Back to Journals » Patient Preference and Adherence » Volume 20
Controlling Symptoms versus Minimizing Negative Treatment Impact: A Grounded Theory Study of Heterogeneity in Patient Preferences for Psoriasis Treatments
Authors Szabo SM ![]() , Hawkins NS, Germeni E
, Hawkins NS, Germeni E
Received 19 February 2026
Accepted for publication 24 March 2026
Published 8 April 2026 Volume 2026:20 604216
DOI https://doi.org/10.2147/PPA.S604216
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Shelagh M Szabo, Neil S Hawkins, Evi Germeni
Health Economics & Health Technology Assessment (HEHTA), School of Health and Wellbeing, University of Glasgow, Glasgow, Scotland, UK
Correspondence: Shelagh M Szabo, Health Economics & Health Technology Assessment (HEHTA), School of Health and Wellbeing,University of Glasgow Clarice Pears Building (Level 3), 90 Byres Road Glasgow G12 8TB, Glasgow, Scotland, UK, Email [email protected]
Purpose: Patients vary in preferences for health outcomes, risks, and treatments. However, heterogeneity in patient preferences is not typically considered in health technology assessment (HTA) decision-making. Using plaque psoriasis as a case study, we aimed to provide an in-depth understanding of how preferences are shaped and explore real-world preference heterogeneity subgroups for psoriasis treatments.
Patients and Methods: In this grounded theory study, 38 Canadians with moderate-to-severe psoriasis engaged in one-to-one, semi-structured interviews between October 2023 and December 2024. Theoretical sampling was guided by treatment history, and data collection and analysis occurred in parallel. Data were coded in NVIVO using the constant comparison technique. Themes were developed iteratively, and a conceptual model was developed to illustrate how treatment priorities, personal and contextual factors shape preferences for specific psoriasis therapeutic modalities.
Results: Participant ages ranged from 25 to 66 years; 24 were female, 19 were currently experiencing moderate-to-severe symptoms and 16 had received injectable biologics. We identified that treatment priorities could be grouped under two headings: control of psoriasis symptoms and minimization of negative treatment impact. All participants valued treatment effectiveness, while preferences for other treatment aspects varied. Prioritizing symptom control was also driven by social and emotional factors (such as avoiding stigma and embarrassment, or impact on daily activities) and the need to control multiple comorbid conditions. Those prioritizing the minimization of negative treatment impact often valued treatments that were convenient or easy to take, avoiding “unnecessary” medical treatment, and avoiding adverse events and dependence. Similar underlying preference drivers could result in different reported preferences. While wanting a “convenient” treatment was common, some considered a daily pill ideal and others a monthly injection; according to what fitted best into their current lifestyle. While acceptance of their chronic health condition was a commonly discussed theme, some operationalized this as preferences for more intensive treatments (minimizing psoriasis impact), versus less intensive regimens (minimizing treatment burden). Some participants reported being unable to afford co-payments for treatments they would prefer to take. Preferences varied according to age, psoriasis severity, life stage and treatment experience.
Conclusion: Heterogeneity in patient preferences for aspects of psoriasis impact and treatment translate into a range of different preferences for specific psoriasis therapies. These findings support considering preference heterogeneity in expanding decision-making frameworks to ensure patient voices are considered within HTA.
Keywords: qualitative, treatment experience, healthcare priorities, healthcare decision-making, patient preferences
Introduction
Patients vary in their preferences for specific attributes of treatments, risks, and health outcomes.1–3 Shared clinical decision-making, wherein clinicians and patients jointly select a treatment they judge will best suit an individual patient, acknowledges this heterogeneity in preferences.3 However, this heterogeneity in patient preferences is not typically explicitly considered in decision-making around treatment access, by health technology assessment (HTA) agencies, for example,4–6 despite its importance from both an ethical and outcomes perspective.7 Consideration of heterogeneity in patient preferences not only helps ensure that decisions made for healthcare access are palatable to the people who will use that healthcare; but also may lead to better health outcomes because people are more likely to adhere to their preferred treatments.3,8
Plaque psoriasis is a common chronic inflammatory skin condition that follows a relapsing-remitting course.9–13 While those with mild symptoms may have adequate symptom control using topical agents,14 those with moderate or severe symptoms typically require more intensive systemic treatments including classic immunosuppressive therapies (eg cyclosporin or methotrexate), novel oral small molecules (apremilast or deucravacitinib) or injectable biologics.15,16 A 2017 systematic review including observational and interventional studies of patient preferences and treatment satisfaction noted that patient preferences for psoriasis treatments are heterogeneous. The authors highlighted that some patients place more emphasis on process (eg treatment delivery) vs outcome (eg treatment efficacy) attributes and that preferences change over time.17
Recent quantitative preference studies, including discrete choice experiments (DCEs), have further explored the existence of heterogeneity in preferences for plaque psoriasis treatments, and identified demographic and clinical factors associated with preferences for specific treatment attributes.18 Boeri et al noted that the latent class methods used in those analyses can be particularly valuable for identifying segments in a population for whom to develop alternative treatments;18 this could be individuals whose preferences are not being satisfied with current treatments, or who are unable to take those treatments, for example. However, common criticisms of DCEs include that stated preferences reflect hypothetical, not real-world scenarios and decision-making; and that they can provide a limited understanding of the context underlying eliciting preferences.19,20 Qualitative methods can provide complementary evidence to that generated using quantitative methods, illuminating the broader contextual factors that influence an individual’s perception of their health and the meanings people attach to their health experiences.21 In this case, these methods can provide insight into the mechanisms underlying how treatment preferences develop, and inform an understanding of which alternate treatments may satisfy an individual whose preferences are not being met with available therapies.
Previous qualitative studies in psoriasis have examined aspects such as the symptom experience while on biologics,22 perspectives on dosing,23 and contributors to preferences for systemic psoriasis treatments.24 These methods have also been used to explore the importance of factors such as perceived treatment effectiveness or treatment burden in influencing treatment decision-making among certain subgroups of individuals with psoriasis,25 and to highlight patients’ desire for treatment options that consider individual needs and preferences.26 However, qualitative methods have not yet been used in depth to explore drivers of preferences, and heterogeneity in preferences, across the spectrum of individuals with moderate-to-severe psoriasis. A detailed exploration of patient preferences for the range of available psoriasis therapies, considering factors such as treatment priorities and personal context, is lacking. Grounded theory is a systematic qualitative research approach that aims to construct a theory based on the collection and analysis of real-world data.27 In this case, we developed a theory to explain why particular treatment preferences are reported among those with moderate-to-severe plaque psoriasis, considering the context in which those preferences occur. The objective of this study was therefore to provide an in-depth understanding of how preferences are shaped and explore real-world heterogeneity in preferences for psoriasis treatments and the mechanisms underlying these.
