially deeply involved in controlling microcirculatory perfusion, representing a critical upstream mechanism influencing PI.
Our results showed that children with POTS had significantly higher plasma AngII levels (114.07 ± 7.69 pg/mL) compared to healthy controls (109.20 ± 10.44 pg/mL), and markedly lower PI values (4.64 ± 1.54% vs 6.19 ± 1.64%; both p < 0.05 after Holm–Bonferroni correction). These findings suggest that increased AngII is associated with enhanced neurohumoral activation, while the reduction in PI indicates impaired peripheral perfusion, which is a key feature in the hemodynamic profile of POTS.
Correlation analysis revealed a moderate but significant negative relationship between AngII and PI (r = –0.459, p < 0.001), supporting the notion that higher neurohumoral activity is linked to more pronounced microcirculatory dysfunction. This relationship highlights a potential pathophysiological mechanism in POTS, where excessive RAAS activation could contribute to decreased peripheral blood flow and the resultant symptoms of orthostatic intolerance.
In terms of diagnostic performance, Receiver operating characteristic curve analysis indicated that PI alone is a strong discriminator for POTS (area under the curve = 0.753), demonstrating high sensitivity and specificity. AngII also showed moderate diagnostic value (area under the curve = 0.654), though less robust than PI. When AngII and PI were combined in a predictive model, the diagnostic accuracy (area under the curve = 0.750) was essentially comparable to PI alone. The reason for the minimal increase in area under the curve when AngII is added to PI may be due to the moderate correlation between these two variables, as well as the fact that PI directly captures hemodynamic changes associated with POTS, whereas AngII primarily reflects upstream neurohumoral alterations.
Binary logistic regression further emphasized the independent predictive value of PI for POTS (OR = 0.577, 95% CI: 0.442–0.755, p < 0.001). Although AngII was elevated in the POTS group, its association with POTS was not statistically significant in the multivariate model (OR = 1.020, 95% CI: 0.974–1.069, p = 0.397). This lack of significance may be explained by the shared physiological pathway and moderate correlation between AngII and PI, which attenuate the unique contribution of AngII when both are included in the same model.
The role of Ang II in POTS extends beyond systemic circulation, potentially deeply involved in controlling microcirculatory perfusion, representing a critical upstream mechanism influencing PI. Another critical result from our analysis pertains to the relative importance of the biomarkers. While both AngII and PI were altered in POTS children, only PI retained its status as a significant, independent predictor in the multivariate logistic regression model. The loss of statistical significance for AngII when PI was included in the model is a pivotal finding. It suggests that the pathophysiological effects of elevated AngII—primarily vasoconstriction—are ultimately captured and more directly reflected in the reduction of peripheral perfusion, as measured by PI. Therefore, from a diagnostic standpoint, PI serves as a more robust and immediate integrator of the final common hemodynamic pathway in POTS, whereas AngII’s role is more that of an upstream mediator.
Notably, our results confirm the high clinical value of PI as a noninvasive, rapid, and reliable tool for diagnosing pediatric POTS. The ability of PI to reflect real-time peripheral perfusion changes offers significant advantages in routine clinical settings, facilitating timely screening, diagnosis, and monitoring of children with POTS.
Nevertheless, the clinical value of AngII should not be underestimated. Unlike PI, which reflects peripheral perfusion at a single time point, AngII provides critical information about the neurohumoral status and pathophysiological process underlying POTS. AngII may help identify specific subgroups of patients with more pronounced RAAS activation, guide future individualized therapeutic interventions, and improve our mechanistic understanding of the disease beyond what PI alone can offer. Thus, AngII serves as a meaningful adjunct in both research and select clinical scenarios where deeper insight into neurohumoral regulation is required.
Taken together, these data underscore that while PI is a powerful, noninvasive tool for the diagnosis of POTS in children, AngII remains valuable for understanding disease mechanisms and may inform future stratification or targeted intervention strategies. The integration of PI and neurohumoral AngII assessments provides a more comprehensive perspective on pediatric POTS and may support more individualized approaches to patient care.
Although suggestive, this study has several limitations. First, the relatively small sample size from a single center may limit the statistical power and generalizability of our findings, particularly for subgroup analyses and the precise estimation of cutoff values. Second, we measured only part of the RAAS system. The absence of data on the counter-regulatory ACE2/Ang-(1-7)/Mas axis means our pathophysiological model is incomplete, and the drivers of AngII accumulation remain partially explained, which could affect the interpretation of the AngII results. Third, this cross-sectional study lacks dynamic tracking data. Consequently, the temporal and causal relationship between AngII elevation and PI reduction cannot be established, and our proposed mechanism, while plausible, remains speculative. Future studies should incorporate follow-up and interventional designs to further explore the role of Ang II and PI changes in disease progression and treatment response, providing a stronger evidence basis for the mechanistic understanding and clinical management of POTS.
Conclusion
In children with POTS, RAAS dysregulation is evident, characterized by elevated Ang II alongside reduced peripheral perfusion indexed by PI. PI outperformed Ang II for diagnosis (area under the curve 0.753 vs 0.654) and remained an independent predictor (OR 0.577, 95% CI 0.442–0.755; p<0.001). Ang II correlated inversely with PI (r=−0.459; p<0.001), and adding Ang II to PI did not meaningfully improve discrimination (combined area under the curve 0.750). PI thus represents a practical, noninvasive tool for screening and monitoring, whereas Ang II adds mechanistic and potential stratification value. Larger multicenter, longitudinal and interventional studies—integrating the ACE2/Ang-(1–7)/Mas axis—are warranted to refine risk stratification and guide targeted therapy.20
Data Sharing Statement
The data supporting the findings of this investigation are available upon reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
This study was submitted to and approved by the Science and Technology Ethics Committee of the First Affiliated Hospital of Shihezi University (Approval No. KJ2024-468-01).
