Back to Journals » International Journal of Nanomedicine » Volume 11
Controlled release of curcumin from curcumin-loaded nanomicelles to prevent peritendinous adhesion during Achilles tendon healing in rats
Authors Zhang W, Li X, Comes Franchini M ![]() , Xu K, Locatelli E, Martin R
, Xu K, Locatelli E, Martin R ![]() , Monaco I, Li Y
, Monaco I, Li Y ![]() , Cui S
, Cui S
Received 8 January 2016
Accepted for publication 28 February 2016
Published 22 June 2016 Volume 2016:11 Pages 2873—2881
DOI https://doi.org/10.2147/IJN.S103867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Carlos Rinaldi
Weizhong Zhang,1 Xuanyi Li,2 Mauro Comes Franchini,3 Ke Xu,1 Erica Locatelli,3 Robert C Martin,2 Ilaria Monaco,3 Yan Li,2 Shusen Cui1
1Department of Hand Surgery, China-Japan Union Hospital, Jilin University, Changchun, People’s Republic of China; 2Division of Surgical Oncology, Department of Surgery, University of Louisville School of Medicine, Louisville, KY, USA; 3Department of Industrial Chemistry “Toso Montanari”, University of Bologna, Bologna, Italy
Abstract: We introduced curcumin-loaded nanomicelles into a tendon-healing model to evaluate their effects on tendon healing and adhesion. Three groups consisting of 36 rats underwent rupture and repair of the Achilles tendon. The treatment group received an injection of curcumin-loaded nanomicelles (gold nanorods [GNRs]-1/ curcumin in polymeric nanomicelles [curc@PMs] at a dosage of 0.44 mg curcumin/kg in 0.1 mL saline) into the surgical site and exposed to laser postoperatively at weeks 1, 2, and 3, for three times 10 seconds each, on the surgical site in the rats that underwent tendon rupture and repair, while the other two groups received 0.44 mg curcumin/kg in 0.1 mL saline and 0.1 mL of saline, respectively. The specimens were harvested at 4 weeks and subjected to biomechanical and histological evaluation. The scoring results of tendon adhesion indicated that GNRs-1/curc@PMs group was in the lowest grade of peritendinous adhesions compared to the other groups. Histological assessment further confirmed the preventive effect of GNRs-1/curc@PMs on tendon adhesion. These findings indicated greater tendon strength with less adhesion in the group treated with GNRs-1/curc@PMs combined with laser exposure, and that nanoparticle-based therapy may be applied to prevent adhesion in clinical patients.
Keywords: nanorods, peritendinous adhesion, curcumin
Introduction
Tendon adhesion is one of the most concerning complications after surgical repair of flexor tendon injury.1 Tendon adhesion binds the flexor tendons with each other, which restricts normal tendon gliding and consequently leads to poor functional recovery. In spite of improvements in surgical technique and postoperative mobilization, postoperative tendon adhesion still presents a major clinical problem in hand surgery.2 During tendon healing, a combination of intrinsic and extrinsic processes occurs simultaneously. Intrinsic healing occurs within the tendon as a result of the activity of tenocytes and appropriate nutrition available to them. Extrinsic healing occurs through the chemotaxis of the specialized fibroblasts into the defect from the ends of the tendon sheath.3 Tendon adhesion results primarily from an excessive fibrotic response between the tendons and the synovial sheath.4 With increasing information available concerning the nature of the scar tissue responsible for the peritendinous adhesions, control of excessive scar formation is essential to restore the functional integrity of a healing tendon after surgery.
Many adjunctive modalities have been explored as a means of primarily reducing adhesions. Anti-fibrotic, anti-inflammatory, and anti-oxidation strategies have been proposed to prevent tendon adhesion.5,6 However, the attempts at systemic treatment have not been successful because of several limitations: 1) Systemic treatment may not have efficient bioavailability of drugs to alter the cellular and molecular milieu in which the tendon heals. 2) The systemic-treated drugs may not achieve required pharmacokinetics because of short half-life for the prolonged periods of healing and adhesion. 3) Inflammation is a common early event of tissue healing; prolonged period of inhibition of inflammation may impair tendon healing. Nanoparticles, with controlled drug release ability, have been popularly used in drug delivery.7–9 Due to the nano-size range, nanoparticles containing drug could overcome the above-mentioned limitations.
Previously, Ag nanoparticles incorporated in poly(L-lactide) fibrous membranes were used in preventing adhesion as well as decreasing inflammation without significant cytotoxicity.10,11 Recently, a strategy of simultaneously loading lipophilic gold nanorods (GNRs) and curcumin into polymeric nanomicelles (GNRs-1/curc@PMs) made of biocompatible PLGA-b-PEG copolymer through a double re-emulsification process has been developed and used for in vivo treatment.12 Our synthesized novel nanosystem, GNRs-1/curc@PMs, was demonstrated to be safe and effective in treating premalignant esophageal adenocarcinoma. Most importantly, curcumin release from GNRs-1/curc@PMs was controllable:12 indeed, GNRs are considered particularly as attractive agents for hyperthermia-based treatments, and they were recently exploited for laser-induced and selective rupturing of polymeric capsule.13,14 As we know, curcumin shows strong antioxidant and anti-inflammatory activities, and over 7,000 articles have discussed the molecular basis of curcumin’s attributed antioxidant, anti-inflammatory, antibacterial, antiapoptosis, anticancer, and related activities in the past 2 decades.15 In a rat tendon injury model, curcumin significantly improved the healing and function of injured tendon.16 The improvement of tendon healing and function was through its antioxidant and anti-inflammatory properties which associated with well-organized collagen fiber and extensive deposition of collagen in the regenerated tendon tissues.16
In this study, we proposed to use GNRs-1/curc@PMs by local administration with controlled release of curcumin to reduce tendon adhesion. We investigated the effects of GNRs-1/curc@PMs on tendon healing and adhesion in a rat model. We found that local administration of GNRs-1/curc@PMs combined with near-infrared (NIR) light exposure can prevent peritendinous adhesion during Achilles tendon healing.