Materials and Methods
Study Design
Between October 2023 and December 2024, a grounded theory study was conducted among a sample of Canadians with plaque psoriasis classified as moderate-to-severe within the preceding two years by a physician. As we were aiming to understand the experience of people with psoriasis in relation to variability in their treatment preferences, as well as the factors underlying this relationship, we selected a grounded theory approach as it explicitly aims to capture the variability and complexity of phenomena.27–30 We adopted an interpretivist approach to grounded theory, which emphasizes the subjective nature in understanding human experiences and creation of reality.31,32
Sampling and Recruitment
Consistent with the grounded theory approach, a theoretical sampling strategy was adopted, which corresponded to the research question. Study participants were initially selected to reflect heterogeneity in psoriasis severity and treatment experience, including past or present experience with injectable biologics, oral therapies, and topicals. We initially aimed to recruit a minimum of 6 people with experience with each of injectable (biologic), oral, and topical experience. Over time, to secure a sufficiently diverse sample and driven by our ongoing assessment of whether theoretical saturation had been achieved (see below), our recruitment strategy evolved to also recruit a minimum of 3 people with experience with novel orals and 3 people who had previously discontinued biologic therapy. We also additionally recruited 3 people without employer-sponsored medication coverage, to better understand the concerns and priorities of this group.
Recruitment occurred through a medical fieldwork recruiter by Email and telephone. Information about the research goals and the consent form were shared with potentially interested participants; those interested and eligible were scheduled for an interview. The participants and researchers had no relationship prior to the study.
Data Collection and Analysis
To inform data collection, a semi-structured interview guide was developed (Appendix A) and pilot tested with two health researchers and one patient with psoriasis. One-on-one Zoom-based interviews were conducted; the use of teleconference-based interviews is preferred by many study participants and allows inclusion of a geographically diverse sample.33,34
To open the interview, informed consent was obtained, both for participation in the interview and for publication of direct quotations. The interviewer also shared a synopsis of the research and the potential implications for healthcare decision-making. Then, participants described the impact of psoriasis on daily life, treatment experience and preferences, and their perceptions of the impact of their personal views and those of their care team on their selected treatment. Participants also provided details of sociodemographics and ethnicity (participants could select more than one option), information on insurance status and any medication co-payments, and details of past and present psoriasis severity and treatments. Prior to the end of the interview, the interviewer summarized the key points discussed for confirmation; interview transcripts were not shared for further review with participants. Memos were drafted after each interview to document interviewer perceptions and initiate comparisons between and within interviews. Interviews lasted 45–60 minutes, were audio-recorded and transcribed. Besides the interviewer and participant, no other individuals were present, and repeat interviews were not conducted. Interview guides were iteratively updated based on insights gathered from the preceding interviews.
Data were collected and analyzed in parallel, using the constant comparison technique.28 Interview transcripts and memos were reviewed and coded in NVIVO 14. Coding was inductive, iterative and first applied line-by-line.28 Open coding was used to label available data according to concepts, perceptions and experiences described; labels were used based on in vivo words where available. Axial coding was then applied to group initial codes and highlight when initial codes varied in relation to which situations. Initial codes were compared within and across transcripts, and categories generated to identify factors associated with treatment preferences and priorities, as well as details of the personal situations in which preferences arose. Selective coding was then applied to group codes according to treatment preferences (based on oral, injectable and topical treatment modalities), treatment priorities, personal factors that contribute to preferences, and contextual factors influencing the relationship between these. Drivers of treatment priorities were categorized and compared between people with differing priorities. Theoretical saturation was fostered through memoing and constant comparison as described above, and analysis occurring concurrent with data collection.28 Theoretical saturation was judged to have been reached when additional data only generated additional examples of existing categories of preference drivers, personal and contextual factors; as noted above, this required additional sampling of key participants groups to achieve.
One female researcher (SMS) trained in qualitative methods conducted all interviews and was responsible for the analysis. The research team met throughout data collection and analysis to consult on the process, discuss key findings and implications, and share insights. Interviewing continued until information saturation was deemed reached, in that no new insight into treatment priorities, preferences, and the drivers underlying these were identified.
Synthesis
Demographic and clinical characteristics of the sample were summarized quantitatively using Microsoft Excel. The coding tree for the analysis was the basis for a conceptual model developed to highlight the relationships between treatment priorities, personal drivers, and contextual factors, with preferences for specific psoriasis therapeutic modalities. Treatment priorities were summarized according to personal drivers. Key factors influencing heterogeneity in preferences were highlighted. These data were used to classify pathways by which individuals could arrive at preferences for oral, topical, or injectable therapies for moderate-to-severe psoriasis; and explore how similar or different preferences could result from individuals with different drivers of preferences and treatment priorities. Participant quotes were selected to illustrate key concepts and categories.
Reflexivity and Ethical Considerations
Consistent with the tenets of grounded theory, efforts were made to limit pre-conceived notions before initiating the project.35 Nonetheless, we acknowledge that prior education and experience would have impacted both the topics under investigation within this study, as well as the interpretation of the data collected. The study team has a shared interest in understanding the applications of preferences in healthcare decision-making, coming from varied backgrounds with expertise in HTA, qualitative research methods, and preferences and quality of life assessment. We also have previous experience and familiarity with evidence submitted to HTA in support of therapeutics for psoriasis. To mitigate the effect of how our backgrounds, pre-existing knowledge and potential biases would impact study design, data collection and analysis, we engaged in reflexive memo writing and team discussions throughout the study. These included ongoing reflection on our perspectives and their influence on the research process, within the interviews themselves, in our initial interpretation of these, as well as in our subsequent analytic and data presentation decisions. These considerations and decisions were documented throughout the data collection and analysis. To ensure the analysis remained grounded in participant experiences, the authors periodically checked assumptions through comparisons within data and with memos, identifying interview-based evidence and quotations for assertions in line with recommended practices.28
This study complied with the tenets of the Declaration of Helsinki and was approved by the Western Copernicus Group Institutional Review Board (Canada; study #1358915) and the Ethics Committee of the College of Medical, Veterinary and Life Sciences at the University of Glasgow (protocol #200230025). The reporting of this study was guided by the COREQ (COnsolidated criteria for REporting Qualitative Research) checklist (Appendix B).36
Results
Participants
Thirty-eight Canadians with moderate-to-severe psoriasis participated; one individual dropped out prior to the interview for personal reasons. Ages ranged from 25 to 66 years and 24 (63.2%) were female (Table 1). Twenty-six individuals (68.4%) self-identified as White, five (13.2%) as Black, four (10.5%) as First Nations, and two (5.3%) as Asian. Three (7.9%) identified as Latin American. Nineteen participants (50.5%) reported having moderate-to-severe symptoms at the time of the interview. Psoriasis plaques typically affected multiple body areas, most commonly the scalp (65.8%), elbows (60.5%) and hands (50.0%); the frequency of symptoms over the past 24 hours is presented in Figure 1. Twelve participants (31.6%) were taking injectable biologics, and four had previously taken a biologic but discontinued due to side effects or perceptions of waning effectiveness. While 33 (86.9%) had insurance coverage for medications, 25 (75.8%) still had some level of copayment. In terms of personal tolerance for healthcare spending, 26 (68.4%) reported being moderately or very sensitive to healthcare costs. Twelve individuals reported they had another autoimmune condition (eg psoriatic arthritis, Crohn’s disease) in addition to plaque psoriasis.
