Back to Journals » Clinical Ophthalmology » Volume 19
Corneal Topographic Changes Due to Pediatric Epiblepharon Surgery
Authors Shindo J ![]() , Matsumura N
, Matsumura N ![]() , Nakamura J, Asano M
, Nakamura J, Asano M ![]() , Ohno T, Mizuki N
, Ohno T, Mizuki N
Received 4 November 2024
Accepted for publication 18 January 2025
Published 3 February 2025 Volume 2025:19 Pages 349—356
DOI https://doi.org/10.2147/OPTH.S503661
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jun Shindo,1,2 Nozomi Matsumura,1 Jutaro Nakamura,2 Mizuki Asano,1 Tomoko Ohno,1 Nobuhisa Mizuki2
1Department of Ophthalmology, Kanagawa Children’s Medical Center, Yokohama, Kanagawa, 232-8555, Japan; 2Department of Ophthalmology and Visual Science, Yokohama City University Graduate School of Medicine, Yokohama, Kanagawa, 236-0004, Japan
Correspondence: Jun Shindo, Department of Ophthalmology, Kanagawa Children’s Medical Center, Mutsukawa, Yokohama, Kanagawa, 232-8555, Japan, Tel +81 45 711 2351, Fax +81 45 721 3324, Email [email protected]
Purpose: This study aimed to investigate changes in corneal morphology following pediatric lower-lid epiblepharon surgery using a topographic modeling system 5 (TMS-5®).
Patients and Methods: A randomized controlled trial compared two surgical interventions for pediatric epiblepharon: incisional (modified Hotz procedure with lid margin splitting) and nonincisional. Corneal topography analysis using the TMS-5® served as an outcome measure. The study included 89 eyes from 50 children aged 3– 12 years (mean age, 7.5 ± 2.4 years) diagnosed with moderate epiblepharon. Patients were randomly assigned to the incisional (45 eyes from 25 patients) or nonincisional (44 eyes from 25 patients) groups. Parameters including surface regularity index (SRI), Standard Deviation of Corneal Power (SDP), Irregular Astigmatism Index (IAI), and corneal astigmatism (CYL) were evaluated. The positive rate of Keratoconus Screening System (Keratoconus Index [KCI] and Keratoconus Severity Index [KSI]) was assessed.
Results: The 6-month postoperative mean changes in corneal astigmatism were − 0.34 ± 0.96 D (p = 0.012) and − 0.21 ± 0.67 D (p = 0.22) in the incisional and nonincisional groups, respectively. Corneal astigmatism parameters significantly improved following both surgical procedures (p < 0.01). Preoperatively, 14.6% and 28.1% of patients were suspected of keratoconus using KCI and KSI, respectively, with a significantly reduced postoperative suspicion positivity rate (p < 0.01).
Conclusion: Corneal astigmatism significantly improved in the incisional group. Both surgical methods improved the postoperative corneal surface smoothness, corneal refractive power variability, and irregular astigmatism. Patients with epiblepharon were occasionally suspected of keratoconus when assessed with TMS, with a higher frequency indicated by KSI.
Keywords: topographic modeling system, epiblepharon, cornea, keratoconus, astigmatism
Introduction
Epiblepharon primarily affects the lower eyelids and is frequently observed in East Asian children. It is characterized by a skin fold that overlaps the eyelid margin, pushing the eyelashes against the eyeball.1 This can cause irritation, discharge, excessive tearing, light sensitivity, the sensation of a foreign object in the eye, and visual disturbances due to corneal damage. Initial management is conservative; however, surgical intervention may sometimes be necessary.1–4 Patients with epiblepharon are more likely to have astigmatism than the general population.2,5 The impact of surgical intervention on astigmatism in these patients remains unclear.2,5–10
Nonincisional suturing and incisional surgery (modified Hotz procedure) are the two most common surgical techniques for epiblepharon.1,4,11 A multicenter randomized controlled trial was conducted and used to compare the impact of both surgical techniques on total astigmatism 6 months postoperatively.10 Our findings revealed significant improvements in total astigmatism following the incisional method, which achieved significantly better correction, with 77.8% of cases showing well-corrected results compared with 55.4% in the nonincisional surgery group. The average 6-month postoperative change in total astigmatism for the incisional and nonincisional groups was −0.24 ± 0.42 D and −0.01 ± 0.47 D, respectively.10
Further investigations were warranted to determine whether these changes in total astigmatism were attributable to alterations in corneal astigmatism, and if so, to which specific corneal indices. As part of our study endpoints, preoperative and postoperative corneal morphology was measured using the topographic modeling system (TMS) to assess how epiblepharon surgery affects corneal morphology in children.