Materials and methods
Preparation of lipophilic GNRs-1
GNRs stabilized with the surfactant agent hexadecyltrimethylammonium bromide (GNRs-CTAB) were prepared following reported procedures in a batch scale of 300 mL, and GNRs with an aspect ratio (length/width) equal to 5, having a length of ~50 nm and a width of ~10 nm, were obtained.17 After purification, GNRs-CTAB were incubated with a specifically designed ligand (ethyl 11-mercaptoundecanoate, organic ligand 1) dissolved in ethanol for 24 hours in order to obtain lipophilic GNRs (GNRs-1) and to completely remove the surfactant CTAB, which is known to be cytotoxic.18 After the ligand exchange, GNRs-1 became lipophilic and easily re-dispersible in common organic solvents like chloroform or dichloromethane and were entrapped into polymeric micelles.
Preparation of GNRs-1/curc@PMs
GNRs-1/curc@PMs were prepared as reported previously.12 In brief, 100 mg of PLGA-b-PEG-COOH was solubilized in 10 mL of CH2Cl2 containing GNRs-1, and then 100 mL of ultrapure water was slowly added: the mixture was emulsified with a tip probe sonicator (600 W input, 1 minute, 80% amplitude). Ten milligrams of curcumin was dissolved in 10 mL of CH2Cl2, and then 100 mL of ultrapure water was slowly added: the mixture was emulsified with a tip probe sonicator (600 W input, 1 minute, 80% amplitude). Afterward, the two solutions were mixed together and re-emulsified (1 minute, 80% amplitude) in order to allow micelles formation and creation of nanocarriers containing both GNRs and curcumin. The residual organic solvent was evaporated under reduced pressure. The particles were then concentrated and purified with a centrifugal filter device (Amicon Ultra, Ultracel membrane with 100,000 NMWL; Millipore, Billerica, MA, USA), washed with water, and filtered on a 0.22 μm polyether sulfone Sterivex™-GP syringe filter (Millipore).
Surgical model of tendon rupture and repair, treatments, and laser exposure
Eight-week-old Sprague Dawley rats were housed and given commercial rat chow and tap water, and maintained on a 12-hour light/dark cycle. They were allowed to acclimate for 2 weeks prior to surgery. Solid food was withdrawn 1 day before the surgery. A total of 30 rats were used to perform the procedure of tendon rupture and repair (TRR), and randomly divided into three groups: TRR + GNRs-1/curc@PMs + laser, TRR + curcumin, and TRR + saline. Each experimental group consisted of ten rats. This study was conducted according to the experimental practices and standards approved by the Animal Welfare and Research Ethics Committee from Jilin University in China. Animal care and used guidelines were in accordance with the guidelines outlined by the National Technical Committee on Laboratory Animal Science of the Standardization Administration of China.
To establish the model of TRR, the animals were anesthetized with 60 mg/kg of sodium pentobarbital, and the pedal reflex was used to monitor the depth of anesthesia. The skin at the incision site was epilated using hair remover before surgery. All surgical procedures were carried out under general anesthesia in sterile conditions. A 2 cm incision was made above the right Achilles tendon, and the superficial Achilles tendon was exposed and isolated. The peritendon was transected with a size 15 scalpel blade perpendicular to the collagen fibers, creating a rupture from 5 mm proximal to the calcaneal insertion of the tendon (Figure 1A). The plantar tendon was transected to prevent an internal splint phenomenon. After transection, the Achilles tendon was sutured back together with Prolene 0-4 with a Kessler–Kirchmeyer stitch (Figure 1B). For the treatments, the rats were injected 0.1 mL of GNRs-1/curc@PMs, at a dosage of 0.44 mg curcumin/kg, into the proximal and distal tendon around the anastomotic site (Figure 1C). Two control groups were injected with 0.1 mL of curcumin solution at a dosage of 0.44 mg curcumin/kg and 0.1 mL saline, respectively, into the proximal and distal tendon around the anastomotic site as curcumin control and saline control. After treatments, the incision was stitched, and the lag was splinted by plastic plates (Figure 1D and E). All the animals were monitored for signs of pain and infection postoperation. The animals were allowed unrestricted cage movement. The TRR of animals was performed for the laser exposure. The light source used for the NIR exposure was DPSSL MDL-N-808-10W (CNIOI Co, Ltd, Changchun, People’s Republic of China), with a wavelength of 808 nm. Indeed, an 808 nm incident laser wavelength is generally preferred over other wavelengths, since it falls in the so-called biological window where the absorption of radiation by hemoglobin and water is at a minimum: this results in a reduced absorption of the laser by tissues, and thus in a better light penetration. For the laser exposure, the power density was optimized by a pilot study, and 3 W/cm2 was chosen as the working scale for NIR light exposure, while the distance between mice and laser source was kept at 20 cm. The laser exposure was performed postoperatively at weeks 1, 2, and 3, for totally three times, 10 seconds each (Figure 1F). The animals that underwent TRR were euthanized at 4 weeks. The entire repaired Achilles tendon of rats was harvested for macroscopic evaluation, biomechanical, and histological examination. This study was conducted according to the experimental practices and standards approved by the Animal Welfare and Research Ethics Committee at Jilin University.