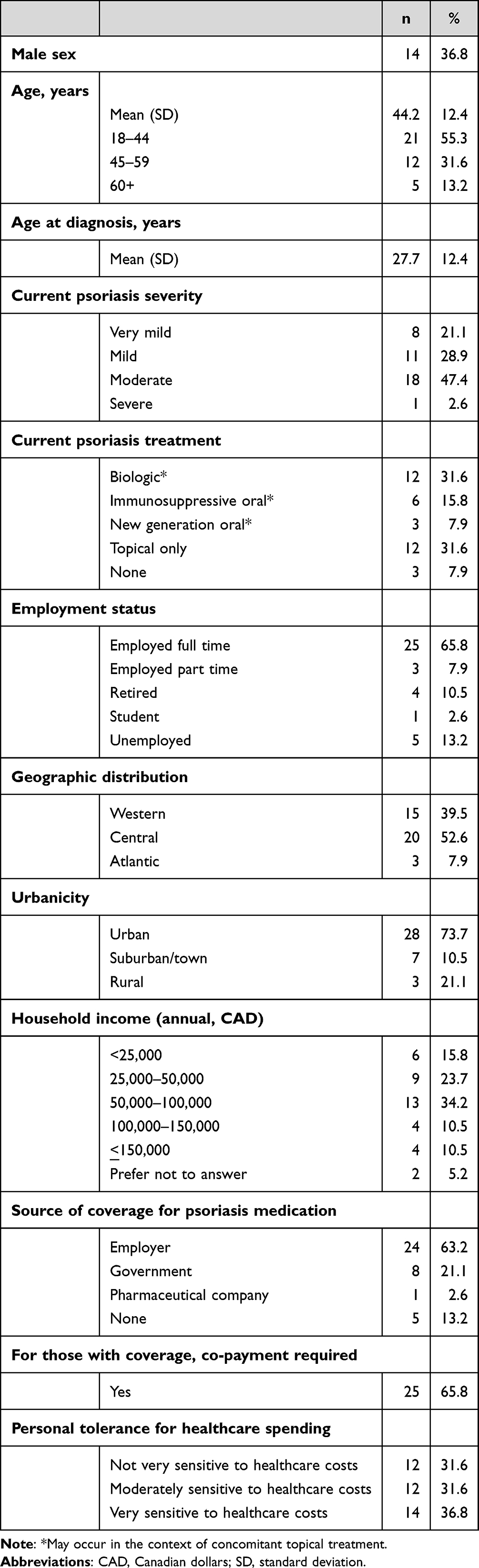 |
Table 1 Key Self-Reported Participant Sociodemographic, Clinical and Personal Characteristics |
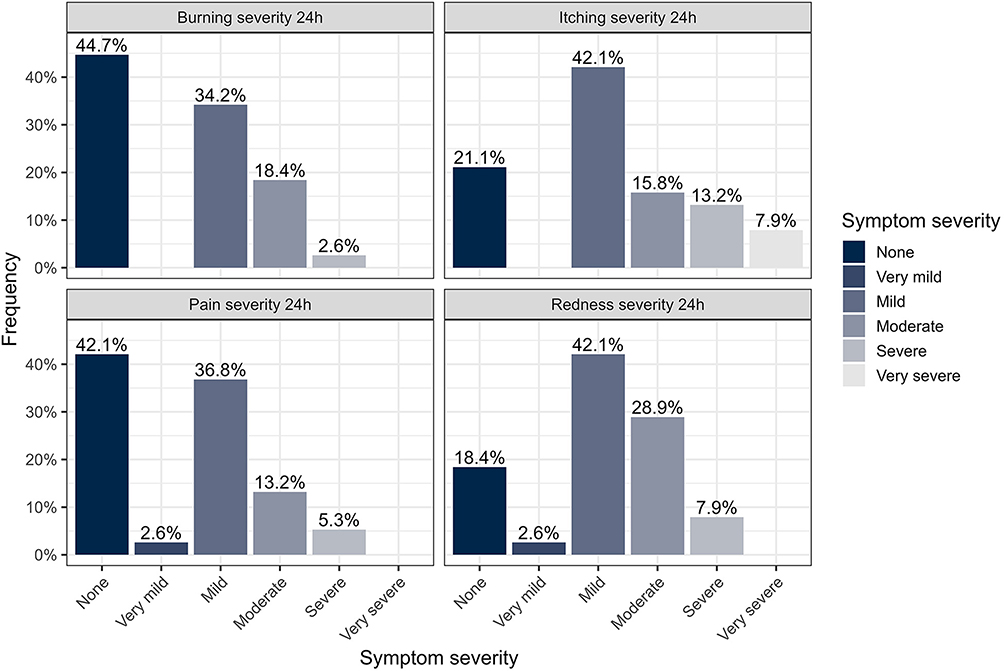 |
Figure 1 The intensity of psoriasis symptoms over the past 24 hours for a) pain, b) redness, c) itching and d) burning. Abbreviations: h, hours. |
Grounded Theory
Analysis of the interview data resulted in a conceptual model describing how treatment priorities interact with personal and contextual factors to produce preferences for specific therapies (Figure 2). The core category of the grounded theory was “heterogeneous treatment preferences”. The model illustrates how participants described varying drivers of preferences related to two governing treatment priorities: controlling psoriasis symptoms, and minimizing negative treatment impact. Observed drivers of those treatment priorities are displayed in Figure 3, and we note that exact drivers of priorities varied by individual. Treatment priorities are influenced by personal factors which include factors related to participants’ degree of acceptance or desire to control their health condition, and their preferences for how they receive and prioritize information related to their health and treatment. Participant narratives also revealed a set of contextual factors described by personal and clinical characteristics that influence both their treatment priorities and the personal factors that govern how they feel about psoriasis and make decisions about their health. The interaction of personal factors, contextual factors and treatment priorities produce an individual’s preference for a particular treatment. As a result, we found that preferences for treatment with oral, injectable and topical therapies varied between individuals with moderate-to-severe psoriasis; and participants provided varying explanations for their preferences. Finally, an individual’s preference for a specific therapy interacts with affordability and jurisdiction-specific treatment access to result in the treatment ultimately selected.
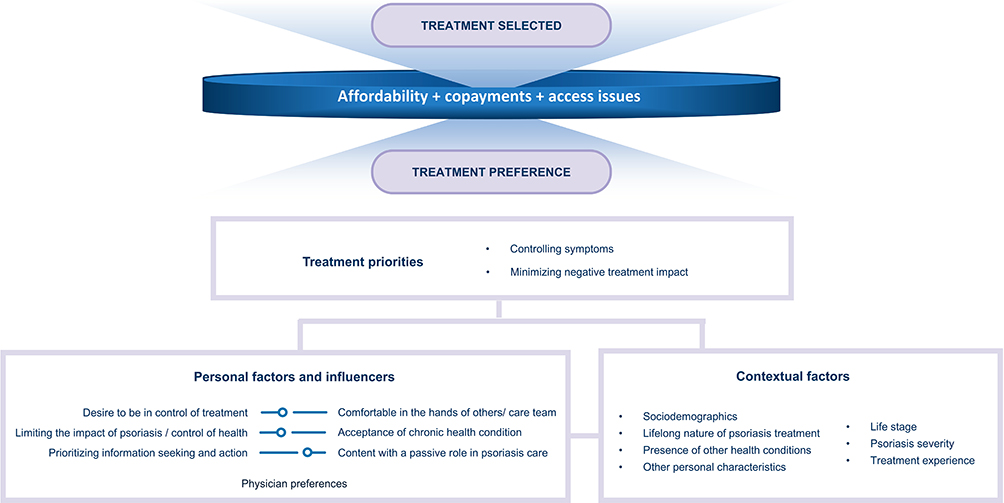 |
Figure 2 Conceptual model illustrating the relationship between treatment priorities, personal and contextual factors in producing treatment preferences; and the impact of affordability, copayments, and access issues in producing the eventual treatment selected. |
 |
Figure 3 Observed drivers of the two governing treatment priorities identified: focusing on controlling symptoms, or minimizing negative treatment impact. |
Treatment Priorities
While many participants expressed a desire to control their symptoms (prioritizing treatment efficacy; 60.5%), others focused on minimizing negative treatment impact (for example, wanting a less invasive or less frequent treatment; 39.5%). Illustrative quotations for drivers of treatment priorities are provided in Table 2. Those who prioritized controlling their symptoms generally preferred a treatment providing benefits traditionally characterized as therapeutic efficacy, including magnitude of symptom control, speed of effect, and consistency in effect over time (Figure 3 and Table 2).