Materials and Methods
Patient Selection and Randomization
Patients aged 3–12 years old who were diagnosed with lower-lid epiblepharon accompanied by keratitis and moderate (grade 2) cilia–corneal touch severity (based on a grading scale of 1 to 3) were selected for this study (Figure 1A–C). Patients were recruited from Yokohama City University Hospital and Kanagawa Children’s Medical Center between September 2017 and July 2019.10 Patients with a history of eyelid or facial surgery, upper eyelid ciliary touch, ptosis, eyelid opening or closing abnormalities, systemic syndromes, craniofacial anomalies, corneal opacity, or keratoconus were excluded. Keratoconus was excluded based on findings from slit-lamp examination.
 |
Figure 1 Grade of Ciliary Touch (Right Eye). The classification was adapted from a study by Lee et al.12 From left to right, the categories are grade 1(A): mild; grade 2(B): moderate; and grade 3(C): severe. Ciliary touch was assessed in the primary eye position. |
Randomization was conducted via a central data center using Excel-generated random numbers. Patient registration numbers were submitted to this center, where each patient was randomly allocated with equal probability to one of two surgical treatment groups: (1) the incisional surgery group, employing a modified Hotz procedure with lid margin splitting (LMS), or (2) the nonincisional surgery group, utilizing a buried sutures technique. This methodology ensured an unbiased distribution of patients between the two surgical interventions under investigation.10
Surgical Techniques
All surgeries were performed under general anesthesia by one of two ophthalmologists, both employing identical techniques. The two surgical methods utilized were the incisional technique (modified Hotz procedure with LMS) and the nonincisional technique (buried sutures).
The incisional technique, based on Hwang et al,13 began with LMS. Using chalazion forceps to grasp the lower lid, a 1 mm deep incision was made along the gray line with a No. 15 scalpel blade. The incision extended from 1 mm lateral to the punctum to the medial third or half of the lower eyelid. The subsidiary skin between the orbicularis skin flap and the tarsus was incised and dissected. The subcutaneous tissue of the orbicularis skin flap was fixed to the lower tarsal margin using three interrupted 6–0 polyglactin sutures. Skin edges were approximated with 8–0 polyglactin sutures, which were left in place.
The nonincisional technique, described by Seo et al,14 utilized a double-armed 7–0 polyester suture. After creating a small incision at the suture exit site, the needle was passed from the inferior fornix to approximately 3–4 mm below the eyelid margin. The conjunctival side was threaded subconjunctivally, while the dermal side was threaded subcutaneously, both directed slightly laterally. Both threads were brought out at the same location, tightly tied, and buried. Two such sutures were placed in each lower eyelid: one medially and one centrally. These buried sutures were not removed.
Examinations and Follow‑up
One month before surgery, the participants underwent randomization and preoperative evaluations. These evaluations included visual acuity testing, autorefraction for refractive assessment, corneal topography using the TMS-5® (TOMEY, Nagoya, Japan), slit-lamp examination with corneal fluorescein staining, and eyelid photography. Postoperative follow-ups were scheduled at 26 ± 4 weeks, involving the same preoperative examinations. The outcomes of the procedures were evaluated 6 months after surgery.
Statistical Analysis and Sample Size Calculations
Sample size calculations for this study are detailed in our previous report.10 Briefly, the primary outcome was a comparison of success rates between the incisional and nonincisional techniques. In our previous report, a retrospective comparison at our institution revealed clinical success rates of 63% and 90% for nonincisions and incisions, respectively. Based on these results, we calculated the required sample sizes using Fisher’s exact test, with an alpha error set at 0.05 and a statistical power of 0.8. Wilcoxon’s signed-rank test was used to evaluate the changes in corneal astigmatism measured using the TMS, as well as related indices. Statistical significance was set at p < 0.05. Comparisons of indices were adjusted using the Bonferroni correction to account for multiple comparisons. DATAtab (Graz, Austria), an online statistics calculator, was used for statistical analyses.