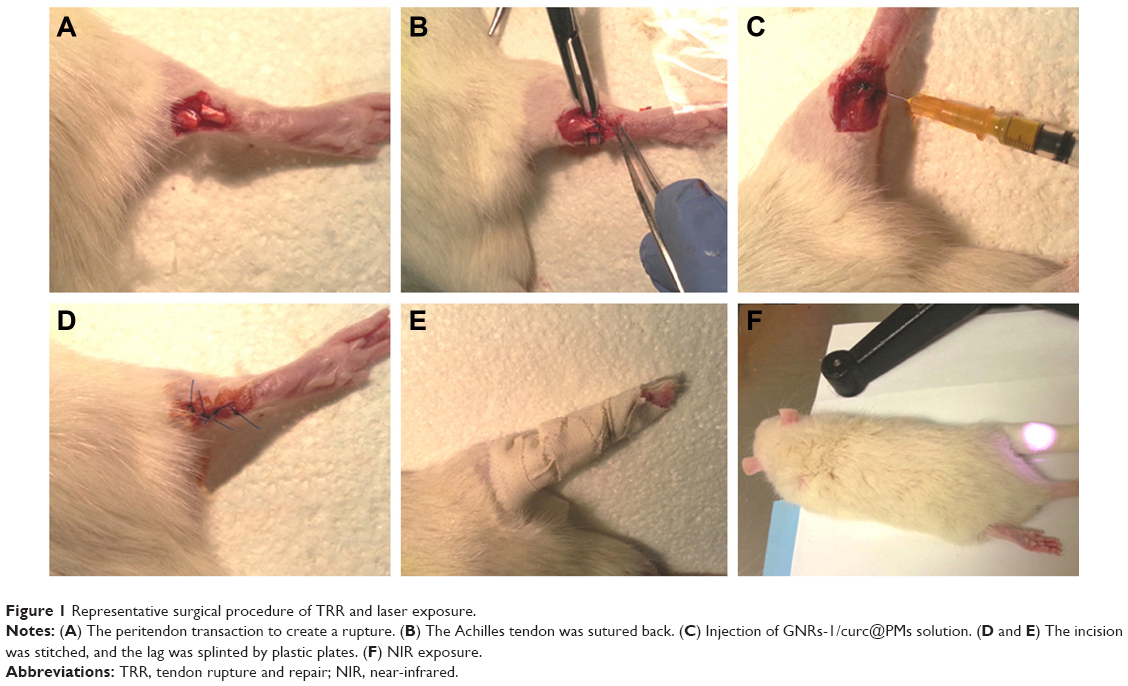 | Figure 1 Representative surgical procedure of TRR and laser exposure. |
Macroscopic evaluation and peritendinous adhesion scoring
Before sacrificing the animals, the surgical site was reopened, and the repaired Achilles tendon was visually examined for signs of inflammation or ulceration. The severity of peritendinous adhesion was evaluated by an adhesion scoring system19 that was used to grade a particular area based on the surgical findings: grade 1, no adhesion; grade 2, adhesion area can be separated by blunt dissection alone; grade 3, adhesion area ≤50% which requires sharp dissection for separation; grade 4, adhesion area of 51%–97.5% which requires sharp dissection for separation; and grade 5, adhesion area of >97.5% requiring sharp dissection for separation. This was performed subjectively by an investigator skilled in performing surgery but blinded to the treatment groups to eliminate any bias.
Biomechanical evaluation of Achilles tendon that underwent TRR
The Achilles tendons that underwent TRR from four animals were used for biomechanical evaluation. To evaluate tensile strength and toughness, the gliding distance and the breaking force of those Achilles tendons were measured using a rheometer (Instron 5548; Instron, Norwood, MA, USA). To evaluate the gliding distance of flexion, the proximal end of the Achilles tendon was fixed to a force gauge, and the distal end of rat tibia was attached to the other end of the device with a clamp. The displacement (mm) was measured when the Achilles tendon was pulled at 20 mm/min until the 50 N maximum tension. The gliding distance of flexion was then recorded. To evaluate breaking force, the proximal and distal ends of the Achilles tendon were fixed to the force gauge of the rheometer. The tendon was pulled apart at a speed of 20 mm/min until rupture of the tendon occurred, and the breaking force was recorded by the rheometer.
Histological examination and grading
The repaired Achilles tendon tissues from six animals were used for the histological examination and immunohistochemical assay. The tendon tissues were fixed in 4% buffered formalin (pH 7.4) for 72 hours. The formalin-fixed tendon tissues were embedded in paraffin. Serial sections of 5 μm were mounted onto glass slides for histopathological and immunohistochemical analysis. Slides of each sample were stained with hematoxylin and eosin for the histological study. They were viewed under a light microscope. Five regions were evaluated for each sample (center of tendon, left border, right border, 2 mm above tendon center, and 2 mm below tendon center). The slides were evaluated in a blinded manner by visual inspection. Histologic grading methods were used to standardize both the extent of adhesions and the peritendinous inflammation among the groups. The extent of adhesions was classified into four grades (1, no adhesions; 2, slight adhesions; 3, moderate adhesions; and 4, severe adhesions) according to the histologic grading criteria published by Tang et al.20 The peritendinous inflammatory reaction was classified into five grades (0, no reaction; 1, minimal leukocyte infiltration into fibro-osseous tendon sheath; 2, leukocyte infiltration in synovium and epitenon; 3, leukocyte infiltration in synovium and endotenon; and 4, diffuse leukocyte infiltration) according to the criteria of Moran et al.21 The histologic grading was evaluated microscopically by two pathologists who were blinded to the treatment groups.