This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
XPCC Science and Technology Research Plan in Key Areas (2023AB018-11), XPCC 2023 Talent Development Fund (CZ001209), XPCC Science and Technology Support Special Plan (2022ZD024), Innovation and Development Special Plan of Shihezi University (CXFZ202115), Talent Development Fund - Key Laboratory of the Corps - Clinical Medical Research Center for Children’s Diseases of the First Affiliated Hospital of the Corps (CZ001209/ Bing Caixing [2023] 80-2023).
Disclosure
The authors declare no competing interests. All authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of reliability and freedom from bias of the data presented and their discussed interpretation. This paper has been uploaded to ResearchGate as a preprint: https://www.researchgate.net/publication/393741088_Correlation_between_activity_level_of_renin-angiotensin-aldosterone_system_and_perfusion_index_in_children_with_postural_tachycardia_syndrome.
References
1. Wang C, Li Y, Liao Y. Writing committee members:; panelists:. 2018 Chinese Pediatric Cardiology Society (CPCS) guideline for diagnosis and treatment of syncope in children and adolescents. Sci Bull. 2018;63(23):1558–1564. doi:10.1016/j.scib.2018.09.019
2. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome[J]. Clin Auton Res. 2011;21(2):69–72. doi:10.1007/s10286-011-0119-5
3. Juan Z, Junbao D, Hong-fang J. Pathogenesis of postural tachycardia syndrome in children [J]. Chin J Pract Pediat. 2012;27(7):540–542.
4. Coutrot M, Dudoignon E, Joachim J, et al. Perfusion index: physical principles, physiological meanings and clinical implications in anaesthesia and critical care[J]. Anaesth Crit Care Pain Med. 2021;40(6):100964. doi:10.1016/j.accpm.2021.100964
5. Hu JW, Yan XJ, Wang YF, et al. Interpretation of pediatric syncope diagnosis guidelines (2016 revision). Chin J Pract Pediat. 2016;31(05):321–325.
6. Aliukonis P, Letauta T, Briedienė R, Naruševičiūtė I, Letautienė S. The role of different PI-RADS versions in prostate multiparametric magnetic resonance tomography assessment. Acta Med Litu. 2017;24(1):44–50. doi:10.6001/actamedica.v24i1.3462
7. Martyniak A, Tomasik PJ. A new perspective on the renin-angiotensin system. Diagnostics. 2022;13(1):16. doi:10.3390/diagnostics13010016
8. Ziaja M, Urbanek KA, Kowalska K, Piastowska-Ciesielska AW. Angiotensin II and angiotensin receptors 1 and 2-multifunctional system in cells biology, what do we know? Cells. 2021;10(2):381. doi:10.3390/cells10020381
9. Seema P, Abdur R, Haroon K, et al. Renin-angiotensin-aldosterone (RAAS): the ubiquitous system for homeostasis and pathologies. Biomed Pharmacother. 2017;94:317–325. doi:10.1016/j.biopha.2017.07.091
10. Mustafa HI, Garland EM, Biaggioni I, et al. Abnormalities of angiotensin regulation in postural tachycardia syndrome. Heart Rhythm. 2011;8(3):422–428. doi:10.1016/j.hrthm.2010.11.009
11. Satish R, Raj I, Biaggioni P, et al. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation. 2005;111.
12. Julian M, Stewart J, Glover L, Marvin S. Medow, Increased plasma angiotensin II in postural tachycardia syndrome (POTS) is related to reduced blood flow and blood volume. Clin Sci. 2005;110.
13. Hasanin A, Mukhtar A, Nassar H. Perfusion indices revisited. J Intensive Care. 2017;5. doi:10.1186/s40560-017-0220-5
14. de Keijzer IN, Massari D, Sahinovic M, Flick M, Vos JJ, Scheeren TWL. What is new in microcirculation and tissue oxygenation monitoring? J Clin Monit Comput. 2022;36(2):291–299. doi:10.1007/s10877-022-00837-x
15. van Genderen ME, van Bommel J, Lima A. Monitoring peripheral perfusion in critically ill patients at the bedside. Curr Opin Crit Care. 2012; 18:273–90.
16. Xiaotong S, Huaiwu H, Mengru X, et al. Peripheral perfusion index of pulse oximetry in adult patients: a narrative review. Eur J Med Res. 2024;29. 10.1186/s40001-024-02048-3
17. Stewart JM, Glover JL, Medow MS. Increased plasma angiotensin II in postural tachycardia syndrome (POTS) is related to reduced blood flow and blood volume. Clin Sci. 2006;110(2):255–263. doi:10.1042/CS20050254
18. Nadasy GL, Balla A, Dornyei G, Hunyady L, Szekeres M. Direct vascular effects of angiotensin II (A systematic short review). Int J Mol Sci. 2024;26(1):113. doi:10.3390/ijms26010113
19. Behuliak M, Bencze M, Boroš A, et al. Chronic inhibition of angiotensin converting enzyme lowers blood pressure in spontaneously hypertensive rats by attenuation of sympathetic tone: the role of enhanced baroreflex sensitivity. Biomed Pharmacother. 2024;176:116796. doi:10.1016/j.biopha.2024.116796
20. Zhang F, Pan J, Lin Z, et al. Correlation between activity level of renin-angiotensin-aldosterone system and perfusion index in children with postural tachycardia syndrome, 14 July 2025, PREPRINT (Version 1) available at research square 10.21203/rs.3.rs-6958804/v1.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.