If it’s what’s going to work, then that’s what I want to do. I’m not particularly concerned about invasiveness…if the treatment’s the best one…if it’s what’s going to work to control my symptoms, then that’s what I want to do….Especially because, the most impacted places are my most visible places too, so they’re super important, right? It’s always my hands, face, and mouth… So my main priority is something that works and works quickly for my symptoms. (35-year old male, presently on a topical, mild symptoms)
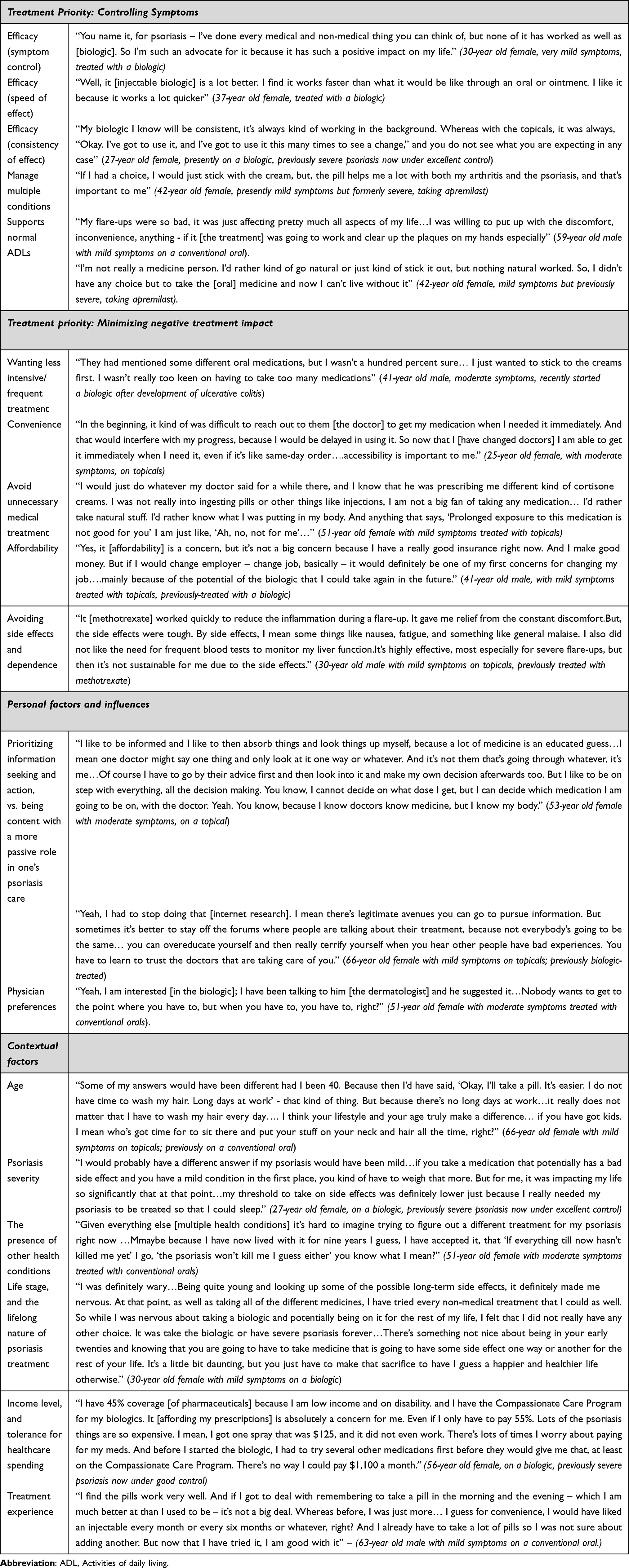 |
Table 2 Participant Quotations Illustrating Heterogeneity in Preferences Due to Differing Treatment Priorities, Personal, and Contextual Factors |
The desire to control symptoms was often prioritized by individuals presently on biologic therapy, and by individuals managing multiple related health conditions. However, prioritizing symptom control was also driven by social and emotional factors. The need for treatments to alleviate feelings of stigma or embarrassment was important, and that treatment can facilitate performing (or resuming) normal life activities was a common theme. Those prioritizing controlling their symptoms also expressed varied modality-specific preferences for symptom control; but related that they will make the treatment “fit” or work for them, even if they think not all of the treatment’s attributes exactly match their preferences: “If it’s the right medication, I’ll make it fit into my lifestyle” (41-year old female, on a topical, mild symptoms).
Not everyone prioritized symptom control, and participants provided a wide range of explanations for their varied preferences. Those who prioritized minimizing negative treatment impact typically preferred a treatment they felt was convenient or easy to take (Figure 3 and Table 2). The implications of a “convenient” treatment varied per individual; and could include, for example, a treatment not requiring clinical visits, one avoiding lifestyle modifications or one that was affordable (see quotes, Table 2). In general, these specifications were viewed by participants as supporting their ability to take, and thereby their adherence to, their treatment. Many of those who prioritized minimizing negative treatment impact were interested in avoiding “unnecessary” medical treatment; which could involve minimizing the amount of medicine one takes, or choosing a minimally invasive or “natural” option. These preferences were typically expressed by participants on less intensive therapies; these individuals also tended to have less well-controlled symptoms.
Avoiding adverse events and dependence was another common driver among those focussing on minimizing negative treatment impact. Many who noted this priority had chosen to discontinue a past treatment because of the side effects, even if they were getting good symptom relief from their therapy. For some, this priority acted as a barrier to trying a potentially more efficacious or tolerable treatment than they had previously tried; for example, among those with poorly controlled symptoms who were reluctant to try a biologic requiring regular injections. These individuals also discussed the need to balance risks of long-term side effects from a treatment for a lifelong condition, against their satisfaction with the degree of present symptom control.
I’ve never really liked pills… Doesn’t matter the type of drug or whatever, it just didn’t make me feel comfortable… But, I’ve always been scared of needles, so I wouldn’t say I really liked it when I was on the injectable. And then there’s the long term risks, you know? So I wouldn’t say I 100% liked it, but it was something that I just had to deal with. Until my psoriasis was a bit better and then I just didn’t want to any more. (26-year old female, presently on a topical with mild symptoms; previously treated with an advanced oral and injectable)
Many of those prioritizing minimizing negative treatment impact expressed a desire for the treatment to fit into their lifestyle as it currently stood, even if this resulted in poorer symptom control.