Statistical analysis
Student’s t-tests assuming unequal variance were performed. The results were expressed as mean values ± standard deviation. Comparisons were made among the bile perfusion groups and saline control groups by analysis of variance. A P-value of <0.05 was considered statistically significant.
Results
Analysis of GNRs-1/curc@PMs
The preparation of the micelles containing GNRs-1/curc@PMs was achieved by using the oil-in-water technique and by exploiting a methodology already optimized by us.22 The obtained GNRs-1@PMs were characterized by means of dynamic light scattering, atomic absorption analysis, transmission electron microscopy, UV–vis analysis, and gravimetric analysis. The dynamic light scattering showed a hydrodynamic diameter of 119.0±1.6 nm with a narrow size distribution (Polidispersity index =0.282±0.030) and a ζ-potential value of −41.6 mV (Figure 2A). The transmission electron microscopy images confirmed the entrapment of GNRs into micelles and the integrity of their structure (Figure 2B). The UV–vis analysis confirmed the optical properties of GNRs and curcumin (Figure 2C). Gold concentration was found to be 98 ppm, corresponding to a solution 0.53 mM, while curcumin concentration was determined to be 2.2 mM. We calculated that the two moieties were entrapped into polymeric micelles with a yield of 44% for GNRs and 41% for curcumin.
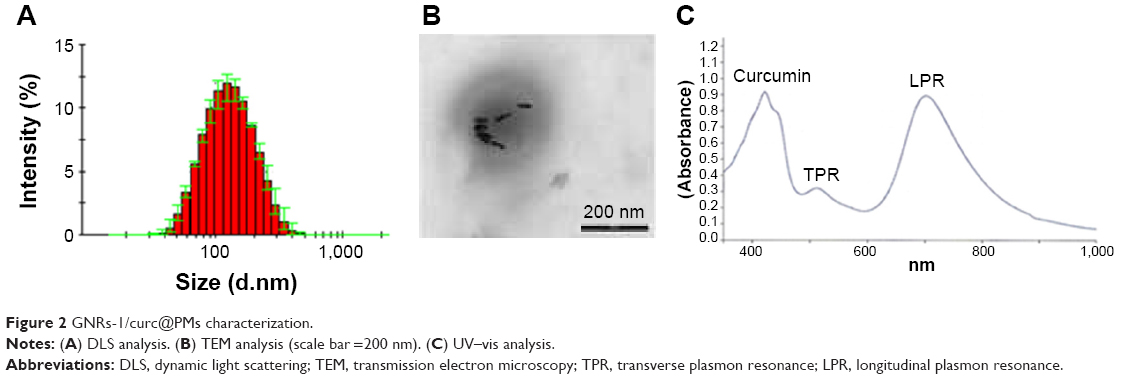 | Figure 2 GNRs-1/curc@PMs characterization. |
Macroscopic findings
One week postoperation, the skin incision healed well in all rats. There was no significant infection around the sutured incision. The animals walked in their cages without any difficulty, and they received post-op NIR light exposure for three times at surgical sites of Achilles tendons. Four weeks after TRR surgery, all the animals were sacrificed, and the Achilles tendons were observed macroscopically. The Achilles tendons that underwent TRR were completed healed in all the three groups; however, adhesion around the surgical sites of the Achilles tendons that underwent TRR was obviously observed in the saline group. The Achilles tendons that underwent TRR were connected by scar tissues, and adhesions were observed surrounding the surgical sites in all the saline-treated mice. For the tendons treated with GNRs-1/curc@PMs and laser, fewer and weak adhesions were observed at the repaired site, which were separated easily. No obvious adhesion around the surgical sites of Achilles tendons that underwent TRR was observed macroscopically in both the curcumin group and the GNRs-1/curc@PMs group (Figure 3). The peritendinous adhesions at the repaired tendons were assessed by visual examination based on a scoring system. The scoring results indicated that GNRs-1/curc@PMs group was in the lowest grade of peritendinous adhesions compared to the other groups (Figure 3).