Ethical Approval and Consent to Participate
This research adhered to the ethical principles outlined in the Declaration of Helsinki. The institutional review boards of Yokohama City University Hospital and Kanagawa Children’s Medical Center approved the study protocol, informed consent, and assent forms (approval no. 102–01). The legal guardians of all patients involved in the study provided written informed consent. Patients aged over six who could understand the study’s purpose assented to participate in the study. The study was supervised by an independent data and safety monitoring committee. This study is registered on the UMIN Clinical Trial Registry website (www.umin.ac.jp/UMIN000027321).
Results
This study analyzed 89 eyes from 50 patients (22 men and 28 women) aged 3–12 years old (mean age: 7.5 years old) selected from 132 patients and assessed for eligibility. The incisional and nonincisional methods were applied to 25 patients (45 eyes) and 25 patients (44 eyes), respectively, by random assignment. The respective distribution of males and females was 8 (32%) and 17 (68%) in the incisional group and 14 (56%) and 11 (44%) in the nonincisional group. The age, sex, number of cases, and preoperative corneal astigmatism in both groups were statistically similar (Table 1). All participants completed the study and adhered to the follow-up period of 26 ± 4 weeks, with no dropouts recorded. Figure 2 presents representative preoperative and postoperative sequential images of a cornea affected by epiblepharon captured using the TMS-5® (Figure 2A and B). The figure illustrates that the distortion of the Placido rings projected onto the cornea became less pronounced after the surgery, indicating an improved corneal topography.
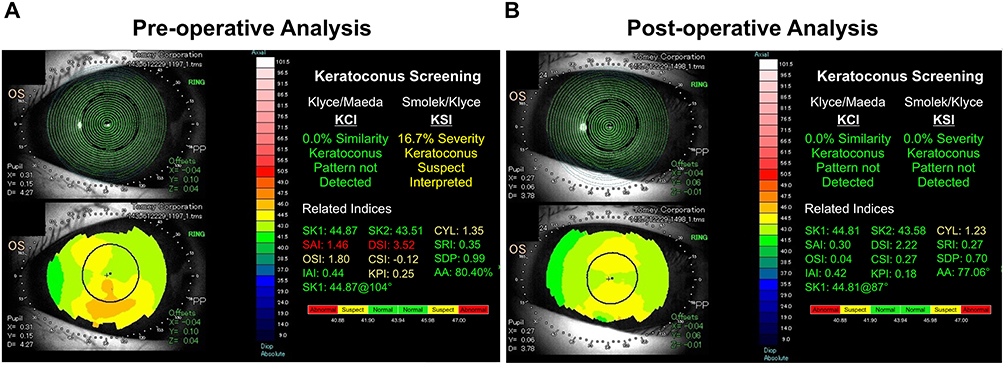 |
