Back to Journals » Open Access Journal of Contraception » Volume 10
Contraception with estradiol valerate and dienogest: adherence to the method
Authors Fruzzetti F ![]() , Paoletti AM, Fidecicchi T, Posar G, Giannini R, Gambacciani M
, Paoletti AM, Fidecicchi T, Posar G, Giannini R, Gambacciani M ![]()
Received 9 February 2019
Accepted for publication 11 April 2019
Published 10 May 2019 Volume 2019:10 Pages 1—6
DOI https://doi.org/10.2147/OAJC.S204655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Franca Fruzzetti,1 Anna Maria Paoletti,2 Tiziana Fidecicchi,1 Giulia Posar,1 Riccardo Giannini,3 Marco Gambacciani1
1Department of Obstetrics and Gynecology, Pisa University Hospital, Pisa, Italy; 2Department of Obstetrics and Gynecology, Cagliari University Hospital, Cagliari, Italy; 3Department of Surgical, Medical, Molecular Pathology and Critical Area, University of Pisa, Pisa, Italy
Purpose: The aim of the study was to examine the discontinuation rate of hormonal contraception with estradiol valerate (E2V) and dienogest (DNG).
Patients and methods: We collected data at the Family Planning Clinics of the Departments of Obstetrics and Gynecology of Pisa and Cagliari. We included in the analysis 354 consecutive women using oral contraceptive pills containing E2V and DNG. We analyzed the rate and the reason for discontinuation, classifying the reasons in 5 categories: 1) minor side effects, 2) adverse events, 3) other events not directly caused by the drug or conditions for which the pill could represent a risk factor, 4) no compliance with the method and 5) no further need.
Results: Of the 354 women examined, 50.8% had discontinued E2V/DNG pill. Excluding women who stopped the pill because of no further need (10.5%), 27.4% discontinued because of minor side effects, 1.7% discontinued for adverse events, 9.9% because of other events not directly caused by the drug or conditions for which the pill could represent a risk factor and 1.4% because of difficulties with compliance. Irregular bleedings were the main reasons reported for discontinuation. The time to discontinuation for irregular bleedings was significantly (p<0.02) longer in adults than in adolescents and slightly but not significantly longer in women who received information about this possible effect.
Conclusion: Unacceptable cycle control was the principal cause of discontinuation of pill with E2V and DNG. An appropriate information about this possible effect may improve adherence to this combined oral contraceptive.
Keywords: estradiol valerate, hormonal contraceptives, irregular bleedings, dienogest
Introduction
The most important problem of combined oral contraceptives (COCs) is still the high rate of discontinuation due to side effects. Since 2010, COCs containing 17β-estradiol (E2-COCs) have been introduced in the market. The well-known pharmacokinetic properties of estradiol (E2) and E2 valerate (E2V)1 contribute to decreasing the incidence of some hormone withdrawal-associated symptoms, possibly reducing the rate of discontinuation.2,3 Moreover, these preparations have negligible effects on carbohydrate and lipid metabolism and hemostasis, showing a safer profile than COCs containing ethinylestradiol (EE-COCs).4–6 In fact, E2 exerts a weaker impact on hepatic metabolism than EE and it is less potent in inducing synthesis of hepatic proteins.1,7,8
There are two different formulations, the combined monophasic one containing E2 and nomegestrol acetate and the quadriphasic formulation containing E2V associated with dienogest (DNG).5,6,9–11
The combination of E2V with a potent progestin like DNG was formulated in order to obtain a better cycle control than the one expected with E2.9 The extended regimen of this combination and the stable levels of E2 throughout the cycle may reduce the incidence of some minor side effects.3 In a Phase III study, the appearance of irregular bleedings is similar to that of the pill with EE and levonorgestrel (LNG), but with a higher incidence of amenorrhea.10
Our study was designed to analyze in a real-life setting the rate and causes of discontinuation with hormonal contraceptives containing E2V/DNG.
Methods
Study design
We collected data at the Family Planning Clinic of the Department of Obstetrics and Gynecology of Pisa and Cagliari University Hospital.