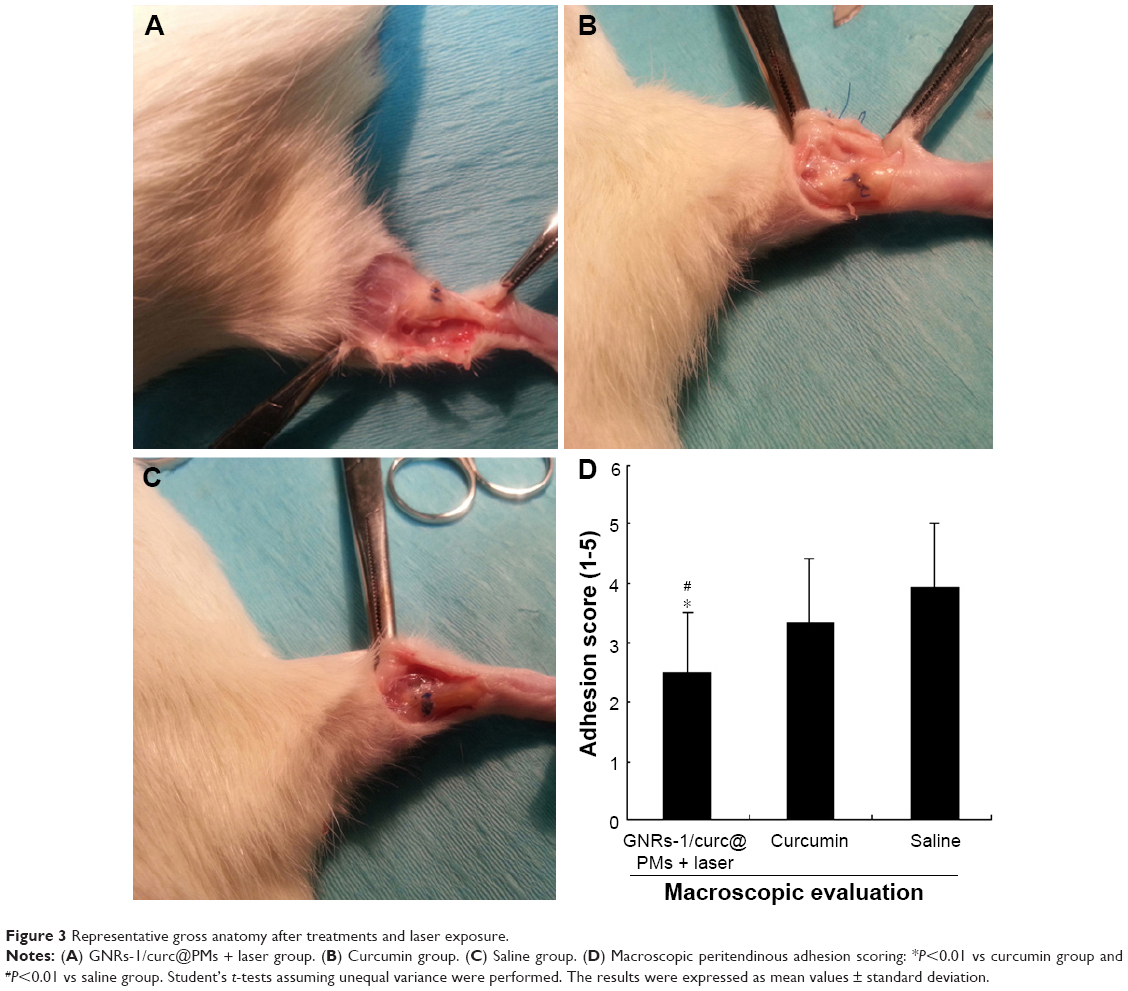 | Figure 3 Representative gross anatomy after treatments and laser exposure. |
Biomechanical improvement
During the functional assessment with mechanical testing, we tested tensile strength and toughness of Achilles tendons that underwent TRR by measuring the gliding distance of flexion and the breaking force. Four weeks after TRR, the range of motion in the TRR + GNRs-1/curc@PMs + laser group was better than the TRR + curcumin group and TRR + saline group. This difference was statistically significant (P<0.01). However, there was no significant difference in breaking force among all the three groups (Figure 4).
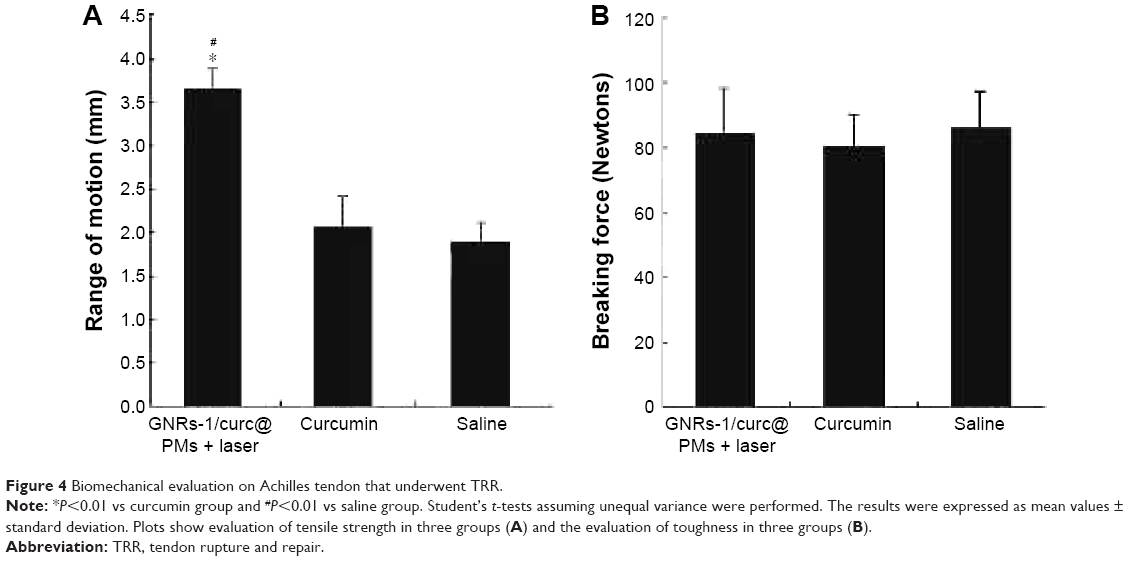 | Figure 4 Biomechanical evaluation on Achilles tendon that underwent TRR. |
Histomorphological findings
Histological results from the sections of the repaired tendons stained with hematoxylin and eosin are shown in Figure 5. Obvious collagen fiber hyperplasia and fibroblast proliferation were observed, and thick fibrous adhesion tissues developed at the repair sites in the saline group. There was no clear peritendinous adhesion, but a little scattered weak fiber formation around the repaired tendons in curcumin group was observed. After 4 weeks of treatment with GNRs-1/curc@PMs + laser, collagen fiber orientation in the tendon end site seemed to be more consistent, and adhesion of the tendon and the surrounding tissue was reduced. Histological assessments of adhesion and inflammation in all the treatment groups were performed. In comparison with the control group and curcumin group, the grade of adhesions in the GNRs-1/curc@PMs + laser treatment group was significantly lower (P<0.01). The grade of inflammation in the GNRs-1/curc@PMs + laser treatment group was also significantly lower (P<0.01) compared to the saline control group but not the curcumin group (Figure 5).