Figure 2 Preoperative and Postoperative Corneal Topographic Changes Visualized using TMS-5® in a Representative Case. The left panel displays the results of the preoperative TMS-5® analysis (A), whereas the right panel shows the results six months postoperatively (B). The upper left of the panel displays Placido rings projected onto the cornea, whereas the lower left presents a color map of corneal refractive power. The upper right panel displays the results of keratoconus screening, whereas the lower right panel displays related indices. The postoperative panel on the right demonstrates improvement in each item. |
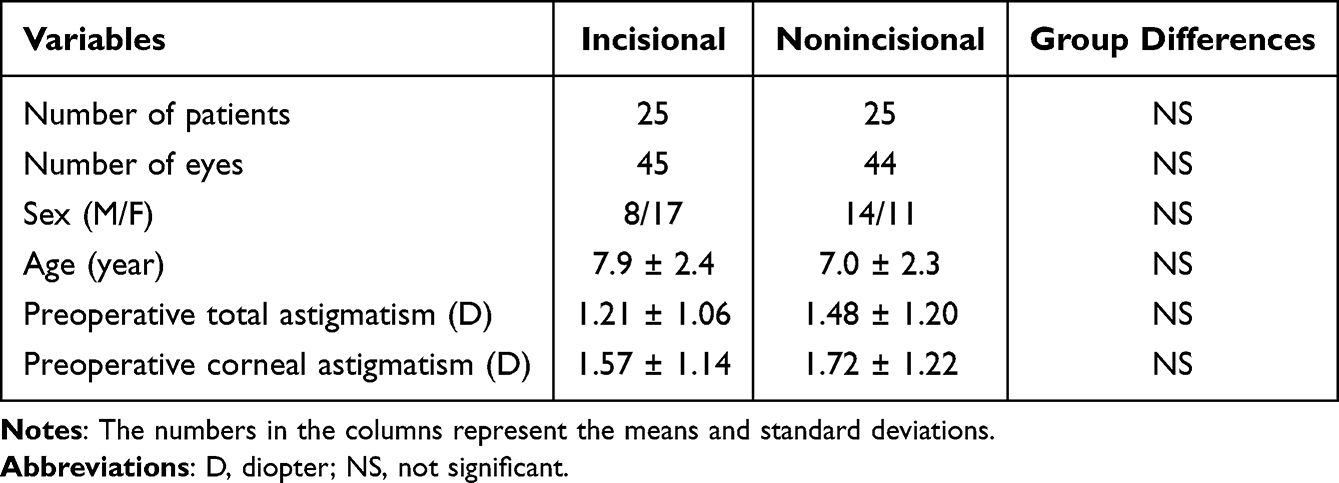 |
Table 1 Characteristics of Patients Enrolled in This Study |
Corneal Astigmatism
Table 2 details the changes in corneal astigmatism measured by TMS-5® before and after surgery. The mean preoperative corneal astigmatism with the incisional method was 1.57 ± 1.14 D, which reduced significantly to 1.23 ± 0.86 D postoperatively (p = 0.012). In contrast, the mean preoperative corneal astigmatism with the nonincisional method was 1.72 ± 1.22 D, which only slightly decreased to 1.51 ± 1.17 D postoperatively, showing no statistically significant improvement (p = 0.22) (Table 2).
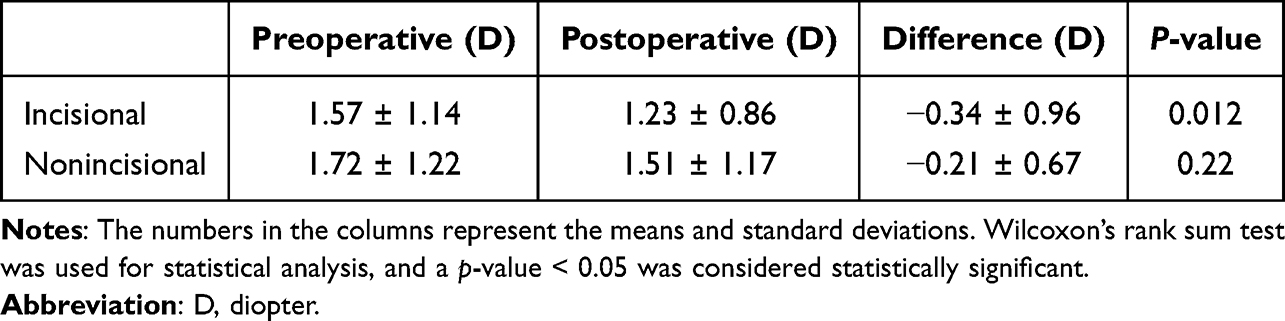 |
Table 2 Comparison of Pre and Postoperative Corneal Astigmatism Among Patients with Epiblepharon |
TMS Indices and Keratoconus Screening
Figure 3 illustrates the SRI, SDP, and IAI changes, reflecting different aspects of corneal astigmatism (Figure 3: Incisional (A) and Non-incisional (B)). All indices showed postoperative improvements with both surgical methods (p < 0.01) (Table 3). Table 4 presents the keratoconus suspicion positivity rate determined by the Keratoconus Screening System’s KCI and KSI (Table 4). The study group did not include patients with clinically diagnosed keratoconus. The KSI exhibited a notably higher positivity rate than the KCI in the preoperative examination. Nevertheless, the positivity rate for both KCI and KSI decreased significantly postoperatively (p < 0.01).