The pill considered for this study was the quadriphasic compound containing E2V 1–3 mg plus DNG 2–3 mg. We searched the patients in our databases of informatic medical records among women who came to our clinics between January 2014 and March 2018. We considered the following eligible for the study: women who attended our clinics and started the use of the pill after its prescription in that period and women who attended our clinics in that period and were already taking the pill because it has been prescribed in our clinics before the period considered (for these women we recorded their baseline information before the start of the pill intake). In order to exclude possible biases, we included in our analysis only women who were first-time users (ie, not switching from another pill). E2V/DNG was administered using an E2 step-down and a progestin step-up approach over 26 days (E2V 3 mg on days 1 and 2, E2V 2 mg and DNG 2 mg on days 3–7, E2V 2 mg and DNG 3 mg on days 8–24, E2V 1 mg on days 25 and 26 and placebo on days 27 and 28).
We found 354 women, and we analyzed their clinical charts. For baseline analysis, we collected information about age and body mass index, educational level (dividing it in “primary school” or “higher than primary school”) and parity (nulliparous or parous) before the beginning of the treatment. All women considered had complete baseline information.
On March 2018, we evaluated if women were still using the pill or if they discontinued it. We recorded the time (expressed in total months of pill intake) and reason for discontinuation and if the women received the information about the possible side effects at the time of prescription. In 19.7% of women, this information was not present in the charts and we obtained it by phone.
We recorded the reasons for stopping in 5 categories: 1) minor side effects (ie, symptoms or events supposedly related to the pill that are not life-threatening and do not cause hospitalization, disability or permanent damage), 2) adverse events (ie, undesirable symptoms or events supposedly related to the use of the pill that can have serious outcomes and require a medical intervention), 3) other events (ie, not life-threatening medical reasons not directly caused by the drug or other conditions for which the pill could represent a risk factor), 4) no compliance with the method (ie, women who do not assume the pill in the proper way) and 5) no further need.
The protocol was approved by the Ethics Committee of the Departments of Obstetrics and Gynecology of Pisa University Hospital (Pisa, Italy) and of Cagliari University Hospital (Cagliari, Italy). All procedures performed in the study were in accordance with the ethical standards of the Committee on Institutional human experimentation and with the Helsinki declaration of 1975, as revised in 1983. Patients gave their written informed consent to data collection and to the review of their anonymous data for clinical publication.
Statistical analysis
All data are reported as mean±SD (M±SD) or as percentage (%). We used the Kaplan–Meier analysis to evaluate the time-to-event for discontinuation stratified according to the reasons. We tested if the discontinuation rate between adolescents and adults was different with the Chi-squared test. We tested the differences in the time of discontinuation for irregular bleeding between adolescents and adults and between women who did and who did not receive the information at the time of prescription with Mann–Whitney U-test.
Statistical analysis was performed using Statistica Software (Statsoft, Palo Alto, CA, USA).
Results
We analyzed 354 consecutive women who received a prescription of the quadriphasic compound containing E2V and DNG. The age range was 14–54 years. Eighty-five (24%) of them were 20 years old or less. Table 1 reports the characteristics of the population. One hundred and eighty (50.8%) of 354 women taking E2-COCs reported to have stopped COCs for some reason. The time until interruption of the hormonal contraceptive ranged from 1 to 84 months (15.2±17.5 months). Excluding women who stopped the pill, the remaining women were still on contraception at the time of the interview from 23±18.7 months (range 1–96 months). There is no difference in the discontinuation rate between adolescents and adults (44.7% vs 52.8%, p=0.19) and the mean time until discontinuation was similar (14.5±16.6 vs 15.4±7.7 months).