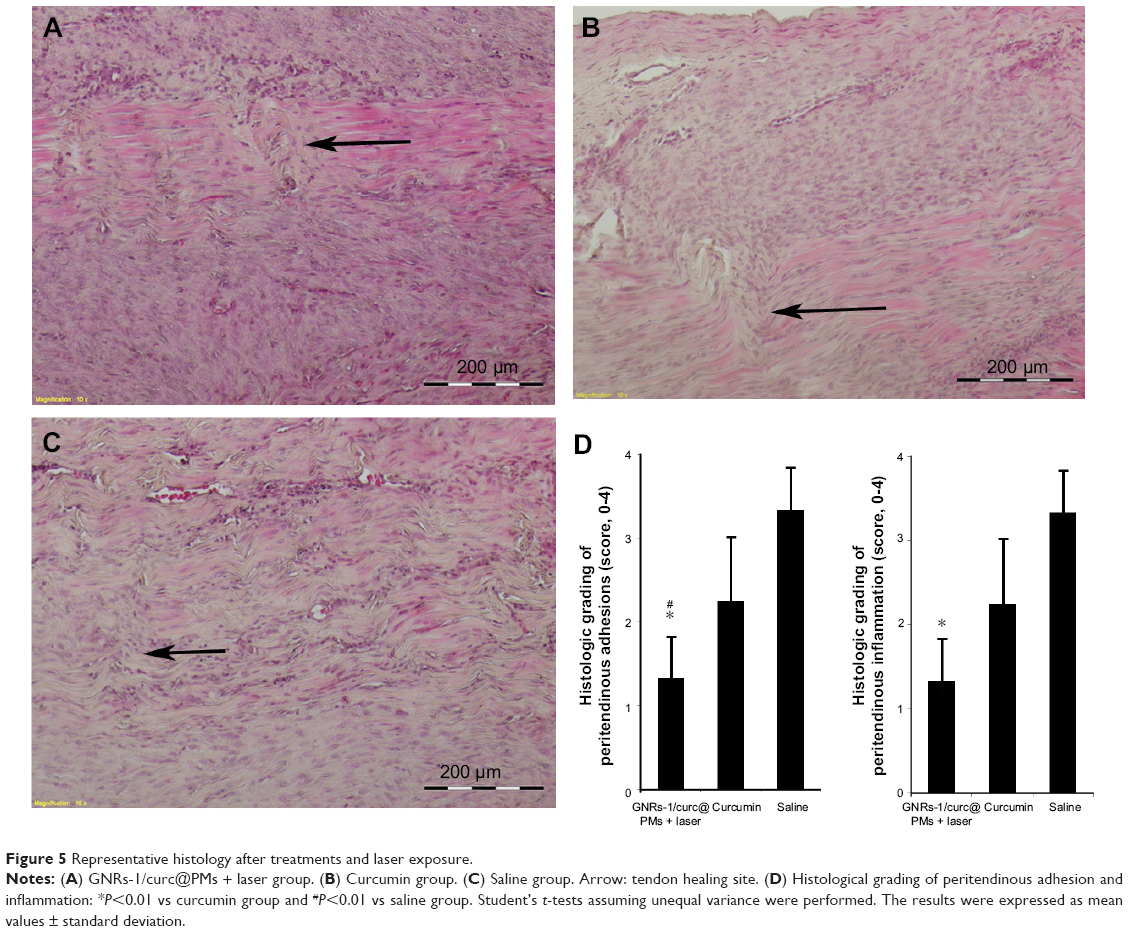 | Figure 5 Representative histology after treatments and laser exposure. |
Discussion
In the present study, we, for the first time, used nanomicelles loaded with GNRs and curcumin (GNRs-1/curc@PMs) to treat locally peritendinous adhesions in a rat model with TRR. With controlled release of curcumin into the surgical sites of TRR, it was found that GNRs-1/curc@PMs combined with NIR light exposure can prevent peritendinous adhesion during Achilles tendon healing. The attempt of using nanoparticle-based drug delivery to prevent peritendinous adhesion could provide a novel therapeutic strategy for clinical application.