The treatment should fit into my daily life without being overly time consuming. I feel like convenience is really important because managing psoriasis can already feel like a lot to juggle. Treatments that are quicker, easier to use…things I can apply them at home without disrupting my day…More time consuming treatments can be challenging because they require clinical visits, and this can interfere with my work and other commitments. Also, systemic treatments like methotrexate can involve additional steps, like frequent doctor visits, blood tests – this can feel really overwhelming. So, I value treatment that allows me to maintain my routine without too much extra effort or planning so I can focus on other aspects of my life. (30-year old male with mild symptoms on topicals, previously treated with methotrexate)
Personal Factors and Influences
Heterogeneity in treatment priorities is related to differing underlying personal factors and influences (Figure 2). These personal factors often reflected dichotomies between two conflicting viewpoints; for example, a desire to be in control of one’s treatment, versus a high degree of comfort being in the hands of one’s treatment team, both influence the treatment participants sought.
You have to trust your doctors at some point. I had a specialist … and this is what he was recommending. And, you know, that was his field of study. So I do what he says; you know, I think he knows what he’s talking about better than I do. (66-year old female with mild symptoms on topicals, previously biologic-treated)
In some ways, you’re your own best doctor without the degree. You know how you feel, and what works for you and what doesn’t … Me, I look things up. I look up all my pills. I have a list of all the medication I take. I can tell a doctor, “This is what I’ve done.” So, yeah, I’m informed and aware. You don’t have to explain all this stuff to me…Just get down to it, you know? Get to the point. (41-year old female with moderate symptoms on a conventional oral)
While some participants sought to actively limit the impact of psoriasis on their daily life and emotional status, others worked for acceptance of their chronic health condition. These perspectives also influenced the extent and types of treatments in which participants were interested.
I don’t like giving myself a needle. I really hate it. But what I like is it’s keeping things at bay. My arthritis isn’t flared up as much, and neither is my psoriasis. So for that reason I like it, but I really don’t like giving myself an injection, but I do what I have to do. (63-year old female with moderate symptoms on a biologic)
If things are really highly internally stressful then I’m like, ‘Okay, yeah, I’ll do it [consider a more intensive psoriasis treatment]’…But then I just think ‘Okay, it’s just my skin. That’s okay. I just need to accept my skin as it is (33-year old female with moderate symptoms on a topical)
Relatedly, the extent to which participants prioritized information seeking and action, compared to being content with a more passive role in one’s psoriasis care, also influenced the types of treatments and healthcare pursued. Individuals prioritizing information seeking included those who would choose highly efficacious treatments (if recommended by their physician and supported by their own research). However, this driver also led some highly engaged individuals to choose alternative or less efficacious treatments, depending on the sources of medical information with which they engaged. Heterogeneity in patient treatment priorities and preferences are also contributed to by physician treatment preferences. The exact contribution of physician preferences depends on the extent to which individuals are comfortable being guided by their care team, and how much an individual’s treatment preferences align with those of their physician (Table 2).
How these underlying personal factors produce preferences is also a contributor to heterogeneity. For example, while acceptance of their chronic health condition was commonly discussed, some operationalized this as preferences for less intensive regimens (focusing on reducing the impact of their treatment; as highlighted by P02, above) versus preferring more intensive treatments (to best control their symptoms impact).
I think I’ve accepted my psoriasis now, and that I’m on some serious medications, you know? I’m okay with that because I look at the symptoms, and I’m pretty sure I have PTSD over how bad I was. So, how easy the medication is to take or that kind of thing… Nothing compares to how bad I was. If they told me to jump off of a cliff with a bungee cord, I would’ve done it if it was going to heal me. I can say that confidently because I had zero life worth living when I was really bad. So, I understand that being on biologics could have very potential serious side effects down the road. I mean, I know that some cause cancer and all kinds of kidney problems and that kind of stuff. I have weighed that out. Yeah, no, I would do anything to not go back to the way that it was. (56-year old female on a biologic, previously severe psoriasis now under good control)
Contextual Factors
In addition to preferences varying according to personal factors, they also varied according to contextual factors such as age, psoriasis severity, other comorbid health conditions, life stage, the lifelong nature of psoriasis treatment, and treatment experience. Illustrative quotations for contextual factors are provided in Table 2. Participants related how age and life stage impact their treatment priorities; for example, some reported they had more space for time-consuming or frequent treatments after retirement, compared to when they were working and raising young children. Relatedly, participants expressed how treatment priorities shift in the face of major life events like weddings; and how they factored family planning into treatment choice. Younger participants in particular flagged concerns with the need for a lifelong treatment and potential toxicities over the long term. The presence of other health conditions could have varied effects on treatment priorities; while for some, the idea of one efficacious treatment managing multiple conditions was important, for others the cumulative effect of having to manage multiple conditions increased their interest in choosing a less intensive treatment for their psoriasis.
Income level, as well as tolerance for spending personal money on healthcare, are also important and interact with affordability concerns. While some participants did not highlight affordability as a barrier, others reported being unable to afford co-payments for treatments they would be interested in. Participants also highlighted the potential impact of more costly medications on their wider career choices and lifestyle: Needing to consider level of insurance provided at a new employer was a concern for some presently on biologics. Finally, treatment experience was an important contextual factor, and this effect was multidirectional. Past treatment experiences, including side effects, could both prevent someone from selecting a new treatment entirely, or could contribute to an individual’s perspectives while on treatment (for example, in the case of persistent anxiety about features of a specific treatment). While some who reported an initial preference against a treatment found it acceptable after they started, others expressed disappointment when treatments in which they were interested were intolerable or had low efficacy. Both situations resulted in changes in treatment preferences over time.
How Priorities, Personal, and Contextual Factors Produce Treatment Preferences
We reviewed the pathways by which study participants arrived at preferences for oral, injectable or topical therapies. Preferences for oral and injectable therapies arose from people either preferring to control symptoms or to reduce treatment impact; preferences for topicals arose from a desire to reduce treatment impact or to avoid systemic therapy.
We noted that similar drivers of treatment priority categories could result in different preferred therapies among different people. For people prioritizing a “convenient” treatment, some considered a daily pill ideal and others a monthly injection; according to what fits best into their current lifestyle.