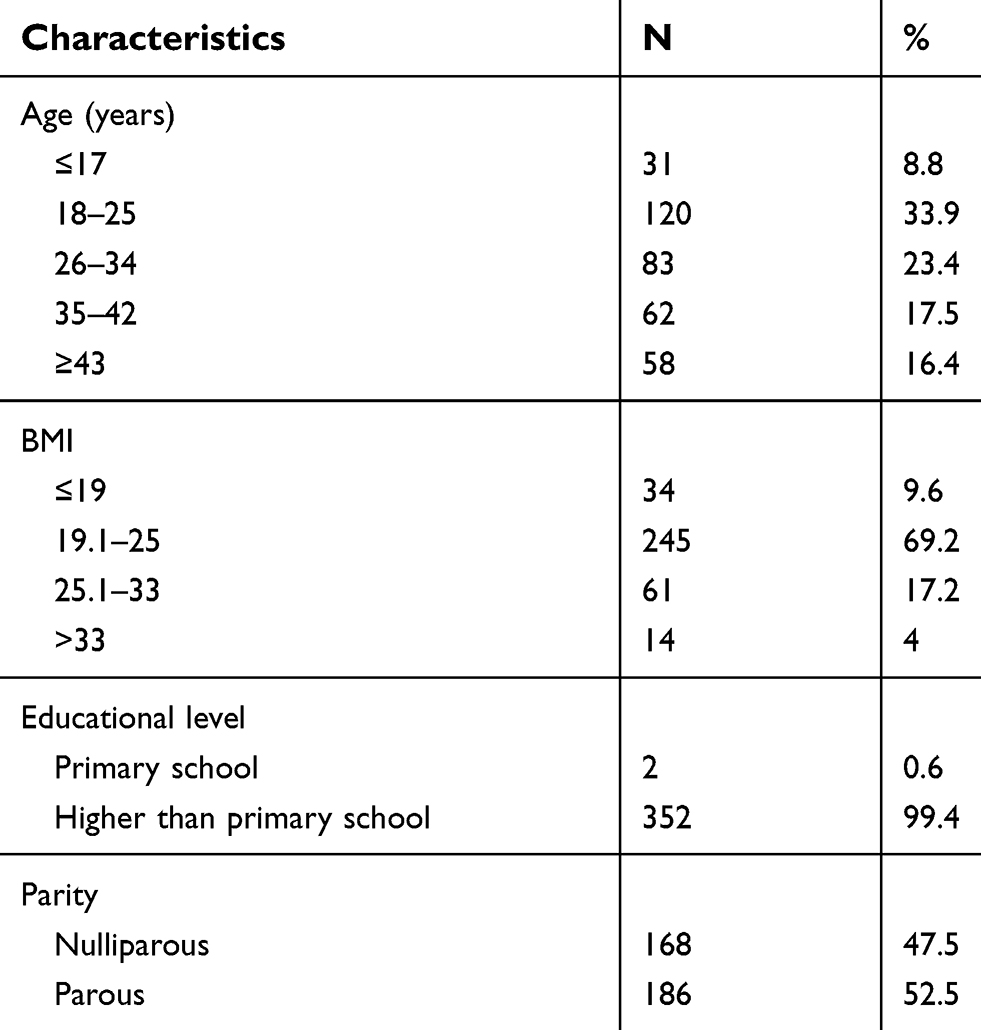 | Table 1 Baseline demographic characteristics of the women (N=354) |
Excluding women who stopped the pill because of no further need (n=37; 10.5%), the most frequent reason for discontinuation was the appearance of minor side effects (n=97; 27.4%). Six women (1.7%) discontinued for adverse events and 35 (9.9%) for other events supposedly not directly caused by the drug or for other conditions for which the pill could represent a risk factor. No compliance for the method was reported by 5 women (1.4%). Most of the women (N=152, 84.4%) interrupted in the first 2 years of pill intake.
Table 2 reports the analysis of minor side effects and the rate of discontinuation. Some of the women who stopped for minor side effects suffered from two or more side effects contemporarily. The most frequent minor side effect was an unacceptable bleeding pattern (n=53; 15.0%), followed by headache (4.0%), mood instability (3.7%), symptoms of hyperandrogenism (3.1%), weight gain (2.5%) and breast tenderness (2.0%). Dysmenorrhea was reported by 0.6% and decreased libido by 0.3% of E2-COCs users.