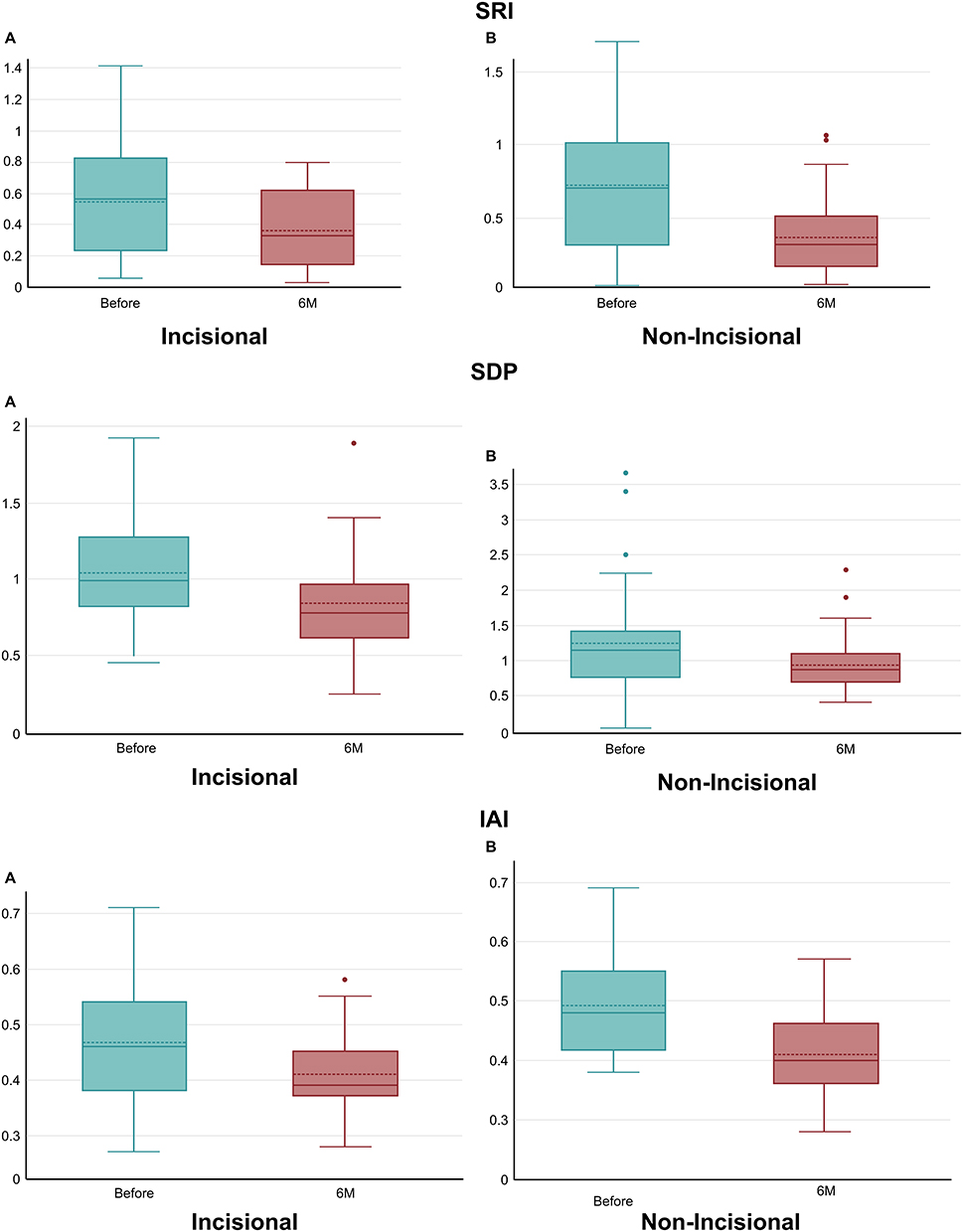 |
Figure 3 Preoperative and Postoperative Changes in Corneal Topography Indices. Preoperative and postoperative SRI, SDP, and IAI changes were analyzed using Wilcoxon’s rank sum test. The p-values for SRI, SDP, and IAI for the incisional (A) and nonincisional (B) groups were <0.01, indicating significant postoperative improvements. Abbreviations: SRI, surface regularity index; SDP, Standard Deviation of Corneal Power; IAI, Irregular Astigmatism Index. |
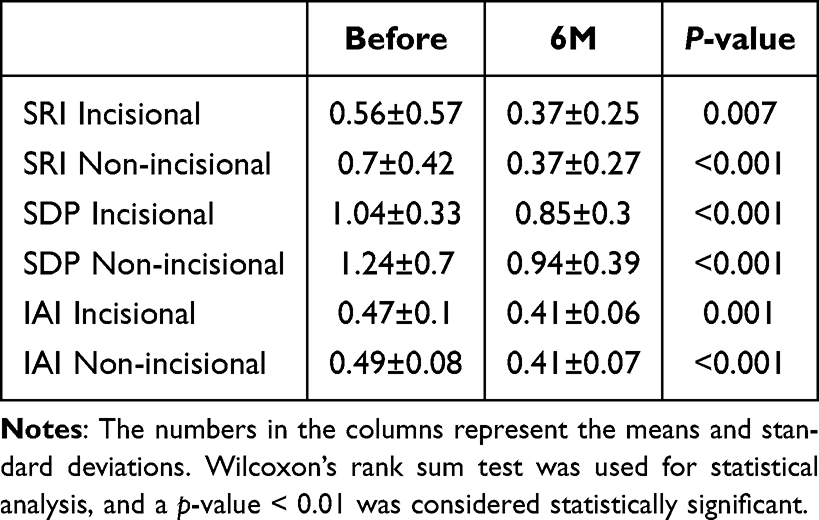 |
Table 3 Comparison of Pre and Postoperative Changes in the SRI, SDP, and IAI |
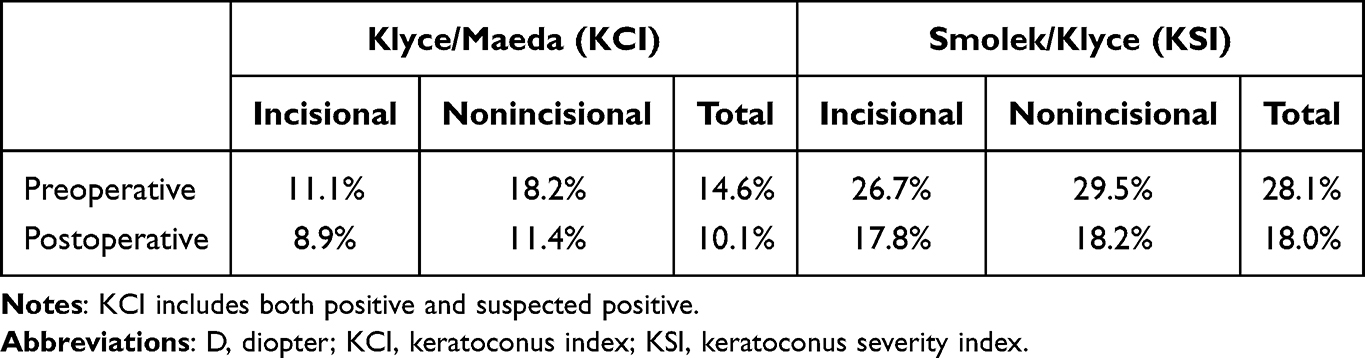 |
Table 4 Positive Rate of the Keratoconus Screening System Among Patients with Epiblepharon |
Discussion
In this study, we examined whether the observed improvements in total astigmatism were attributable to reductions in corneal astigmatism measured using the TMS-5®. The incisional group demonstrated a statistically significant decrease in corneal astigmatism (p = 0.012), whereas the nonincisional group did not exhibit a similar improvement (p = 0.22). These findings strongly suggest that the observed reduction in total astigmatism following surgery using the incisional technique is attributable to the reduced corneal astigmatism.