A growing body of evidence suggests that extrinsic healing mostly contributed to excessive scar formation. Several pharmacological adjuvants have evolved in the search to find the solution for preventing excessive scar formation after tendon repair surgery. Inflammatory response involving inflammatory cells migrating into the injured site is being considered as an important factor that promotes scar formation. Although evidence suggested that nonsteroidal anti-inflammatory drugs may have a beneficial effect of reducing adhesion, inhibition of inflammation may impair tendon healing similar to what has been observed in fracture healing.23,24 Therefore, an ideal drug would be that which does not inhibit normal wound healing but reduces adhesion at the operative site. Experimentally applying nano-technique for preventing peritendinous adhesions has been reported; however, these attempts made use of either nanofibrous membrane25,26 or AgNP-loaded poly(L-lactide) electrospun fibrous membrane27 as an alternative to current antiadhesion barrier films. No study has been available for the nano-based drug delivery for preventing peritendinous adhesions. In this study, the GNRs-1/curc@PMs were designed to release Au and curcumin under the control of NIR light exposure. The important features of GNRs-1/curc@PMs were biocompatibility and controlled release of Au and curcumin. When administrated locally into the TRR operative site, these GNRs-1/curc@PMs with novel physicochemical properties, especially controlled release of curcumin, could benefit intrinsic healing but not extrinsic healing. The potential mechanisms could be the following: 1) Without NIR irradiation for first week postoperation, GNRs-1/curc@PMs were stable with no release in the TRR operative site and formed a biocompatible barrier between repaired tendons and surrounding tissues. This biocompatible barrier benefited intrinsic healing, and avoided the migration of inflammatory cells into the injured site. Importantly, because no anti-inflammatory drug was released within a week of TRR, the natural process of tendon healing was not affected. 2) Curcumin was shown to be a highly pleiotropic molecule interacting with numerous inflammatory molecular targets, indicating that it was a potential therapeutic agent in many inflammatory diseases.15 Recently, curcumin was reported to improve healing properties of injured tendon through well-organized collagen fiber, extensive deposition of collagen, decreased malondialdehyde level, and increased biomechanical properties and Mn superoxide dismutase activity of the regenerated tendon tissues.16 In this study, upon NIR irradiation, heat was locally generated due to Au nanorods. Au nanorods absorbed the irradiation, and heat was locally generated inside the nanomicelles. The pretreated GNRs-1/curc@PMs released curcumin from nanomicelles and delivered it to the injured site. This controlled delivery of curcumin into the injured site occurred at the second week after TRR, and this is an important time point for the prevention of adhesion because most proinflammatory products contributing to excessive scar appear 2–4 weeks after tendon repair.28 3) During exposure to NIR at 808 nm wavelength at 1 week postoperation, curcumin, an anti-inflammatory agent that limits the extrinsic healing, was released and delivered into the anastomotic site. In addition, heat and Au were also released and delivered into the anastomotic site simultaneously. As the inflammatory phase of tendon healing is characterized by synovial inflammation, both heat and Au could also benefit by controlling the proinflammatory products. This was supported by a similar study, in which Au half-shell nanoparticles containing methotrexate for the treatment of rheumatoid arthritis showed greater therapeutic effects than that of a conventional treatment with methotrexate solution in collagen-induced arthritic mice.29 But the effect of heat and Au on peritendinous adhesions needs to be further demonstrated. 4) GNRs have the distinctive surface chemistries and crystal faces. It has been reported that frequency of the surface plasmon band allows for NIR absorption at the cross sections permitting a deeper penetration into living tissues.30 Although GNRs (data not shown) or curcumin show some benefits on peritendinous adhesion, neither of them has such obvious preventive effects as shown by the GNRs-1/curc@PMs treatment. This indicates that there can be the synergetic effect from the components of GNRs-1/curc@PMs. Nevertheless, our novel drug delivery system of GNRs-1/curc@PMs provided a potential method to maximize therapeutic efficacy and minimize dosage-related side effects of nonsteroidal anti-inflammatory drugs in the treatment of TRR in rats.
In conclusion, this study has shown that application of GNRs-1/curc@PMs to the TRR in rats significantly reduced the formation of peritendinous fibrous adhesions. GNRs-1/curc@PMs may provide a simple means of preventing postoperative adhesions. Further study needs to be carried out to attempt to elucidate the mechanism of GNRs-1/curc@PMs in the prevention of the adhesions in order to delineate the ideal dose and time point required for their use.
Disclosure
The authors report no conflicts of interest in this work.