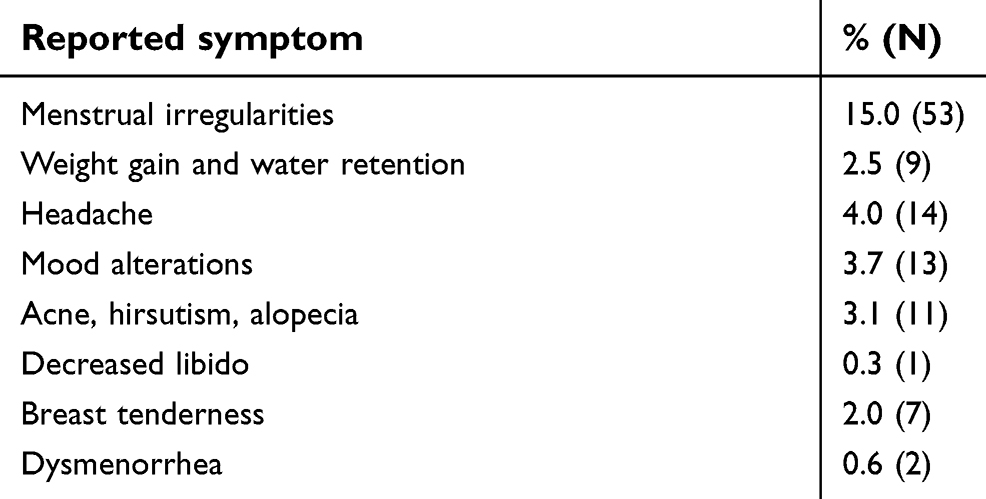 | Table 2 Minor side effects (ie, symptoms or events supposedly related to the pill that are not life-threatening and do not cause hospitalization, disability or permanent damage) reported as cause of discontinuation of the pill with estradiol valerate and dienogest. The results are expressed as a percentage of number of women who discontinued for such effects on the total number (354) of women examined. The absolute number of women who suffered from each side effect is shown in brackets. Some women reported more than one minor side effect contemporarily |
When unacceptable bleeding pattern was the reason, 31 women (58.5%) interrupted the medication within 6 months from the beginning, the others after a longer period (until 3 years). The time of interruption for irregular bleeding was significantly shorter in the adolescent group (5.2±5.2 months) than in the adult group (10±8.3 months; p<0.02) (Figure 1). Twenty-five women (47.2%) who interrupted for an unacceptable bleeding pattern reported that they had not received information about the possibility that amenorrhea and spotting might occur during treatment with pills with E2. The mean duration of pill intake in women who received information at the time of prescription was slightly but not significantly longer (11±9.7 months) than women who did not (7±4.9 months, p=0.06) (Figure 2).
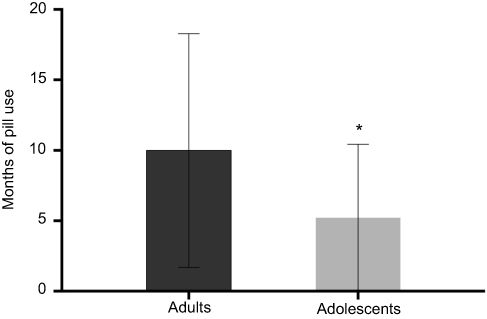 | Figure 1 Interruption of pill with estradiol valerate and dienogest because of unacceptable bleeding according to the age of women. The time (M ± SD) from beginning of pill intake to discontinuation in adolescents was significantly shorter than in the adult group. *: p<0.02. |
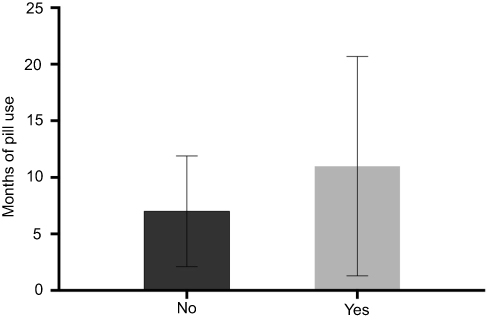 | Figure 2 Interruption of pill with estradiol valerate and dienogest for unacceptable cycle control. Women who were informed about the possible appearance of irregular bleedings interrupted after a longer period than subjects who did not receive the information, but the difference was not significant (p=0.06). Data are expressed as M ± SD. |
Adverse events and all the other medical reasons for discontinuation are listed in Table 3. Among the 6 patients that discontinued because of a severe adverse event, 2 patients had a deep-venous thrombosis (VT). In one case VT occurred after 3 months from the onset of the pill. A more detailed analysis revealed that this woman had a factor V Leiden deficiency. In the other patient, VT occurred after surgery. In 3 cases women reported a superficial venous phlebitis. The woman who reported an episode of depression already had a diagnosis of bipolar disorder.