Further corneal topography analysis revealed improvements in SRI, SDP, and IAI for both surgical methods. Each index captures a distinct aspect of the corneal condition: the SRI measures corneal surface smoothness, the SDP quantifies the standard deviation of corneal refractive power, and the IAI assesses irregular astigmatism. The SRI is particularly useful for estimating the impact of irregular astigmatism on visual acuity.15 Previous studies have reported that patients with abnormalities in these indices exhibit significantly lower character contrast sensitivity than those without abnormalities.16 Moreover, another report demonstrated improvements in postoperative higher-order aberrations and astigmatism following epiblepharon surgery.12,17 The SRI, SDP, and IAI improvements observed in this study suggest potential enhancements in visual function following surgery. Therefore, proactive surgical interventions are warranted for children with epiblepharon who exhibit visual function disorders, including astigmatism and photophobia.
Although several TMS indices reflecting the state of the corneal surface, including SRI, SDP, and IAI, improved significantly with both surgical methods, only the incisional method significantly reduced corneal astigmatism. This outcome suggests the involvement of factors other than just improving trichiasis-induced corneal surface irregularities. One possible explanation is that differences in postsurgical eyelid pressure on the cornea offered by these two methods may have contributed to the superior reduction of corneal astigmatism observed with the incisional method. Further research is required to confirm this hypothesis.
The TMS-5® incorporates two programs for keratoconus screening: the Klyce–Maeda and Smolek–Klyce methods, indexed by KCI and KSI, respectively.16,18 The KCI and KSI employ 8 and 10 indices, respectively, to diagnose the likelihood of keratoconus.16,18 The KSI incorporates three additional indices (CYL, SRI, and SDP) not found in KCI.18 This study demonstrated significant postoperative improvements in these unique KSI indices, suggesting that these additional indices may contribute to a higher incidence of abnormal values (suspected keratoconus) detected by KSI than by KCI. No patients in this study were clinically diagnosed with keratoconus; thus, the reduced postoperative positivity rate for suspected keratoconus suggests that all preoperative keratoconus suspicions were false positives. However, it is important to consider that persistent corneal irritation, such as eye rubbing, may contribute to keratoconus development.19,20 For example, familial cases of keratoconus among siblings with congenital distichiasis indicate that chronic irritation from trichiasis may induce keratoconus.21 Our study identified a subset of patients with abnormal values in the Keratoconus Screening System. This finding warrants further investigation into whether rubbing-related corneal trauma caused by untreated epiblepharon contributes to the underlying etiology of keratoconus.
Astigmatism is a known risk factor for amblyopia in children. However, epiblepharon can exhibit spontaneous resolution. Therefore, a comprehensive evaluation of visual function based on severity, visual acuity, astigmatism, and corneal topography is crucial for determining the optimal timing for surgical intervention.
Limitations of this study are the number of cases and the fact that the evaluation of improvement in corneal astigmatism was not the primary endpoint.
Conclusion
Our study showed that incisional surgery significantly improved corneal astigmatism in children with epiblepharon. Both surgical techniques—incisional and nonincisional—improved corneal surface regularity, corneal power distribution, and irregular astigmatism. Both KCI and KSI positivity rates decreased. These findings highlight the effectiveness of appropriate surgical intervention in improving corneal morphology in pediatric epiblepharon cases.
Data Sharing Statement
The data sets analyzed during the current study are available from the corresponding author (NM) upon reasonable request.
Acknowledgments
The authors would like to thank Dr. Koji Yamamoto for his invaluable assistance with the statistical analysis. The authors would like to express their sincere gratitude to the late Dr. Masaki Takeuchi for his dedicated contribution to this research.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sundar G, Young SM, Tara S, Tan AM, Amrith S. Epiblepharon in east Asian patients: the Singapore experience. Ophthalmology. 2010;117(1):184–189. doi:10.1016/j.ophtha.2009.06.044
2. Khwarg SI, Lee YJ. Epiblepharon of the lower eyelid: classification and association with astigmatism. Korean J Ophthalmol. 1997;11(2):111. doi:10.3341/kjo.1997.11.2.111
3. Noda S, Hayasaka S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol. 1989;73(2):126–127. doi:10.1136/bjo.73.2.126
4. Woo KI, Yi K, Kim YD. Surgical correction for lower lid epiblepharon in Asians. Br J Ophthalmol. 2000;84(12):1407–1410. doi:10.1136/bjo.84.12.1407