After doing the injections now for a while…I would say I probably prefer an injection to an oral medication just because I don’t have to think about it every day. (27-year old female on a biologic, previously severe psoriasis now under excellent control)
I was used to taking vitamin and herbal pills, so [taking another pill] wasn’t really a big deal for me. I take that first thing in the morning. I have a system on my phone…so, it’s easy enough to remember to take my pills when I need. (41-year old female with moderate symptoms on a conventional oral)
The same preferred therapy could result from people with two different treatment priorities. People prioritizing efficacy (to best control their symptoms) or those who find taking a medicine only once every three months most convenient (to reduce their treatment impact), would both prefer injectable biologics:
I know my biologic will be consistent, it’s always kind of working in the background. Whereas the topicals, it was always, “Okay. I’ve got to use it, and I’ve got to use it this many times to see a change,” and you don’t see it. It was on my mind a lot, like “Okay, I got to use shampoo today”…I found with the injection, just the cognitive load is a lot less, because I know it will work. (66-year old female with mild symptoms on topicals, previously biologic-treated)
I think about the injection twice a month, whereas other medications that I take orally, like every morning you got to go, “Okay, I have to take this.” I prefer it - yeah, I think if I was offered an oral medication, like the same one but orally and daily, I probably would stick with the injection. (27-year old female on a biologic, previously severe psoriasis now under excellent control)
The same preferred therapy could also result from people with two entirely different drivers of a specific treatment priority. People favoring minimally invasive treatments or with needle phobias, for example, would both avoid injectable biologics. As two participants with active symptoms from their psoriasis who are presently on topicals noted,
I want to feel like I’m in control of the psoriasis, not vice versa. Because me using pills, I would take it at any time and just go, you know? Even if I’m rushing somewhere, I just take it and go. But for me to inject myself, it would almost make me feel like I have diabetes or something and it wouldn’t be on my own schedule (28-year old female, presently on a topical, previously treated with a conventional oral)
I’m afraid of needles, and my doctor knows that, so I haven’t been offered an injection, but he’s offered pills and stuff; I’ve never actually tried the injection. I’ve always had a fear of needles, so I get very nervous. …. So, if I can avoid a needle, I will. Another thing about injections that makes me a little bit nervous, especially if it’s a long-acting one… the longevity, you have to wait for it to work its way out of your body, that scares me. If it doesn’t suit you, that makes me quite nervous about long-lasting injections. (38-year old female, presently on a topical with moderate symptoms)
We hypothesize these variations in preferences are related to how treatment priorities, and personal and contextual factors, interact within different individuals. Patterns in interaction between treatment priorities, and personal and contextual factors, observed among study participants are depicted in Figure 4.
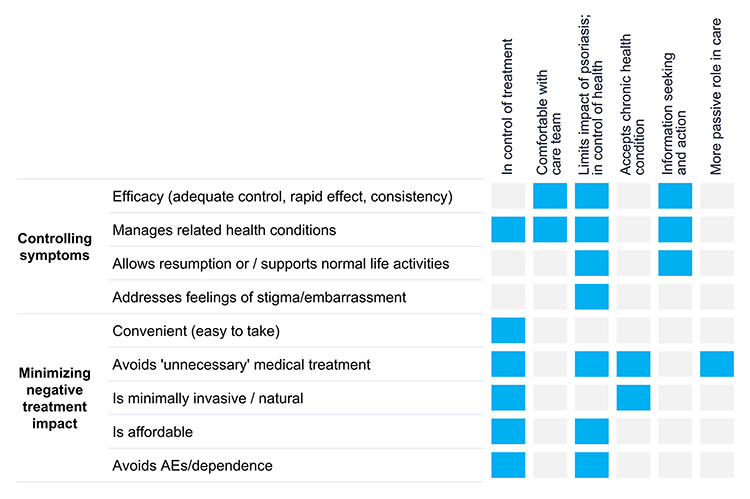 |
Figure 4 Observed interactions of treatment priorities (x axis) and personal factors (y axis) that produce an individual’s treatment preferences. Abbreviations: AE, adverse events. |
Discussion
Variability in treatment priorities, personal factors, and individual contexts can translate into markedly different preferences for specific psoriasis therapies. This study, employing a rigorous grounded theory approach, concluded that while in some individuals there was some overlap, most people were guided by a desire to either maximize control of their symptoms or reduce the negative impact of their treatment.
Individuals with priorities focused on symptom control typically selected injectable biologics or newer-generation oral medications; which is consistent with findings from other studies that individuals selecting biologics place a large importance on treatment efficacy.24,37 Baliela et al, also noted the importance of attributes related to managing symptom burden – particularly, attributes focusing on extent and speed of response – in their thematic analysis of biologic-naïve adults in the Nordic countries.25 Similar to our findings, they also noted the need for a treatment to fit into one’s lifestyle. However, we found that priority expressed by the subset of our sample more focused on managing treatment impact; and that those driven to control their symptoms would make a treatment they wanted to fit into their lifestyle to achieve their desired clinical benefit.
As noted above, for individuals focused on minimizing treatment impact, having a treatment that fits into their lifestyle was a priority, often more than treatment effectiveness. However, what contributed to a good “fit” could vary considerably between individuals, according to factors such as perceived convenience, necessity of intervention, or adverse events of treatment. We noted this priority among both individuals who were naïve to more advanced treatments, and those who chose to discontinue these. The contextual factors providing the motivations among those individuals often differed. While both might prioritize the impact of adverse events when selecting treatments, those who discontinued medicines (particularly biologics) had often selected those treatments for symptom control. Nonetheless, they had to make a choice focused on treatment impact because of tolerability. These two subgroups might be satisfied by different future treatments, which highlights the importance of understanding why people hold the preferences they do (in addition to quantifying the strength of their preferences).
Heterogeneity in preferences for psoriasis treatments has previously been demonstrated in quantitative studies, as has the impact of specific demographic and clinical factors on preferences for treatment attributes.18 For example, the study by Boeri et al, identified how average preference values vary according to different treatment attributes such as dosage characteristics, levels of treatment efficacy, and risk of side effects. They also identified different classes of preferences; for example, they identified a subgroup who prioritized efficacy and a subgroup who preferred to avoid injections. The data from our study complement and extend on those quantitative findings by considering treatment preferences more broadly than according to specific treatment attributes, by exploring mechanisms that can explain how preferences are constructed or why people hold the preferences they do, and by better characterizing the motivations of those who could benefit from alternative treatments. Our study also extends on existing qualitative research by including people with more varied treatment and life experiences, and considering the context and personal factors in which treatment decisions are made, to better understand preference heterogeneity.24,25 Better understanding heterogeneity in preferences for psoriasis treatments is important at the individual level from the patient perspective, to help ensure treatment satisfaction and compliance;24 but also from a health economics perspective, in terms of maximizing patient utility while on treatment.3,8
These qualitative findings are also important for population-level healthcare decision-making because understanding the mechanisms underlying the heterogeneous preferences of patients for psoriasis therapies can reveal how to better align available treatments with patient priorities. For example, one participant selected a biologic because they prioritize symptom control (and will do what is needed to take care of their psoriasis), but at the same time hates injections (ie they have an unsatisfied desire to minimize their treatment impact). This contrasts with another participant, who selected a biologic because they prioritize efficacy, but who also does not mind injections. While the clinical benefit achieved by these two individuals would likely be similar – presuming they take their medication as intended - the utility of the first person could be improved by a treatment with similar efficacy but a modality better aligning with preferences. People who prioritize focusing on treatment impact may adhere better and therefore obtain better clinical results, when using a treatment they like.38 From a healthcare decision-making perspective, this is important as it would facilitate patients achieving the clinical benefits on which economic evaluations are based.3
Also important for population-level decision-making, these findings support the identification of subgroups for whom therapeutic substitutions might better satisfy their preferences. For example, for both someone taking a biologic to limit psoriasis impact but who dislikes injections, and someone who accepts their chronic health condition and uses topicals, an efficacious oral treatment could satisfy their preferences more than their current therapies. We noted that preferences vary based on the alignment of particular treatment aspects with an individual’s underlying personal beliefs and priorities. Identifying patterns of treatment priorities and drivers can help delineate treatment strategies that could satisfy an individual’s preferences, even if their most preferred therapy was unavailable; or to help decision-makers understand the patient-perceived value of approving new therapies, given existing treatment modalities.