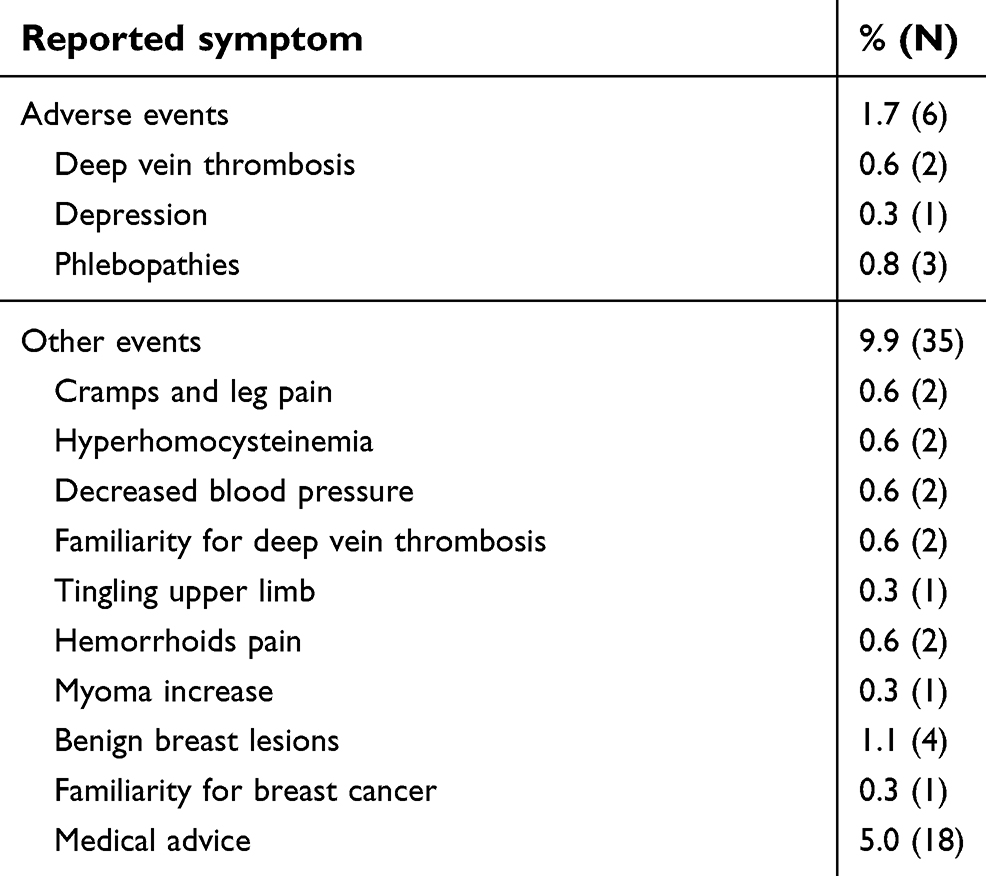 | Table 3 Adverse events (ie, undesirable symptoms or events supposedly related to the use of the pill that can have serious outcomes and require a medical intervention) and other events (ie, not life-threatening medical reasons not directly caused by the drug or other conditions for which the pill could represent a risk factor) reported as cause of discontinuation of hormonal contraception with estradiol valerate and dienogest. The results are expressed as a percentage of total number of women who discontinued for such effects on the total number (354) of women examined. The absolute number of women who reported each symptom is shown in brackets |
Discussion
This is a small observational study undertaken to evaluate the discontinuation rate of hormonal contraception with E2V/DNG in a real-life setting during a random period of 4 years. The aim was to test the supposed improved compliance of E2-COCs toward hormonal contraception. Our study shows that the percentage of women discontinuing E2-COCs is still high, but most of the patients were still taking the pill after 1 year (65%), suggesting the clinical acceptability of the compound in young and adult women. In a previous study, we reported that one-third of users may discontinue pills containing 30 mcg or 20 mcg of EE, mainly due to minor side effects, with irregular bleedings, weight gain and headache being the main reasons reported for discontinuation.12 The unacceptable bleeding pattern is the principal cause for discontinuation also for E2-COCs, whereas the incidence of other minor side effects (weight gain, headache, etc.) was very low. In a European Phase III trial, with 20 cycles of observation, only 2.5% of women discontinued treatment prematurely due to bleeding irregularities.13 Our data are higher than the above, but quite similar to those of a large clinical study performed in a real-life setting (27.7%).14 The discontinuation rate for irregular bleedings that we observed with E2-COCs was higher than that (5.3%) observed in a previous study performed on women who took pills with 20 mcg of EE,12 possibly due to the higher stability of the endometrium when synthetic estrogens were used.15 This may be considered an expected finding since the progestin-induced stimulation of endometrial 17 beta-hydroxysteroid dehydrogenase causes a rapid local inactivation of E2.7,9,15 By contrast, EE cannot be metabolized by this enzyme, as the ethinyl group blocks the oxidation of the 17 beta-hydroxy group. It is noteworthy that the mean time to discontinuation is about 9 months, suggesting that in spite of an unsatisfactory bleeding pattern, women, in general, did not experience problematic bleedings inducing them to quickly interrupt the pill and women wanted to continue with the E2 pill on the whole.