References
Khanna A, Friel M, Gougoulias N, Longo UG, Maffulli N. Prevention of adhesions in surgery of the flexor tendons of the hand: what is the evidence? Br Med Bull. 2009;90:85–109. | ||
Pulos N, Bozentka DJ. Management of complications of flexor tendon injuries. Hand Clin. 2015;31:293–299. | ||
Manske PR. Flexor tendon healing. J Hand Surg Br. 1988;13:237–245. | ||
Wong JK, Lui YH, Kapacee Z, Kadler KE, Ferguson MW, McGrouther DA. The cellular biology of flexor tendon adhesion formation: an old problem in a new paradigm. Am J Pathol. 2009;175:1938–1951. | ||
Hung LK, Fu SC, Lee YW, Mok TY, Chan KM. Local vitamin-C injection reduced tendon adhesion in a chicken model of flexor digitorum profundus tendon injury. J Bone Joint Surg Am. 2013;95:e41. | ||
Tan V, Nourbakhsh A, Capo J, Cottrell JA, Meyenhofer M, O’Connor JP. Effects of nonsteroidal anti-inflammatory drugs on flexor tendon adhesion. J Hand Surg Am. 2010;35:941–947. | ||
Cabral RM, Baptista PV. Anti-cancer precision theranostics: a focus on multifunctional gold nanoparticles. Expert Rev Mol Diagn. 2014;14:1041–1052. | ||
Shchukin DG, Shchukina E. Capsules with external navigation and triggered release. Curr Opin Pharmacol. 2014;18:42–46. | ||
Uskokovic V. Nanostructured platforms for the sustained and local delivery of antibiotics in the treatment of osteomyelitis. Crit Rev Ther Drug Carrier Syst. 2015;32:1–59. | ||
Chen S, Wang G, Wu T, et al. Silver nanoparticles/ibuprofen-loaded poly(L-lactide) fibrous membrane: anti-infection and anti-adhesion effects. Int J Mol Sci. 2014;15:14014–14025. | ||
Chen CH, Chen SH, Shalumon KT, Chen JP. Dual functional core-sheath electrospun hyaluronic acid/polycaprolactone nanofibrous membranes embedded with silver nanoparticles for prevention of peritendinous adhesion. Acta Biomater. 2015;26:225–235. | ||
Martin RC, Locatelli E, Li Y, et al. Gold nanorods and curcumin-loaded nanomicelles for efficient in vivo photothermal therapy of Barrett’s esophagus. Nanomedicine (Lond). 2015;10:1723–1733. | ||
Lee MH, Hribar KC, Brugarolas T, Kamat NP, Burdick JA, Lee D. Harnessing interfacial phenomena to program the release properties of hollow microcapsules. Adv Funct Mater. 2012;22:131–138. | ||
Gupta MK, Meng F, Johnson BN, et al. 3D printed programmable release capsules. Nano Lett. 2015;15:5321–5329. | ||
He Y, Yue Y, Zheng X, Zhang K, Chen S, Du Z. Curcumin, inflammation, and chronic diseases: how are they linked? Molecules. 2015;20:9183–9213. | ||
Jiang D, Gao P, Lin H, Geng H. Curcumin improves tendon healing in rats: a histological, biochemical, and functional evaluation. Connect Tissue Res. 2016;57(1):20–27. | ||
Nikoobakht B, El-Sayed MA. Preparation and growth mechanism of gold nanorods (NRs) using seed-mediated growth method. Chem Mater. 2003;15:1957–1962. | ||
Gentili D, Ori G, Comes FM. Double phase transfer of gold nanorods for surface functionalization and entrapment into PEG-based nanocarriers. Chem Commun (Camb). 2009;(39):5874–5876. | ||
Ishiyama N, Moro T, Ishihara K, et al. The prevention of peritendinous adhesions by a phospholipid polymer hydrogel formed in situ by spontaneous intermolecular interactions. Biomaterials. 2010;31:4009–4016. | ||
Tang JB, Shi D, Zhang QG. Biomechanical and histologic evaluation of tendon sheath management. J Hand Surg Am. 1996;21:900–908. | ||
Moran SL, Ryan CK, Orlando GS, Pratt CE, Michalko KB. Effects of 5-fluorouracil on flexor tendon repair. J Hand Surg Am. 2000;25:242–251. | ||
Franchini MC, Ponti J, Lemor R, Fournelle M, Broggi F, Locatelli E. Polymeric entrapped thiol-coated gold nanorods: cytotoxicity and suitability as molecular optoacoustic contrast agent. J Mater Chem. 2010;20:10908–10914. | ||
Gerstenfeld LC, Al Ghawas M, Alkhiary YM, et al. Selective and nonselective cyclooxygenase-2 inhibitors and experimental fracture-healing. Reversibility of effects after short-term treatment. J Bone Joint Surg Am. 2007;89:114–125. | ||
Simon AM, O’Connor JP. Dose and time-dependent effects of cyclooxygenase-2 inhibition on fracture-healing. J Bone Joint Surg Am. 2007;89:500–511. | ||
Wu QJ, Li L, Wang N, et al. Biodegradable and thermosensitive micelles inhibit ischemia-induced postoperative peritoneal adhesion. Int J Nanomed. 2014;9:727–734. | ||
Chen SH, Chen CH, Shalumon KT, Chen JP. Preparation and characterization of antiadhesion barrier film from hyaluronic acid-grafted electrospun poly(caprolactone) nanofibrous membranes for prevention of flexor tendon postoperative peritendinous adhesion. Int J Nanomed. 2014;9:4079–4092. | ||
Liu S, Zhao JW, Ruan HJ, et al. Antibacterial and anti-adhesion effects of the silver nanoparticles-loaded poly(L-lactide) fibrous membrane. Mater Sci Eng C Mater. 2013;33:1176–1182. | ||
Wu YF, Tang JB. Tendon healing, edema, and resistance to flexor tendon gliding: clinical implications. Hand Clin. 2013;29:167–178. | ||
Lee SM, Kim HJ, Ha YJ, et al. Targeted chemo-photothermal treatments of rheumatoid arthritis using gold half-shell multifunctional nanoparticles. ACS Nano. 2013;7:50–57. | ||
Arvizo R, Bhattacharya R, Mukherjee P. Gold nanoparticles: opportunities and challenges in nanomedicine. Expert Opin Drug Deliv. 2010;7:753–763. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.