Consistent with a 2017 review,17 we also showed that preferences for psoriasis treatments can be heterogeneous. We extended on the considerations of preferences for process vs. outcome attributes, by further investigating the factors underlying such preferences. We also noted how preferences can differ by other factors such as life stage and psoriasis severity. Our conceptual model highlights the importance of other contextual factors in contributing to treatment preferences. This includes treatment affordability, which is a concern for many Canadians with psoriasis and related conditions treated with advanced therapies.39 These findings are therefore relevant to health care systems with private insurance or material co-payments, and findings may differ in countries with different health care contexts – for example, in lower-income countries where access to and experience with biologics may be less. As there are many other geographic (eg climate) and sociocultural factors (eg dress choice) that impact the lived experience of those with psoriasis, the impact of the other contextual and personal factors described in our conceptual model may also vary for individuals in different settings. We focused on providing thick descriptions to support considerations of transferability, and an understanding of relevance of these findings to different contexts.40
The findings of this study are aligned with other qualitative and quantitative studies of preferences in oncology as well as in chronic diseases like diabetes and asthma or chronic obstructive pulmonary disease, that have also identified patient groups interested in prioritizing symptom control versus minimizing aspects of treatment burden.41–44 A key strength of this study is the robust qualitative methodology employed. Grounded theory aims to explain observed behavior and account for variability in experiences,27,29,30 consistent with exploring heterogeneity in treatment preferences. In addition, rather than considering hypothetical treatment scenarios, reported preferences are grounded in real-world treatment experience. Theoretical sampling was performed to ensure a sufficiently large sample with different perspectives to fully develop the grounded theory. Nonetheless, the sample was still community- and volunteer-based and views may not reflect the perspectives of all Canadians with moderate-to-severe psoriasis. In addition, because theoretical sampling was used to guide the selection of participants, we caution that as is true with most qualitative studies the frequencies of patient characteristics observed are not intended to necessarily reflect the characteristics of the wider population with psoriasis.45 We also note that the use of Zoom-based interviews could have introduced the selection of a more technology-comfortable sample.46
A single researcher performed the interviewing and analysis with consultation from the wider study team, a strategy which may be criticized for producing skew in the data or lack replicability. We attempted to mitigate the effects of this design feature through the use of strategies such as memoing and practicing reflexivity,47 and although the data were coded by a single researcher the categories describing the theory itself were developed through regular review and discussion with the wider study team.
We also note that, due to restricted access at present, it was somewhat challenging to identify individuals with contemporary experience with newer generation orals – however, we were eventually able to recruit three such participants. Preferences in this study are based on real-world prior experiences and contrasting with preferences of treatment-naïve individuals, or hypothetical treatment preferences derived from DCEs for example, may provide valuable additional context. How consistent these findings would be in jurisdictions where treatment access differs, is unclear.
Conclusion
We explored the reasons and mechanisms underlying preferences for psoriasis treatments, documenting heterogeneity. Understanding these mechanisms can provide insight into how to potentially better align available treatments to patient priorities at the population level, as well as improve an individual’s utility while on treatment. The findings from this study also highlight potential treatment options for those with psoriasis whose preferences are not satisfied by existing therapies. Ideally, the findings of this study will help provide context for potential approaches to better support care in this population and inform discussions between patients and physicians about treatments that would best suit individual patients. These findings can also provide considerations to help improve the design of preference studies and economic evaluations, and support the importance of incorporating patient priorities into HTA to ensure population-level healthcare decisions align with patient preferences.
Abbreviations
ADL, Activities of daily living; AE, Adverse events; COREQ, COnsolidated criteria for REporting Qualitative Research; DCE, Discrete choice experiments; H, Hours; HTA, Health technology assessment; PTSD, Post traumatic stress disorder; SD, Standard deviation.
Data Sharing Statement
The datasets produced during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Western Copernicus Group Institutional Review Board (Canada; study #1358915) and the Ethics Committee of the College of Medical, Veterinary and Life Sciences at the University of Glasgow (protocol #200230025). Informed consent was obtained from all participants.
Acknowledgment
An abstract related to this paper was presented at the Professional Society of Pharmacoeconomics & Outcomes Research’s 2025 European meeting, as a poster presentation of interim findings. The poster’s abstract was published in “Poster Abstracts” in Value in Health: https://www.valueinhealthjournal.com/article/S1098-3015(24)06378-2/pdf.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Buckell JV, A D, Quaife M, Regier DA, Quaife M. Utility maximization versus regret minimization in health choice behavior: evidence from four datasets. Health Econ. 2022;31(2):363–18. doi:10.1002/hec.4455
2. Mulligan K, Baid D, Doctor JN, Phelps CE, Lakdawalla DN. Risk preferences over health: empirical estimates and implications for medical decision-making. J Health Econ. 2024;94:102857. doi:10.1016/j.jhealeco.2024.102857
3. Brazier JE, Dixon S, Ratcliffe J. The role of patient preferences in cost-effectiveness analysis: a conflict of values? Pharmacoeconomics. 2009;27(9):705–712. doi:10.2165/11314840-000000000-00000
4. Lavelle TA, Kent DM, Lundquist CM, et al. Patient variability seldom assessed in cost-effectiveness studies. Med Decis Mak. 2018;38(4):487–494. doi:10.1177/0272989X17746989
5. Hiligsmann M, Liden B, Beaudart C, et al. HTA community perspectives on the use of patient preference information: lessons learned from a survey with members of HTA bodies. Int J Technol Assess Health Care. 2024;40(1):e17. doi:10.1017/S0266462324000138
6. National Institute for Health and Care Excellence. NICE health technology evaluations: the manual. 2022; Available from: https://www.nice.org.uk/process/pmg36/chapter/economic-evaluation.