Adolescents stopped the pill for irregular bleeding more and quicker than adults. This finding is very important in clinical practice and must be taken into consideration at the time of prescription. Irregular bleedings and amenorrhea sometimes may arise concerns about their possible negative meanings and adolescents may be more affected by this concern.
Our data also show that the interruption for a low cycle control was mainly noted in users who at the time of prescription had not been informed about the possibility that the use of E2-COCs may be associated with an increased rate of absent withdrawal bleeding or unscheduled bleeding. Our study had not been performed to evaluate the importance and the value of counseling in influencing the rate of discontinuation. Women were only asked if they received the information about possible changes in their cycles, ie, amenorrhea or spotting. Women who had not been informed were more likely to interrupt the pill within 6 months, whereas women who had been informed stopped after a longer period, with a mean duration of pill intake before discontinuation of about 12 months. The difference is not statistically significant because of the small sample of women analyzed. However, the slightly longer time of pill intake in women who had been informed underlines the importance of giving information at the time of prescription, making a detailed counseling about possible side effects and their meaning and focusing on possible changes in the bleeding pattern.
The incidence of major side effects was very low: we observed two cases of VT, one because of thrombophilia and the other after surgery, underlining the relevance of this possible complication also in users of the pill with E2. No other important major side effects were reported, even in those cases where discontinuation had been suggested by a physician for medical reasons.
The principal weakness is that this is a retrospective study. In fact, the study had not been designed to prospectively evaluate in a population of first pill users if E2-COCs had a different discontinuation rate compared to EE-COCs and if an adequate counseling at the time of prescription could modify the behavior of the pill users and then the results. Data had been collected looking into the charts containing all information collected during follow-up visits of women who in a frame of time had their first prescription of a E2-pill in our outpatient clinics.
In conclusion, in our study, the major reason for discontinuation of E2-COCs was the low cycle control. However, the discontinuation occurred after a mean time longer than 1 year. The incidence of other side effects was very low. Moreover, our data suggest that a proper information may improve adherence, reducing the premature pill discontinuation. This further emphasizes the role of the physician at the time of prescription in giving adequate information about all possible side effects related to E2-COCs use and in particular the possible changes in the bleeding pattern. Further larger studies are warranted in order to confirm the role of physician counseling on E2-COC adherence.
Abbreviation list
COCs, combined oral contraceptives; DNG, dienogest; E2, 17β-estradiol; E2-COCs, combined oral contraceptives containing 17β-estradiol; E2V, estradiol valerate; EE, ethinylestradiol; EE-COCs, combined oral contraceptives containing ethinylestradiol; LNG, levonogestrel; VT, venous thrombosis.
Acknowledgment
With thank P Lai for her valuable assistance.