5. Sohn SW, Woo KI, Chang HR. Astigmatism in children with epiblepharon. J Korean Ophthalmol Soc. 2002;43:1827–1832.
6. Kim MS, Lee DS, Woo KI, Chang HR. Changes in astigmatism after surgery for epiblepharon in highly astigmatic children: a controlled study. J Am Assoc Pediatric Ophthalmol Strabismus. 2008;12(6):597–601. doi:10.1016/j.jaapos.2008.06.010
7. Kim NM, Jung JH, Choi HY. The effect of epiblepharon surgery on visual acuity and with-the-rule astigmatism in children. Korean J Ophthalmol. 2010;24(6):325. doi:10.3341/kjo.2010.24.6.325
8. Park SW, Ji YS, Park YG. The effect of surgical correction of epiblepharon on astigmatism in children. J Pediatr Ophthalmol Strabismus. 2008;45(1):31–35. doi:10.3928/01913913-20080101-18
9. Preechawai P, Amrith S, Wong I, Sundar G. Refractive changes in epiblepharon. Am J Ophthalmol. 2007;143(5):835–839.e1. doi:10.1016/j.ajo.2007.01.043
10. Takeuchi M, Matsumura N, Ohno T, Fujita T, Asano M, Mizuki N. Comparing the effectiveness of two surgical techniques for treating lower lid epiblepharon in children: a randomized controlled trial. Sci Rep. 2023;13(1):5857. doi:10.1038/s41598-023-32050-4
11. Hotz FC. A new operation for entropion and trichiasis. Arch Ophthal. 1879;8:249–263.
12. Lee H, Jang S, Park M, Park J, Baek S. Effects of epiblepharon surgery on higher-order aberrations. J Am Assoc Pediatric Ophthalmol Strabismus. 2016;20(3):226–231. doi:10.1016/j.jaapos.2016.01.015
13. Hwang SW, Khwarg SI, Kim JH, Kim NJ, Choung H. Lid margin split in the surgical correction of epiblepharon. Acta Ophthalmol. 2008;86(1):87–90. doi:10.1111/j.1600-0420.2007.01005.x
14. Seo JW, Kang S, Ahn C, Esmaeli B, Sa H-S. Non-incisional eyelid everting suture technique for treating lower lid epiblepharon. Br J Ophthalmol. 2018;102(11):1504–1509. doi:10.1136/bjophthalmol-2017-311635
15. Shiotani Y, Maeda N, Inoue T, et al. Comparison of topographic indices that correlate with visual acuity in videokeratography. Ophthalmology. 2000;107(3):559–564. doi:10.1016/s0161-6420(99)00084-6
16. Maeda N, Sato S, Watanabe H, et al. Prediction of letter contrast sensitivity using videokeratographic indices. Am J Ophthalmol. 2000;129(6):759–763. doi:10.1016/s0002-9394(00)00380-9
17. Lee DH, Jung JH, Ahn JH. Changes in corneal curvature after epiblepharon surgery in children. J Craniofac Surg. 2018;29(2):e191–e195. doi:10.1097/scs.0000000000004235
18. Smolek MK, Klyce SD. Zernike polynomial fitting fails to represent all visually significant corneal aberrations. Invest Ophthalmol Vis Sci. 1997;44(11):4676. doi:10.1167/iovs.03-0190
19. Kandarakis A, Karampelas M, Soumplis V, et al. A case of bilateral self-induced keratoconus in a patient with tourette syndrome associated with compulsive eye rubbing: case report. BMC Ophthalmol. 2011;11(1):28. doi:10.1186/1471-2415-11-28
20. Mcmonnies CW. Mechanisms of rubbing-related corneal trauma in keratoconus. Cornea. 2009;28(6):607–615. doi:10.1097/ico.0b013e318198384f
21. Dongre P, Bothra N, Chaurasia S. Keratoconus in two siblings with congenital distichiasis. Eur J Ophthalmol. 2023;33(4):1553–1557. doi:10.1177/11206721231162441
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.