7. Bridges JFP, de Bekker-Grob EW, Hauber B, et al. A roadmap for increasing the usefulness and impact of patient-preference studies in decision making in health: a good practices report of an ispor task force. Value Health. 2023;26(2):153–162. doi:10.1016/j.jval.2022.12.004
8. Swift JK, Callahan JL, Cooper M, Parkin SR. The impact of accommodating client preference in psychotherapy: a meta-analysis. J Clin Psychol. 2018;74(11):1924–1937. doi:10.1002/jclp.22680
9. Bu J, Ding R, Zhou L, Chen X, Shen E. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol. 2022;13:880201. doi:10.3389/fimmu.2022.880201
10. Mantovani L, Medaglia M, Piacentini P, et al. Burden of moderate-to-severe plaque psoriasis and new therapeutic approaches (secukinumab): an italian perspective. Dermatol Ther. 2016;6(2):151–167. doi:10.1007/s13555-016-0114-9
11. Gisondi P, Bellinato F, Girolomoni G, Albanesi C. Pathogenesis of chronic plaque psoriasis and its intersection with cardio-metabolic comorbidities. Front Pharmacol. 2020;11:117. doi:10.3389/fphar.2020.00117
12. Ko SH, Chi CC, Yeh ML, Wang SH, Tsai YS, Hsu MY. Lifestyle changes for treating psoriasis. Cochrane Database Syst Rev. 2019;7(7):Cd011972. doi:10.1002/14651858.CD011972.pub2
13. Treloar V. Integrative dermatology for psoriasis: facts and controversies. Clin Dermatol. 2010;28(1):93–99. doi:10.1016/j.clindermatol.2009.03.016
14. Elmets CA, Korman NJ, Prater EF, et al. Joint AAD-NPF Guidelines of care for the management and treatment of psoriasis with topical therapy and alternative medicine modalities for psoriasis severity measures. J Am Acad Dermatol. 2021;84(2):432–470. doi:10.1016/j.jaad.2020.07.087
15. Menter A, Gelfand JM, Connor C, et al. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J Am Acad Dermatol. 2020;82(6):1445–1486. doi:10.1016/j.jaad.2020.02.044
16. Menter A, Strober BE, Kaplan DH, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029–1072. doi:10.1016/j.jaad.2018.11.057
17. Florek AG, Wang CJ, Armstrong AW. Treatment preferences and treatment satisfaction among psoriasis patients: a systematic review. Arch Dermatol Res. 2018;310(4):271–319. doi:10.1007/s00403-018-1808-x
18. Boeri M, Saure D, Schacht A, Riedl E, Hauber B. Modeling heterogeneity in patients’ preferences for psoriasis treatments in a multicountry study: a comparison between random-parameters logit and latent class approaches. Pharmacoeconomics. 2020;38:593–606. doi:10.1007/s40273-020-00894-7
19. de Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. doi:10.1002/hec.1697
20. Vass C, Rigby D, Payne K. The role of qualitative research methods in discrete choice experiments. Med Decis Mak. 2017;37(3):298–313. doi:10.1177/0272989X16683934
21. Popay J, Williams G. Qualitative research and evidence-based healthcare. J R Soc Med. 1998;91(Suppl 35):32–37. doi:10.1177/014107689809135S08
22. Trettin B, Feldman SR, Andersen F, Danbjorg DB, Agerskov H. A changed life: the life experiences of patients with psoriasis receiving biological treatment. Br J Dermatol. 2020;183(3):516–523. doi:10.1111/bjd.18876
23. van der Schoot LS, Verhoef LM, van Ee I, et al. Patients’ perspectives towards biologic dose reduction in psoriasis: a qualitative study. Arch Dermatol Res. 2023;315(6):1735–1745. doi:10.1007/s00403-023-02566-w
24. Zaino M, Parks E, McNeil J, Feldman S. Patients’ preferences regarding modes of systemic psoriasis treatment - a qualitative study. J Psoriasis Psoriatic Arthritis. 2024;9(4):136–142. doi:10.1177/24755303241253200
25. Balieva FN, Catton L, Clareus BW, et al. Treatment preferences in young adults with moderate to severe psoriasis: a qualitative study from the nordic countries. Dermatol Ther. 2023;13(8):1873–1887. doi:10.1007/s13555-023-00973-5
26. Khoury LR, Skov L, Moller T. Facing the dilemma of patient-centred psoriasis care: a qualitative study identifying patient needs in dermatological outpatient clinics. Br J Dermatol. 2017;177(2):436–444. doi:10.1111/bjd.15292
27. Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago: Aldine Publishing Co; 1967.
28. Strauss A, Corbin J. Basics of Qualitative Research: Procedures and Tehcniques for Developing Grounded Theory. Thousand Oaks: Sage; 1998.
29. Holton JA. Grounded Theory as a general research methodology. The Grounded Theory Rev. 2008;7(2):67–93.
30. Annells M. Grounded theory method: philosophical perspectives, paradigm of inquiry, and postmodernism. Qual Health Res. 1996;6:379. doi:10.1177/104973239600600306
31. Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluation criteria. Qual Sociol. 1990;13(1):3–21. doi:10.1007/BF00988593
32. Weed M. Capturing the essence of grounded theory: the importance of understanding commonalities and variants. Qual Res Sport Exerc Health. 2017;9(1):149–156. doi:10.1080/2159676X.2016.1251701
33. Archibald MM, Ambagtsheer RC, Casey MG, Lawless M. Using zoom videoconferencing for qualitative data collection: perceptions and experiences of researchers and participants. Int J Qual Methods. 2019;18:1609406919874596. doi:10.1177/1609406919874596
34. Oliffe JL, Kelly MT, Gonzalez Montaner G, Yu Ko WF. Zoom interviews: benefits and concessions. Int J Qual Methods. 2021;20:16094069211053522. doi:10.1177/16094069211053522
35. Creswell JW, Poth CN. Qualitative Inquiry and Research Design: Choosing Among Five Approaches.
36. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
37. Gorelick J, Shrom D, Sikand K, et al. Understanding treatment preferences in patients with moderate to severe plaque psoriasis in the USA: results from a cross-sectional patient survey. Dermatol. Ther. 2019;9(4):785–797. doi:10.1007/s13555-019-00334-1
38. Losi S, Berra CCF, Fornengo R, Pitocco D, Biricolti G, Feredrici MO. The role of patient preferences in adherence to treatment in chronic disease: a narrative review. Drug Target Insights. 2021;15:13–20. doi:10.33393/dti.2021.2342
39. Bever A, Dunne J, Reynolds J, et al. Exploring perceptions of biologic therapies: a qualitative study among canadians living with severe asthma. Adv Ther. 2024;41(4):1401–1418. doi:10.1007/s12325-024-02803-2
40. Tracy SJ. Qualitative quality: eight “big-tent” criteria for excellent qualitative research. Qual Inq. 2010;16(10):837–851. doi:10.1177/1077800410383121
41. Baggott C, Chan A, Hurford S, et al. Patient preferences for asthma management: a qualitative study. BMJ Open. 2020;10(8):e037491. doi:10.1136/bmjopen-2020-037491
42. Calhoun SR, Vass C, Myers K, et al. Patient preferences for adjuvant therapy in renal cell carcinoma: a discrete-choice experiment. Future Oncol. 2025;21(7):843–851. doi:10.1080/14796694.2025.2463276
43. Dombeck C, Swezey T, Gonzalez Sepulveda JM, et al. Patient perspectives on considerations, tradeoffs, and experiences with multiple myeloma treatment selection: a qualitative descriptive study. BMC Cancer. 2023;23(1):65. doi:10.1186/s12885-022-10458-x
44. Ozdemir S, Baid D, Verghese NR, et al. Patient preferences for medications in managing type 2 diabetes mellitus: a discrete choice experiment. Value Health. 2020;23(7):842–850. doi:10.1016/j.jval.2020.01.023
45. Sandelowski M. Real qualitative researchers do not count: the use of numbers in qualitative research. Res Nurs Health. 2001;24(3):230–240. doi:10.1002/nur.1025
46. Lobe B, Morgan DL, Hoffman K. A systematic comparison of in-person and video-based online interviewing. Int J Qual Methods. 2022;21:16094069221127068. doi:10.1177/16094069221127068
47. Berger R. Now I see it, now I don’t: researcher’s position and reflexivity in qualitative research. Qual Res. 2015;15(2):219–234. doi:10.1177/1468794112468475
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.