Disclosure
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. Kuhl H. Pharmacology of estrogens and progestogens: influence of different routes of administration. Climacteric. 2005;8(sup1):3–63. doi:10.1080/13697130500148875
2. Jensen JT, Parke S, Mellinger U, Serrani M, Mabey RG. Hormone withdrawal-associated symptoms: comparison of oestradiol valerate/dienogest versus ethinylestradiol/norgestimate. Eur J Contracept Reprod Heal Care. 2013;18(4):274–283. doi:10.3109/13625187.2013.785516
3. Macìas G, Merki-Feld GS, Parke S, Mellinger U, Serrani M. Effects of a combined oral contraceptive containing oestradiol valerate/dienogest on hormone withdrawal-associated symptoms: results from the multicentre, randomised, double-blind, active-controlled HARMONY II study. J Obstet Gynaecol (Lahore). 2013;33(6):591–596. doi:10.3109/01443615.2013.800851
4. Junge W, Mellinger U, Parke S, Serrani M. Metabolic and haemostatic effects of estradiol valerate/dienogest, a novel oral contraceptive. Clin Drug Investig. 2011;31(8):573–584. doi:10.2165/11590220-000000000-00000
5. Klipping C, Duijkers I, Parke S, Mellinger U, Serrani M, Junge W. Hemostatic effects of a novel estradiol-based oral contraceptive. Drugs R D. 2011;11(2):159–170. doi:10.2165/11591200-000000000-00000
6. Gaussem P, Alhenc-Gelas M, Thomas J-L, et al. Haemostatic effects of a new combined oral contraceptive, nomegestrol acetate/17β-estradiol, compared with those of levonorgestrel/ethinyl estradiol. Thromb Haemost. 2011;105(03):560–567. doi:10.1160/TH10-05-0327
7. Kuhnz W, Blode H, Zimmermann H. Pharmacokinetics of exogenous natural and synthetic estrogens and antiestrogens. Oettel M, Schillinger E, Ed Handb Exp Pharmacol Estrogens Antiestrogens II Berlin Springer Verlag. 1993;135(2):261–322.
8. Lindberg UB, Crona N, Stigendal L, Teger-Nilsson AC, Silfverstolpe G. A comparison between effects of estradiol valerate and low dose ethinyl estradiol on haemostasis parameters. Thromb Haemost. 1989;61(1):65–69.
9. Fruzzetti F, Bitzer J. Review of clinical experience with estradiol in combined oral contraceptives. Contraception. 2010;81(1):8–15. doi:10.1016/j.contraception.2009.08.010
10. Ahrendt H-J, Makalová D, Parke S, Mellinger U, Mansour D. Bleeding pattern and cycle control with an estradiol-based oral contraceptive: a seven-cycle, randomized comparative trial of estradiol valerate/dienogest and ethinyl estradiol/levonorgestrel. Contraception. 2009;80(5):436–444. doi:10.1016/j.contraception.2009.03.018
11. Mansour D, Verhoeven C, Sommer W, et al. Efficacy and tolerability of a monophasic combined oral contraceptive containing nomegestrol acetate and 17beta-oestradiol in a 24/4 regimen, in comparison to an oral contraceptive containing ethinylestradiol and drospirenone in a 21/7 regimen. Eur J Contracept Reprod Health Care. 2011;16(6):430–443. doi:10.3109/13625187.2011.614029
12. Fruzzetti F, Perini D, Fornaciari L, Russo M, Bucci F, Gadducci A. Discontinuation of modern hormonal contraceptives: an Italian survey. Eur J Contracept Reprod Heal Care. 2016;21(6):449–454. doi:10.1080/13625187.2016.1234598
13. Palacios S, Wildt L, Parke S, Machlitt A, Römer T, Bitzer J. Efficacy and safety of a novel oral contraceptive based on oestradiol (oestradiol valerate/dienogest): a Phase III trial. Eur J Obstet Gynecol Reprod Biol. 2010;149(1):57–62. doi:10.1016/j.ejogrb.2009.11.001
14. Briggs P, Serrani M, Vogtlander K, Parke S. Continuation rates, bleeding profile acceptability, and satisfaction of women using an oral contraceptive pill containing estradiol valerate and dienogest versus a progestogen-only pill after switching from an ethinylestradiol-containing pill in a real-life setting: results of the CONTENT study. Int J Womens Health. 2016;8:477–487. doi:10.2147/IJWH.S107586
15. Gurpide E, Marks C. Influence of endometrial 17β-hydroxysteroid dehydrogenase activity on the binding of estradiol to receptors. J Clin Endocrinol Metab. 1981;52(2):252–255. doi:10.1210/jcem-52-2-252
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.